
The Clinical Trial Outcomes of Cranberry, D-Mannose and NSAIDs in the Prevention or Management of Uncomplicated Urinary Tract Infections in Women: A Systematic Review
Abstract
:1. Introduction
2. Results and Discussion
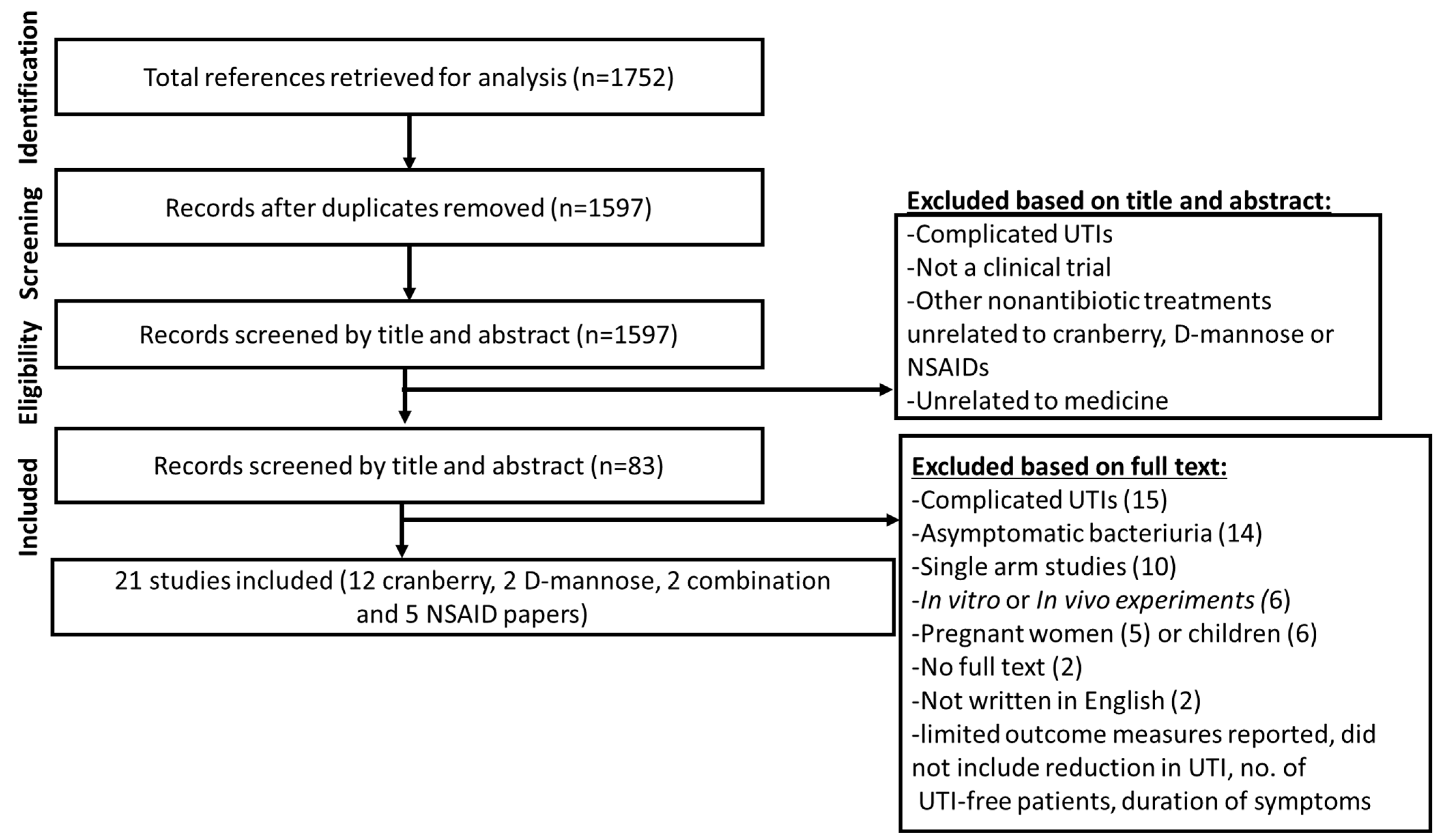
2.1. Search Results
2.2. Clinical Trial Designs
2.3. Interventions, Active Ingredients and Comparisons
2.4. Effectiveness of Nonantibiotic Agents in Preventing UTI
2.5. Side Effects
2.6. Limitations of Clinical Trial Data
2.7. Limitations of This Review
3. Conclusions
4. Materials and Methods
4.1. Search Strategy
4.2. Inclusion and Exclusion Criteria
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Paul, R. State of the globe: Rising antimicrobial resistance of pathogens in urinary tract infection. J. Glob. Infect. Dis. 2018, 10, 117–118. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 91: Treatment of urinary tract infections in nonpregnant women. Obstet. Gynecol. 2008, 111, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Rahn, D. Urinary tract infections: Contemporary management. Urol. Nurs. 2008, 28, 333–341. [Google Scholar] [PubMed]
- Al-Shaikh, G.; Syed, S.; Osman, S.; Bogis, A.; Al-Badr, A. Pessary use in stress urinary incontinence: A review of advantages, complications, patient satisfaction, and quality of life. Int. J. Womens Health 2018, 10, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Jung, C.; Brubaker, L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric 2019, 22, 242–249. [Google Scholar] [CrossRef]
- Hooton, T.M.; Scholes, D.; Hughes, J.P.; Winter, C.; Roberts, P.L.; Stapleton, A.E.; Stergachis, A.; Stamm, W.E. A prospective study of risk factors for symptomatic urinary tract infection in young women. N. Engl. J. Med. 1996, 335, 468–474. [Google Scholar] [CrossRef]
- Hu, K.K.; Boyko, E.J.; Scholes, D.; Normand, E.; Chen, C.L.; Grafton, J.; Fihn, S.D. Risk factors for urinary tract infections in postmenopausal women. Arch. Intern. Med. 2004, 164, 989–993. [Google Scholar] [CrossRef] [Green Version]
- Storme, O.; Tiran Saucedo, J.; Garcia-Mora, A.; Dehesa-Davila, M.; Naber, K.G. Risk factors and predisposing conditions for urinary tract infection. Ther. Adv. Urol. 2019, 11, 1756287218814382. [Google Scholar] [CrossRef]
- Ejrnaes, K. Bacterial characteristics of importance for recurrent urinary tract infections caused by Escherichia coli. Dan. Med. Bull. 2011, 58, B4187. [Google Scholar]
- Hannan, T.J.; Totsika, M.; Mansfield, K.J.; Moore, K.H.; Schembri, M.A.; Hultgren, S.J. Host-pathogen checkpoints and population bottlenecks in persistent and intracellular uropathogenic Escherichia coli bladder infection. FEMS Microbiol. Rev. 2012, 36, 616–648. [Google Scholar] [CrossRef] [Green Version]
- Justice, S.S.; Hunstad, D.A.; Seed, P.C.; Hultgren, S.J. Filamentation by Escherichia coli subverts innate defenses during urinary tract infection. Proc. Natl. Acad. Sci. USA 2006, 103, 19884–19889. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.A.; Hooton, T.M.; Stamm, W.E.; Humphrey, P.A.; Hultgren, S.J. Detection of intracellular bacterial communities in human urinary tract infection. PLoS Med. 2007, 4, e329. [Google Scholar] [CrossRef] [PubMed]
- Robino, L.; Scavone, P.; Araujo, L.; Algorta, G.; Zunino, P.; Vignoli, R. Detection of intracellular bacterial communities in a child with Escherichia coli recurrent urinary tract infections. Pathog. Dis. 2013, 68, 78–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robino, L.; Scavone, P.; Araujo, L.; Algorta, G.; Zunino, P.; Pirez, M.C.; Vignoli, R. Intracellular bacteria in the pathogenesis of Escherichia coli urinary tract infection in children. Clin. Infect. Dis. 2014, 59, e158–e164. [Google Scholar] [CrossRef] [Green Version]
- Horsley, H.; Malone-Lee, J.; Holland, D.; Tuz, M.; Hibbert, A.; Kelsey, M.; Kupelian, A.; Rohn, J.L. Enterococcus faecalis subverts and invades the host urothelium in patients with chronic urinary tract infection. PLoS ONE 2013, 8, e83637. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Chen, Z.; Gawthorne, J.A.; Mukerjee, C.; Varettas, K.; Mansfield, K.J.; Schembri, M.A.; Moore, K.H. Detection of intracellular bacteria in exfoliated urothelial cells from women with urge incontinence. Pathog. Dis. 2016, 74, ftw067. [Google Scholar] [CrossRef]
- O’Brien, V.P.; Hannan, T.J.; Nielsen, H.V.; Hultgren, S.J. Drug and Vaccine Development for the Treatment and Prevention of Urinary Tract Infections. Urin. Tract Infect. Mol. Pathog. Clin. Manag. 2017, 4, 589–646. [Google Scholar] [CrossRef] [Green Version]
- Mortazavi-Tabatabaei, S.A.R.; Ghaderkhani, J.; Nazari, A.; Sayehmiri, K.; Sayehmiri, F.; Pakzad, I. Pattern of Antibacterial Resistance in Urinary Tract Infections: A Systematic Review and Meta-analysis. Int. J. Prev. Med. 2019, 10, 169. [Google Scholar] [CrossRef]
- OUTBREAK Consortium. A One Health Antimicrobial Resistance Economic Perspective; UTS: Sydney, Australia, 2020. Available online: https://outbreakproject.com.au/wp-content/uploads/2020/12/OUTBREAK_REPORT_2020_economics_ERRATUM.pdf (accessed on 22 March 2022).
