
The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Literature Search
2.2. Study Characteristics
2.3. TNF-α and COVID-19 Severity
2.4. TNF-α and COVID-19 Mortality
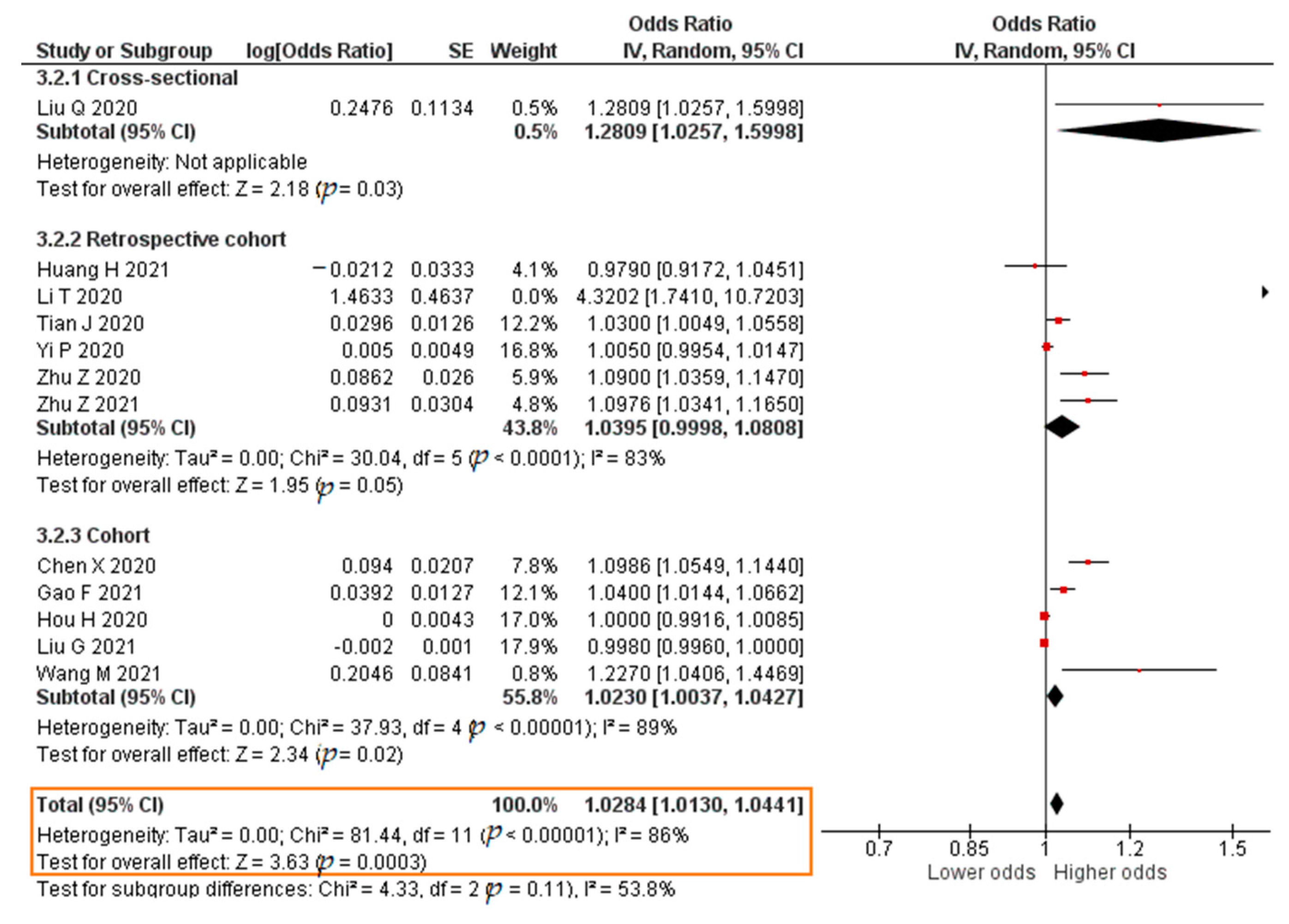
2.5. IL-6 and COVID-19 Severity
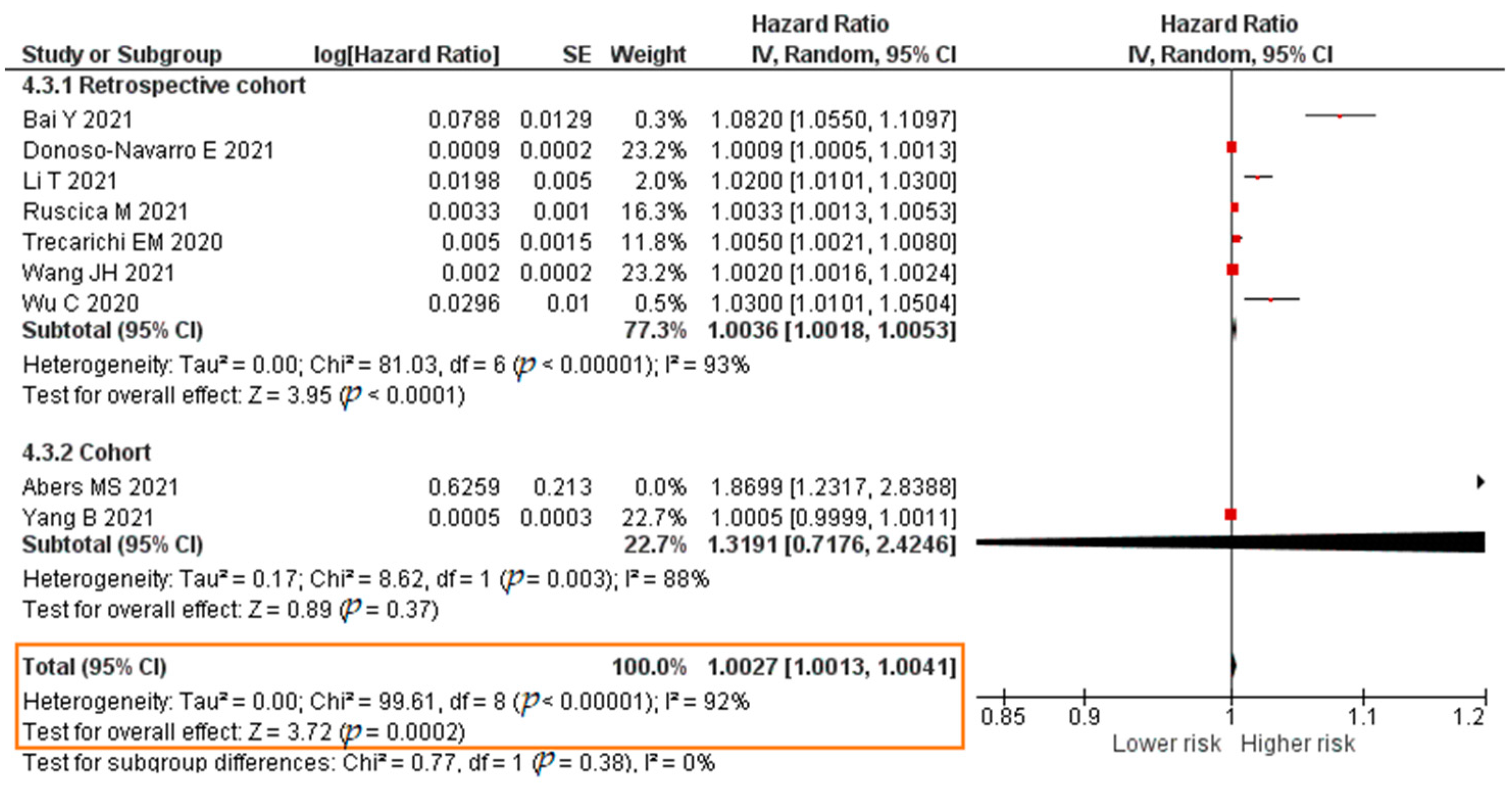
2.6. IL-6 and COVID-19 Mortality
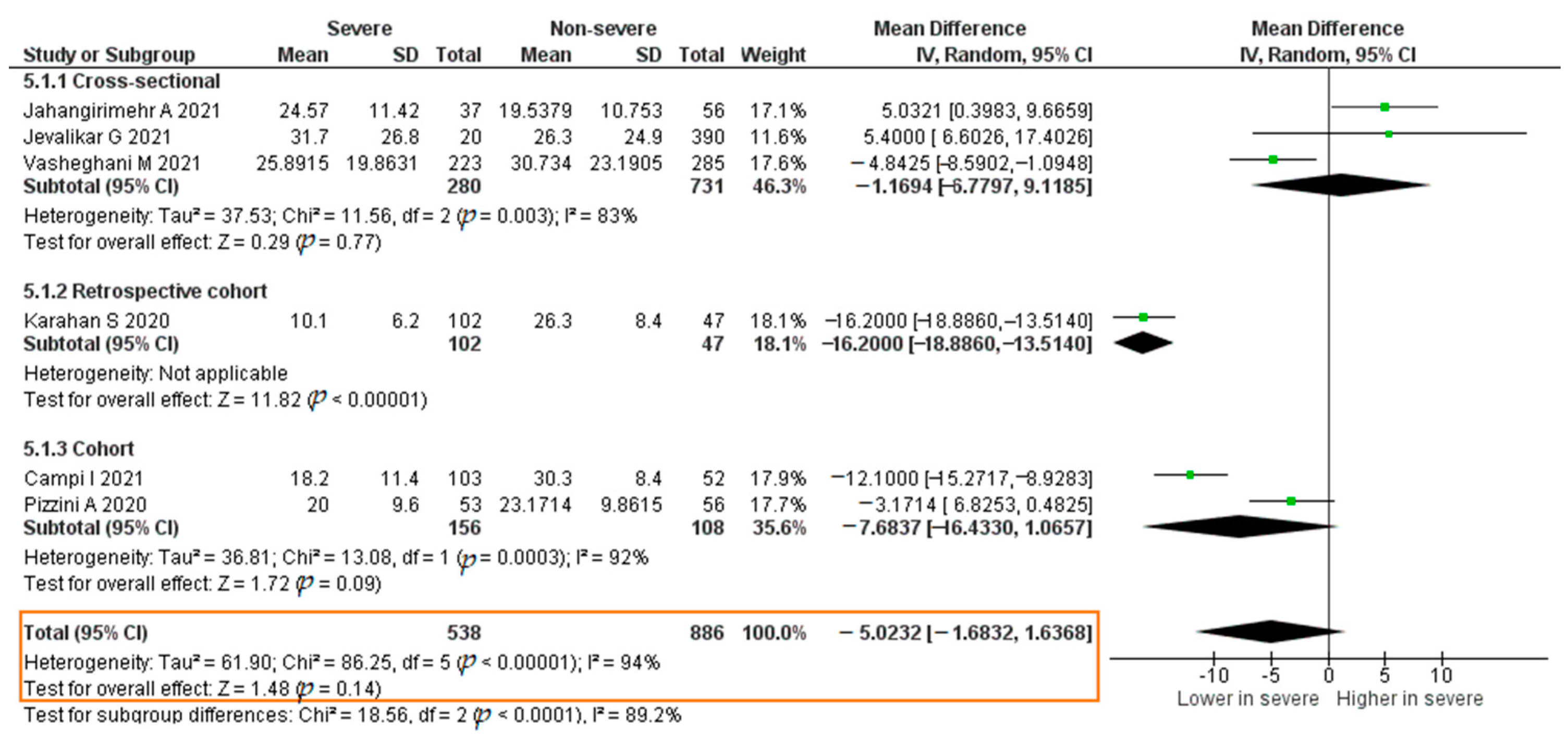
2.7. Vitamin D and COVID-19 Severity
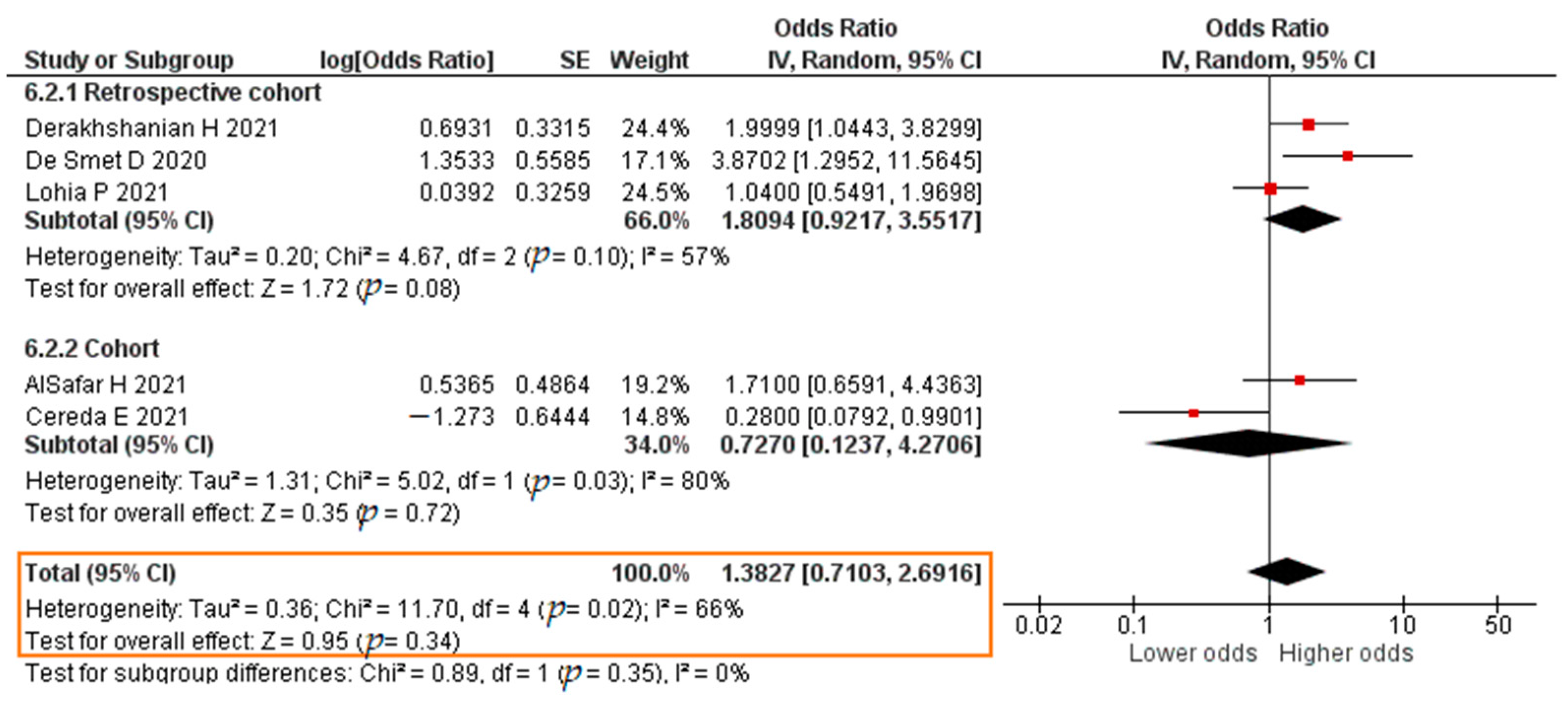
2.8. Vitamin D and COVID-19 Mortality
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 24 April 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Capstick, T.; Ahmed, R.; Kow, C.S.; Mazhar, F.; Merchant, H.A.; Zaidi, S.T.R. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: A systematic review and meta-analysis. Expert Rev. Respir. Med. 2020, 14, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: A global literature survey. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F.B.; Anderson, R.N. The Leading Causes of Death in the US for 2020. JAMA 2021, 325, 1829–1830. [Google Scholar] [CrossRef] [PubMed]
- Satuan Tugas Penanganan COVID-19 (COVID-19 Task Force). Peta Sebaran COVID-19 (COVID-19 Distribution Map). Available online: https://covid19.go.id/peta-sebaran-covid19 (accessed on 15 May 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 728–793. [Google Scholar] [CrossRef] [PubMed]
- Fara, A.; Mitrev, Z.; Rosalia, R.A.; Assas, B.M. Cytokine storm and COVID-19: A chronicle of pro-inflammatory cytokines. Open Biol. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Yang, L.; Liu, S.; Liu, J.; Zhang, Z.; Wan, X.; Huang, B.; Chen, Y.; Zhang, Y. COVID-19: Immunopathogenesis and Immunotherapeutics. Sig. Transduct. Target. Ther. 2020, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm. Regener. 2020, 40, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front. Immunol. 2020, 11, 1–13. [Google Scholar] [CrossRef]
- Bao, J.; Li, C.; Zhang, K.; Kang, H.; Chen, W.; Gu, B. Comparative analysis of laboratory indexes of severe and non-severe patients infected with COVID-19. Clin. Chim. Acta 2020, 509, 180–194. [Google Scholar] [CrossRef]
- Gao, Y.; Li, T.; Han, M.; Li, X.; Wu, D.; Xu, Y.; Zhu, Y.; Liu, Y.; Wang, X.; Wang, L. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J. Med. Virol. 2020, 92, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Wang, D.; Chen, C.; Lu, W.; Liu, H.; Lv, T.; Song, Y.; Zhang, F. PaO2/FiO2 and IL-6 are risk factors of mortality for intensive care COVID-19 patients. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.; Cheng, S.; Le, J.; Huang, J.; Feng, L.; Zhang, B.; Li, Y. Clinical characteristics and co-infections of 354 hospitalized patients with COVID-19 in Wuhan, China: A retrospective cohort study. Microbes Infect. 2020, 22, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Guo, P.; Zhang, L.; Wang, F. Serum Interleukin-6 Concentrations and the Severity of COVID-19 Pneumonia: A Retrospective Study at a Single Center in Bengbu City, Anhui Province, China, in January and February 2020. Med. Sci. Monit. 2020, 26, e926941. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.Y.; Wang, R.R.; Zhang, D.W.; Tu, Y.H.; Chen, C.S.; Ji, S.; Li, C.X.; Li, X.Y.; Zhou, M.X.; Cao, W.S.; et al. Risk factors for severe COVID-19: Evidence from 167 hospitalized patients in Anhui, China. J. Infect. 2020, 81, e89–e92. [Google Scholar] [CrossRef] [PubMed]
