
High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Children in Vietnam: An Observational, Hospital-Based Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
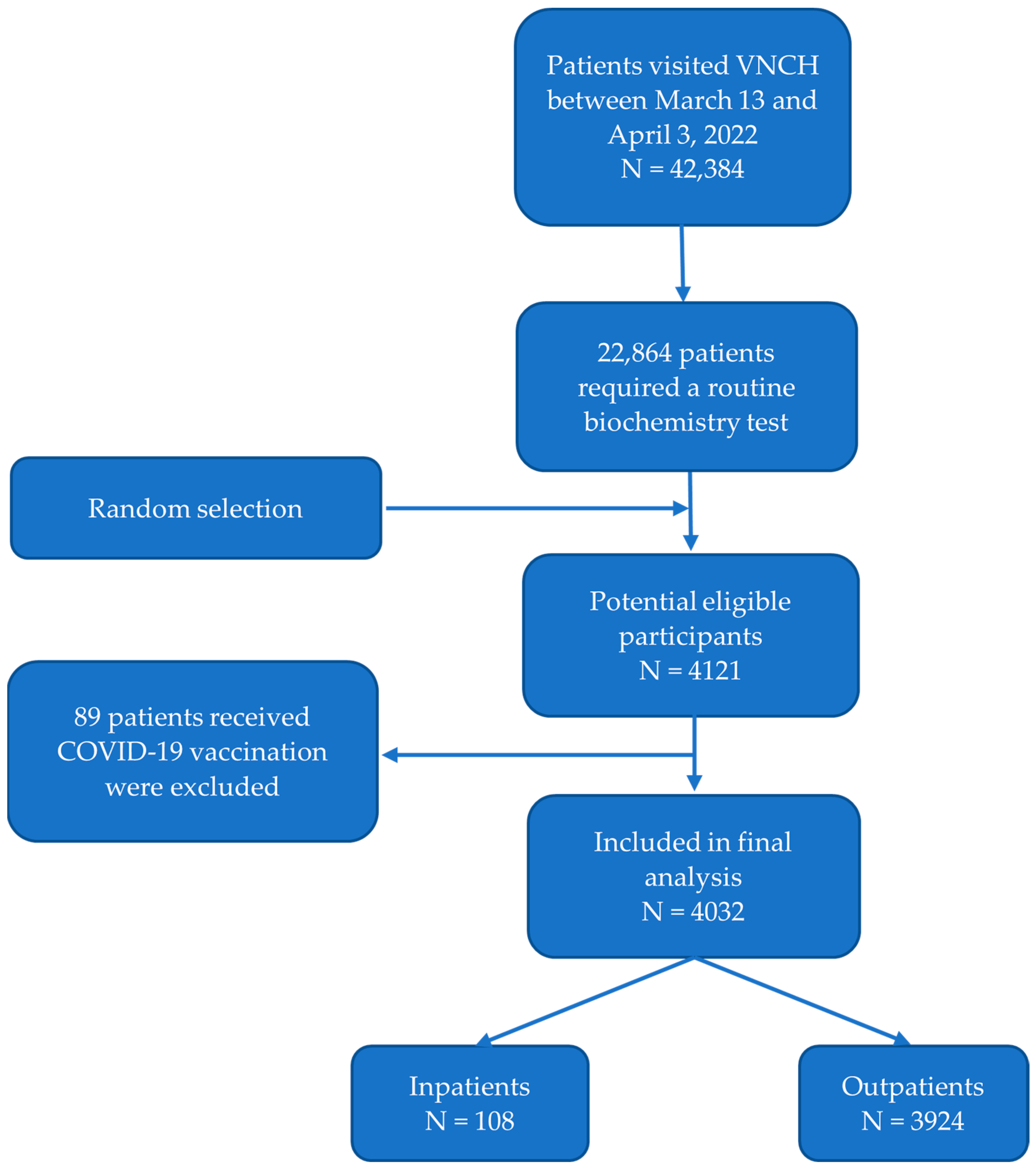
2.1. Study Design and Patients
2.2. Data Collection
2.3. Serological Samples and Laboratory Procedure
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Seroprevalence and Titer Level of Anti-SARS-CoV-2 Antibodies
3.3. Factors Associated with Anti-SARS-CoV-2 Antibody Seropositivity and Antibody Titer Level
3.3.1. Gender, Types of Care, and History of Prematurity
3.3.2. Age
3.3.3. Presence of Infected Household Members
3.3.4. Residences
3.3.5. History of Underlying or Using Corticosteroids or Immunosuppressants
3.3.6. Infants Aged ≤ 12 Months Old
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, O.P.; Bhandari, P.; Raut, A.; Kacimi, S.E.O.; Huy, N.T. Coronavirus Disease (COVID-19): Comprehensive Review of Clinical Presentation. Front. Public Health 2021, 8, 582932. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Chen, Y.; Liu, M.; Shi, S.; Tian, J. Impacts of immunosuppression and immunodeficiency on COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, e93–e95. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Mehta, N.S.; Mytton, O.T.; Mullins, E.; Fowler, T.A.; Falconer, C.L.; Murphy, O.B.; Langenberg, C.; Jayatunga, W.; Eddy, D.H.; Nguyen Van Tam, J.S. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clin. Infect. Dis. 2020, 71, 2469–2479. [Google Scholar] [CrossRef]
- Chou, J.; Thomas, P.G.; Randolph, A.G. Immunology of SARS-CoV-2 infection in children. Nat. Immunol. 2022, 23, 177–185. [Google Scholar] [CrossRef]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Principi, N.; Bosis, S.; Esposito, S. Effects of coronavirus infections in children. Emerg. Infect. Dis. 2010, 16, 183–188. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Levorson, R.E.; Christian, E.; Hunter, B.; Sayal, J.; Sun, J.; Bruce, S.A.; Garofalo, S.; Southerland, M.; Ho, S.; Levy, S.; et al. A cross-sectional investigation of SARS-CoV-2 seroprevalence and associated risk factors in children and adolescents in the United States. PLoS ONE 2021, 16, e0259823. [Google Scholar] [CrossRef] [PubMed]
- Dawood, F.S.; Porucznik, C.A.; Veguilla, V.; Stanford, J.B.; Duque, J.; Rolfes, M.A.; Dixon, A.; Thind, P.; Hacker, E.; Castro, M.; et al. Incidence Rates, Household Infection Risk, and Clinical Characteristics of SARS-CoV-2 Infection Among Children and Adults in Utah and New York City, New York. JAMA Pediatr. 