- Blango, M.G.; Mulvey, M.A. Persistence of uropathogenic Escherichia coli in the face of multiple antibiotics. Antimicrob. Agents Chemother 2010, 54, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Safety and Quality in Health Care. Antimicrobial Stewardship in Australian Health Care Sydney, NSW: ACSQHC. 2018. Available online: https://www.safetyandquality.gov.au/sites/default/files/2022-09/Antimicrobial-stewardship-in-Australian-health-care.pdf (accessed on 1 February 2022).
- Barea, B.M.; Veeratterapillay, R.; Harding, C. Nonantibiotic treatments for urinary cystitis: An update. Curr. Opin. Urol. 2020, 30, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Guay, D.R. Cranberry and urinary tract infections. Drugs 2009, 69, 775–807. [Google Scholar] [CrossRef]
- Jepson, R.G.; Craig, J.C. A systematic review of the evidence for cranberries and blueberries in UTI prevention. Mol. Nutr. Food Res. 2007, 51, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Foo, L.Y.; Lu, Y.; Howell, A.B.; Vorsa, N. A-Type proanthocyanidin trimers from cranberry that inhibit adherence of uropathogenic P-fimbriated Escherichia coli. J. Nat. Prod. 2000, 63, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, A.J.; Chmiel, J.S.; Duncan, J.L.; Falkowski, W.S. Mannose-sensitive adherence of Escherichia coli to epithelial cells from women with recurrent urinary tract infections. J. Urol. 1984, 131, 906–910. [Google Scholar] [CrossRef]
- Michaels, E.K.; Chmiel, J.S.; Plotkin, B.J.; Schaeffer, A.J. Effect of D-mannose and D-glucose on Escherichia coli bacteriuria in rats. Urol. Res. 1983, 11, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.A.; Hausladen, D.A.; Yoon, J.H.; Weiss, R.M. Prostaglandin E2 production and cyclooxygenase-2 induction in human urinary tract infections and bladder cancer. J. Urol. 2002, 168, 1568–1573. [Google Scholar] [CrossRef]
- Takagi-Matsumoto, H.; Ng, B.; Tsukimi, Y.; Tajimi, M. Effects of NSAIDs on bladder function in normal and cystitis rats: A comparison study of aspirin, indomethacin, and ketoprofen. J. Pharmacol. Sci. 2004, 95, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Whiteside, S.A.; Dave, S.; Reid, G.; Burton, J.P. Ibuprofen lacks direct antimicrobial properties for the treatment of urinary tract infection isolates. J. Med. Microbiol. 2019, 68, 1244–1252. [Google Scholar] [CrossRef]
- Fu, Z.; Liska, D.; Talan, D.; Chung, M. Cranberry Reduces the Risk of Urinary Tract Infection Recurrence in Otherwise Healthy Women: A Systematic Review and Meta-Analysis. J. Nutr. 2017, 147, 2282–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gbinigie, O.A.; Spencer, E.A.; Heneghan, C.J.; Lee, J.J.; Butler, C.C. Cranberry Extract for Symptoms of Acute, Uncomplicated Urinary Tract Infection: A Systematic Review. Antibiotics 2020, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.G.; Williams, G.; Craig, J.C. Cranberries for preventing urinary tract infections. Cochrane Database Syst. Rev. 2012, 10, CD001321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luis, A.; Domingues, F.; Pereira, L. Can Cranberries Contribute to Reduce the Incidence of Urinary Tract Infections? A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Clinical Trials. J. Urol. 2017, 198, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Lenger, S.M.; Bradley, M.S.; Thomas, D.A.; Bertolet, M.H.; Lowder, J.L.; Sutcliffe, S. D-mannose vs other agents for recurrent urinary tract infection prevention in adult women: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2020, 223, 265e1–265e13. [Google Scholar] [CrossRef]
- Kyriakides, R.; Jones, P.; Somani, B.K. Role of D-Mannose in the Prevention of Recurrent Urinary Tract Infections: Evidence from a Systematic Review of the Literature. Eur. Urol. Focus 2021, 7, 1166–1169. [Google Scholar] [CrossRef]
- Parazzini, F.; Ricci, E.; Fedele, F.; Chiaffarino, F.; Esposito, G.; Cipriani, S. Systematic review of the effect of D-mannose with or without other drugs in the treatment of symptoms of urinary tract infections/cystitis (Review). Biomed. Rep. 2022, 17, 69. [Google Scholar] [CrossRef]
- Ong Lopez, A.M.C.; Tan, C.J.L.; Yabon, A.S., 2nd; Masbang, A.N. Symptomatic treatment (using NSAIDS) versus antibiotics in uncomplicated lower urinary tract infection: A meta-analysis and systematic review of randomized controlled trials. BMC Infect. Dis. 2021, 21, 619. [Google Scholar] [CrossRef]
- Carey, M.R.; Vaughn, V.M.; Mann, J.; Townsend, W.; Chopra, V.; Patel, P.K. Is Non-Steroidal Anti-Inflammatory Therapy Non-Inferior to Antibiotic Therapy in Uncomplicated Urinary Tract Infections: A Systematic Review. J. Gen. Intern. Med. 2020, 35, 1821–1829. [Google Scholar] [CrossRef] [Green Version]