- Yi, P.; Yang, X.; Ding, C.; Chen, Y.; Xu, K.; Ni, Q.; Zhao, H.; Li, Y.; Zhang, X.; Liu, J.; et al. Risk factors and clinical features of deterioration in COVID-19 patients in Zhejiang, China: A single-centre, retrospective study. BMC Infect. Dis. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Yang, A.P.; Li, H.M.; Tao, W.Q.; Yang, X.J.; Wang, M.; Yang, W.J.; Liu, J.P. Infection with SARS-CoV-2 causes abnormal laboratory results of multiple organs in patients. Aging 2020, 12, 10059–10069. [Google Scholar] [CrossRef] [PubMed]
- Baktash, V.; Hosack, T.; Patel, N.; Shah, S.; Kandiah, P.; Van den Abbeele, K.; Mandal, A.K.J.; Missouris, C.G. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad. Med. J. 2021, 97, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.K.A.M.; Lima, L.A.; de Aquino, P.E.A.; de Sousa, J.A.C.; Gadelha, C.V.J.; Calou, I.B.F.; Lopes, M.J.P.; Lima, F.A.V.; Neves, K.R.T.; de Andrade, G.M.; et al. Vitamin D (VD3) antioxidative and anti-inflammatory activities: Peripheral and central effects. Eur. J. Pharmacol. 2020, 879, 1–12. [Google Scholar] [CrossRef]
- Miroliaee, A.E.; Salamzadeh, J.; Shokouhi, S.; Sahraei, Z. The study of vitamin D administration effect on CRP and Interleukin-6 as prognostic biomarkers of ventilator associated pneumonia. J. Crit. Care 2018, 44, 300–305. [Google Scholar] [CrossRef]
- Peterson, C.A.; Heffernan, M.E. Serum tumor necrosis factor-alpha concentrations are negatively correlated with serum 25(OH)D concentrations in healthy women. J. Inflamm. 2008, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cantorna, M.T.; Snyder, L.; Lin, Y.D.; Yang, L. Vitamin D and 1,25(OH)2D regulation of T cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef] [Green Version]
- Fisher, S.A.; Rahimzadeh, M.; Brierley, C.; Gration, B.; Doree, C.; Kimber, C.E.; Plaza Cajide, A.; Lamikanra, A.A.; Roberts, D.J. The role of vitamin D in increasing circulating T regulatory cell numbers and modulating T regulatory cell phenotypes in patients with inflammatory disease or in healthy volunteers: A systematic review. PLoS ONE 2019, 14, e0222313. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight 2021, 6, e144455. [Google Scholar] [CrossRef]
- Hou, H.; Zhang, B.; Huang, H.; Luo, Y.; Wu, S.; Tang, G.; Liu, W.; Mao, L.; Mao, L.; Wang, F.; et al. Using IL-2R/lymphocytes for predicting the clinical progression of patients with COVID-19. Clin. Exp. Immunol. 2020, 201, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Jiang, X.; Zeng, X.; Pan, Y.; Xu, H. Analysis of Lymphocyte Subpopulations and Cytokines in COVID-19-Associated Pneumonia and Community-Acquired Pneumonia. J. Immunol. Res. 2021, 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Yuan, X.; Xiao, J.; Zhong, Q.; Yang, C.; Liu, B.; Cai, Y.; Lu, Z.; Wang, J.; Wang, Y.; et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: A multicentre, retrospective, cohort study. Lancet Oncol. 2020, 21, 893–903. [Google Scholar] [CrossRef]
