
Efficacy and Safety of Pathogen-Reduced Platelets Compared with Standard Apheresis Platelets: A Systematic Review of RCTs



Abstract
:1. Introduction
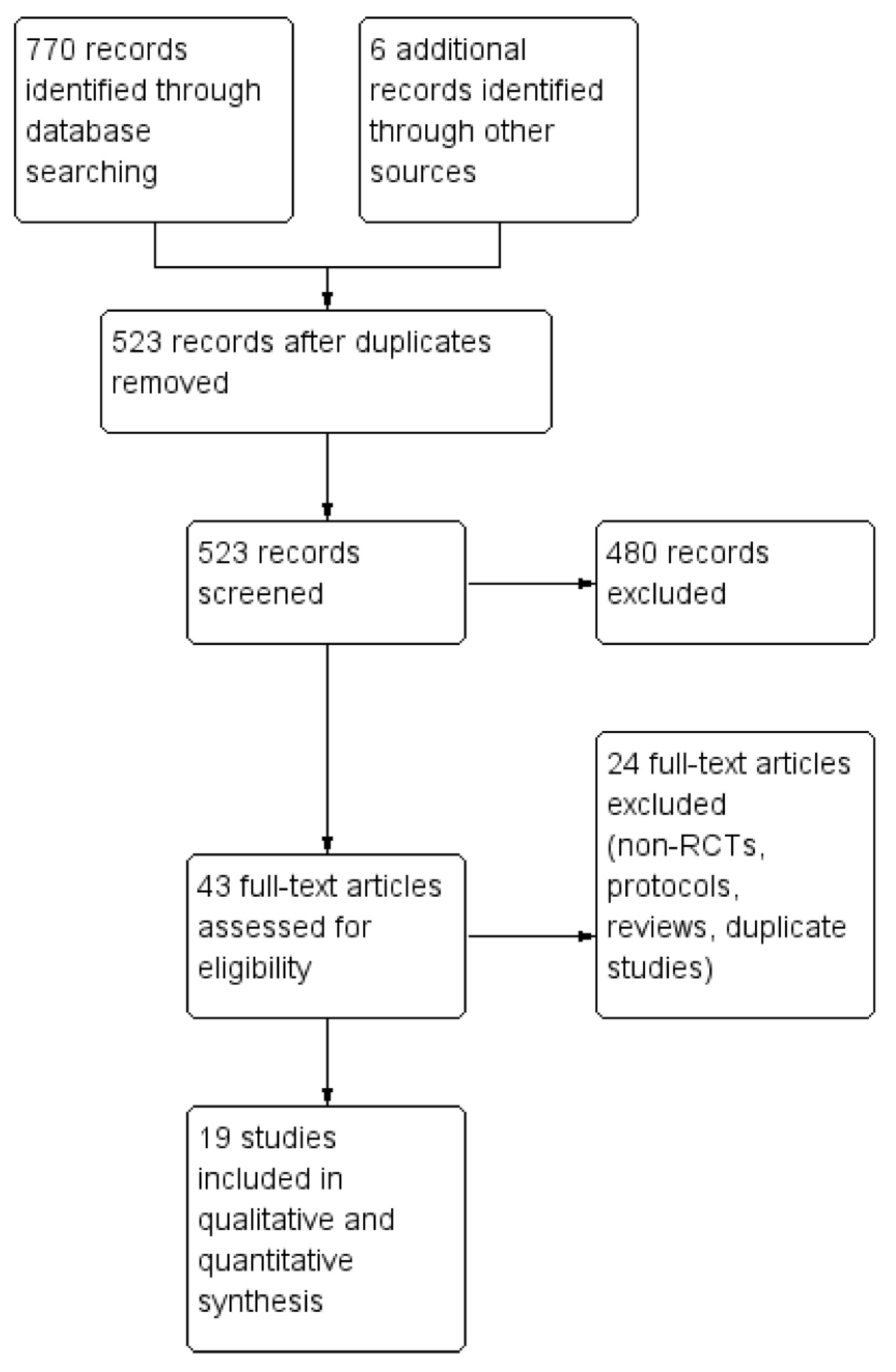
2. Results
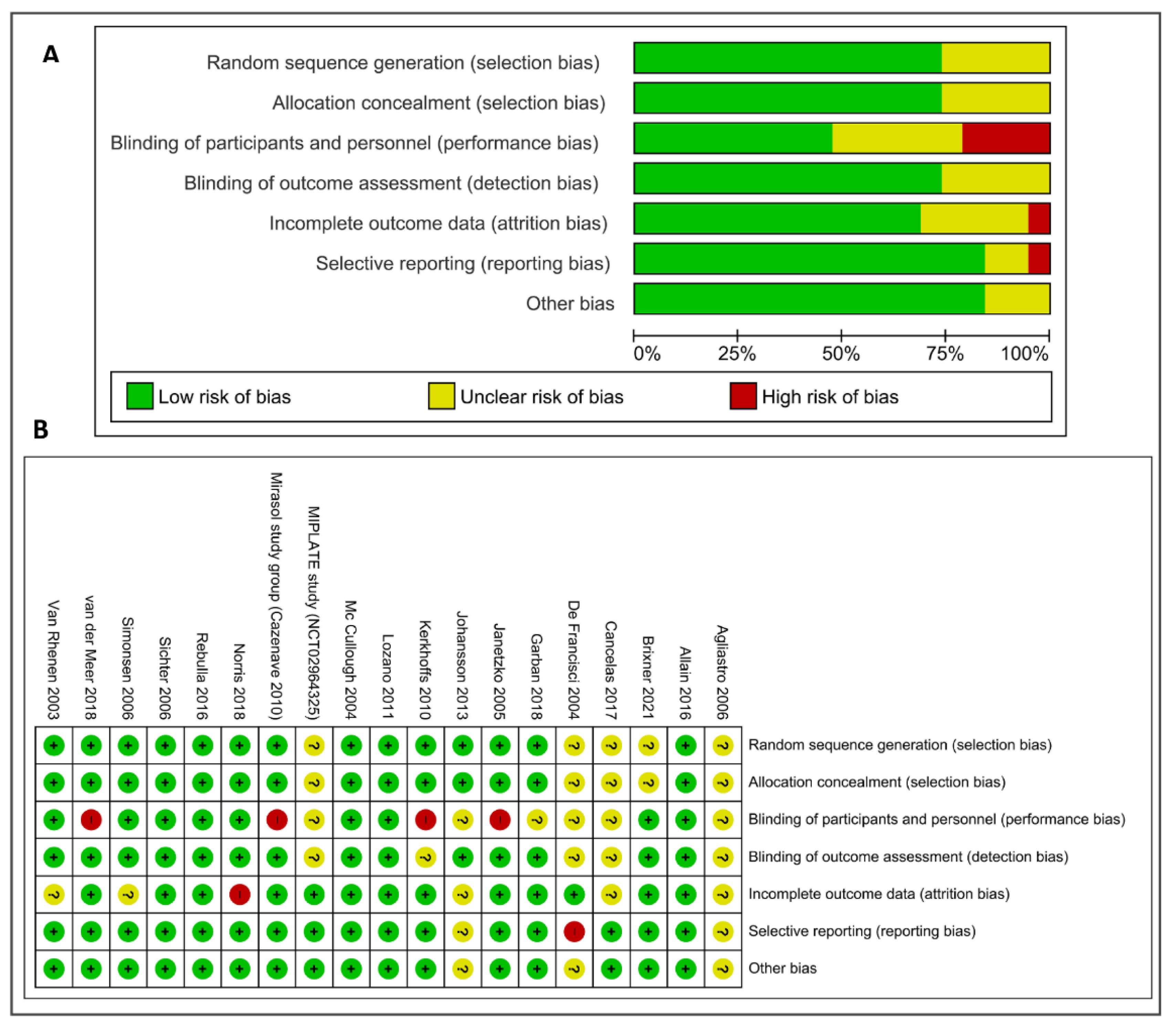
2.1. Risk of Bias in Included Studies
2.2. Effects of Interventions
2.3. Outcomes
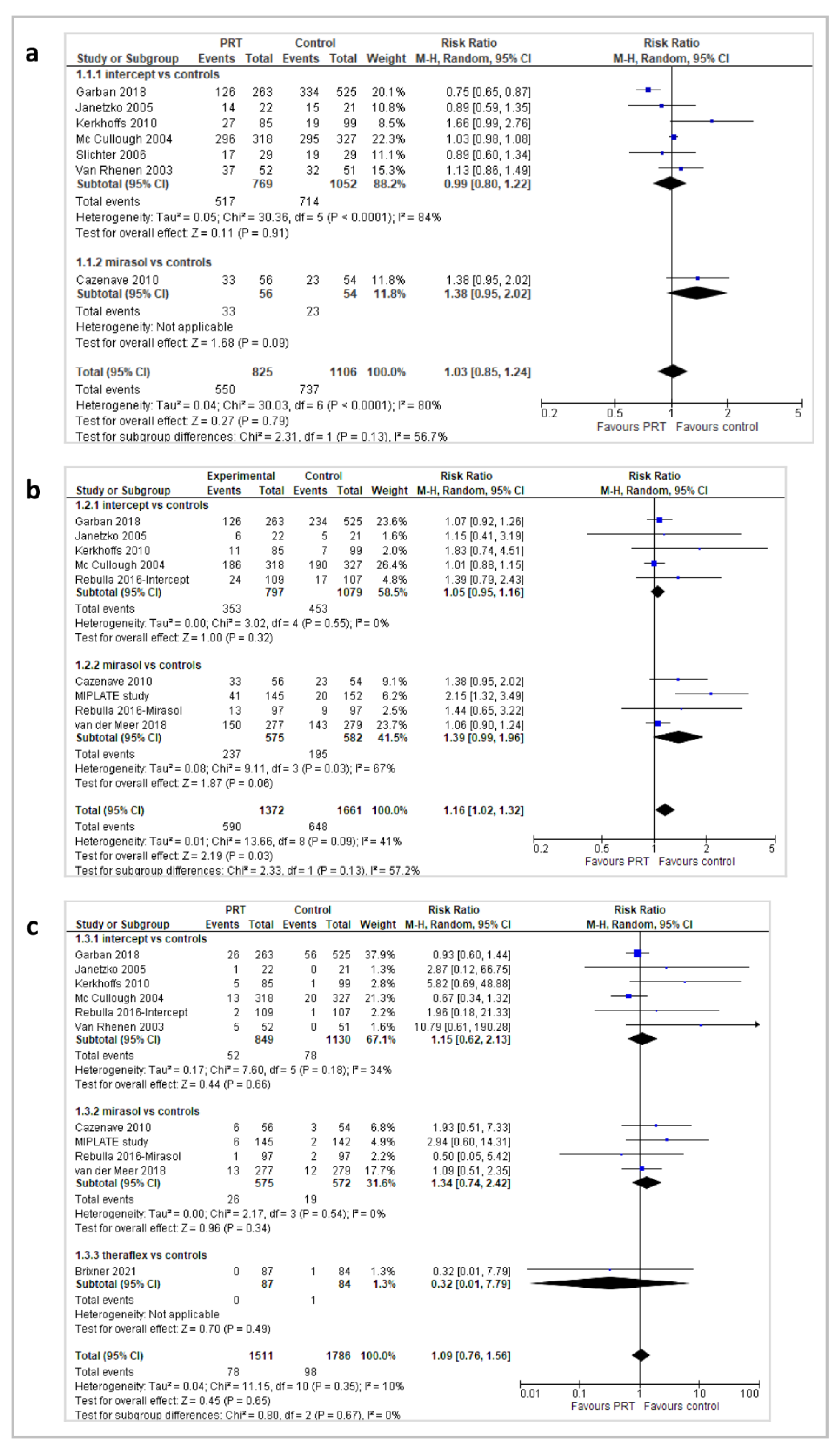
2.3.1. Bleeding Events
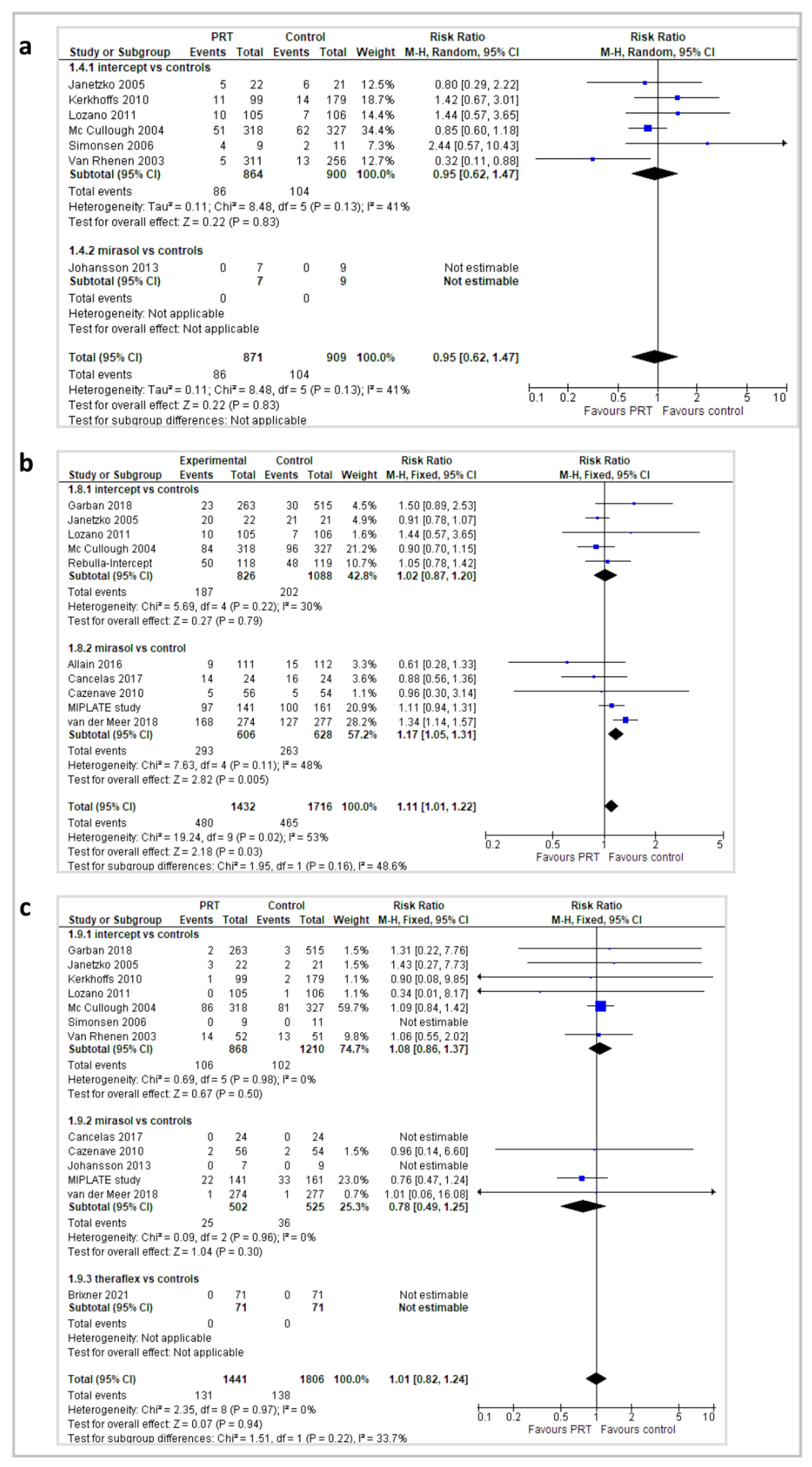
2.3.2. Adverse Events
2.3.3. Platelet Count Increment (CI) and Corrected Count Increment (CCI) at 1 and 24 h
2.3.4. Platelet Refractoriness and Platelet Alloimmunization
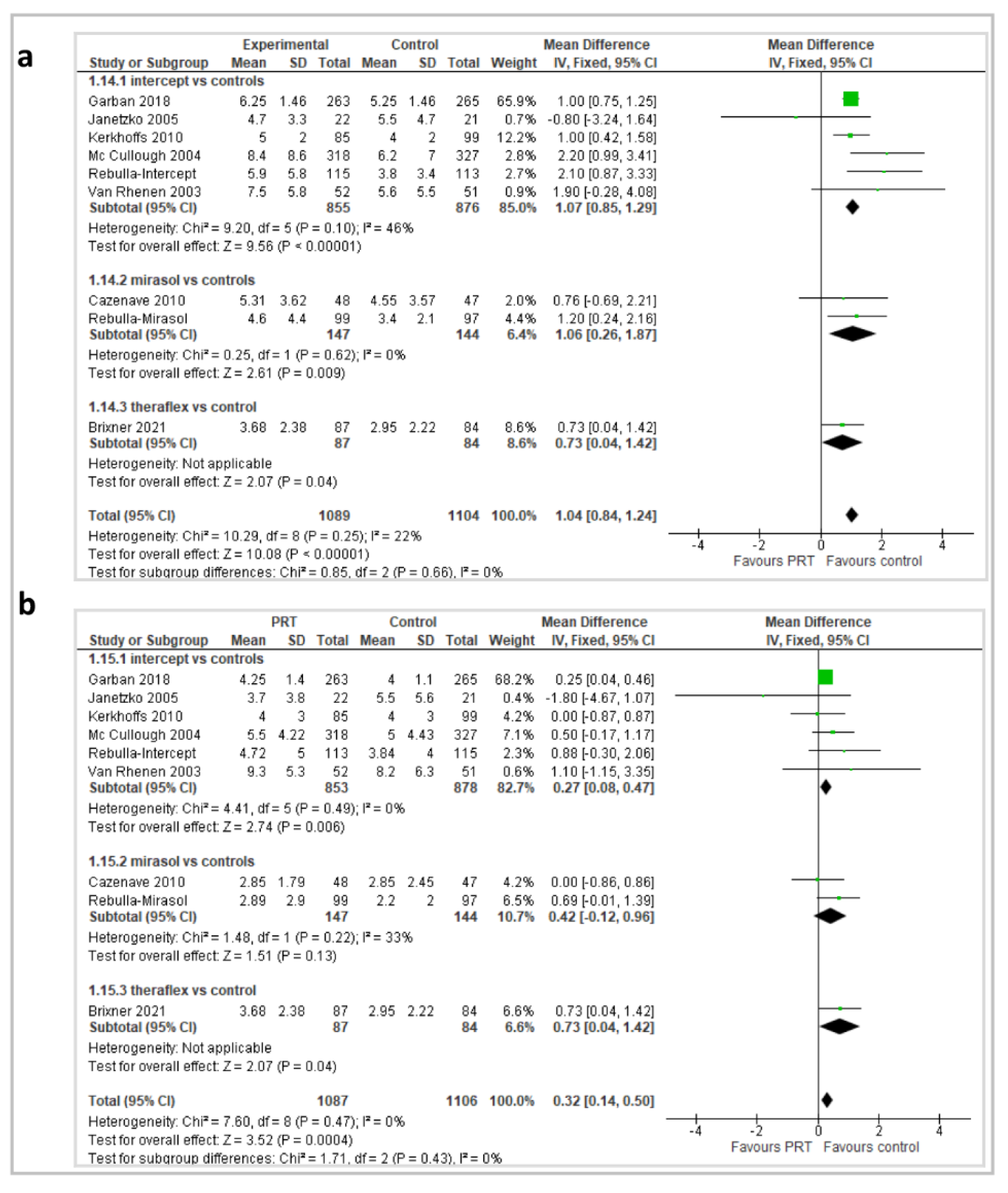
2.3.5. Platelet Transfusions, Platelet Transfusion Interval, and Red Blood Cell Transfusions
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Data Collection and Analysis
4.3. Outcomes
4.4. Subgroup Analyses
4.5. Assessment of Risk of Bias in Included Studies
5. Conclusions and Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Decreto del Ministero Della Salute 2 Novembre 2015. Disposizioni Relative ai Requisiti di Qualità e Sicurezza del Sangue e Degli Emocomponenti. Gazzetta Ufficiale n. 300—Suppl. Ordinario n. 69, 28 Dicembre 2015. Available online: https://www.gazzettaufficiale.it/eli/id/2015/12/28/15A09709/sg (accessed on 20 January 2022). (In Italian).