- Koradia, P.; Kapadia, S.; Trivedi, Y.; Chanchu, G.; Harper, A. Probiotic and cranberry supplementation for preventing recurrent uncomplicated urinary tract infections in premenopausal women: A controlled pilot study. Expert Rev. Anti Infect. Ther. 2019, 17, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, A.E.; Dziura, J.; Hooton, T.M.; Cox, M.E.; Yarova-Yarovaya, Y.; Chen, S.; Gupta, K. Recurrent urinary tract infection and urinary Escherichia coli in women ingesting cranberry juice daily: A randomized controlled trial. Mayo Clin. Proc. 2012, 87, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Barbosa-Cesnik, C.; Brown, M.B.; Buxton, M.; Zhang, L.; DeBusscher, J.; Foxman, B. Cranberry juice fails to prevent recurrent urinary tract infection: Results from a randomized placebo-controlled trial. Clin. Infect. Dis. 2011, 52, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Maki, K.C.; Kaspar, K.L.; Khoo, C.; Derrig, L.H.; Schild, A.L.; Gupta, K. Consumption of a cranberry juice beverage lowered the number of clinical urinary tract infection episodes in women with a recent history of urinary tract infection. Am. J. Clin. Nutr. 2016, 103, 1434–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyere, F.; Azzouzi, A.R.; Lavigne, J.P.; Droupy, S.; Coloby, P.; Game, X.; Karsenty, G.; Issartel, B.; Ruffion, A.; Misrai, V.; et al. A Multicenter, Randomized, Placebo-Controlled Study Evaluating the Efficacy of a Combination of Propolis and Cranberry (Vaccinium macrocarpon) (DUAB(R)) in Preventing Low Urinary Tract Infection Recurrence in Women Complaining of Recurrent Cystitis. Urol. Int. 2019, 103, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Vostalova, J.; Vidlar, A.; Simanek, V.; Galandakova, A.; Kosina, P.; Vacek, J.; Vrbkova, J.; Zimmermann, B.F.; Ulrichova, J.; Student, V. Are High Proanthocyanidins Key to Cranberry Efficacy in the Prevention of Recurrent Urinary Tract Infection? Phytother. Res. 2015, 29, 1559–1567. [Google Scholar] [CrossRef]
- Ledda, A.; Bottari, A.; Luzzi, R.; Belcaro, G.; Hu, S.; Dugall, M.; Hosoi, M.; Ippolito, E.; Corsi, M.; Gizzi, G.; et al. Cranberry supplementation in the prevention of non-severe lower urinary tract infections: A pilot study. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 77–80. [Google Scholar]
- Kontiokari, T.; Sundqvist, K.; Nuutinen, M.; Pokka, T.; Koskela, M.; Uhari, M. Randomised trial of cranberry-lingonberry juice and Lactobacillus GG drink for the prevention of urinary tract infections in women. BMJ 2001, 322, 1571. [Google Scholar] [CrossRef] [Green Version]
- Stothers, L. A randomized trial to evaluate effectiveness and cost effectiveness of naturopathic cranberry products as prophylaxis against urinary tract infection in women. J. Urol. 2002, 9, 1558–1562. [Google Scholar]
- Beerepoot, M.A.; ter Riet, G.; Nys, S.; van der Wal, W.M.; de Borgie, C.A.; de Reijke, T.M.; Prins, J.M.; Koeijers, J.; Verbon, A.; Stobberingh, E.; et al. Cranberries vs antibiotics to prevent urinary tract infections: A randomized double-blind noninferiority trial in premenopausal women. Arch. Intern. Med. 2011, 171, 1270–1278. [Google Scholar] [CrossRef] [Green Version]
- Babar, A.; Moore, L.; Leblanc, V.; Dudonne, S.; Desjardins, Y.; Lemieux, S.; Bochard, V.; Guyonnet, D.; Dodin, S. High dose versus low dose standardized cranberry proanthocyanidin extract for the prevention of recurrent urinary tract infection in healthy women: A double-blind randomized controlled trial. BMC Urol. 2021, 21, 44. [Google Scholar] [CrossRef]
- Kranjcec, B.; Papes, D.; Altarac, S. D-mannose powder for prophylaxis of recurrent urinary tract infections in women: A randomized clinical trial. World J. Urol. 2014, 32, 79–84. [Google Scholar] [CrossRef]
- Porru, D.; Parmigiani, A.; Tinelli, C.; Barletta, D.; Choussos, D.; Di Franco, C.; Bobbi, V.; Bassi, S.; Miller, O.; Gardella, B.; et al. Oral D-mannose in recurrent urinary tract infections in women: A pilot study. J. Clin. Urol. 2014, 7, 208–213. [Google Scholar] [CrossRef]
- Mainini, G.; Passaro, M.; Schiattarella, A.; Franciscis, P.; Donna, M.C.D.; Trezza, G. Prevention and treatment of cystitis during menopause: Efficacy of a nutraceutical containing D-mannose, inulin, cranberry, bearberry, Olea europaea, Orthosiphon and Lactobacillus acidophilus. Prz. Menopauzalny 2020, 19, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Murina, F.; Vicariotto, F.; Lubrano, C. Efficacy of an orally administered combination of Lactobacillus paracasei LC11, cranberry and D-mannose for the prevention of uncomplicated, recurrent urinary tract infections in women. Urologia 2021, 88, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Gágyor, I.; Bleidorn, J.; Kochen, M.M.; Schmiemann, G.; Wegscheider, K.; Hummers-Pradier, E. Ibuprofen versus fosfomycin for uncomplicated urinary tract infection in women: Randomised controlled trial. BMJ 2015, 351, h6544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vik, I.; Bollestad, M.; Grude, N.; Bærheim, A.; Damsgaard, E.; Neumark, T.; Bjerrum, L.; Cordoba, G.; Olsen, I.C.; Lindbæk, M. Ibuprofen versus pivmecillinam for uncomplicated urinary tract infection in women-A double-blind, randomized non-inferiority trial. PLoS Med. 2018, 15, e1002569. [Google Scholar] [CrossRef] [PubMed]