- Wang, J.H.; Chen, R.D.; Yang, H.K.; Zeng, L.C.; Chen, H.; Hou, Y.Y.; Hu, W.; Yu, J.S.; Li, H. Inflammation-associated factors for predicting in-hospital mortality in patients with COVID-19. J. Med. Virol. 2021, 93, 2908–2917. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Fan, Y.; Chai, Y.; Cheng, W.; Wang, K.; Cao, J.; Hu, X. Association of Clinical and Immunological Characteristics With Disease Severity and Outcomes in 211 Patients With COVID-19 in Wuhan, China. Front. Cell Infect. Microbiol. 2021, 11, 667487:1–667487:21. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Yunis, J.; Yao, Y.; Shi, J.; Yang, Y.; Zhou, P.; Liang, K.; Wan, Y.; Mehdi, A.; Chen, Z.; et al. High levels of soluble CD25 in COVID-19 severity suggest a divergence between anti-viral and pro-inflammatory T-cell responses. Clin. Transl. Immunol. 2021, 10, e1251. [Google Scholar] [CrossRef]
- Yang, B.; Chang, X.; Huang, J.; Pan, W.; Si, Z.; Zhang, C.; Li, H. The role of IL-6/lymphocyte ratio in the peripheral blood of severe patients with COVID-19. Int. Immunopharmacol. 2021, 97, 1–8. [Google Scholar] [CrossRef]
- Zhu, Z.; Cai, T.; Fan, L.; Lou, K.; Hua, X.; Huang, Z.; Gao, G. Clinical value of immune-inflammatory parameters to assess the severity of coronavirus disease 2019. Int. J. Infect. Dis. 2020, 95, 332–339. [Google Scholar] [CrossRef]
- Avila-Nava, A.; Cortes-Telles, A.; Torres-Erazo, D.; López-Romero, S.; Chim Aké, R.; Gutiérrez Solis, A.L. Serum IL-6: A potential biomarker of mortality among SARS-CoV-2 infected patients in Mexico. Cytokine 2021, 143, 1–6. [Google Scholar] [CrossRef]
- Bai, Y.; Wang, E.; Zhao, S.; Li, J.; Zhu, Y.; Zhang, Y.; Cao, L.; Liu, H.; Dong, Y.; Wang, F.; et al. Implications of Laboratory Tests in Disease Grading and Death Risk Stratification of COVID-19: A Retrospective Study in Wuhan, China. Front. Med. (Lausanne) 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Bhadade, R.; Harde, M.; deSouza, R.; Kasbe, A.; Deshpande, C.; Dave, S.; Joshi, M.; Bharmal, R.; Madke, T. Appraisal of Critically Ill COVID-19 Patients at a Dedicated COVID Hospital. J. Assoc. Physicians India 2020, 68, 14–19. [Google Scholar] [PubMed]
- Chen, C.; Zhang, J.; Li, C.; Hu, Z.; Zhang, M.; Tu, P.; Liu, L.; Zong, W. The characteristics and death risk factors of 132 COVID-19 pneumonia patients with comorbidities: A retrospective single center analysis in Wuhan, China. medRxiv 2021. [Google Scholar] [CrossRef]
