
Determinants of HIV-1 Late Presentation in Patients Followed in Europe

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of European Population
2.2. Determinants Associated with Late Presentation
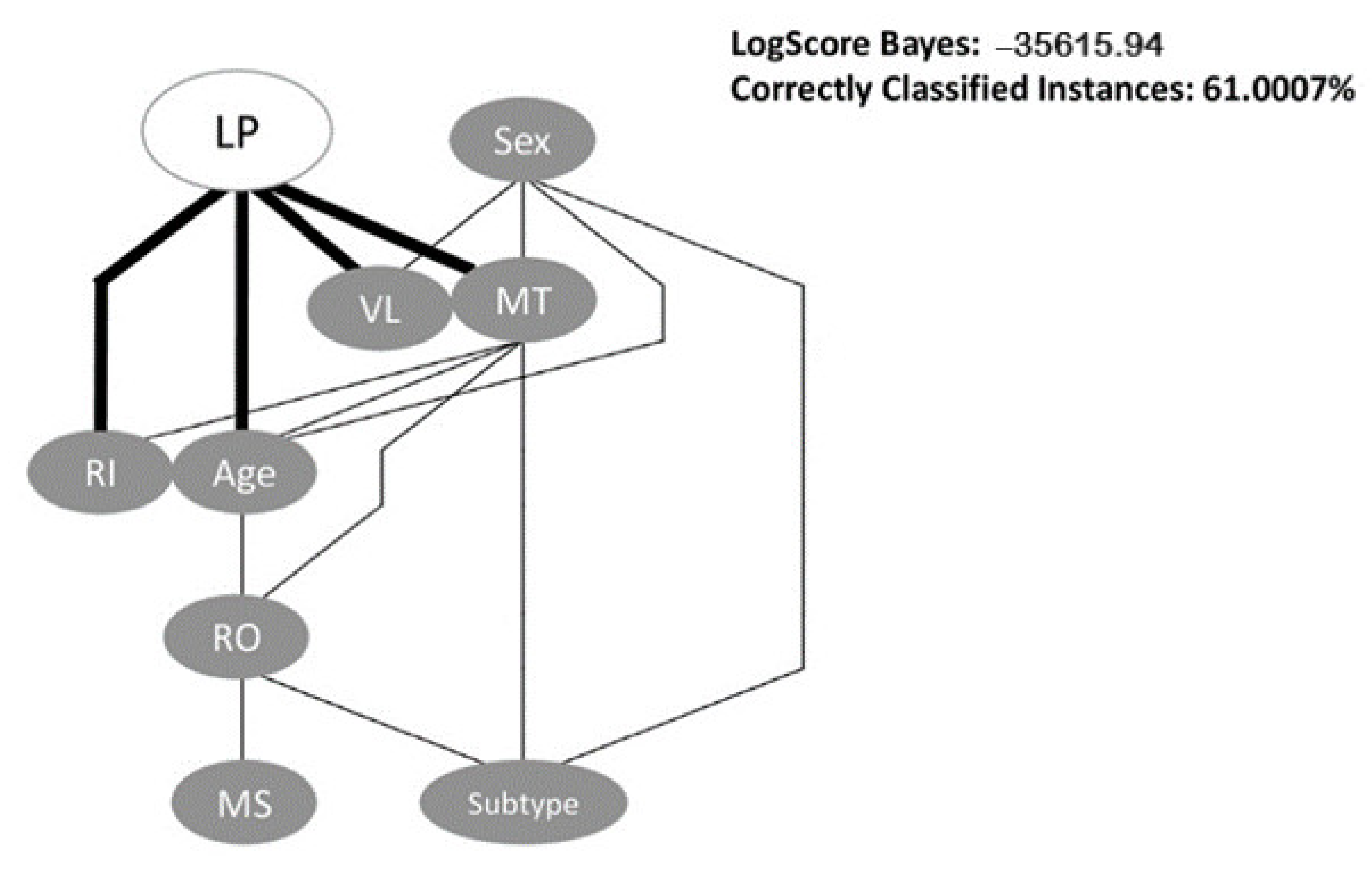
2.3. Bayesian Network
2.4. Ambiguity Rate and CD4 Analysis
2.5. Analysis of Late Presenters Rate over Time
3. Discussion
4. Materials and Methods
4.1. Study Group
4.2. Subtyping
4.3. Study Variables
- Migrant/Native-Based on Country of Origin and Country of Follow-up (if country of origin and country of follow-up is the same, then patient is native; if country of origin and country of follow-up is not the same, then patient is migrant)
- Age at Diagnosis-Based on the difference between Year of Birth and Date of the first HIV Positive test;
- Region of Origin- Based on Country of Origin;
- Treatment Status at date of first CD4 count-Based on the difference between sample collection date of first CD4 count and first therapy date; for purposes of classification of Late Presentation, only patients naïve at date of first CD4 count were considered;
- Treatment Status at date of first Drug Resistance Test-based on the difference between sample collection date for first drug resistance test and date of start of first therapy;
- Recentness of infection-Based on ambiguity rate of genomic sequences. We defined Chronic infection as an ambiguity value higher than 0.45% and Recent infection as an ambiguity value equal or below 0.45% [36]. Additionally, only genomic sequences larger than 500 nucleotides and with ambiguity rate lower than 2.5% were considered.