- Bleidorn, J.; Gágyor, I.; Kochen, M.M.; Wegscheider, K.; Hummers-Pradier, E. Symptomatic treatment (ibuprofen) or antibiotics (ciprofloxacin) for uncomplicated urinary tract infection?--results of a randomized controlled pilot trial. BMC Med. 2010, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, K.; Lee, W.K.; Oh, C.Y.; Lee, S.H.; Cho, S.T.; Bang, W.J.; Shin, T.Y.; Choo, M.S.; Cho, J.S.; Lee, Y.G.; et al. Is A Combination of Antibiotics and Non-Steroidal Anti-Inflammatory Drugs More Beneficial Than Antibiotic Monotherapy For The Treatment of Female Acute Uncomplicated Cystitis? A Randomized Controlled Pilot Study. Urol. J. 2018, 15, 365–369. [Google Scholar] [CrossRef]
- Howell, A.B.; Vorsa, N.; Der Marderosian, A.; Foo, L.Y. Inhibition of the adherence of P-fimbriated Escherichia coli to uroepithelial-cell surfaces by proanthocyanidin extracts from cranberries. N. Engl. J. Med. 1998, 339, 1085–1086. [Google Scholar] [CrossRef]
- Zafriri, D.; Ofek, I.; Adar, R.; Pocino, M.; Sharon, N. Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells. Antimicrob. Agents Chemother. 1989, 33, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Chahales, P.; Thanassi, D.G. Structure, Function, and Assembly of Adhesive Organelles by Uropathogenic Bacteria. Microbiol. Spectr. 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Behzadi, P. Classical chaperone-usher (CU) adhesive fimbriome: Uropathogenic Escherichia coli (UPEC) and urinary tract infections (UTIs). Folia Microbiol. 2020, 65, 45–65. [Google Scholar] [CrossRef] [PubMed]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-antibiotic Antimicrobial Strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulvey, M.A. Adhesion and entry of uropathogenic Escherichia coli. Cell Microbiol. 2002, 4, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Lupo, F.; Ingersoll, M.A.; Pineda, M.A. The glycobiology of uropathogenic E. coli infection: The sweet and bitter role of sugars in urinary tract immunity. Immunology 2021, 164, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Bouckaert, J.; Berglund, J.; Schembri, M.; De Genst, E.; Cools, L.; Wuhrer, M.; Hung, C.S.; Pinkner, J.; Slättegård, R.; Zavialov, A.; et al. Receptor binding studies disclose a novel class of high-affinity inhibitors of the Escherichia coli FimH adhesin. Mol. Microbiol. 2005, 55, 441–455. [Google Scholar] [CrossRef]
- Rice, J.C.; Peng, T.; Spence, J.S.; Wang, H.Q.; Goldblum, R.M.; Corthesy, B.; Nowicki, B.J. Pyelonephritic Escherichia coli expressing P fimbriae decrease immune response of the mouse kidney. J. Am. Soc. Nephrol. 2005, 16, 3583–3591. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.; Waksman, G. Chaperone–usher pathways: Diversity and pilus assembly mechanism. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 1112–1122. [Google Scholar] [CrossRef] [Green Version]
- Sihra, N.; Goodman, A.; Zakri, R.; Sahai, A.; Malde, S. Nonantibiotic prevention and management of recurrent urinary tract infection. Nat. Rev. Urol. 2018, 15, 750–776. [Google Scholar] [CrossRef]
- Ranfaing, J.; Dunyach-Remy, C.; Louis, L.; Lavigne, J.P.; Sotto, A. Propolis potentiates the effect of cranberry (Vaccinium macrocarpon) against the virulence of uropathogenic Escherichia coli. Sci. Rep. 2018, 8, 10706. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, A.J.; Amundsen, S.K.; Jones, J.M. Effect of carbohydrates on adherence of Escherichica coli to human urinary tract epithelial cells. Infect. Immun. 1980, 30, 531–537. [Google Scholar] [CrossRef]
- Wellens, A.; Garofalo, C.; Nguyen, H.; Van Gerven, N.; Slättegård, R.; Hernalsteens, J.P.; Wyns, L.; Oscarson, S.; De Greve, H.; Hultgren, S.; et al. Intervening with urinary tract infections using anti-adhesives based on the crystal structure of the FimH-oligomannose-3 complex. PLoS ONE 2008, 3, e2040. [Google Scholar] [CrossRef]
- Ofek, I.; Goldhar, J.; Eshdat, Y.; Sharon, N. The importance of mannose specific adhesins (lectins) in infections caused by Escherichia coli. Scand. J. Infect. Diseases. Suppl. 1982, 33, 61–67. [Google Scholar]
- Abraham, S.N.; Miao, Y. The nature of immune responses to urinary tract infections. Nat. Rev. Immunol. 2015, 15, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quaglietta, L.; Martinelli, M.; Staiano, A. Serious infectious events and ibuprofen administration in pediatrics: A narrative review in the era of COVID-19 pandemic. Ital. J. Pediatr. 2021, 47, 20. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.; Trill, J.; Simpson, C.; Webley, F.; Radford, M.; Stanton, L.; Maishman, T.; Galanopoulou, A.; Flower, A.; Eyles, C.; et al. Uva-ursi extract and ibuprofen as alternative treatments for uncomplicated urinary tract infection in women (ATAFUTI): A factorial randomized trial. Clin. Microbiol. Infect. 2019, 25, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Rubin, R.H.; Shapiro, E.D.; Andriole, V.T.; Davis, R.J.; Stamm, W.E. Evaluation of new anti-infective drugs for the treatment of urinary tract infection. Infectious Diseases Society of America and the Food and Drug Administration. Clin. Infect. Dis. 1992, 15 (Suppl. 1), S216–S227. [Google Scholar] [CrossRef]
- Grabe, M.; Bishop, M.; Bjerklund-Johansen, T.; Botto, H.; Cek, M.; Lobel, B.; Naber, K.; Palou, J.; Tenke, P.; Wagenlehner, F. Guidelines on urological infections. Eur. Assoc. Urol. 2015, 182, 237–257. [Google Scholar]