2022, 176, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Wachter, F.; Regensburger, A.P.; Antonia, S.P.; Knieling, F.; Wagner, A.L.; Simon, D.; Hoerning, A.; Woelfle, J.; Überla, K.; Neubert, A.; et al. Continuous monitoring of SARS-CoV-2 seroprevalence in children using residual blood samples from routine clinical chemistry. Clin. Chem. Lab. Med. 2022, 60, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Alfraij, A.; Bin, A.A.A.; Al-Otaibi, A.M.; Alsharrah, D.; Aldaithan, A.; Kamel, A.M.; Almutairi, M.; Alshammari, S.; Almazyad, M.; Macarambon, J.M.; et al. Characteristics and outcomes of coronavirus disease 2019 (COVID-19) in critically ill pediatric patients admitted to the intensive care unit: A multicenter retrospective cohort study. J. Infect. Public Health 2021, 14, 193–200. [Google Scholar] [CrossRef]
- Takahashi, H.; Ichinose, N.; Okada, Y. False-negative rate of SARS-CoV-2 RT-PCR tests and its relationship to test timing and illness severity: A case series. IDCases 2022, 28, e01496. [Google Scholar] [CrossRef]
- Kanji, J.N.; Zelyas, N.; MacDonald, C.; Pabbaraju, K.; Khan, M.N.; Prasad, A.; Hu, J.; Diggle, M.; Berenger, B.M.; Tipples, G. False negative rate of COVID-19 PCR testing: A discordant testing analysis. Virol. J. 2021, 18, 13. [Google Scholar] [CrossRef]
- Waterfield, T.; Watson, C.; Moore, R.; Ferris, K.; Tonry, C.; Watt, A.; McGinn, C.; Foster, S.; Evans, J.; Lyttle, M.D.; et al. Seroprevalence of SARS-CoV-2 antibodies in children: A prospective multicentre cohort study. Arch. Dis. Child. 2021, 106, 680–686. [Google Scholar] [CrossRef]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, S.; Li, H.; Wang, Y.; Lu, Z.; Liu, Z.; Lai, Q.; Ji, Y.; Huang, X.; Li, Y.; et al. Viral and Antibody Kinetics of COVID-19 Patients with Different Disease Severities in Acute and Convalescent Phases: A 6-Month Follow-Up Study. Virol. Sin. 2020, 35, 820–829. [Google Scholar] [CrossRef] [PubMed]
- McConnell, D.; Hickey, C.; Bargary, N.; Trela-Larsen, L.; Walsh, C.; Barry, M.; Adams, R. Understanding the Challenges and Uncertainties of Seroprevalence Studies for SARS-CoV-2. Int. J. Environ. Res. Public Health 2021, 18, 4640. [Google Scholar] [CrossRef]
- Lewis, H.C.; Ware, H.; Whelan, M.; Subissi, L.; Li, Z.; Ma, X.; Nardone, A.; Valenciano, M.; Cheng, B.; Noel, K.; et al. SARS-CoV-2 infection in Africa: A systematic review and meta-analysis of standardised seroprevalence studies, from January 2020 to December 2021. BMJ Glob. Health 2022, 7, e008793. [Google Scholar] [CrossRef] [PubMed]
- Vial, P.; González, C.; Icaza, G.; Ramirez-Santana, M.; Quezada-Gaete, R.; Núñez-Franz, L.; Apablaza, M.; Vial, C.; Rubilar, P.; Correa, J.; et al. Seroprevalence, spatial distribution, and social determinants of SARS-CoV-2 in three urban centers of Chile. BMC Infect. Dis. 2022, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- ADVIA Centaur SARS-CoV-2 Total (COV2T)—Instructions for Use. Available online: https://www.fda.gov/media/138446/download (accessed on 28 October 2022).
- Sinaei, R.; Pezeshki, S.; Parvaresh, S.; Sinaei, R. Why COVID-19 is less frequent and severe in children: A narrative review. World J. Pediatr. 2021, 17, 10–20. [Google Scholar] [CrossRef]