- Velati, C.; Romanò, L.; Pati, I.; Marano, G.; Piccinini, V.; Catalano, L.; Pupella, S.; Vaglio, S.; Veropalumbo, E.; Masiello, F.; et al. Prevalence, incidence and residual risk of transfusion-transmitted hepatitis B virus infection in Italy from 2009 to 2018. Blood Transfus. 2019, 17, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Velati, C.; Romanò, L.; Piccinini, V.; Marano, G.; Catalano, L.; Pupella, S.; Facco, G.; Pati, I.; Tosti, M.E.; Vaglio, S.; et al. Prevalence, incidence and residual risk of transfusion-transmitted hepatitis C virus and human immunodeficiency virus after the implementation of nucleic acid testing in Italy: A 7-year (2009–2015) survey. Blood Transfus. 2018, 16, 422–432. [Google Scholar] [CrossRef]
- Gould, E.; Pettersson, J.; Higgs, S.; Charrel, R.; De Lamballerie, X. Emerging arboviruses: Why today? One Health 2017, 4, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Italian National Blood Centre. Linea Guida per la Prevenzione Della Contaminazione Batterica del Sangue Intero e Degli Emocomponenti; Linee Guida CNS 02 del 07.07.2008; Italian National Blood Centre: Rome, Italy, 2008. [Google Scholar]
- Blajchman, M.A. ES08.02 Bacterial contamination of cellular blood components: Risks, sources and control. Vox Sang. 2004, 87, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Kopko, P.; Holland, P. Mechanisms of severe transfusion reactions. Transfus. Clin. Biol. 2001, 8, 278–281. [Google Scholar] [CrossRef]