- LP vs. NLP- Based on CD4 count, LP were defined as patients with CD4 count lower than 350 cells/mm3 and NLP were defined as patients with CD4 count higher than 350 cells/mm3.
4.4. Statistical Analysis
4.5. Bayesian Networks
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| CD4 Count | R2 | Unstandardized B | Standardized Coefficients Beta | p-Value | 95% Confidence Interval for B | Spearman’s Correlation | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bond | p-Value | Correlation Coefficient | |||||
| Ambiguity Rate | 0.023 | −69.52 | −0.152 | <0.001 | −74.61 | −64.44 | <0.001 | −0.190 |
| CD4 Count | R2 | Unstandardized B | Standardized Coefficients Beta | p-Value | 95% Confidence Interval for B | Spearman’s Correlation | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bond | p-Value | Correlation Coefficient | |||||
| Ambiguity Rate | 0.015 | −57.11 | −0.123 | <0.001 | −63.27 | −50.95 | <0.001 | −0.159 |
| CD4 Count | R2 | Unstandardized B | Standardized Coefficients Beta | p-Value | 95% Confidence Interval for B | Spearman’s Correlation | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bond | p-Value | Correlation Coefficient | |||||
| Ambiguity Rate | 0.051 | −96.72 | −0.226 | <0.001 | −105.54 | −87.91 | <0.001 | −0.265 |
| CD4 Count | R2 | Unstandardized B | Standardized Coefficients Beta | p-Value | 95% Confidence Interval for B | Spearman’s Correlation | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bond | p-Value | Correlation Coefficient | |||||
| Ambiguity Rate | 0.014 | −52.78 | −0.120 | <0.001 | −73.38 | −32.17 | <0.001 | −0.144 |
References
- WHO. HIV/AIDS. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids. (accessed on 4 January 2021).
- Global HIV & AIDS Statistics — 2020 Fact Sheet | UNAIDS. Available online: https://www.unaids.org/en/resources/fact-sheet. (accessed on 4 January 2021).
- Understanding Fast-Track. Available online: https://www.unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf. (accessed on 18 May 2020).