- Jannelli, M.L.; Wu, J.M.; Plunkett, L.W.; Williams, K.S.; Visco, A.G. A randomized controlled trial of clean intermittent self-catheterization versus suprapubic catheterization after urogynecologic surgery. Am. J. Obstet. Gynecol. 2007, 197, 72.e71–72.e74. [Google Scholar] [CrossRef]
- Wong, H.F.; Lee, L.C.; Han, H.C. Cost-effective screening for urinary tract infections in urogynaecological patients. Int. Urogynecology J. Pelvic Floor Dysfunct. 2008, 19, 671–676. [Google Scholar] [CrossRef]
- Ottiger, C.; Schaer, G.; Huber, A.R. Time-course of quantitative urinary leukocytes and bacteria counts during antibiotic therapy in women with symptoms of urinary tract infection. Clin. Chim. Acta Int. J. Clin. Chem. 2007, 379, 36–41. [Google Scholar] [CrossRef]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int. Urogynecology J. 2010, 21, 5–26. [Google Scholar] [CrossRef]
- Howell, A.B. Bioactive compounds in cranberries and their role in prevention of urinary tract infections. Mol. Nutr. Food Res. 2007, 51, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Déprez, S.; Brezillon, C.; Rabot, S.; Philippe, C.; Mila, I.; Lapierre, C.; Scalbert, A. Polymeric proanthocyanidins are catabolized by human colonic microflora into low-molecular-weight phenolic acids. J. Nutr. 2000, 130, 2733–2738. [Google Scholar] [CrossRef]
- Alton, G.; Hasilik, M.; Niehues, R.; Panneerselvam, K.; Etchison, J.R.; Fana, F.; Freeze, H.H. Direct utilization of mannose for mammalian glycoprotein biosynthesis. Glycobiology 1998, 8, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Patán, F.; Bartolomé, B.; Martín-Alvarez, P.J.; Anderson, M.; Howell, A.; Monagas, M. Comprehensive assessment of the quality of commercial cranberry products. Phenolic characterization and in vitro bioactivity. J. Agric. Food Chem. 2012, 60, 3396–3408. [Google Scholar] [CrossRef] [PubMed]
- Pappas, E.; Schaich, K.M. Phytochemicals of cranberries and cranberry products: Characterization, potential health effects, and processing stability. Crit. Rev. Food Sci. Nutr. 2009, 49, 741–781. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.M.; Clark, J.; Mar, C.D.; Glasziou, P. Increased fluid intake to prevent urinary tract infections: Systematic review and meta-analysis. Br. J. Gen. Pract. 2020, 70, e200–e207. [Google Scholar] [CrossRef]
- Spaulding, C.N.; Klein, R.D.; Ruer, S.; Kau, A.L.; Schreiber, H.L.; Cusumano, Z.T.; Dodson, K.W.; Pinkner, J.S.; Fremont, D.H.; Janetka, J.W.; et al. Selective depletion of uropathogenic E. coli from the gut by a FimH antagonist. Nature 2017, 546, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Gouin, S.G.; Wellens, A.; Bouckaert, J.; Kovensky, J. Synthetic multimeric heptyl mannosides as potent antiadhesives of uropathogenic Escherichia coli. ChemMedChem 2009, 4, 749–755. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| A: Study Design of Cranberry Trials | |||||
| Name Year | Study Design | Focus | Intervention | Mean Age | Sample Size (Reported Power *) |
| A1. Koradia, 2019 [41] | Randomised, double-blind, placebo-controlled, parallel group pilot clinical trial; 6 months duration | rUTI Prevention | Group 1: BKPro-Cyan (36 mg PAC) Group 2: Placebo capsule 2×/day | Group 1:34.6 (SD:9.6) Group 2:34.8 (SD:10.1) | 90 |
| A2. Maki, 2016 [44] | Randomised, double-blind, placebo-controlled, multicentre clinical trial; 6 months duration | rUTI Prevention | Group 1: 8-oz (240-mL) cranberry (DMAC-method I: 41.1 ± 7.1 DMAC-method II: 119 ± 16.9) Group 2: Placebo beverage (240 mL) | Group 1:40.9 (SEM:1.1) Group 2:41.0 (SEM:1.0) | 373 (Yes) |
| A3. Bruyère, 2019 [45] | Randomised double-blinded, controlled study; 6 months duration | rUTI Prevention | Group 1: 2× cranberry-propolis-zinc (DUAB) /day Group 2: 2× placebo capsules/day; | Group 1:53.0 (SD:17.4) Group 2:53.0 (SD:19.2) | 85 (Yes) |
| A4. Vostalova, 2015 [46] | Single centre, randomised, double-blind placebo-controlled trial 7 months duration | rUTI Prevention | Group 1: Cranberry: 500 mg CFP (2× 250 mg CFP capsules) 1×/day (2.8 mg PAC) Group 2: Placebo capsule | Group 1:35.6 (SD:12.9) Group 2:38.0 (SD:13.4) | 182 (Yes) |
| A5. Ledda, 2015 [47] | Pilot registry study 2 months duration | rUTI Prevention | Group 1: Cranberry: 500 mg CFP (2× 250 mg CFP capsules) 1×/day (2.8 mg PAC) Group 2: Placebo; | Group 1:39 (SD:4) Group 2:39 (SD:3) | 44 |
| A6. Kontiokari, 2001 [48] | Open, randomised controlled 12 month follow up trial | rUTI Prevention | Group 1: 50 mL cranberry-lingonberry juice concentrate daily, 6 months Group 2: 100 mL of lactobacillus drink 5 days /week for 12 months Group 3: No intervention | Group 1:32 (SD:9.8) Group 2:30 (SD:11.8) Group 3:29 (SD:10.5) | 150 (No) |
| A7. Stothers, 2002 [49] | Randomised, controlled, double-blind clinical trial; 12 months duration | rUTI Prevention | Group 1: Placebo arm: 2×/day + 250 mL placebo juice 3×/day Group 2: Tablet arm: 1 cranberry 2×/day + 250 mL placebo juice 3×/day Group 3: Juice arm: 250 mL of unsweetened cranberry juice 3×/day + 1 placebo 2×/day; | Average (all groups) 42 | 150 |
| A8. Stapleton, 2012 [42] | Randomised double-blinded, controlled study 6 months duration | rUTI Prevention | Group 1: 4 oz of cranberry juice daily Group 2: 8 oz of cranberry juice daily Group 3: Placebo juice | Group 1:25.3 (SD:6.6) Group 2:26.4 (SD:6.5) | 176 (No) |