- Chen, H.; Chen, R.; Yang, H.; Wang, J.; Hou, Y.; Hu, W.; Yu, J.; Li, H. Development and validation of a nomogram using on admission routine laboratory parameters to predict in-hospital survival of patients with COVID-19. J. Med. Virol. 2021, 93, 2332–2339. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Huang, J.; Huang, Y.; Chen, J.; Huang, Y.; Jiang, X.; Shi, Y. Characteristics of immune cells and cytokines in patients with coronavirus disease 2019 in Guangzhou, China. Hum. Immunol. 2020, 81, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Donoso-Navarro, E.; Arribas Gómez, I.; Bernabeu-Andreu, F.A. IL-6 and Other Biomarkers associated with Poor Prognosis in a Cohort of Hospitalized Patients with COVID-19 in Madrid. Biomark. Insights 2021, 16, 1–8. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Yan, H.D.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Association and Interaction Between Serum Interleukin-6 Levels and Metabolic Dysfunction-Associated Fatty Liver Disease in Patients With Severe Coronavirus Disease 2019. Front. Endocrinol. 2021, 12, 1–9. [Google Scholar] [CrossRef]
- Gou, L.; Xiang, M.; Ran, X.; Wang, F.; Zhang, S.; Li, S.; Dong, K.; Chen, X.; Huang, Y.; Meng, C.; et al. Hyperosmolarity Deserves More Attention in Critically Ill COVID-19 Patients with Diabetes: A Cohort-Based Study. Diabetes Metab. Syndr. 2021, 14, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Song, B.; Xu, Z.; Jiao, Y.; Huang, L.; Zhao, P.; Huang, J.; Zhou, Z.; Zhao, Z.; Tian, J.; et al. Predictors of Coronavirus Disease 2019 Severity: A Retrospective Study of 64 Cases. Jpn J. Infect. Dis. 2021, 74, 54–60. [Google Scholar] [CrossRef]
- Laguna-Goya, R.; Utrero-Rico, A.; Talayero, P.; Lasa-Lazaro, M.; Ramirez-Fernandez, A.; Naranjo, L.; Segura-Tudela, A.; Cabrera-Marante, O.; Rodriguez de Frias, E.; Garcia-Garcia, R.; et al. IL-6-based mortality risk model for hospitalized patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 799–807. [Google Scholar] [CrossRef]
- Lavillegrand, J.R.; Garnier, M.; Spaeth, A.; Mario, N.; Hariri, G.; Pilon, A.; Berti, E.; Fieux, F.; Thietart, S.; Urbina, T.; et al. Elevated plasma IL-6 and CRP levels are associated with adverse clinical outcomes and death in critically ill SARS-CoV-2 patients: Inflammatory response of SARS-CoV-2 patients. Ann. Intensive Care 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Li, T.; Lu, L.; Zhang, W.; Tao, Y.; Wang, L.; Bao, J.; Liu, B.; Duan, J. Clinical characteristics of 312 hospitalized older patients with COVID-19 in Wuhan, China. Arc. Gerontol. Geriatr. 2020, 91, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wang, X.; Zhuang, X.; Wang, H.; Li, A.; Huang, L.; Zhang, X.; Xue, Y.; Wei, F.; Ma, C. Baseline characteristics and changes of biomarkers in disease course predict prognosis of patients with COVID-19. Intern. Emerg. Med. 2021, 16, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Dai, Y.; Feng, M.; Wang, X.; Liang, W.; Yang, F. Associations between serum amyloid A, interleukin-6, and COVID-19: A cross-sectional study. J. Clin. Lab. Anal. 2020, 34, e23527. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.Q.; Cheng, A.; Wang, Y.; Li, H.; Hu, L.; Zhao, X.; Wang, T.; He, F. Cytokines and their relationship with the severity and prognosis of coronavirus disease 2019 (COVID-19): A retrospective cohort study. BMJ Open 2020, 10, e041471. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Obata, R.; Rizk, D.; Kuno, T. The association of interleukin-6 value, interleukin inhibitors, and outcomes of patients with COVID-19 in New York City. J. Med. Virol. 2021, 93, 463–471. [Google Scholar] [CrossRef]