- Guaraldi, G.; Zona, S.; Menozzi, M.; Brothers, T.D.; Carli, F.; Stentarelli, C.; Dolci, G.; Santoro, A.; Da Silva, A.R.D.; Rossi, E.; et al. Late presentation increases risk and costs of non-infectious comorbidities in people with HIV: An Italian cost impact study. AIDS Res. Ther. 2017, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Conway, A.S.; Esteve, A.; Fernández-Quevedo, M.; Casabona, J. Determinants and Outcomes of Late Presentation of HIV Infection in Migrants in Catalonia, Spain: PISCIS Cohort 2004–2016. J. Immigr. Minor. Health 2018, 21, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Gesesew, H.A.; Ward, P.; Woldemichael, K.; Mwanri, L. Late presentation for HIV care in Southwest Ethiopia in 2003–2015: Prevalence, trend, outcomes and risk factors. BMC Infect. Dis. 2018, 18, 59. [Google Scholar] [CrossRef] [Green Version]
- Antinori, A.; Coenen, T.; Costagiola, D.; Dedes, N.; Ellefson, M.; Gatell, J.; Girardi, E.; Johnson, M.; Kirk, O.; Lundgren, J.; et al. Late presentation of HIV infection: A consensus definition. HIV Med. 2010, 12, 61–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Late Presentation Working Groups in EuroSIDA and COHERE. Estimating the burden of HIV late presentation and its attributable morbidity and mortality across Europe 2010–2016. BMC Infect. Dis. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Hu, X.; Liang, B.; Zhou, C.; Jiang, J.; Huang, J.; Ning, C.; Liu, J.; Zhou, B.; Zang, N.; Lai, J.; et al. HIV late presentation and advanced HIV disease among patients with newly diagnosed HIV/AIDS in Southwestern China: A large-scale cross-sectional study. AIDS Res. Ther. 2019, 16, 6. [Google Scholar] [CrossRef]
- Luma, H.N.; Jua, P.; Donfack, O.-T.; Kamdem, F.; Ngouadjeu, E.; Mbatchou, H.B.; Doualla, M.-S.; Mapoure, Y.N. Late presentation to HIV/AIDS care at the Douala general hospital, Cameroon: Its associated factors, and consequences. BMC Infect. Dis. 2018, 18, 298. [Google Scholar] [CrossRef] [Green Version]
- Wilton, J.; Light, L.; Gardner, S.; Rachlis, B.; Conway, T.; Cooper, C.; Cupido, P.; Kendall, C.E.; Loutfy, M.; McGee, F.; et al. Late diagnosis, delayed presentation and late presentation among persons enrolled in a clinical HIV cohort in Ontario, Canada (1999–2013). HIV Med. 2019, 20, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Frank, E.; Holmes, G.; Pfahringer, B.; Reutemann, P.; Witten, I.H. The WEKA Data Mining Software: An Update. SIGKDD Explor. 2009, 11, 10–18. [Google Scholar] [CrossRef]
- Chkhartishvili, N.; Chokoshvili, O.; Bolokadze, N.; Tsintsadze, M.; Sharvadze, L.; Gabunia, P.; Dvali, N.; Abutidze, A.; Tsertsvadze, T. Late presentation of HIV infection in the country of Georgia: 2012–2015. PLOS ONE 2017, 12, e0186835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infographic: HIV Infection - Late Diagnosis. Available online: https://www.ecdc.europa.eu/en/publications-data/infographic-hiv-infection-late-diagnosis (accessed on 4 January 2021).
- Darling, K.E.; Hachfeld, A.; Cavassini, M.; Kirk, O.; Furrer, H.; Wandeler, G. Late presentation to HIV care despite good access to health services: Current epidemiological trends and how to do better. Swiss Med. Wkly. 2016, 146, 14348. [Google Scholar] [CrossRef] [Green Version]
- Wójcik-Cichy, K.; Jabłonowska, O.; Piekarska, A.; Jabłonowska, E. The high incidence of late presenters for HIV/AIDS infection in the Lodz province, Poland in the years 2009–2016: We are still far from the UNAIDS 90% target. AIDS Care 2018, 30, 1538–1541. [Google Scholar] [CrossRef]
- Van Opstal, S.E.M.; Van Der Zwan, J.S.; Wagener, M.N.; Been, S.K.; Miedema, H.S.; Roelofs, P.; Van Gorp, E.C.M. Late Presentation of HIV Infection in the Netherlands: Reasons for Late Diagnoses and Impact on Vocational Functioning. AIDS Behav. 2018, 22, 2593–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bath, R.E.; Emmett, L.; Verlander, N.Q.; Reacher, M. Risk factors for late HIV diagnosis in the East of England: Evidence from national surveillance data and policy implications. Int. J. STD AIDS 2018, 30, 37–44. [Google Scholar] [CrossRef]
