
Pragmatic Strategy for Fecal Specimen Storage and the Corresponding Test Methods for Clostridioides difficile Diagnosis

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Step 1: Analyze Bibliomic Data
2.2. Step 2: Perform an Experiment to Bridge the Gaps
2.2.1. Vegetative Cell and Spore Counts of C. difficile at Different Storage Conditions
2.2.2. C. difficile DNA Stability at Different Storage Conditions
2.3. Step 3: Compare the Storage Effects
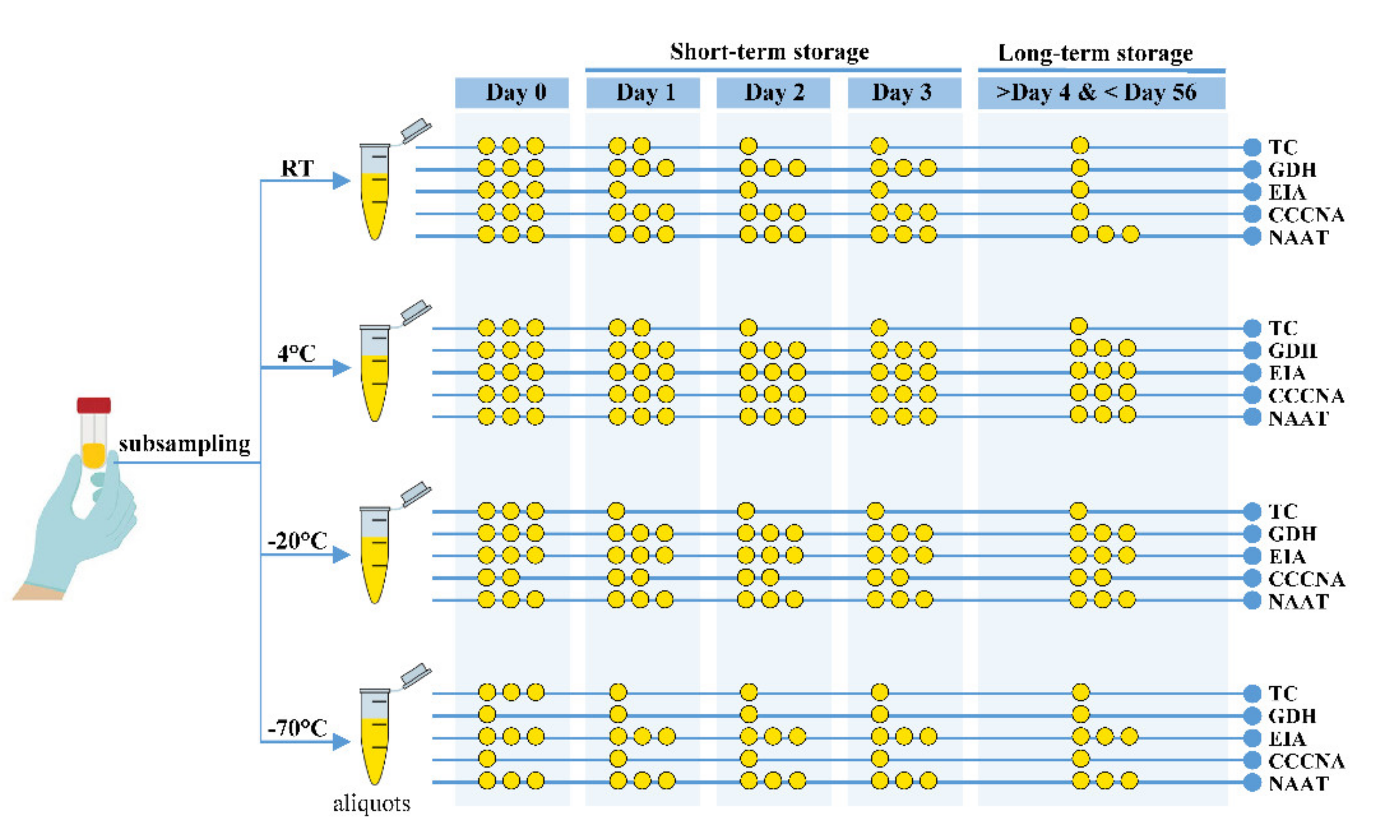
2.4. Step 4: Develop Handling and Storage Strategy
- Shorten the handling time;
- Avoid repeated dramatic temperature fluctuation;
- Avoid freeze–thaw cycles;
- Before testing the samples, distribute the feces into aliquots for future application;
- Store the aliquots at room, refrigeration (4 °C), and freezing (−20 °C or −70 °C) temperatures (if possible).