- Martinez-Urbistondo, M.; Mora-Vargas, A.; Expósito-Palomo, E.; Castejón, R.; Citores, M.J.; Rosado, S.; de Mendoza, C.; Baños, I.; Fernández-Cruz, A.; Daimiel, L.; et al. Inflammatory-Related Clinical and Metabolic Outcomes in COVID-19 Patients. Mediat. Inflamm. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Ruscica, M.; Macchi, C.; Iodice, S.; Tersalvi, G.; Rota, I.; Ghidini, S.; Terranova, L.; Valenti, L.; Amati, F.; Aliberti, S.; et al. Prognostic parameters of in-hospital mortality in COVID-19 patients-An Italian experience. Eur. J. Clin. Investig. 2021, 51, e13629. [Google Scholar] [CrossRef]
- Sai, F.; Liu, X.; Li, L.; Ye, Y.; Zhu, C.; Hang, Y.; Huang, C.; Tian, L.; Huang, H.; Xu, X. Clinical characteristics and risk factors for mortality in patients with coronavirus disease 2019 in intensive care unit: A single- center, retrospective, observational study in China. Ann. Palliat Med. 2021, 10, 2859–2868. [Google Scholar] [CrossRef]
- Trecarichi, E.M.; Mazzitelli, M.; Serapide, F.; Pelle, M.C.; Tassone, B.; Arrighi, E.; Perri, G.; Fusco, P.; Scaglione, V.; Davoli, C.; et al. Clinical characteristics and predictors of mortality associated with COVID-19 in elderly patients from a long-term care facility. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, F.; Wang, C.; Wu, J.; Liu, J.; Chen, X.; Xiao, H.; Liu, Z.; Wu, Z.; Lu, X.; et al. Children Hospitalized with Severe COVID-19 in Wuhan. Pediatr. Infect. Dis. J. 2020, 39, e91–e94. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, C.; Bai, Y.; Wang, C.; Zhong, Y.; Lu, N.; Tian, L.; Cai, F.; Jin, R. Risk factors related to the severity of COVID-19 in Wuhan. Int. J. Med. Sci. 2021, 18, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhu, Z.; Yang, Y.; Fan, L.; Ye, S.; Lou, K.; Hua, X.; Huang, Z.; Shi, Q.; Gao, G. Low serum level of apolipoprotein A1 may predict the severity of COVID-19: A retrospective study. J. Clin. Lab. Anal. 2021, 35, e23911. [Google Scholar] [CrossRef] [PubMed]
- AlSafar, H.; Grant, W.B.; Hijazi, R.; Uddin, M.; Alkaabi, N.; Tay, G.; Mahboub, B.; Al Anouti, F. COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents. Nutrients 2021, 13, 1714. [Google Scholar] [CrossRef]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 1–13. [Google Scholar] [CrossRef]
- Cereda, E.; Bogliolo, L.; Klersy, C.; Lobascio, F.; Masi, S.; Crotti, S.; De Stefano, L.; Bruno, R.; Corsico, A.G.; Di Sabatino, A.; et al. Vitamin D 25OH deficiency in COVID-19 patients admitted to a tertiary referral hospital. Clin. Nutr. 2021, 40, 2469–2472. [Google Scholar] [CrossRef]