- Buddeberg, F.; Schimmer, B.B.; Spahn, D.R. Transfusion-transmissible infections and transfusion-related immunomodulation. Best Pr. Res. Clin. Anaesthesiol. 2008, 22, 503–517. [Google Scholar] [CrossRef] [Green Version]
- Vasconcelos, E.; Seghatchian, J. Bacterial contamination in blood components and preventative strategies: An overview. Transfus. Apher. Sci. 2004, 31, 155–163. [Google Scholar] [CrossRef]
- Brecher, M.E.; Hay, S.N. Bacterial Contamination of Blood Components. Clin. Microbiol. Rev. 2005, 18, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Wagner, S.J. Transfusion-transmitted bacterial infection: Risks, sources and interventions. Vox Sang. 2004, 86, 157–163. [Google Scholar] [CrossRef]
- Domanović, D.; Cassini, A.; Bekeredjian-Ding, I.; Bokhorst, A.; Bouwknegt, M.; Facco, G.; Galea, G.; Grossi, P.; Jashari, R.; Jungbauer, C.; et al. Prioritizing of bacterial infections transmitted through substances of human origin in Europe. Transfusion 2017, 57, 1311–1317. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Fatalities Reported to FDA Following Blood Collection and Transfusion Annual Sum-mary for Fiscal Year 2019. Available online: https://www.fda.gov/media/147628/download (accessed on 4 April 2022).