- At day 0, use stool samples stored at RT or refrigeration temperature (4 °C) for all test methods (TC, GDH, EIA, CCCNA, and NAAT);
- For TC before day 2, use stool samples stored at RT or 4 °C;
- For TC after day 2, use stool samples stored at 4 °C or a freeze temperature of −20 °C or −70 °C;
- For short-term (72 h) GDH assays, use stool samples stored at RT, 4 °C, or −20 °C;
- For long-term (after 72 h) GDH assays, use stool samples stored at 4 °C or −20 °C;
- For EIA during either short-term or long-term storage, use stool samples stored at 4 °C or a freeze temperature of −20 °C or −70 °C;
- For CCCNA during short-term storage, use stool samples stored at RT and 4 °C;
- For CCCNA during long-term storage, use stool samples stored at 4 °C;
- For NAAT, use any stool sample stored at any temperature (RT, 4 °C, −20 °C, or
- −70 °C).
2.5. Step 5: Verify the Strategy by Internal Review
3. Discussion
4. Materials and Methods
4.1. Literature Search
4.2. Bacterial Culture
4.3. Spiked Fecal and Storage Conditions
4.4. Vegetative and Spore Cell Counts from Plates
4.5. Real-Time PCR Detection Assay
4.6. Patient and Public Involvement
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| ATCC Strain | Strain | Toxinotype | Toxin | ||
|---|---|---|---|---|---|
| A | B | CDT | |||
| 43598 17857 17858 43255 43594 43596 43599 43600 51695 700792 9689 BAA-1382 BAA-1805 BAA-1870 BAA-1871 BAA-1872 BAA1873 BAA-1874 BAA-1875 BAA-2155 BAA-2156 | 1470 870 1253 VPI 10463 W1194 545 2022 2149 BDMS 18 AN 14797-2 90556-M6S 630 N/A 4118 4111 4206 5283 4205 5325 LBM 0801058 LBM 0801040 | VIII O O O O O O O O O O O IIIb IIIb O O O O V XXII O | − + + + + + + + + + + + + + + + + + + + + | + + + + + + + + + + + + + + + + + + + + + | + − − − − − − − − − − − + + − − − − − + − |
Appendix B
| Name | Toxin A (tcdA) | Toxin B (tcdB) | ||||
|---|---|---|---|---|---|---|
| Ref. 1 | This Study | Difference | Ref. 2 | This Study | Difference | |
| ATCC 43598 ATCC 17857 ATCC 17858 ATCC 43255 ATCC 43594 ATCC 43596 ATCC 43599 ATCC 43600 ATCC 51695 ATCC 700792 ATCC 9689 ATCC BAA-1382 ATCC BAA-1805 ATCC BAA-1870 ATCC BAA-1871 ATCC BAA-1872 ATCC BAA1873 ATCC BAA-1874 ATCC BAA-1875 ATCC BAA-2155 ATCC BAA-2156 | N/S 3 21.75 21.08 21.76 21.03 23.15 21.47 23.97 20.59 21.36 19.79 20.25 23.67 24.44 21.03 20.65 20.78 22.22 20.20 21.11 21.18 | N/S 3 18.48 22.42 18.59 19.12 20.52 19.40 19.46 20.45 19.32 20.14 22.63 18.80 20.47 22.08 21.17 17.11 21.00 20.38 20.42 18.26 | N/S 3 3.27 −1.34 3.16 1.91 2.63 2.07 4.50 0.14 2.03 −0.35 −2.38 4.87 3.97 −1.06 −0.52 3.68 1.22 −0.18 0.68 2.92 | 24.92 26.07 24.73 26.02 25.04 26.92 25.32 28.75 24.19 25.72 24.15 24.40 22.22 28.93 25.17 24.21 19.76 26.11 18.68 25.34 24.93 | 16.58 16.07 17.12 16.08 18.31 14.72 15.06 14.54 16.57 16.58 18.94 18.74 22.99 17.44 16.64 15.77 18.24 16.52 26.25 15.55 15.80 | 8.34 10.00 7.61 9.94 6.73 12.20 10.25 14.20 7.62 9.14 5.21 5.65 −0.77 11.50 8.53 8.43 1.52 9.59 −7.56 9.79 9.13 |
| Average | 21.58 | 20.01 | 1.56 | 24.83 | 17.40 | 7.44 |
References