- Posfay-Barbe, K.M.; Wagner, N.; Gauthey, M.; Moussaoui, D.; Loevy, N.; Diana, A.; L’Huillier, A.G. COVID-19 in Children and the Dynamics of Infection in Families. Pediatrics 2020, 146, e20201576. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Helgason, A.; Jonsson, H.; Magnusson, O.T.; Melsted, P.; Norddahl, G.L.; Saemundsdottir, J.; Sigurdsson, A.; Sulem, P.; Agustsdottir, A.B.; et al. Spread of SARS-CoV-2 in the Icelandic Population. N. Engl. J. Med. 2020, 382, 2302–2315. [Google Scholar] [CrossRef]
- Dimeglio, C.; Mansuy, J.M.; Charpentier, S.; Claudet, I.; Izopet, J. Children are protected against SARS-CoV-2 infection. J. Clin. Virol. 2020, 128, 104451. [Google Scholar] [CrossRef]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Knabl, L.; Mitra, T.; Kimpel, J.; Rössler, A.; Volland, A.; Walser, A.; Ulmer, H.; Pipperger, L.; Binder, S.C.; Riepler, L.; et al. High SARS-CoV-2 seroprevalence in children and adults in the Austrian ski resort of Ischgl. Commun. Med. (Lond.) 2021, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Lenicek, K.J.; Zrinski, T.R.; Stevanovic, V.; Lukic-Grlic, A.; Tabain, I.; Misak, Z.; Roic, G.; Kaic, B.; Mayer, D.; Hruskar, Z.; et al. Seroprevalence of SARS-CoV-2 infection among children in Children’s Hospital Zagreb during the initial and second wave of COVID-19 pandemic in Croatia. Biochem. Med. (Zagreb) 2021, 31, 020706. [Google Scholar] [CrossRef] [PubMed]
- Zinszer, K.; McKinnon, B.; Bourque, N.; Pierce, L.; Saucier, A.; Otis, A.; Cheriet, I.; Papenburg, J.; Hamelin, M.È.; Charlana, K.; et al. Seroprevalence of SARS-CoV-2 Antibodies Among Children in School and Day Care in Montreal, Canada. JAMA Netw. Open 2021, 4, e2135975. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. Why does the Omicron sub-variant spread faster than the original? Nature 2022, 602, 556–557. [Google Scholar] [CrossRef]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and Covid-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef]
- Kundu, A.; Maji, S.; Kumar, S.; Bhattacharya, S.; Chakraborty, P.; Sarkar, J. Clinical aspects and presumed etiology of multisystem inflammatory syndrome in children (MIS-C): A review. Clin. Epidemiol. Glob. Health 2022, 14, 100966. [Google Scholar] [CrossRef]
- Mallapaty, S. COVID jabs for kids: They’re safe and they work—So why is uptake so patchy? Nature 2022, 610, 246–248. [Google Scholar] [CrossRef]
- Anderson, E.J.; Campbell, J.D.; Creech, C.B.; Frenck, R.; Kamidani, S.; Munoz, F.M.; Nachman, S.; Spearman, P. Warp Speed for Coronavirus Disease 2019 (COVID-19) Vaccines: Why Are Children Stuck in Neutral? Clin. Infect. Dis. 2021, 73, 336–340. [Google Scholar] [CrossRef]
- Saxena, S.; Skirrow, H.; Wighton, K. Vaccinating children aged under 5 years against COVID-19. BMJ 2022, 378, o1863. [Google Scholar] [CrossRef]