- Fakoya, I.; Arco, D.; Álvarez, D.; Copas, A.J.; Teixeira, B.; Block, K.; Gennotte, A.-F.; Volny-Anne, A.; Bil, J.P.; Touloumi, G.; et al. Factors Associated With Access to HIV Testing and Primary Care Among Migrants Living in Europe: Cross-Sectional Survey. JMIR Public Health Surveill. 2017, 3, 84. [Google Scholar] [CrossRef] [PubMed]
- MacCarthy, S.; Brignol, S.; Reddy, M.; Nunn, A.; Dourado, I. Late presentation to HIV/AIDS care in Brazil among men who self-identify as heterosexual. Revista de Saúde Pública 2016, 50, 54. [Google Scholar] [CrossRef]
- Ross, J.; Cunningham, C.O.; Hanna, D.B. HIV outcomes among migrants from low-income and middle-income countries living in high-income countries. Curr. Opin. Infect. Dis. 2018, 31, 25–32. [Google Scholar] [CrossRef]
- Pimentel, V.; Pingarilho, M.; Alves, D.; Diogo, I.; Fernandes, S.; Miranda, M.; Pineda-Pena, A.-C.; Libin, P.; Martins, M.R.O.; Vandamme, A.-M.; et al. Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017. Viruses 2020, 12, 268. [Google Scholar] [CrossRef] [Green Version]
- Hachfeld, A.; Darling, K.; Calmy, A.; Ledergerber, B.; Weber, R.; Battegay, M.; Wissel, K.; Di Benedetto, C.; Fux, C.; E Tarr, P.; et al. Why do sub-Saharan Africans present late for HIV care in Switzerland? HIV Med. 2019, 20, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Suárez-García, I.; Sobrino-Vegas, P.; Dalmau, D.; Rubio, R.; Iribarren, J.A.; Blanco, J.R.; Gutierrez, F.; Alonso, M.M.; Bernal, E.; García, D.V.; et al. Clinical outcomes of patients infected with HIV through use of injected drugs compared to patients infected through sexual transmission: Late presentation, delayed anti-retroviral treatment and higher mortality. Addiction 2016, 111, 1235–1245. [Google Scholar] [CrossRef]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, 1192–1207. [Google Scholar] [CrossRef] [Green Version]
- Balayan, T.; Oprea, C.; Yurin, O.; Jevtović, Đ.; Begovac, J.; Lakatos, B.; Sedlacek, D.; Karpov, I.; Horban, A.; Kowalska, J.D.; et al. People who inject drugs remain hard-to-reach population across all HIV continuum stages in Central, Eastern and South Eastern Europe – data from Euro-guidelines in Central and Eastern Europe Network. Infect. Dis. 2019, 51, 277–286. [Google Scholar] [CrossRef]
- Lunar, M.M.; Lepej Židovec, S.; Poljak, M. Sequence ambiguity determined from routine pol sequencing is a reliable tool for real-time surveillance of HIV incidence trends. Infect. Genet. Evol. 2019, 69, 146–152. [Google Scholar] [CrossRef]
- Darcis, G.; Lambert, I.; Sauvage, A.-S.; Frippiat, F.; Meuris, C.; Uurlings, F.; LeComte, M.; Léonard, P.; Giot, J.-B.; Fombellida, K.; et al. Factors associated with late presentation for HIV care in a single Belgian reference center: 2006–2017. Sci. Rep. 2018, 8, 8594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mocroft, A.; Lundgren, J.D.; Sabin, M.; Monforte, A.D.; Brockmeyer, N.N.; Casabona, J.J.; Castagna, A.; Costagliola, D.; Dabis, F.; De Wit, S.; et al. Risk Factors and Outcomes for Late Presentation for HIV-Positive Persons in Europe: Results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE). PLoS Med. 2013, 10, e1001510. [Google Scholar] [CrossRef] [Green Version]
- Mocroft, A.; Lundgren, J.D.; Antinori, A.; Ad, M. The late presenters working group in COHERE in EuroCoord Late presentation for HIV care across Europe: Update from the Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study, 2010 to 2013. Eurosurveillance 2015, 20, 30070. [Google Scholar] [CrossRef] [Green Version]
- Euresist Data Analysis—Database. Available online: http://engine.euresist.org/database/ (accessed on 4 January 2021).