- Bartlett, J.G. Clostridium difficile-associated Enteric Disease. Curr. Infect. Dis. Rep. 2002, 4, 477–483. [Google Scholar] [CrossRef]
- Heinlen, L.; Ballard, J.D. Clostridium difficile infection. Am. J. Med. Sci. 2010, 340, 247–252. [Google Scholar] [CrossRef]
- Vedantam, G.; Clark, A.; Chu, M.; McQuade, R.; Mallozzi, M.; Viswanathan, V.K. Clostridium difficile infection: Toxins and non-toxin virulence factors, and their contributions to disease establishment and host response. Gut Microbes 2012, 3, 121–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, L.C.; Owings, M.; Jernigan, D.B. Clostridium difficile infection in patients discharged from US short-stay hospitals, 1996-2003. Emerg. Infect. Dis. 2006, 12, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Simor, A.E.; Bradley, S.F.; Strausbaugh, L.J.; Crossley, K.; Nicolle, L.E.; SHEA Long-Term–Care Committee. Clostridium difficile in long-term-care facilities for the elderly. Infect. Control Hosp. Epidemiol. 2002, 23, 696–703. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.C.; Mu, Y.; Dumyati, G.K.; Farley, M.M.; Winston, L.G.; Johnston, H.L.; Meek, J.I.; Perlmutter, R.; Holzbauer, S.M.; Beldavs, Z.G.; et al. Burden of Nursing Home-Onset Clostridium difficile Infection in the United States: Estimates of Incidence and Patient Outcomes. Open Forum Infect. Dis. 2016, 3, ofv196. [Google Scholar] [CrossRef]
- Starr, J. Clostridium difficile associated diarrhoea: Diagnosis and treatment. BMJ 2005, 331, 498–501. [Google Scholar] [CrossRef] [Green Version]
- Caliendo, A.M.; Gilbert, D.N.; Ginocchio, C.C.; Hanson, K.E.; May, L.; Quinn, T.C.; Tenover, F.C.; Alland, D.; Blaschke, A.J.; Bonomo, R.A.; et al. Better tests, better care: Improved diagnostics for infectious diseases. Clin. Infect. Dis. 2013, 57 (Suppl. 3), S139–S170. [Google Scholar] [CrossRef] [Green Version]
- Delmee, M.; Van Broeck, J.; Simon, A.; Janssens, M.; Avesani, V. Laboratory diagnosis of Clostridium difficile-associated diarrhoea: A plea for culture. J. Med. Microbiol. 2005, 54, 187–191. [Google Scholar] [CrossRef]
- Peterson, L.R.; Robicsek, A. Does my patient have Clostridium difficile infection? Ann. Intern. Med. 2009, 151, 176–179. [Google Scholar] [CrossRef]
- Chapin, K.C.; Dickenson, R.A.; Wu, F.; Andrea, S.B. Comparison of five assays for detection of Clostridium difficile toxin. J. Mol. Diagn. 2011, 13, 395–400. [Google Scholar] [CrossRef]
- She, R.C.; Durrant, R.J.; Petti, C.A. Evaluation of enzyme immunoassays to detect Clostridium difficile toxin from anaerobic stool culture. Am. J. Clin. Pathol. 2009, 131, 81–84. [Google Scholar] [CrossRef]
- Gyorke, C.E.; Wang, S.; Leslie, J.L.; Cohen, S.H.; Solnick, J.V.; Polage, C.R. Evaluation of Clostridium difficile fecal load and limit of detection during a prospective comparison of two molecular tests, the illumigene C. difficile and Xpert C. difficile/Epi tests. J. Clin. Microbiol. 2013, 51, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pancholi, P.; Kelly, C.; Raczkowski, M.; Balada-Llasat, J.M. Detection of toxigenic Clostridium difficile: Comparison of the cell culture neutralization, Xpert C. difficile, Xpert C. difficile/Epi, and Illumigene C. difficile assays. J. Clin. Microbiol. 2012, 50, 1331–1335. [Google Scholar] [CrossRef] [Green Version]