- Lv, M.; Luo, X.; Shen, Q.; Lei, R.; Liu, X.; Liu, E.; Li, Q.; Chen, Y. Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Children and Adolescents: A Systematic Review. Vaccines 2021, 9, 1102. [Google Scholar] [CrossRef]
- Tian, F.; Yang, R.; Chen, Z. Safety and efficacy of COVID-19 vaccines in children and adolescents: A systematic review of randomized controlled trials. J. Med. Virol. 2022, 94, 4644–4653. [Google Scholar] [CrossRef] [PubMed]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Xing, Y.; Shi, L.; Li, W.; Gao, Y.; Pan, S.; Wang, Y.; Wang, W.; Xing, Q. Coinfection and Other Clinical Characteristics of COVID-19 in Children. Pediatrics 2020, 146, e20200961. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.A.; Saliba, V.; Lopez Bernal, J.; Ramsay, M.E.; Ladhani, S.N. SARS-CoV-2 infection and transmission in educational settings: A prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect. Dis. 2021, 21, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Callender, L.A.; Curran, M.; Bates, S.M.; Mairesse, M.; Weigandt, J.; Betts, C.J. The Impact of Pre-existing Comorbidities and Therapeutic Interventions on COVID-19. Front. Immunol. 2020, 11, 1991. [Google Scholar] [CrossRef]
- Zilla, M.L.; Keetch, C.; Mitchell, G.; McBreen, J.; Shurin, M.R.; Wheeler, S.E. SARS-CoV-2 Serologic Immune Response in Exogenously Immunosuppressed Patients. J. Appl. Lab. Med. 2021, 6, 486–490. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Ronchi, A.; Crippa, B.L.; Artieri, G.; Ballerini, C.; Crimi, R.; Mosca, F.; Pugni, L. Coronavirus Disease 2019 Vaccination During Pregnancy and Breastfeeding: A Review of Evidence and Current Recommendations in Europe, North America, and Australasia. Front. Pediatr. 2022, 10, 883953. [Google Scholar] [CrossRef]
- Rad, H.S.; Röhl, J.; Stylianou, N.; Allenby, M.C.; Bazaz, S.R.; Warkiani, M.E.; Guimaraes, F.; Clifton, V.L.; Kulasinghe, A. The Effects of COVID-19 on the Placenta During Pregnancy. Front. Immunol. 2021, 12, 743022. [Google Scholar] [CrossRef]
- Juan, J.; Gil, M.M.; Rong, Z.; Zhang, Y.; Yang, H.; Poon, L.C. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: Systematic review. Ultrasound Obstet. Gynecol. 2020, 56, 15–27. [Google Scholar] [CrossRef]
- Ng, K.W.; Faulkner, N.; Cornish, G.H.; Rosa, A.; Harvey, R.; Hussain, S.; Ulferts, R.; Earl, C.; Wrobel, A.G.; Benton, D.J.; et al. Preexisting and de novo humoral immunity to SARS-CoV-2 in humans. Science 2020, 370, 1339–1343. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Value (N = 4032) |
|---|---|
| Demographic data | |
| Age, months (median, IQR) | 39 (14–82) |
| Male sex (n, %) | 2447 (60.7%) |
| Kinh Ethnic (n, %) | 3950 (97.9%) |
| Residences (n, %) | |
| Hanoi | 2452 (60.8%) |
| Other provinces | 1580 (39.2%) |
| Underlying conditions (n, %) | |