- De Smet, D.; De Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated with COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2021, 155, 381–388. [Google Scholar] [CrossRef]
- Derakhshanian, H.; Rastad, H.; Ghosh, S.; Zeinali, M.; Ziaee, M.; Khoeini, T.; Farrokhpour, M.; Qorbani, M.; Ramezani Ghamsari, M.; Hasani, H.; et al. The predictive power of serum vitamin D for poor outcomes in COVID-19 patients. Food Sci. Nutr. 2021, 9, 6307–6313. [Google Scholar] [CrossRef]
- Jahangirimehr, A.; Khalighi, A.; Shahvali, E.A.; Labibzadeh, M.; Bahmanyari, N. Evaluating the Relationship Between Disease Severity and Serum Levels of Zinc, Calcium and Vitamin D in COVID-19 Patients. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Jevalikar, G.; Mithal, A.; Singh, A.; Sharma, R.; Farooqui, K.J.; Mahendru, S.; Dewan, A.; Budhiraja, S. Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Karahan, S.; Katkat, F. Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey. J. Nutr. Health Aging 2021, 25, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lohia, P.; Nguyen, P.; Patel, N.; Kapur, S. Exploring the link between vitamin D and clinical outcomes in COVID-19. Am. J. Physiol. Endocrinol. Metab. 2021, 320, E520–E526. [Google Scholar] [CrossRef]
- Pizzini, A.; Aichner, M.; Sahanic, S.; Böhm, A.; Egger, A.; Hoermann, G.; Kurz, K.; Widmann, G.; Bellmann-Weiler, R.; Weiss, G.; et al. Impact of Vitamin D Deficiency on COVID-19-A Prospective Analysis from the CovILD Registry. Nutrients 2020, 12, 2775. [Google Scholar] [CrossRef]
- Vasheghani, M.; Jannati, N.; Baghaei, P.; Rezaei, M.; Marjani, M. The Association of 25 (OH) Vitamin D Levels and Severity and Outcome of COVID-19: A Cross-sectional Study. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Kennel, K.A.; Drake, M.T.; Hurley, D.L. Vitamin D deficiency in adults: When to test and how to treat. Mayo Clin. Proc. 2010, 85, 752–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalliolias, G.D.; Ivashkiv, L.B. TNF biology, pathogenic mechanisms and emerging therapeutic strategies. Nat. Rev. Rheumatol. 2016, 12, 49–62. [Google Scholar] [CrossRef]
- Abbas, A.K.; Lichtman, A.H.; Pillai, S. Cellular and Molecular Immunology, 9th ed.; Elsevier: Philadelphia, PA, USA, 2018; ISBN 978-0-323-47978-3. [Google Scholar]
- Merza, M.Y.; Hwaiz, R.A.; Hamad, B.K.; Mohammad, K.A.; Hama, H.A.; Karim, A.Y. Analysis of cytokines in SARS-CoV-2 or COVID-19 patients in Erbil city, Kurdistan Region of Iraq. PLoS ONE 2021, 16, e0250330:1–e0250330:7. [Google Scholar] [CrossRef]
- Mulchandani, R.; Lyngdoh, T.; Kakkar, A.K. Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13429. [Google Scholar] [CrossRef]
- Huang, W.; Li, M.; Luo, G.; Wu, X.; Su, B.; Zhao, L.; Zhang, S.; Chen, X.; Jia, M.; Zhu, J.; et al. The Inflammatory Factors Associated with Disease Severity to Predict COVID-19 Progression. J. Immunol. 2021, 206, 1597–1608. [Google Scholar] [CrossRef]