- Brecher, S.M.; Novak-Weekley, S.M.; Nagy, E. Laboratory diagnosis of Clostridium difficile infections: There is light at the end of the colon. Clin. Infect. Dis. 2013, 57, 1175–1181. [Google Scholar] [CrossRef]
- Alfa, M.J.O.N.; Murray, B.L. Fecal specimens for Clostridium difficile Diagnostic Testing are Stable for up to 72 hours at 4 °C. J. Med. Microbiol. Diagn. 2014, 3, 140. [Google Scholar] [CrossRef]
- Arroyo, L.G.; Rousseau, J.; Willey, B.M.; Low, D.E.; Staempfli, H.; McGeer, A.; Weese, J.S. Use of a selective enrichment broth to recover Clostridium difficile from stool swabs stored under different conditions. J. Clin. Microbiol. 2005, 43, 5341–5343. [Google Scholar] [CrossRef] [Green Version]
- Becker, S.L.; Chatigre, J.K.; Coulibaly, J.T.; Mertens, P.; Bonfoh, B.; Herrmann, M.; Kuijper, E.J.; N’Goran, E.K.; Utzinger, J.; von Muller, L. Molecular and culture-based diagnosis of Clostridium difficile isolates from Cote d’Ivoire after prolonged storage at disrupted cold chain conditions. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 660–668. [Google Scholar] [CrossRef] [Green Version]
- Bowman, R.A.; Riley, T.V. Isolation of Clostridium difficile from stored specimens and comparative susceptibility of various tissue culture cell lines to cytotoxin. FEMS Microbiol. Lett. 1986, 34, 31–35. [Google Scholar] [CrossRef]
- Freeman, J.; Wilcox, M.H. The effects of storage conditions on viability of Clostridium difficile vegetative cells and spores and toxin activity in human faeces. J. Clin. Pathol. 2003, 56, 126–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.R.; Young, S.A.; Davis, T.E., Jr.; Wang, Z.X.; Duncan, J.; Noutsios, C.; Liesenfeld, O.; Osiecki, J.C.; Lewinski, M.A. Evaluation of the cobas Cdiff Test for Detection of Toxigenic Clostridium difficile in Stool Samples. J. Clin. Microbiol. 2017, 55, 3426–3436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schora, D.M.; Peterson, L.R.; Usacheva, E.A. Immunological Stability of Clostridium difficile Toxins in Clinical Specimens. Infect. Control Hosp. Epidemiol. 2018, 39, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Weese, J.S.; Staempfli, H.R.; Prescott, J.F. Survival of Clostridium difficile and its toxins in equine feces: Implications for diagnostic test selection and interpretation. J. Vet. Diagn. Investig. 2000, 12, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect. Control Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef]
- Recommended Protocol for Testing for Clostridium difficile and Subsequent Culture. Health Protection Scotland 2016. Available online: https://www.hps.scot.nhs.uk/web-resources-container/recommended-protocol-for-testing-for-clostridium-difficile-and-subsequent-culture/ (accessed on 14 June 2021).