- Lawyer, G.; Altmann, A.; Thielen, A.; Zazzi, M.; Sönnerborg, A.; Lengauer, T. HIV-1 mutational pathways under multidrug therapy. AIDS Res. Ther. 2011, 8, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zazzi, M.; Incardona, F.; Rosen-Zvi, M.; Prosperi, M.; Lengauer, T.; Altmann, A.; Sönnerborg, A.; Lavee, T.; Schülter, E.; Kaiser, R. Predicting Response to Antiretroviral Treatment by Machine Learning: The EuResist Project. Intervirology 2012, 55, 123–127. [Google Scholar] [CrossRef]
- Pineda-Peña, A.-C.; Faria, N.R.; Imbrechts, S.; Libin, P.; Abecasis, A.; Deforche, K.; Gómez-López, A.; Camacho, R.; de Oliveira, T.; Vandamme, A.-M. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: Performance evaluation of the new REGA version 3 and seven other tools. Infect. Genet. Evol. 2013, 19, 337–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Struck, D.; Lawyer, G.; Ternes, A.-M.; Schmit, J.-C.; Bercoff, D.P. COMET: Adaptive context-based modeling for ultrafast HIV-1 subtype identification. Nucleic Acids Res. 2014, 42, e144. [Google Scholar] [CrossRef] [PubMed]
- Andersson, E.; Shao, W.; Bontell, I.; Cham, F.; Cuong, D.D.; Wondwossen, A.; Morris, L.; Hunt, G.; Sönnerborg, A.; Bertagnolio, S.; et al. Evaluation of sequence ambiguities of the HIV-1 pol gene as a method to identify recent HIV-1 infection in transmitted drug resistance surveys. Infect. Genet. Evol. 2013, 18, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sesen, M.B.; Nicholson, A.E.; Banares-Alcantara, R.; Kadir, T.; Brady, M. Bayesian Networks for Clinical Decision Support in Lung Cancer Care. PLoS ONE 2013, 8, e82349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, Y.; Sahoo, G. Analysis of Parametric & Non Parametric Classifiers for Classification Technique using WEKA. Int. J. Inf. Technol. Comput. Sci. 2012, 4, 43–49. [Google Scholar] [CrossRef] [Green Version]



| Patient Characteristics | Total | Late Presenters | Non-Late Presenters | p-Value |
|---|---|---|---|---|
| Total, n (%) | 89,851 (100%) | 28,889 (50.4%) | 28,388 (49.6%) | |
| Sex, n (%) | 81,777 (91.0%) | 27,972 (50.6%) | 27,315 (49.4%) | <0.001 |
| Male | 60,852 (74.4%) | 20,955 (74.9%) | 20,969 (76.8%) | |
| Female | 20,925 (25.6%) | 7017 (25.1%) | 6346 (23.2%) | |
| Treatment status, n (%) | 19,605 (21.8%) | 10,905 (55.6%) | 8700 (44.4%) | <0.001 |
| Naïve | 11,487(58.6%) | 6040 (55.4%) | 5447 (62.6%) | |
| Treated | 8118 (41.4%) | 4865 (44.6%) | 3253 (37.4%) | |
| Median age at diagnosis in years IQR, n (%) | 25,530 (28.4%) | 11,929 (52.3%) | 10,897 (47.7%) | <0.001 |
| 33.0 (27.0–41.0) | 34.0 (28.0–43.0) | 31.0 (26.0–39.0) | ||
| ≤18 | 700 (2.7%) | 241 (2.0%) | 340 (3.1%) | <0.001 |
| 19–30 | 9767 (38.3%) | 4002 (33.5%) | 4823 (44.3%) | |