- Drew, V.J.; Barro, L.; Seghatchian, J.; Burnouf, T. Towards pathogen inactivation of red blood cells and whole blood targeting viral DNA/RNA: Design, technologies, and future prospects for developing countries. Blood Transfus. 2017, 15, 512–521. [Google Scholar] [CrossRef] [PubMed]
- EDQM. European Directorate for the Quality of Medicines & HealthCare. Guide to the Preparation, Use and Quality Assurance of Blood Components, 20th ed.; EDQM: Strasbourg, France, 2020. [Google Scholar]
- Kerkhoffs, J.-L.H.; Van Putten, W.L.J.; Novotny, V.M.J.; Boekhorst, P.A.T.; Schipperus, M.R.; Zwaginga, J.J.; Van Pampus, L.C.M.; De Greef, G.E.; Luten, M.; Huijgens, P.C.; et al. Clinical effectiveness of leucoreduced, pooled donor platelet concentrates, stored in plasma or additive solution with and without pathogen reduction. Br. J. Haematol. 2010, 150, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efficacy of Mirasol-treated Apheresis Platelets in Patients with Hypoproliferative Thrombocytopenia (MIPLATE). Available online: https://clinicaltrials.gov/ct2/show/NCT02964325 (accessed on 2 April 2022).
- Lozano, M.; Knutson, F.; Tardivel, R.; Cid, J.; Maymó, R.M.; Löf, H.; Roddie, H.; Pelly, J.; Docherty, A.; Sherman, C.; et al. A multi-centre study of therapeutic efficacy and safety of platelet components treated with amotosalen and ultraviolet A pathogen inactivation stored for 6 or 7 d prior to transfusion. Br. J. Haematol. 2011, 153, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Janetzko, K.; Cazenave, J.-P.; Kluter, H.; Kientz, D.; Michel, M.; Beris, P.; Lioure, B.; Hastka, J.; Marblie, S.; Mayaudon, V.; et al. Therapeutic efficacy and safety of photochemically treated apheresis platelets processed with an optimized integrated set. Transfusion 2005, 45, 1443–1452. [Google Scholar] [CrossRef] [PubMed]
- McCullough, J.; Vesole, D.H.; Benjamin, R.J.; Slichter, S.J.; Pineda, A.; Snyder, E.; Stadtmauer, E.A.; Lopez-Plaza, I.; Coutre, S.; Strauss, R.G.; et al. Therapeutic efficacy and safety of platelets treated with a photochemical process for pathogen inactivation: The SPRINT Trial. Blood 2004, 104, 1534–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebulla, P.; Vaglio, S.; Beccaria, F.; Bonfichi, M.; Carella, A.; Chiurazzi, F.; Coluzzi, S.; Cortelezzi, A.; Gandini, G.; Girelli, G.; et al. Clinical effectiveness of platelets in additive solution treated with two commercial pathogen-reduction technologies. Transfusion 2017, 57, 1171–1183. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, A.C.; Johansson, P.I.; Conlan, M.G.; Jacquet, M.; Lin, J.-S.; Junge, K.; Lin, L.; Sorensen, H.; Borregaard, N.; Flament, J. Transfusion of 7-day-old amotosalen photochemically treated buffy-coat platelets to patients with thrombocytopenia: A pilot study. Transfusion 2006, 46, 424–433. [Google Scholar] [CrossRef]
- Van Rhenen, D. Transfusion of pooled buffy coat platelet components prepared with photochemical pathogen inactivation treatment: The euroSPRITE trial. Blood 2002, 101, 2426–2433. [Google Scholar] [CrossRef] [Green Version]
- Brixner, V.; Bug, G.; Pohler, P.; Krämer, D.; Metzner, B.; Voß, A.; Casper, J.; Ritter, U.; Klein, S.; Alakel, N.; et al. Efficacy of UVC-treated, pathogen-reduced platelets versus untreated platelets: A randomized controlled non-inferiority trial. Haematologica 2021, 106, 1086–1096. [Google Scholar] [CrossRef]
- Garban, F.; Guyard, A.; Labussière, H.; Bulabois, C.-E.; Marchand, T.; Mounier, C.; Caillot, D.; Bay, J.-O.; Coiteux, V.; Schmidt-Tanguy, A.; et al. Evaluation of the Efficacy of Platelets Treated with Pathogen Reduction Process (EFFIPAP) Study Group. Comparison of the Hemostatic Efficacy of Pathogen-Reduced Platelets vs Untreated Platelets in Patients With Thrombocytopenia and Malignant Hematologic Diseases. JAMA Oncol. 2018, 4, 468–475. [Google Scholar] [CrossRef]
- Van Der Meer, P.F.; Ypma, P.F.; Van Geloven, N.; Van Hilten, J.A.; Van Wordragen-Vlaswinkel, R.J.; Eissen, O.; Zwaginga, J.J.; Trus, M.; Beckers, E.A.M.; Boekhorst, P.T.; et al. Hemostatic efficacy of pathogen-inactivated vs untreated platelets: A randomized controlled trial. Blood 2018, 132, 223–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, P.I.; Simonsen, A.C.; Brown, P.N.; Ostrowski, S.R.; Deberdt, L.; Van Hoydonck, P.; Yonemura, S.S.; Goodrich, R.P. A pilot study to assess the hemostatic function of pathogen-reduced platelets in patients with thrombocytopenia. Transfusion 2012, 53, 2043–2052. [Google Scholar] [CrossRef] [PubMed]