| No underlying diseases | 3199 (79.1%) |
| Respiratory system | 46 (1.1%) |
| Cardiovascular system | 58 (1.4%) |
| Gastrointestinal system | 92 (2.3%) |
| Kidney and urology system | 117 (2.9%) |
| Immunodeficiency | 14 (0.4%) |
| Other underlying conditions | 516 (12.8%) |
| Seropositive Prevalence (n, %) | 2385 (59.2%) |
| Anti-SARS-CoV-2 antibodies titer level of seropositive subgroup (UI/mL) (median, IQR) | 4.78 (2.38–9.57) |
| Receiving blood product or immunoglobulin infusion within 6 months (n, %) | 22 (0.55%) |
| Subgroups | Overall, n (%) | Positive, n (%) | Negative, n (%) | OR (95%CI) | p-Value * |
|---|---|---|---|---|---|
| Age (months) | |||||
| ≤12 | 939 (23.3%) | 556 (59.2%) | 283 (40.8%) | 1 | |
| 13 to <36 | 967 (23.9%) | 642 (66.4%) | 325 (33.6%) | 1.36 (1.13–1.63) | 0.001 |
| 36 to <60 | 628 (15.6%) | 361 (57.5%) | 267 (42.5%) | 0.93 (0.75–1.14) | 0.49 |
| 60 to <144 | 1382 (34.3%) | 750 (54.3%) | 632 (45.7%) | 0.82 (0.69–0.97) | 0.02 |
| ≥144 | 116 (2.9%) | 76 (65.5%) | 40 (34.5%) | 1.31 (0.87–1.96) | 0.16 |
| Gender | |||||
| Male | 2447 (60.7%) | 1434 (58.6%) | 1013 (41.4%) | 0.94 (0.83–1.08) | 0.38 |
| Female | 1585 (39.3%) | 951 (60.0%) | 634 (40.0%) | ||
| Residence | |||||
| Hanoi | 2452 (60.8%) | 1540 (62.6%) | 912 (37.2%) | 1.46 (1.29–1.67) | 0.0001 |
| Other provinces | 1580 (39.2%) | 845 (53.3%) | 735 (46.5%) | ||
| Types of patient care | |||||
| In-patient | 108 (2.7%) | 59 (54.6%) | 49 (45.5%) | 0.83 (0.55–1.24) | 0.33 |
| Out-patient | 3924 (97.3%) | 2326 (59.3%) | 1598 (40.7%) | ||
| Previous COVID-19 infection of household members | |||||
| Yes | 2476 (61.4%) | 1630 (65.8%) | 846 (34.2%) | 2.04 (1.79–2.33) | 0.001 |
| No | 1556 (38.6%) | 755 (48.5%) | 801 (51.5%) | ||
| History of using corticosteroids or immunosuppressants | |||||
| Yes | 242 (6.0%) | 103 (42.6%) | 139 (57.4%) | 0.49 (0.37–0.64) | 0.001 |
| No | 3790 (94.0%) | 2282 (60.2%) | 1508 (39.8%) | ||
| History of Prematurity | |||||
| Yes | 214 (5.3%) | 119 (55.6%) | 95 (44.4%) | 0.86 (0.65–1.13) | 0.27 |
| No | 3818 (94.7%) | 2256 (59.4%) | 1542 (40.6%) | ||
| Underlying Conditions | |||||
| Yes | 843 (20.9%) | 425 (50.4%) | 418 (49.6%) | 0.64 (0.56–0.74) | 0.001 |
| No | 3189 (79.1%) | 1960 (61.5%) | 1229 (38.5%) | ||
| Subgroups | Positive, N = 2385, n (%) | Mean (UI/mL) | Median (UI/mL) | IQR | p-Value * |
|---|---|---|---|---|---|
| Age (months) | |||||
| ≤12 | 556 (23.3%) | 12.9 | 5.6 | 2.6–10.4 | <0.001 |
| 13 to <36 | 642 (26.9%) | 10.5 | 5.7 | 3.1–10.1 | |
| 36 to <60 | 361 (15.1%) | 13.0 | 4.1 | 1.9–7.7 | |
| 60 to <144 | 750 (31.5%) | 12.8 | 3.4 | 1.9–7.7 | |
| ≥144 | 76 (3.2%) | 165.7 | 63.3 | 7.8–257.9 | |
| Gender | |||||
| Male | 1434 (60.1%) | 18.3 | 4.9 | 2.4–9.7 | 0.36 |
| Female | 951 (39.9%) | 15.3 | 4.6 | 2.4–9.1 | |
| History of Prematurity | |||||
| Yes | 119 (5.0%) | 16.5 | 4.1 | 2.6–9.4 | 0.90 |