| 31–55 | 13,815 (54.1%) | 6920 (58.0%) | 5384 (49.4%) | |
| ≥56 | 1248 (4.9%) | 766 (6.4%) | 350 (3.2%) | |
| Mode of transmission, n (%) | 47,007 (52.3%) | 21,283 (49.5%) | 21,677 (50.5%) | <0.001 |
| Heterosexual | 15,165 (32.3%) | 7894 (37.1%) | 6071 (28.0%) | |
| MSM | 19,696 (41.9%) | 7657 (36.0%) | 10,693 (49.3%) | |
| IDU | 9532 (20.3%) | 4453 (20.9%) | 3896 (18.0%) | |
| Other | 2614 (5.6%) | 1279 (6.0%) | 1017 (4.7%) | |
| Region of origin, n (%) | 54,529 (60.7%) | 21,584 (50.1%) | 21,495 (49.9%) | <0.001 |
| Western Europe | 42,790 (78.5%) | 16,693 (77.4%) | 17,398 (81.0%) | |
| Eastern Europe | 1862 (3.4%) | 693 (3.2%) | 672 (3.1%) | |
| Africa | 5349 (9.8%) | 2250 (10.4%) | 1422 (6.6%) | |
| South America | 3233 (5.9%) | 1341 (6.2%) | 1460 (6.8%) | |
| Other | 1286 (2.4%) | 607 (2.8%) | 543 (2.5%) | |
| Subtype, n (%) | 54,176 (60.3%) | 17,449 (52.7%) | 15,638 (47.3%) | <0.001 |
| HIV-1 Subtype B | 35,454 (64.4%) | 11,966 (68.6%) | 11,745 (75.1%) | |
| HIV-1 Subtype non-B | 18,722 (34.6%) | 5483 (31.4%) | 3893 (24.9%) | |
| Distribution of non-B Subtypes | ||||
| HIV-1 CRF 01_AE | 447 (2.4%) | 183 (3.3%) | 108 (2.8%) | |
| HIV-1 CRF 02_AG | 2973 (15.9%) | 871 (15.9%) | 556 (14.3%) | |
| HIV-1 CRF 06_cpx | 248 (1.3%) | 81 (1.5%) | 58 (1.5%) | |
| HIV-1 CRF 14_BG | 1106 (5.9%) | 337 (6.1%) | 203 (5.2%) | |
| HIV-1 Subtype A | 2521 (13.5%) | 626 (11.4%) | 527 (13.5%) | |
| HIV-1 Subtype C | 1943 (10.4%) | 550 (10.0%) | 400 (10.3%) | |
| HIV-1 Subtype D | 307 (1.6%) | 102 (1.9%) | 74 (1.9%) | |
| HIV-1 Subtype F | 1619 (8.6%) | 444 (8.1%) | 362 (9.3%) | |
| HIV-1 Subtype G | 3815 (20.4%) | 1156 (21.1%) | 701 (28.0%) | |
| Others | 3743 (20.0%) | 1133 (20.7%) | 3893 (23.2%) | |
| Migrant status, n (%) | 54,520 (60.7%) | 21,584 (50.1%) | 21,495 (49.9%) | <0.001 |
| Migrant | 13,408 (24.6%) | 5588 (25.9%) | 4895 (22.8%) | |
| Native | 41,112 (75.4%) | 15,996 (74.1%) | 16,600 (77.2%) | |
| Recentness of infection, n (%) | 50,132 (55.8%) | 15,897 (52.6%) | 14,304 (47.4%) | <0.001 |
| Chronic | 29,972 (59.8%) | 11,069 (69.6%) | 7803 (54.6%) | |
| Recent | 20,160 (40.2%) | 4828 (30.4%) | 6501 (45.4%) | |
| Median CD4 count at diagnosis (cells/mL) IQR, n (%) | 57,277 (63.7%) | 28,889 (50.4%) | 28,388 (49.6%) | <0.001 |
| 348.0 (170.0–548.0) | 172.0 (69.0–264.0) | 550.0 (442.0–720.0) | ||
| Viral Load at diagnosis (log10 copies/mL) IQR, n (%) | 34,046 (37.9%) | 15,106 (50.8%) | 14,605 (49.2%) | <0.001 |
| 4.4 (3.4–5.1) | 4.7 (3.8–5.3) | 4.1 (3.1–4.8) | ||
| ≤4.0 | 12,994 (38.2%) | 4485 (29.7%) | 6819 (46.7%) | <0.001 |
| 4.1–5.0 | 11,715 (34.4%) | 5034 (33.3%) | 5295 (36.3%) | |
| ≥5.1 | 9337 (27.4%) | 5587 (37.0%) | 2491 (17.1%) |