- Allain, J.-P.; Owusu-Ofori, A.K.; Assennato, S.M.; Marschner, S.; Goodrich, R.P.; Owusu-Ofori, S. Effect of Plasmodium inactivation in whole blood on the incidence of blood transfusion-transmitted malaria in endemic regions: The African Investigation of the Mirasol System (AIMS) randomised controlled trial. Lancet 2016, 387, 1753–1761. [Google Scholar] [CrossRef]
- Cancelas, J.A.; Slichter, S.J.; Rugg, N.; Pratt, P.G.; Nestheide, S.; Corson, J.; Pellham, E.; Huntington, M.; Goodrich, R. Red blood cells derived from whole blood treated with riboflavin and ultraviolet light maintain adequate survival in vivo after 21 days of storage. Transfusion 2017, 57, 1218–1225. [Google Scholar] [CrossRef] [Green Version]
- Slichter, S.J.; Raife, T.J.; Davis, K.; Rheinschmidt, M.; Buchholz, D.H.; Corash, L.; Conlan, M.G. Platelets photochemically treated with amotosalen HCl and ultraviolet A light correct prolonged bleeding times in patients with thrombocytopenia. Transfusion 2006, 46, 731–740. [Google Scholar] [CrossRef]
- Cazenave, J.-P.; Folléa, G.; Bardiaux, L.; Boiron, J.-M.; Lafeuillade, B.; Debost, M.; Lioure, B.; Harousseau, J.-L.; Tabrizi, R.; Cahn, J.-Y.; et al. A randomized controlled clinical trial evaluating the performance and safety of platelets treated with MIRASOL pathogen reduction technology. Transfusion 2010, 50, 2362–2375. [Google Scholar] [CrossRef]
- Agliastro, R.E.; De Francisci, G.; Bonaccorso, R.; Spicola, D.; Ziino, O.; Arico, M.; D’Alia, G. Clinical study in pediatric hemato on-cology patients: Efficacy of pathogen inactivated buffy coat platelets versus aphaeresis platelets. Transfusion 2006, 46, 117A. [Google Scholar]
- Norris, P.J.; Kaidarova, Z.; Maiorana, E.; Milani, S.; Lebedeva, M.; Busch, M.P.; Custer, B.; Rebulla, P. Ultraviolet light-based pathogen inactivation and alloimmunization after platelet transfusion: Results from a randomized trial. Transfusion 2018, 58, 1210–1217. [Google Scholar] [CrossRef]
- De Francisci, G.; Bonaccorso, R.; Bellavia, D.; D’Alia, G.; Fiandaca, T.; Giancana, A.; Giancana, B.; Mazzola, A.; Nuara, G.; Burgio, G.; et al. Clinical trial on the use of pathogen inactivated platelets, with Helinx® technology, in cardio paediatric surgery and cirrhotic patients. Transfusion 2004, 44, 17A. [Google Scholar]
- Butler, C.; Doree, C.; Estcourt, L.J.; Trivella, M.; Hopewell, S.; Brunskill, S.J.; Stanworth, S.; Murphy, M.F. Pathogen-reduced platelets for the prevention of bleeding. Cochrane Database Syst. Rev. 2013, 28, CD009072. [Google Scholar] [CrossRef] [Green Version]
- Estcourt, L.J.; Malouf, R.; Hopewell, S.; Trivella, M.; Dorée, C.; Stanworth, S.J.; Murphy, M.F. Pathogen-reduced platelets for the prevention of bleeding. Cochrane Database Syst. Rev. 2017, 7, CD009072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and me-ta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schünemann, H.J.; Oxman, A.D.; Vist, G.E.; Higgins, J.P.; Deeks, J.J.; Glasziou, P.; Guyatt, G.H. Chapter 12: Interpreting results and drawing conclusions. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011); Higgins, J.P.T.C., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 1 April 2022).
- Schünemann, H.J.; Oxman, A.D.; Higgins, J.P.; Vist, G.E.; Glasziou, P.; Guyatt, G.H. Chapter 11: Presenting results and ’Summary of findings’ tables. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011); Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 1 April 2022).
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) [Ref] | Study Design | Study Population | Pathogen Reduction Technology | Control | Outcome/s | Main Results |
|---|---|---|---|---|---|---|
| Kerkhoffs JLH. (2010)[16] | RCT, parallel group | Hemato-oncological pts with thrombocytopenia or expected to be thrombocytopenic caused by myelosuppression. Recruited: 295, treated: 278. | Intercept® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | Pathogen reduction of PLTs probably leads to decreased PLT viability and perhaps compromises hemostatic function. |
| MIPLATE study. (2016–2021)[17] | RCT, DB, parallel group | Hemato-oncological pts. Recruited: 422, treated: 330. | Mirasol® | St-PLTs | Bleeding assessments, refractoriness, alloimmunization, adverse transfusion reactions | The results show an increase in bleeding and refractoriness in treatment with PR-PLTs compared with control. There are no significant differences for serious adverse events. |