- Edwards, A.N.; Suarez, J.M.; McBride, S.M. Culturing and maintaining Clostridium difficile in an anaerobic environment. J. Vis. Exp. 2013, 50787. [Google Scholar] [CrossRef]
- Surawicz, C.M.; Brandt, L.J.; Binion, D.G.; Ananthakrishnan, A.N.; Curry, S.R.; Gilligan, P.H.; McFarland, L.V.; Mellow, M.; Zuckerbraun, B.S. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am. J. Gastroenterol. 2013, 108, 478–498. [Google Scholar] [CrossRef] [PubMed]
- Kilic, A.; Alam, M.J.; Tisdel, N.L.; Shah, D.N.; Yapar, M.; Lasco, T.M.; Garey, K.W. Multiplex Real-Time PCR Method for Simultaneous Identification and Toxigenic Type Characterization of Clostridium difficile From Stool Samples. Ann. Lab. Med. 2015, 35, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armbruster, D.A.; Pry, T. Limit of blank, limit of detection and limit of quantitation. Clin. Biochem. Rev. 2008, 29 (Suppl. 1), S49–S52. [Google Scholar]



| Article Classified in | Number of Articles | Citations | Citations Per Article | ||
|---|---|---|---|---|---|
| Target | Test Method 1 | ||||
| Cell/spore | Viability Cell count | TC TC | 7 1 | 280 92 | 40.0 92.0 |
| Protein | TcdA/B GDH | CCCNA EIA GDH assay | 3 2 2 | 260 67 5 | 86.7 33.5 2.5 |
| DNA | tcdA/B | NAAT | 1 | 3 | 3.0 |
| Sum | 707 | ||||
| Experiment | Bowman and Riley (1986) [19] | Weese et al. (2000) [23] | Freeman and Wilcox (2003) [20] | Arroyo et al. (2005) [17] | Alfa et al. (2014) [16] | Becker et al. (2015) [18] | Peterson et al. (2017) [21] | Schora et al. (2018) [22] | This Study |
|---|---|---|---|---|---|---|---|---|---|
| Storage condition | |||||||||
|
|
|
|
|
|
|
|
|
|
| Toxigenic culture | |||||||||
|
|
|
|
|
|
|
| N/A |
|
| N/A | N/A |
| N/A | N/A | N/A | N/A | N/A |
|
| Protein-based | |||||||||
|
| N/A |
| N/A |
| N/A | N/A | N/A | N/A |
| N/A |
| N/A | N/A | N/A | N/A | N/A |
| |
| N/A | N/A | N/A | N/A |
|
| N/A | N/A | N/A |
| DNA-based | |||||||||
| N/A | N/A | N/A | N/A | N/A | N/A |
| N/A |
|
| Primer | Sequence | Target |
|---|---|---|
| Designed in this study | ||
| tcdA-7582F tcdA-7784R tcdB-3005F tcdB-3161R | CCTGATGGATTTGAATACTTTGC CCATTCGCACCCATAGCTGTA CAGATGCAGCCAAAGTTGTTGA GGGTCACTCGTTTCACTTAGC | tcdA tcdA tcdB tcdB |
| Reference primers used by Kilic et al (2015) [28] | ||
| F R F R | TGATAACGTATAGCTTGACC ATGGTTTACCTCAGATAGG GAAGGATTACCTGTAATTGC CTGCCATTATACCTATCTTAGC | tcdA tcdA tcdB tcdB |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nho, S.W.; Kim, M.; Kim, S.-J.; Foley, S.L.; Nayak, R.; Kweon, O.; Cerniglia, C.E. Pragmatic Strategy for Fecal Specimen Storage and the Corresponding Test Methods for Clostridioides difficile Diagnosis. Pathogens 2021, 10, 1049. https://doi.org/10.3390/pathogens10081049
Nho SW, Kim M, Kim S-J, Foley SL, Nayak R, Kweon O, Cerniglia CE. Pragmatic Strategy for Fecal Specimen Storage and the Corresponding Test Methods for Clostridioides difficile Diagnosis. Pathogens. 2021; 10(8):1049. https://doi.org/10.3390/pathogens10081049
Chicago/Turabian StyleNho, Seong Won, Minjae Kim, Seong-Jae Kim, Steven L. Foley, Rajesh Nayak, Ohgew Kweon, and Carl E. Cerniglia. 2021. "Pragmatic Strategy for Fecal Specimen Storage and the Corresponding Test Methods for Clostridioides difficile Diagnosis" Pathogens 10, no. 8: 1049. https://doi.org/10.3390/pathogens10081049