- Gan, J.; Li, J.; Li, S.; Yang, C. Leucocyte Subsets Effectively Predict the Clinical Outcome of Patients with COVID-19 Pneumonia: A Retrospective Case-Control Study. Front. Public Health 2020, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Li, Z.; Yang, B.; Jin, M.; Sun, Y.; He, Y.; Liu, Y.; Wang, Y.; Si, D.; Ma, P.; et al. Peripheral Inflammatory Cytokines and Lymphocyte Subset Features of Deceased COVID-19 Patients. BioMed Res. Int. 2021, 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ke, C.; Yu, C.; Yue, D.; Zeng, X.; Hu, Z.; Yang, C. Clinical characteristics of confirmed and clinically diagnosed patients with 2019 novel coronavirus pneumonia: A single-center, retrospective, case-control study. Med. Clin. 2020, 155, 327–334. [Google Scholar] [CrossRef]
- Baran, P.; Hansen, S.; Waetzig, G.H.; Akbarzadeh, M.; Lamertz, L.; Huber, H.J.; Ahmadian, M.R.; Moll, J.M.; Scheller, J. The balance of interleukin (IL)-6, IL-6·soluble IL-6 receptor (sIL-6R), and IL-6·sIL-6R·sgp130 complexes allows simultaneous classic and trans-signaling. J. Biol. Chem. 2018, 293, 6762–6775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, P.; Zhu, J.; Zhong, Z.; Li, H.; Pang, J.; Li, B.; Zhang, J. Association of elevated inflammatory markers and severe COVID-19. Medicine 2020, 99, e23315. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, C.; Kang, K.; Peng, Y.; Luo, Y.; Liu, H.; Yang, W.; Zhao, M.; Yu, K. Cytokine Storm May Not Be the Chief Culprit for the Deterioration of COVID-19. Viral Immunol. 2021, 34, 336–341. [Google Scholar] [CrossRef]
- Guirao, J.J.; Cabrera, C.M.; Jiménez, N.; Rincon, L.; Urra, J.M. High serum IL-6 values increase the risk of mortality and the severity of pneumonia in patients diagnosed with COVID-19. Mol. Immunol. 2020, 128, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Li, Y.; Sun, J.; Pan, H.; Yao, F.; Jiao, X. Selection of an Optimal Combination Panel to Better Triage COVID-19 Hospitalized Patients. J. Inflamm. Res. 2020, 13, 773–787. [Google Scholar] [CrossRef]
- Tang, J.; Lin, J.; Zhang, E.; Zhong, M.; Luo, Y.; Fu, Y.; Yang, Y. Serum IL-6 and procalcitonin are two promising novel biomarkers for evaluating the severity of COVID-19 patients. Medicine 2021, 100, e26131. [Google Scholar] [CrossRef]
- Wang, F.; Hou, H.; Luo, Y.; Tang, G.; Wu, S.; Huang, M.; Liu, W.; Zhu, Y.; Lin, Q.; Mao, L.; et al. The laboratory tests and host immunity of COVID-19 patients with different severity of illness. JCI Insight 2020, 5, e137799:1–e137799:12. [Google Scholar] [CrossRef]
- Yin, S.W.; Zhou, Z.; Wang, J.L.; Deng, Y.F.; Jing, H.; Qiu, Y. Viral loads, lymphocyte subsets and cytokines in asymptomatic, mildly and critical symptomatic patients with SARS-CoV-2 infection: A retrospective study. Virol. J. 