| A9. Barbosa-Cesnik, 2011 [43] | Prospective, randomised, double-blind comparison 6 months duration | rUTI Prevention | Group 1: 8 oz (240 mL) of 27% low-calorie cranberry juice cocktail 2×/day (112 mg PAC) Group 2: 8 oz of placebo juice 2×/day | Group 1:21.2 (SD:3.4) Group 2:21.2 (SD:3.5) | 319 (Yes) |
| A10. Gbinigie, 2021 [33] | Open-label feasibility randomised parallel group trial 7 days duration | Acute cystitis Treatment | Group 1: Immediate antibiotics Group 2: First-line antibiotics + cranberry capsules Group 3: Only cranberry capsules 2× cranberry 2×/day | Group 1:52.4 (SD:21.4) Group 2:52.4 (22.4) Group 3:40.8(14.0) | 46 (No) |
| A11. Beerepoot, 2011 [50] | Randomised double-blind, double dummy noninferiority trial 12 months duration | rUTI, prevention | Group 1: Trimethoprim-sulfamethoxazole (TMP-SMX), 480 mg/ day Group 2: Cranberry capsules, 500 mg 2×/day (9.1 mg PAC) | Median (IQR): Group 1:36.1 (27–46) Group 2:34.8 (23–44) | 221 (No) |
| A12. Babar, 2021 [51] | Randomised, controlled, double-blind clinical trial 5.5 months duration | rUTI, prevention | Group 1: Cranberry PAC extract Urophenol (2 × 18.5 mg/day) Group 2: Control low dose (2 × 1 mg/ day | Group 1:32.5 (SD:14.2) Group 2:27.2 (SD:8.8) | 145 |
| B. Study design of D-mannose trials | |||||
| Name Year | Study Design | Focus | Intervention | Mean age | Sample size (Reported Powered *) |
| B1. Kranjčec, 2014 [52] | Prospective, randomised controlled study 6 months duration | rUTI, Prevention | Group 1: 2 g D-mannose powder in 200 mL of water daily Group 2: 50 mg Nitrofurantoin/day Group 3: No prophylaxis | Median (age range) Group 1: 49 (38–56) Group 2: 48 (29–58) Group 3: 52 (38–56) | 308 (Yes) |
| B2. Porru, 2014 [53] | Randomised cross-over trial 6 months duration | rUTI, Prevention | Group 1: TMP-SMX 160 mg/800 mg–2×/day for 5 days, then single dose at night for 1 wk/month for next 23 wks Group 2: D-mannose 1 g 3×/day, every 8 h for 2 weeks, then 1 g–2×/day for 22 weeks Cross-over point at 24 wks | Average (all groups) 42 | 60 |
| C. Study design of combination cranberry and D-mannose trials | |||||
| Name Year | Study Design | Focus | Intervention | Mean age | Sample size (Reported Powered *) |
| C1. Mainini, 2020 [54] | Prospective cohort study 10 days for 12 months | rUTI, Prevention | Group 1: Used compound (Uticlin containing D-mannose, cranberry, bearberry, Olea europaea), inulin, Orthosiphon and Lactobacillus acidophilus) Group 2: No prophylaxis; Advised to consume 1.5 L water/ day | Group 1:53.0 (SD:5.8) Group 2:54.1 (SD:4.5) | 94 |
| C2. Murina, 2021 [55] | Single-centre study 3 months duration | rUTI, Prevention | Group 1: Lactoflorene Cist 1×/day for 10 days/month (Lactobacillus paracasei LC11, cranberry and D-mannose) Group 2: Lactoflorene Cist 1×/day for 90 days Group 3: No treatment | Mean (range) Group 1:38.2 (20–43) Group 2:39.4 (22–45) Group 3:38.4 (21–41) | 55 (Yes) |
| D. Study design of NSAID trials | |||||
| Name Year | Study Design | Focus | Intervention | Mean age | Sample size (Reported Powered*) |
| D1. Moore, 2019 [55] | Factorial randomised trial 3–5 days duration | Acute cystitis, Treatment | Group 1: Uva-ursi + ibuprofen Group 2: Placebo + ibuprofen Group 3: Uva-ursi + no ibuprofen Group 4: Placebo + no ibuprofen, Dosage: Uva-ursi: daily dose of 3600 mg; Ibuprofen: daily dose of 1200 mg | Group 1:45.5 (SD:15.2) Group 2:39.9 (SD:15.5) Group 3:44.6 (SD:16.1) Group 4:44.8 (SD:14.3) | 382 (No) |
| D2 Gágyor, 2015 [56] | Double blind randomised multicentre comparative effectiveness trial; 3 days duration | Acute cystitis, Treatment | Group 1: Fosfomycin 3 g Group 2: Ibuprofen 3 × 400mg | Group 1:37.3 (SD:14.3) Group 2:37.3 (SD:14.6) | 494 (Yes) |
| D3. Vik, 2018 [57] | Double-blind, randomised, parallel group, multicentre non-inferiority trial; 3 days duration | Acute cystitis, Treatment | Group 1: 600 mg Ibuprofen Group 2: 200 mg pivmecillinam 3×/day | Group 1:28.1 (SD:8.6) Group 2:28.5 (SD:10.2) | 383 (Yes) |
| D4. Bleidorn, 2010 [58] | Double-blind, randomised controlled pilot trial 3 days duration | Acute cystitis, Treatment | Group 1: Ibuprofen 3 × 400 mg oral Group 2: Ciprofloxacin 2 × 250 mg (+1 placebo) | Group 1:44.5 Group 2:43.7 | 80 (No) |
| D5. Ko, 2018 [59] | Double-blind, randomised controlled pilot trial 3 days duration | Acute cystitis, Treatment | Group 1: Cepodoxime (100 mg 2×/day) Group 2: Cepodoxime (100 mg) + aceclofenac (100 mg) 2×/day | Average (all groups) 49.9 (SD:13.5) | 55 (No) |
| Measure | Definition | References |
|---|---|---|
| Number of UTI | Statistically significant reduction in the number of UTIs in treatment versus placebo group. | [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,58] |
| Time to first UTI | Statistically significant reduction in the time to first UTI in treatment versus placebo group. | [33,41,44,45,46,52] |
| % Of patients UTI free | Statistically significant difference susceptible patients who did not acquire a UTI during this study period. | [33,41,42,44,45,48,49,50,51,54,55] |