| No | 2256 (94.6%) | 17.1 | 4.8 | 2.4–9.6 | |
| Residences | |||||
| Hanoi | 1540 (64.6%) | 18.9 | 4.9 | 2.4–9.6 | 0.07 |
| Other provinces | 845 (35.4%) | 13.8 | 4.5 | 2.4–9.2 | |
| Types of Patient Care | |||||
| In-patient | 59 (2.5%) | 30.0 | 7.9 | 2.7–16.4 | 0.01 |
| Out-patient | 2326 (97.5%) | 16.8 | 4.7 | 2.4–9.4 | |
| Previous COVID-19 Infection of Household Members | |||||
| Yes | 1630 (68.3%) | 13.2 | 4.6 | 2.4–8.9 | 0.02 |
| No | 755 (31.7%) | 25.5 | 5.2 | 2.4–12.1 | |
| History of Using Corticosteroids or Immunosuppressants | |||||
| Yes | 103 (4.3%) | 15.2 | 3.5 | 1.9–9.8 | 0.10 |
| No | 2282 (95.7%) | 17.2 | 4.8 | 2.4–9.6 | |
| Underlying Conditions | |||||
| Yes | 425 (17.8%) | 17.6 | 3.8 | 2.1–8.5 | 0.005 |
| No | 1960 (82.1%) | 17.0 | 4.9 | 2.4–9.7 | |
| Variables | OR | Estimate with 95% CI | p-Value * |
|---|---|---|---|
| Age group | |||
| ≤12 months | 1 | ||
| 13 to < 36 months | 1.29 | 1.06–1.56 | 0.01 |
| 36 to < 60 months | 0.94 | 0.76–1.63 | 0.58 |
| 60 to < 144 months | 0.79 | 0.67–0.95 | 0.01 |
| ≥144 months | 1.84 | 1.21–2.80 | 0.005 |
| Residence of Hanoi | 1.54 | 1.34–1.77 | <0.001 |
| Presence of COVID-19 infection of household members | 2.36 | 2.06–2.70 | <0.001 |
| Presence of underlying condtions | 0.71 | 0.60–0.85 | <0.001 |
| History of using corticosteroids or immunosuppressants | 0.64 | 0.48–0.86 | 0.003 |
| Variables | Positive, N (%) | Negative, N (%) | OR (95%CI) | p-Value * |
|---|---|---|---|---|
| Maternal History of COVID-19 Vaccination | ||||
| Yes | 276 (60.5%) | 180 (39.5%) | 1.11 (0.85–1.45) | 0.42 |
| No | 280 (58.0%) | 203 (42.0%) | ||
| Maternal History of COVID-19 Infection | ||||
| Yes | 224 (70.9%) | 92 (29.1%) | 2,06 (1.54–2.75) | 0.0001 |
| No | 335 (53.8%) | 288 (46.2%) | ||
| Breastfeeding Status | ||||
| Yes | 495 (60.1%) | 328 (39.9%) | 1.36 (0.90–2.04) | 0.12 |
| No | 61 (52.6%) | 55 (47.4%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, D.M.; Vu, U.T.T.; Hoang, C.N.; Nguyen, H.T.T.; Nguyen, P.H.; Tran, M.C.T.; Chu, A.N.; Phan, P.H. High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Children in Vietnam: An Observational, Hospital-Based Study. Pathogens 2022, 11, 1442. https://doi.org/10.3390/pathogens11121442
Tran DM, Vu UTT, Hoang CN, Nguyen HTT, Nguyen PH, Tran MCT, Chu AN, Phan PH. High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Children in Vietnam: An Observational, Hospital-Based Study. Pathogens. 2022; 11(12):1442. https://doi.org/10.3390/pathogens11121442
Chicago/Turabian StyleTran, Dien Minh, Uyen Tu Thi Vu, Canh Ngoc Hoang, Ha Thu Thi Nguyen, Phu Huy Nguyen, Mai Chi Thi Tran, Anh Ngoc Chu, and Phuc Huu Phan. 2022. "High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Children in Vietnam: An Observational, Hospital-Based Study" Pathogens 11, no. 12: 1442. https://doi.org/10.3390/pathogens11121442