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Al Balushi, A.; AlShekaili, J.; Al Kindi, M.; Ansari, Z.; Al-Khabori, M.; Khamis, F.; Ambusaidi, Z.; Al Balushi, A.; Al Huraizi, A.; Al Sulaimi, S.; et al. Immunological predictors of disease severity in patients with COVID-19. Int. J. Infect. Dis. 2021, 110, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Belletti, A.; Campochiaro, C.; Marmiere, M.; Likhvantsev, V.; Yavorovskiy, A.; Dagna, L.; Landoni, G.; Zangrillo, A.; Hajjar, L.A. Efficacy and safety of IL-6 inhibitors in patients with COVID-19 pneumonia: A systematic review and meta-analysis of multicentre, randomized trials. Ann. Intensive Care 2021, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Mohan, M.; Cherian, J.J.; Sharma, A. Exploring links between vitamin D deficiency and COVID-19. PLoS Pathog 2020, 16, e1008874. [Google Scholar] [CrossRef]
- Kazemi, A.; Mohammadi, V.; Aghababaee, S.K.; Golzarand, M.; Clark, C.C.T.; Babajafari, S. Association of Vitamin D Status with SARS-CoV-2 Infection or COVID-19 Severity: A Systematic Review and Meta-analysis. Adv. Nutr. 2021, 12, 1636–1658. [Google Scholar] [CrossRef] [PubMed]
- Ye, K.; Tang, F.; Liao, X.; Shaw, B.A.; Deng, M.; Huang, G.; Qin, Z.; Peng, X.; Xiao, H.; Chen, C.; et al. Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity? A Case-Control Study. J. Am. Coll Nutr. 2021, 40, 724–731. [Google Scholar] [CrossRef]
- Ersöz, A.; Yılmaz, T.E. The association between micronutrient and hemogram values and prognostic factors in COVID-19 patients: A single-center experience from Turkey. Int. J. Clin. Pract. 2021, 75, e14078. [Google Scholar] [CrossRef]
- Abrishami, A.; Dalili, N.; Mohammadi Torbati, P.; Asgari, R.; Arab-Ahmadi, M.; Behnam, B.; Sanei-Taheri, M. Possible association of vitamin D status with lung involvement and outcome in patients with COVID-19: A retrospective study. Eur. J. Nutri. 2021, 60, 2249–2257. [Google Scholar] [CrossRef]
- Bennouar, S.; Cherif, A.B.; Kessira, A.; Bennouar, D.E.; Abdi, S. Vitamin D Deficiency and Low Serum Calcium as Predictors of Poor Prognosis in Patients with Severe COVID-19. J. Am. Coll. Nutr. 2021, 40, 104–110. [Google Scholar] [CrossRef]
- Diaz-Curiel, M.; Cabello, A.; Arboiro-Pinel, R.; Mansur, J.L.; Heili-Frades, S.; Mahillo-Fernandez, I.; Herrero-González, A.; Andrade-Poveda, M. The relationship between 25(OH) vitamin D levels and COVID-19 onset and disease course in Spanish patients. J. Steroid Biochem. Mol. Biol. 2021, 212, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 June 2021).
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis, 1st ed.; John Wiley & Sons Ltd.: West Sussex, UK, 2009; ISBN 978-0-470-05724-7. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2. Available online: www.training.cochrane.org/handbook (accessed on 18 November 2021).

















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. https://doi.org/10.3390/pathogens11020195
Halim C, Mirza AF, Sari MI. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens. 2022; 11(2):195. https://doi.org/10.3390/pathogens11020195
Chicago/Turabian StyleHalim, Ceria, Audrey Fabianisa Mirza, and Mutiara Indah Sari. 2022. "The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis" Pathogens 11, no. 2: 195. https://doi.org/10.3390/pathogens11020195