| Duration of UTI | Statistically significant difference in the total time frame patients experienced the UTI for up until symptom resolution | [47] |
| Symptom scores | Significant UTI-associated symptom relief experienced in patients after taking treatment | [56,57,58,59,77] |
| A. Outcomes of Cranberry Trials | ||||
|---|---|---|---|---|
| Name Year | UTI Threshold (CFU/mL) Bacteria Isolated | Outcome Reported | Side Effects Reported | Reported Success * |
| A1. Koradia, 2019 [41] | ≥ 103 N/A | No of UTIs: BKProCyan vs. placebo: 4 (9.1%) vs. 33.3% (p = 0.005) Time to first UTI: Median time: 174 vs. 90 days (p = 0.001) UTI free: BKPro-Cyan group vs. placebo group (90.9 vs. 66.7%) Duration of UTI:N/A Symptom Scores:N/A | 3 (6.8%) had abdominal distention (n = 1) and diarrhoea (n = 2) All reported TEAEs were mild in severity, considered related to the study drug and resolved without corrective treatment | Yes |
| A2. Maki, 2016 [44] | ≥ 103 E. coli | No of UTIs: Cranberry vs. placebo: 39 vs. 67 (p = 0.016) Time to first UTI: Cranberry vs. placebo: 33 (17.8%) vs. 50 (26.6%) first UTI with pyuria (p = 0.131) UTI free: Cranberry vs. Placebo: 33 subjects (17.8%) vs. 50 (26.6%) (HR: 0.67; 95% CI: 0.43, 1.05; p = 0.078) Duration of UTI:N/A Symptom Scores:N/A | GI issues: 3 (1.6%) with nausea (p = 0.044) Headache [cranberry group: n = 16 (8.6%); sinusitis [cranberry group: n = 10 (5.4%)] and upper respiratory infection [cranberry group: n = 13 (7.0%); All serious AEs unlikely related to cranberry product | Yes |
| A3. Bruyère, 2019 [45] | ≥ 105 E. coli | No of UTIs: Frequency of cystitis in first 3 mo: 0.7 ± 1.1 propolis + cranberry group vs. 1.3 ± 1.1 placebo (p = 0.0257), but not in the first 6 months Total cystitis episodes within first 3 mo: 1.4 ± 1.0 vs. 2.0 ± 1.0 (p = 0.0680) Time to first UTI: 69.9 ± 45.8 days vs. 43.3 ± 45.9 (p = 0.0258) UTI free: 47.1% in the propolis and cranberry vs. 36.1% in the placebo group (p = 0.3527) Duration of UTI:N/A Symptom Scores:N/A | 3 events: Sigmoid diverticulitis, acute pyelonephritis and hallux valgus corrective surgery. All unrelated to treatment | Yes |
| A4. Vostalova, 2015 [46] | ≥ 105 E. coli | No of UTIs: Average UTIs/subject: 0.12 (10/83 vs. 0.32 (30/93) (p = 0.03) >1 UTI: 9/83 (10.84%) in cranberry vs. 24/93 (25.81%) in placebo (p = 0.04) Time to first UTI: 133 days in the cranberry group vs. 65 days in placebo group (p = 0.04) UTI free:N/A Duration of UTI:N/A Symptom of scores:N/A | None reported | Yes |
| A5. Ledda, 2015 [47] | N/A N/A | No of UTIs: 73.3% reduction in freq. of UTI (p < 0.05) 15.4% reduction in control group (p = 0.012) Time to first UTI:N/A UTI free: N/A Duration of UTIs: 2.5 ± 1.3 vs. 3.6 ± 1.7 days (p < 0.05) Symptom scores:N/A | 3 (13.6%) in cranberry group required medical consultation for UTI symptoms (p < 0.05). However, no AEs reported | Yes |
| A6. Kontiokari, 2001 [48] | ≥ 105 E. coli | No of UTIs: Difference between cranberry and control] (0.36 UTIs /person year) (95% CI 0.03–0.68, p = 0.03) [Cranberry: 0.45: Lactobacillus: 0.91: Control: 0.81 Time to first UTI: N/A UTI free: 8 (16%), 19 (39%) and 18 (36%): 20% reduction in cranberry vs. control (95% CI: 3% to 36%, p = 0.023) Duration of UTI:N/A Symptom scores: N/A | No AEs reported except for occasional complaint of the bitter taste of cranberry juice | Yes |
| A7. Stothers, 2002 [49] | ≥ 105 N/A | No of UTIs: Mean no. UTIs was 0.72 in placebo group, 0.30 in juice group (p < 0.05) and 0.39 in tablet group (p < 0.05) Time to first UTI: N/A UTI free: Placebo: 16 (32%), Juice: 10 (20%, p < 0.05) and tablet 9 (18%, p < 0.05) Duration of UTI:N/A Symptom scores:N/A | Juice: reflux; tablet: mild nausea, increased frequency of bowel movements | No |
| A8. Stapleton, 2012 [42] | ≥ 103 E. coli | No of UTIs: Cranberry vs. placebo: (33/120, 27.5%) vs. placebo group (17/56; 30.4%) Time to first UTI: N/A UTI free: Not significantly different between groups (p = 0.41) Duration of UTI:N/A Symptom scores:N/A | 3 discontinued due to GI symptoms: including constipation, heartburn, vaginal (itching, dryness) and other (migraine) symptoms | No |
| A9. Barbosa-Cesnik, 2011 [43] | ≥ 103 E. coli | No of UTIs: Cranberry vs. placebo: vs. cumulative incidence rate: 19.3% vs. 14.6% (p = 0.21) Time to first UTI: N/A UTI free: N/A Duration of UTI:N/A Symptom scores:N/A | SAEs unrelated to treatment | No |
| A10. Gbinigie, 2021 [33] | >105 N/A | No of UTIs: N/A Time to first UTI: Reduced in group 2 (adjusted mean difference: 0.6; 95%CI: −4.0 to 5.3) and increased in group 3 (adjusted mean diff: 7.9; 95%CI 2.6–13.2) vs. control UTI free: Reduced in group 2 (adjusted HR 1.7. 95% CI: 0.7 to 4.1) but increased in group 3 (adjusted HR 0.6; 95% CI: 0.2 to 1.4), compared with controls Duration of symptoms:N/A Symptom scores:N/A | 7 total events: Immediate antibiotics and immediate cranberry: suprapubic pain, dysuria, backache, cloudy urine. Immediate cranberry and delayed antibiotics: feeling unwell, ache in lower back, backache, stomach-ache, headache and nausea | No |