| Late Presenters/ Non-Late Presenters | Unadjusted | Final Model | ||
|---|---|---|---|---|
| Variable | OR (95%CI) | p-Value | aOR (95%CI) | p-Value |
| Sex | ||||
| Female | Ref | Ref | Ref | Ref |
| Male | 0.90 (0.87–0.94) | <0.001 | 1.05 (0.91–1.21) | 0.522 |
| Age at diagnosis | 1.03 (1.02–1.03) | <0.001 | ||
| Age groups | ||||
| <18 | 0.55 (0.47–0.65) | <0.001 | 0.48 (0.33–0.69) | <0.001 |
| 19–30 | 0.65 (0.61–0.68) | <0.001 | 0.70 (0.63–0.79) | <0.001 |
| 31–55 | Ref | Ref | Ref | Ref |
| >56 | 1.70 (1.49–1.94) | <0.001 | 1.54 (1.15–2.06) | 0.004 |
| Mode of transmission | ||||
| Heterosexual | Ref | Ref | Ref | Ref |
| MSM | 0.55 (0.53–0.58) | <0.001 | 0.74 (0.64–0.86) | <0.001 |
| IDU | 0.88 (0.83–0.93) | <0.001 | 1.12 (0.96–1.31) | 0.137 |
| Other | 0.97 (0.88–1.06) | 0.462 | 1.29 (0.99–1.70) | 0.062 |
| Region of Origin | ||||
| Western Europe | Ref | Ref | Ref | Ref |
| Eastern Europe | 1.08 (0.97–1.20) | 0.191 | 1.07 (0.78–1.48) | 0.683 |
| Africa | 1.65 (1.54–1.77) | <0.001 | 1.76 (1.37–2.26) | <0.001 |
| South America | 0.96 (0.89–1.03) | 0.267 | 1.41 (1.07–1.87) | 0.015 |
| Other | 1.17 (1.04–1.31) | 0.011 | 1.39 (0.92–2.09) | 0.118 |
| Subtype | ||||
| HIV-1 Subtype B | Ref | Ref | ||
| HIV-1 Subtype non-B | 1.38 (1.32–1.45) | <0.001 | ||
| Migrant Status | ||||
| Migrant | Ref | Ref | ||
| Native | 0.84 (0.81–0.88) | <0.001 | ||
| Recentness of infection | ||||
| Chronic | Ref | Ref | Ref | Ref |
| Recent | 0.52 (0.50–0.55) | <0.001 | 0.61 (0.55–0.68) | <0.001 |
| Log Viral load at diagnosis | 1.45 (1.42–1.48) | <0.001 | ||
| Log Viral load groups | ||||
| <4.0 | Ref | Ref | Ref | Ref |
| 4.1–5.0 | 1.45 (1.37–1.53) | <0.001 | 1.37 (1.22–1.55) | <0.001 |
| >5.1 | 3.41 (3.21–3.62) | <0.001 | 3.41 (2.96–3.91) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, M.N.S.; Pingarilho, M.; Pimentel, V.; Martins, M.d.R.O.; Vandamme, A.-M.; Bobkova, M.; Böhm, M.; Seguin-Devaux, C.; Paredes, R.; Rubio, R.; et al. Determinants of HIV-1 Late Presentation in Patients Followed in Europe. Pathogens 2021, 10, 835. https://doi.org/10.3390/pathogens10070835
Miranda MNS, Pingarilho M, Pimentel V, Martins MdRO, Vandamme A-M, Bobkova M, Böhm M, Seguin-Devaux C, Paredes R, Rubio R, et al. Determinants of HIV-1 Late Presentation in Patients Followed in Europe. Pathogens. 2021; 10(7):835. https://doi.org/10.3390/pathogens10070835
Chicago/Turabian StyleMiranda, Mafalda N. S., Marta Pingarilho, Victor Pimentel, Maria do Rosário O. Martins, Anne-Mieke Vandamme, Marina Bobkova, Michael Böhm, Carole Seguin-Devaux, Roger Paredes, Rafael Rubio, and et al. 2021. "Determinants of HIV-1 Late Presentation in Patients Followed in Europe" Pathogens 10, no. 7: 835. https://doi.org/10.3390/pathogens10070835