| Lozano M. (2011)[18] | RCT, DB, parallel group | Hemato-oncological pts. Recruited: 242, treated: 211. | Intercept® | St-PLTs | PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, adverse transfusion reactions | PR-PLTs stored for up to 7 d provided 1 h CCI and CI within therapeutic ranges not significantly inferior to St-PLTs. |
| Janetzko K. (2005)[19] | RCT, DB, parallel group | Pts with thrombocytopenia and hemato-oncological diagnosis. Recruited: 43, treated: 43. | Intercept® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | PR-PLT concentrates provide effective PLT transfusion support to thrombocytopenic patients and adequate hemostasis. |
| McCullough J. (2004)[20] | RCT, DB, parallel group | Patients with thrombocytopenia. Recruited: 671, treated: 645. | Intercept® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | PR-PLTs were clinically effective in maintaining hemostasis and appear to be associated with an acceptable safety profile. |
| Rebulla P. (2017)[21] | RCT, parallel group | Hemato-oncological pts. Recruited: 438, treated: 424 (228 Intercept®, 196 Mirasol®). | Intercept®, Mirasol® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | The study provides additional information on the safety and efficacy of PR-PLTs treated with two commercial pathogen reduction technologies. |
| Simonsen AC. (2006)[22] | RCT, DB, parallel group, crossover | Hemato-oncological pts. Recruited: 28, treated: 25. | Intercept® | St-PLTs | PLT transfusion interval, CI and CCI 1 h post-transfusion, adverse transfusion reactions | This study failed to show noninferiority within the specified margin of inferiority; 7-day-old PR-PLTs showed acceptable efficacy and safety compared with 7-day-old St-PLTs. |
| Van Rhenen D. (2003)[23] | RCT, DB, parallel group | Hemato-oncological pts. Recruited: 103, treated: 103. | Intercept® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | PR-PLTs offer the potential to further improve the safety of PLT transfusion using technology compatible with current methods to prepare buffy coat PLT components. |
| Brixner V. (2021)[24] | RCT, DB, parallel group | Hemato-oncological pts. Recruited: 175, treated: 171. | Theraflex® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CI and CCI 1 and 24 h post-transfusion, refractoriness, alloimmunization, adverse transfusion reactions | Transfusion of PR-PLTs produced with the UVC technology is safe, but noninferiority was not demonstrated. |
| Garban F. (2018)[25] | RCT, parallel group | Hemato-oncological pts. Recruited: 842, treated: 795. | Intercept® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, CCI 24 h post-transfusion, adverse transfusion reactions | The hemostatic efficacy of PR to PLTs in additive solution; such noninferiority was not achieved when comparing PR-PLTs with PLTs in plasma. |
| Van der Meer PF. (2018)[26] | RCT, parallel group | Hemato-oncological pts. Recruited: 469, treated: 469. | Mirasol® | St-PLTs | Bleeding assessments, PLT transfusion interval, adverse transfusion reactions | The noninferiority criterion for PR-PLTs was met in the intention-to-treat analysis. |
| Johansson PI. (2013)[27] | RCT, parallel group, crossover | Hemato-oncological pts. Recruited: 15, treated: 15. | Mirasol® | St-PLTs | Adverse transfusion reactions | PR-PLTs that remain in circulation provide comparable hemostatic function to untreated PLTs. |
| Allain JP. (2016)[28] | RCT, DB, parallel group | Hematological pts. Recruited: 227, treated: 223. | Mirasol® | Standard whole blood | Adverse transfusion reactions | There was no increase in adverse events in patients who received the treated blood. |
| Cancelas JA. (2017)[29] | RCT, parallel group | In vitro 41 subjects, in vivo 26 subjects. | Mirasol® | Standard RBCs | Adverse transfusion reactions | RBCs prepared using amustaline pathogen reduction meet the FDA criteria for post-transfusion recovery and are metabolically and physiologically appropriate for transfusion following 35 days of storage. |
| Slichter SJ. (2006)[30] | RCT, parallel group, crossover | Hemato-oncological pts. Recruited: 60, treated: 32. | Intercept® | St-PLTs | Bleeding assessments, CCI 1 and 24 h post-transfusion, CI and CCI 18 to 24 h, adverse transfusion reactions | PR-PLTs provided correction of prolonged bleeding times and transfusion intervals not significantly different than reference PLTs despite significantly lower PLT count increments and CCIs. |