| A11. Beerepoot, 2011 [50] | ≥ 103 E. Coli | No of UTIs: TMP-SMX vs. Cranberry: After 3 mo: 0.5 (95% CI:0.3–0.7) and 0.7 (95% CI: 0.4–0.9) (p = 0.30) After 12 mo: 1.8 (95% CI: 0.8–2.7) vs. 4.0 (2.3–5.6) (p = 0.02) Time to first UTI: N/A UTI free: TMP-SMX vs. cranberry: Median time: 8 mo vs. 4 mo (p = 0.03) >1 UTI TMP-SMX vs. cranberry: After 3 months: 32.1 (19.7.42.5) and 36.9 (22.9–48.3) (p = 0.75) Duration of UTI:N/A Symptom scores:N/A | None | No |
| A12. Babar, 2021 [51] | ≥ 103 N/A | No of UTIs: High dose vs. low PAC: 45 vs. 59 Time to first UTI: N/A UTI free: Median high dose vs. low PAC: 24.0 wks vs. 16.6 Duration of UTI:N/A Symptom scores:N/A | No serious AEs. Only one person reported dyspepsia, leading to a discontinuation | No |
| B. Outcomes of D-mannose trials | ||||
| Name Year | UTI threshold (CFU/mL) | Outcome reported | Side effects reported | Reported Success * |
| B1. Kranjčec, 2014 [52] | ≥ 103 E. coli | No of UTIs: D-mannose: 15 (14.6%) Nitrofurantoin:21 (20.4%) No prophylaxis:62 (60.8%) (p < 0.001 comparing prophylaxis to control) Time to first UTI: Median time: Mannose: 43 days (IQR: 15–50) vs. Nitrofurantoin: 24 days (IQR: 15–36) vs. no prophylaxis: 28 (20–42) (p = 0.12) UTI free:N/A Duration of UTI:N/A Symptom scores:N/A | 7.8% (p < 0.001) Diarrhoea (8/103) | Yes |
| B2. Porru, 2014 [53] | ≥ 105 E. coli | No of UTIs: Of the 60 women, 45 (75%) had 1 recurrence, 10/60 (16.6%) had 2 recurrences, 5/60 (8.3%) had no r-UTI Time to first UTI: 52.7 days (D-mannose) vs. 200 days (antibiotics) (p < 0.0001) Time to first UTI: N/A UTI free:N/A Duration of symptoms:N/A Symptom scores:N/A | None reported | Yes |
| C. Outcomes of combination cranberry and D-mannose trials | ||||
| Name Year | UTI threshold (CFU/mL) | Outcome reported | Side effects reported | Reported Success * |
| C1. Mainini, 2020 [54] | ≥ 103 E. coli | No of UTIs: Group 1 (active): 6-month follow-up: 8/48 (p = 0.0057) 12-month follow-up: 11/48 (p = 0.0005) Group 2 (placebo): 6-month follow-up: 3/46 (p = 0.2418) 12-month follow-up: 4/46 (p = 0.1168 Time to first UTI:N/A UTI free: Patients without r-UTI: Group 1 (active): 6-month follow-up: 8/48 (p = 0.0057) 12 months: 11/48 (p = 0.0005)Group 2 (placebo): 6-month follow-up: 3/46 (p = 0.2418) 12 months:4/46 (p = 0.1168) Duration of symptoms:N/A Symptom scores:N/A | None reported | Yes |
| C2. Murina, 2021 [55] | ≥ 103 E. coli | No of UTIs: Group 1:16% Group 2:15.5% Group 3:52.9% (p < 0.01) UTI Free: Day 90: Group 1:87.7% Group 2:84.9%. Group 3:42% Day 150: Group 1:65.8% Group 2:68.8% Group 3:36.9% UTI free:N/A Duration of symptoms:N/A Symptom scores:N/A | None reported | Yes |
| D. Outcomes of NSAID trials | ||||
| Name Year | UTI threshold (CFU/mL) | Outcome reported | Side effects reported | Reported Success * |
| D1. Moore, 2019 [77] | N/A N/A | No of UTIs: N/A Time to first UTI:N/A UTI free:N/A Duration of symptoms:N/A Symptom score: Freq. symptom severity on days 2–4, showed no difference in symptom severity between factorial groups | No UUT infections | Yes |
| D2. Gágyor, 2015 [56] | >102 E. coli | No of UTIs: N/A After day 14: Fosfomycin: 11% vs. 6% Ibuprofen (p = 0.049) Time to first UTI:N/A UTI free:N/A Duration of symptoms:N/A Symptom score: Higher symptom burden on days 0–7 in ibuprofen group | 4 in ibuprofen needed hospital admission; 1 GI haemorrhage likely due to Ibuprofen | No |
| D3. Vik, 2018 [57] | ≥103 E. coli | No of UTIs: N/A Time to first UTI:N/A UTI free:N/A Duration of symptoms:N/A Symptom score: Mean symptom sum score: 2.3 for Ibuprofen and 0.7 for pivmecillinam, estimated difference of 1.6 (95% CI 0.8–2.4) | 7 pyelonephritis cases in ibuprofen group | No |
| D4. Bleidorn, 2010 [58] | >102 E. coli | No of UTIs: Follow up: Day 28, 1 ciprofloxacin patient and 2 ibuprofen patients (p = 1.0) reported relapse Time to first UTI:N/A UTI free:N/A Duration of UTI:N/A Symptom course (SD): ibuprofen vs. ciprofloxacin. Day 7: 0.7 (1.26) vs. 0.6 (0.86) (p = 0.816) | Mostly GI disorders and upper respiratory tract infections, headaches likely unrelated to treatment | No |
| D5. Ko, 2018 [59] | ≥104 E. coli | No of UTIs: N/A Time to first UTI:N/A UTI free:N/A Duration of UTI:N/A Symptom score: Faster symptom resolution in combination therapy at 1.5 days (p = 0.035) | N/A | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konesan, J.; Liu, L.; Mansfield, K.J. The Clinical Trial Outcomes of Cranberry, D-Mannose and NSAIDs in the Prevention or Management of Uncomplicated Urinary Tract Infections in Women: A Systematic Review. Pathogens 2022, 11, 1471. https://doi.org/10.3390/pathogens11121471
Konesan J, Liu L, Mansfield KJ. The Clinical Trial Outcomes of Cranberry, D-Mannose and NSAIDs in the Prevention or Management of Uncomplicated Urinary Tract Infections in Women: A Systematic Review. Pathogens. 2022; 11(12):1471. https://doi.org/10.3390/pathogens11121471
Chicago/Turabian StyleKonesan, Jenane, Lu Liu, and Kylie J. Mansfield. 2022. "The Clinical Trial Outcomes of Cranberry, D-Mannose and NSAIDs in the Prevention or Management of Uncomplicated Urinary Tract Infections in Women: A Systematic Review" Pathogens 11, no. 12: 1471. https://doi.org/10.3390/pathogens11121471