| Cazenave JP. (2010)[31] | RCT, parallel group | Hemato-oncological pts. Recruited: 118, treated: 110. | Mirasol® | St-PLTs | Bleeding assessments, no. of PLT and RBC transfusions, PLT transfusion interval, CCI 1 and 24 h post-transfusion, refractoriness, adverse transfusion reactions | The study failed to show noninferiority of PR-PLTs based on predefined CCI criteria. |
| Agliastro RE. (2006)[32] | RCT, parallel group | Hemato-oncological pts. Recruited: 30, treated: 30. | Intercept® | St-PLTs | Refractoriness, alloimmunization | The study was only available as an abstract and did not provide usable data on all adverse events. |
| Norris JP. (2018)[33] | RCT, parallel group | Hemato-oncological pts. Recruited: 358, treated: 358 (179 Intercept®, 179 Mirasol®). | Intercept®, Mirasol® | St-PLTs | Alloimmunization | The study was not sufficiently powered to determine whether pathogen reduction treatment provides protection from human leukocyte antigen alloimmunization in PLT transfusion recipients. |
| De Francisci G. (2004)[34] | RCT, parallel group | 16 children with congenital cyanogen cardiopathy, 28 adults with cirrhosis who are thrombocytopenic. Recruited: 44, treated: 44. | Intercept® | St-PLTs | Bleeding assessments, CCI 1 and 24 h post-transfusion, adverse transfusion reactions | Study published as abstract, original study protocol not available for comparison. Minimal participant background characteristics reported. For the cirrhotic group, 1 h CCI not reported. No standard deviations reported for mean 1 and 24 h CCIs. Pre- and post-transfusion PLT counts not reported for either intervention. |
| Pathogen Reduction PLTs | ||||||
|---|---|---|---|---|---|---|
| Patient or population: 17 trials in hemato-oncological patients Settings: in and outpatients Intervention: PR-PLTs Comparison: St-PLTs | ||||||
| Outcomes | Illustrative comparative risks * (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Controls (St-PLTs) | Intervention (PR-PLTs) | |||||
| Bleeding events | ||||||
| Any bleeding events | 666 per 1000 | 699 per 1000 (from 559 to 859) | RR 1.03 (95% CIs, −0.85 to 1.24) | 1931 patients (7 trials, 6 with Intercept®, 1 with Mirasol®) | ⊕⊕⊕⊕ high 1 | No between-groups difference in the occurrence of bleeding was observed in the overall analysis and in subgroup analyses of Intercept® and Mirasol® trials. |
| Significant bleeding | 390 per 1000 | 452 per 1000 (from 397 to 514) | RR 1.16 (95% CIs, 1.02/1.32) | 3033 patients (9 trials, 5 with Intercept®, 4 with Mirasol®) | ⊕⊕⊕⊝ moderate ^ | Significant bleeding (WHO grade ≥ 2) was more commonly observed in PR-PLT group compared with St-PLT in the overall analysis, although no between-groups difference was observed in subgroup analysis of Intercept® and Mirasol® trials. |
| Severe bleeding | 54.8 per 1000 | 59.7 per 1000 (from 41.6 to 85.4) | RR 1.09 (95% CIs, 0.76/1.56) | 3299 patients (11 trials, 6 with Intercept®, 4 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊝ moderate ^ | For the outcome severe bleeding (WHO grade ≥ 3), no between-groups difference was observed in the overall analysis and in subgroup analyses of Intercept®, Mirasol®, and Theraflex® trials. |
| Adverse events | ||||||
| Any adverse event | 292 per 1000 | 318 per 1000 (from 294 to 347) | RR 1.09 (95% CIs, 1.01/1.19) | 3345 patients (11 trials, 6 with Intercept® and 5 with Mirasol®) | ⊕⊕⊝⊝ low 2 | In the overall analysis and in the subgroup of Mirasol® trials, overall adverse events were more commonly observed in PR-PLT group compared with St-PLTs. No between-groups difference was observed in subgroup analysis of Intercept® trials. |
| Serious adverse events | 76 per 1000 | 76 per 1000 (from 62 to 94) | RR 1.01 (95% CIs, 10.82/1.24) | 3247 patients (11 trials, 7 with Intercept®, 4 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊝ moderate 3 | No between-groups difference in the occurrence of serious adverse events was observed in the overall analysis and in subgroup analyses of Intercept®, Mirasol®, and Theraflex® trials. |
| PLT Count increment | ||||||
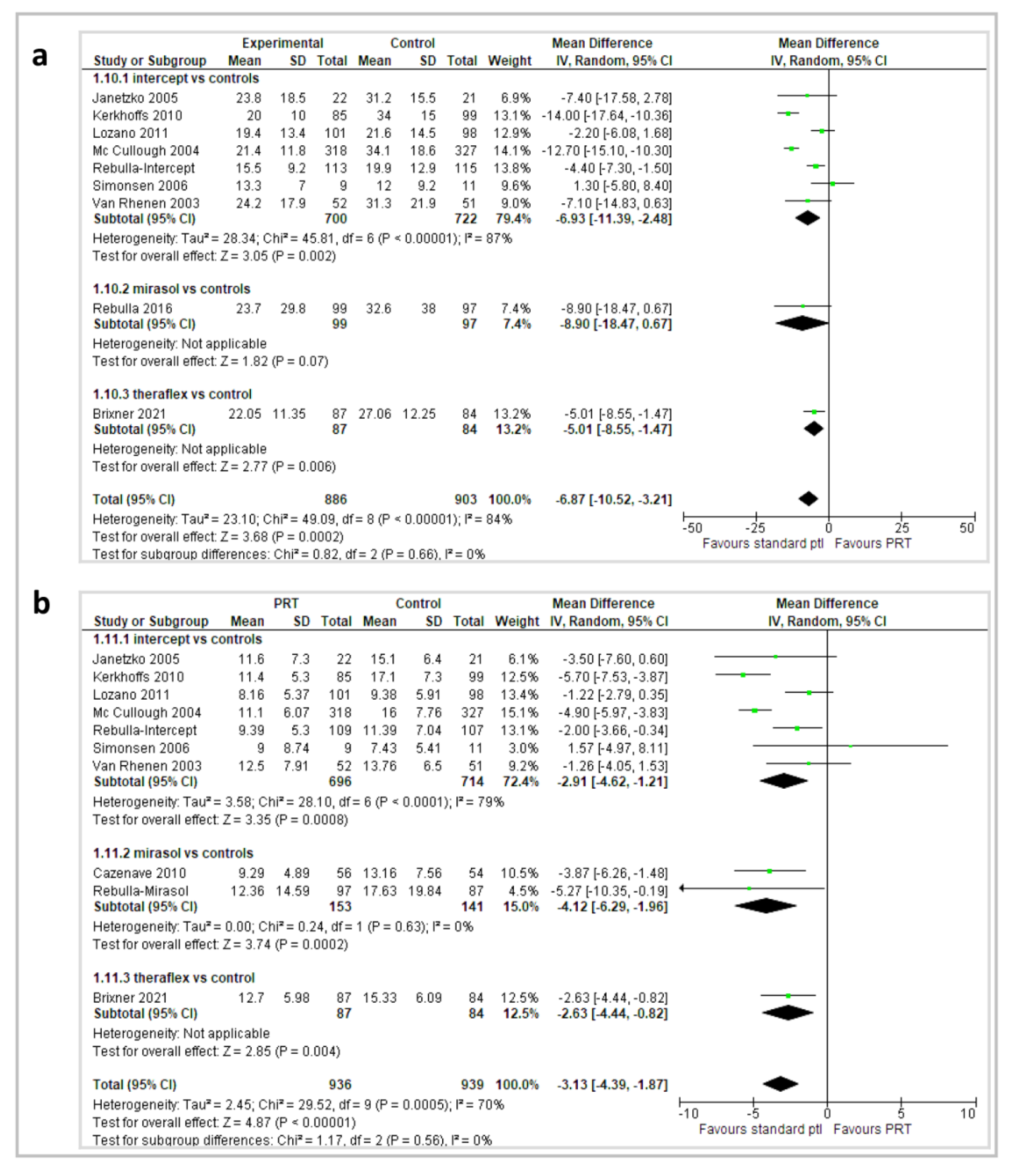
| 1 h CI | The mean 1 h CI ranged across St-PLT group from 13.2 to 24.2 | The mean 1 h CI score in PR group was from 1.3 higher to 14 lower | MD −6.87 (95% CIs, −10.52 to −3.21) | 1847 patients (10 trials, 8 with Intercept®, 1 with Mirasol®, and 1 with Theraflex®) | ⊕⊕⊕⊝ moderate ^ | Combining data across 10 trials showed that participants who received PR-PLT transfusions had a lower 1 h CI. |
| 1 h CCI | The mean 1 h CCI ranged across St-PLT group from 7.4 to 17.1 | The mean 1 h CCI score in PR group was from 1.57 higher to 5.7 lower | MD −3.13 (95% CIs, −4.39 to −1.87) | 1933 patients (11 trials, 8 with Intercept®, 3 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊝ moderate ^ | In the overall analysis and in subgroup analyses, participants who received PR-PLT transfusions had a lower 1 h CCI. |
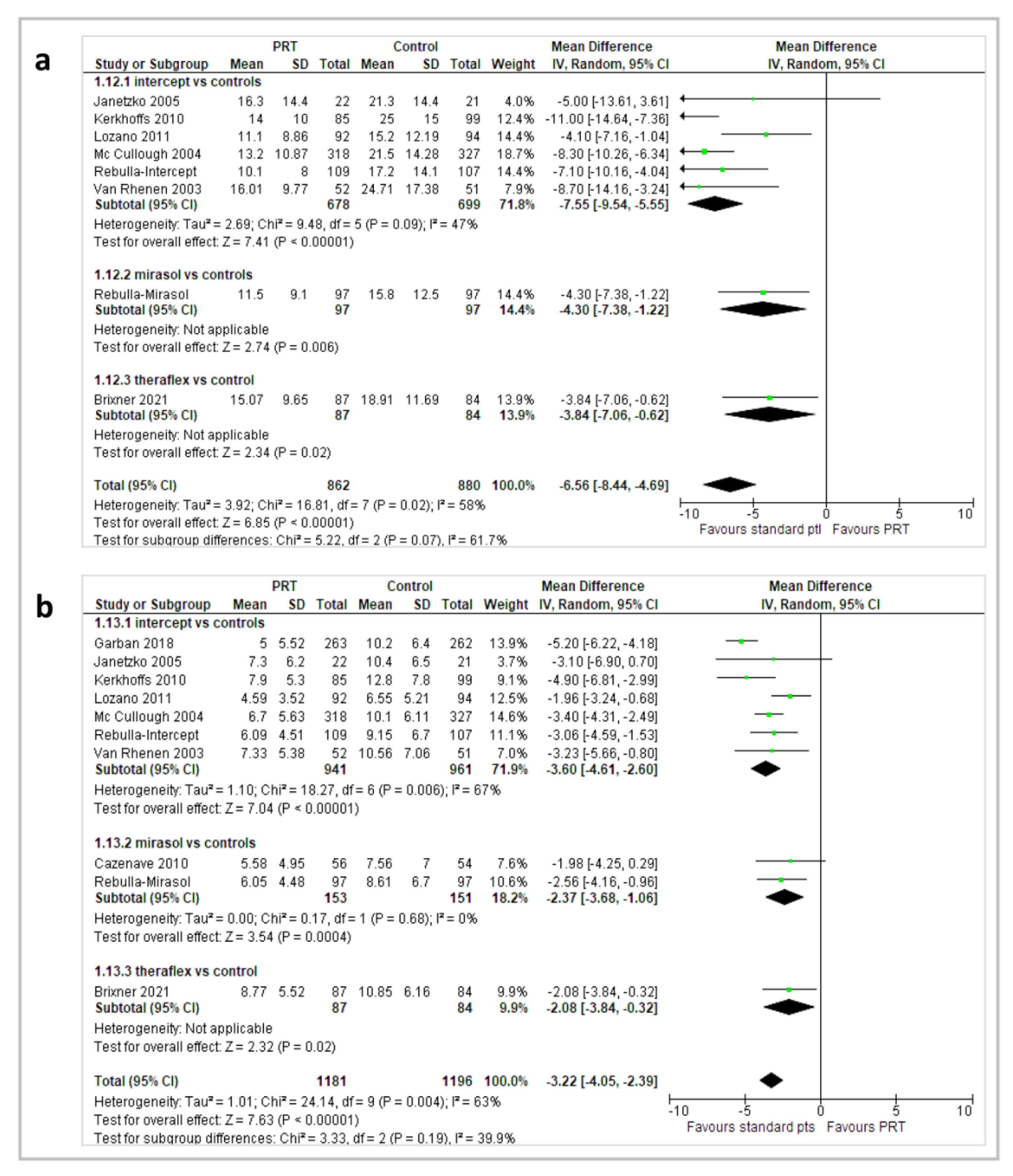
| 24 h CI | The mean 24 h CI ranged across St-PLT group from 15.8 to 25 | The mean 24 h CI score in PR group was from 3.84 to 11 lower | MD −6.65 (95% CIs, −8.44 to −4.86) | 1800 patients (9 trials, 7 with Intercept®, 1 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊝ moderate ^ | In the overall analysis and in subgroup analyses, participants who received PR-PLT transfusions had a lower 24 h CI. |
| 24 h CCI | The mean 24 h CCI ranged across St-PLT group from 7.5 to 12.8 | The mean 24 h CCI score in PR group was from 1.98 to 5.20 lower | MD −3.18 (95% CIs, −3.96 to −2.41) | 2435 patients (11 trials, 8 with Intercept®, 2 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊝ moderate ^ | In the overall analysis and in subgroup analyses, participants who received PR-PLT transfusions had a lower 24 h CCI. |
| Patients with refractoriness | ||||||
| No. of patients with PLT refractoriness | 55.6 per 1000 | 144 per 1000 (from 110 to 188) | RR 2.59 (95% CIs, 1.98/3.39) | 2389 patients (10 trials, 6 with Intercept®, 3 with Mirasol®, 1 with Theraflex® | ⊕⊕⊕⊕ high 1 | In the overall analysis and in the subgroup of Intercept® and Mirasol® trials, the no. of patients with PLT refractoriness was significantly higher in PR-PLT group compared to St-PLT. No statistically significant between-groups difference was observed in a single trial with Theraflex®. |
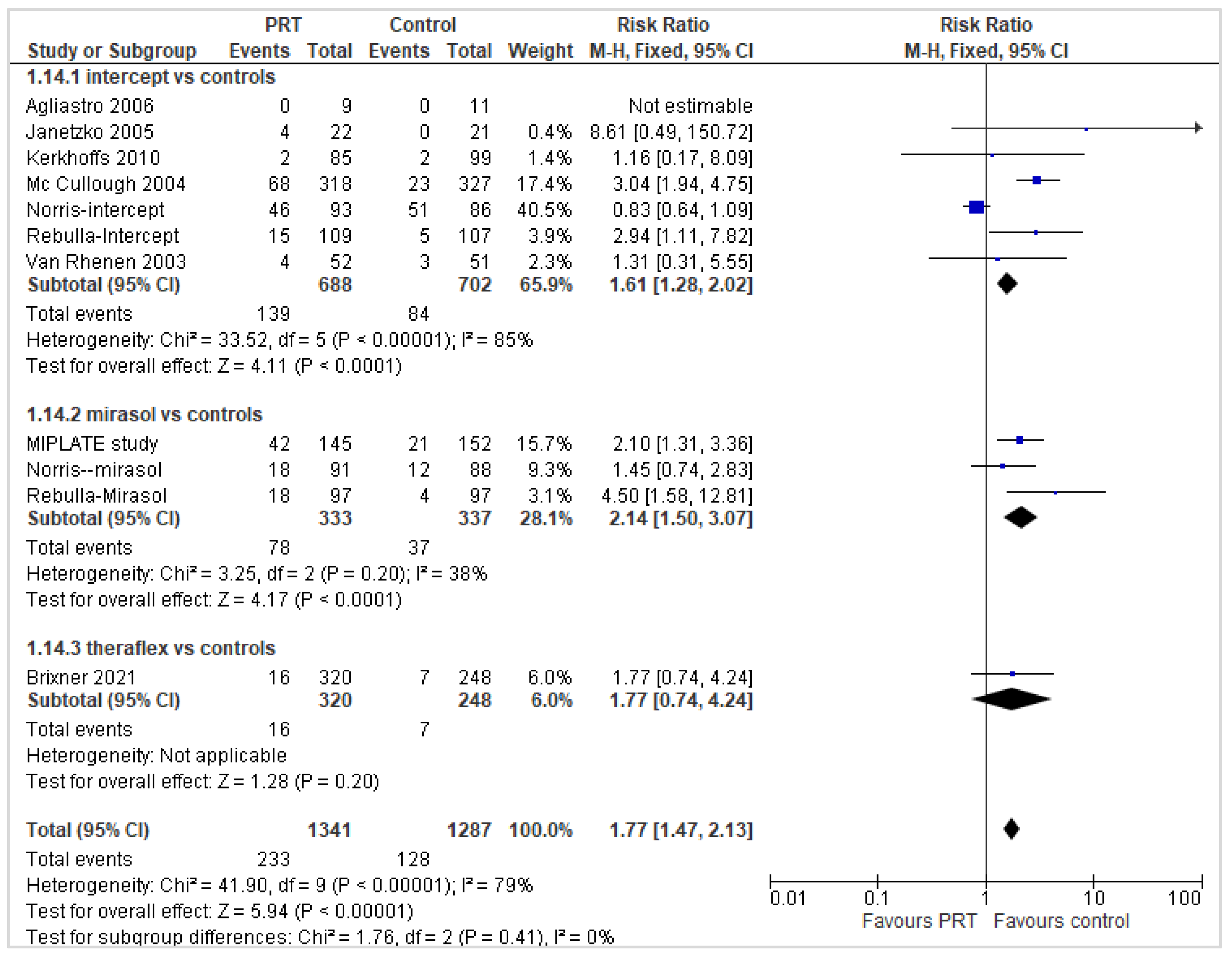
| No. of patients with PLT refractoriness and alloimmunization | 99.4 per 1000 | 175 per 1000 (from 146 to 211) | RR 1.77 (95% CIs, 1.47/2.13) | 2628 patients (11 trials, 7 with Intercept®, 3 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊕ high 1 | In the overall analysis and in the subgroup of Intercept® and Mirasol® trials, the no. of patients with PLT refractoriness and alloimmunization was significantly higher in PR-PLT group compared with St-PLT. No statistically significant between-groups difference was observed in a single trial with Theraflex®. |
| PLT and RBC transfusions | ||||||
| No. of PLT transfusions/participants | The mean no. of PLT. transfusions in St-PLT recipients ranged from 2.95 to 6.2 | The mean no. of PLT transfusions in PR-PLT recipients ranged from 3.68 to 8.4 | MD 1.04 (95% CIs, 0.84/1.24) | 2194 patients (9 trials, 6 with Intercept®, 2 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊕ high 1 | In the overall analysis and in subgroup analyses, PR-PLT recipients had a higher no. of PLT transfusions compared with St-PLT recipients. |
| No. of RBC transfusions/participants | The mean no. of PLT transfusions in St-PLT recipients ranged from 2.2 to 5.5 | The mean no. of PLT transfusions in PR-PLT recipients ranged from 2.85 to 5.5 | MD 0.32 (95% CIs, 0.14/0.50) | 2193 patients (9 trials, 6 with Intercept®, 2 with Mirasol®, 1 with Theraflex®) | ⊕⊕⊕⊕ high 1 | In the overall analysis and in subgroup analyses of Intercept® and Theraflex® trials, PR-PLT recipients had a higher no. of PLT transfusions compared with St-PLT recipients. No significant between-groups difference was observed in Mirasol® trials. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pati, I.; Masiello, F.; Pupella, S.; Cruciani, M.; De Angelis, V. Efficacy and Safety of Pathogen-Reduced Platelets Compared with Standard Apheresis Platelets: A Systematic Review of RCTs. Pathogens 2022, 11, 639. https://doi.org/10.3390/pathogens11060639
Pati I, Masiello F, Pupella S, Cruciani M, De Angelis V. Efficacy and Safety of Pathogen-Reduced Platelets Compared with Standard Apheresis Platelets: A Systematic Review of RCTs. Pathogens. 2022; 11(6):639. https://doi.org/10.3390/pathogens11060639
Chicago/Turabian StylePati, Ilaria, Francesca Masiello, Simonetta Pupella, Mario Cruciani, and Vincenzo De Angelis. 2022. "Efficacy and Safety of Pathogen-Reduced Platelets Compared with Standard Apheresis Platelets: A Systematic Review of RCTs" Pathogens 11, no. 6: 639. https://doi.org/10.3390/pathogens11060639