
Epidemiological Aspects of Maternal and Congenital Toxoplasmosis in Panama

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Seroprevalence of T. gondii Infection in Pregnant Women and Newborns
2.2. Risk Factors Associated with T. gondii Infection
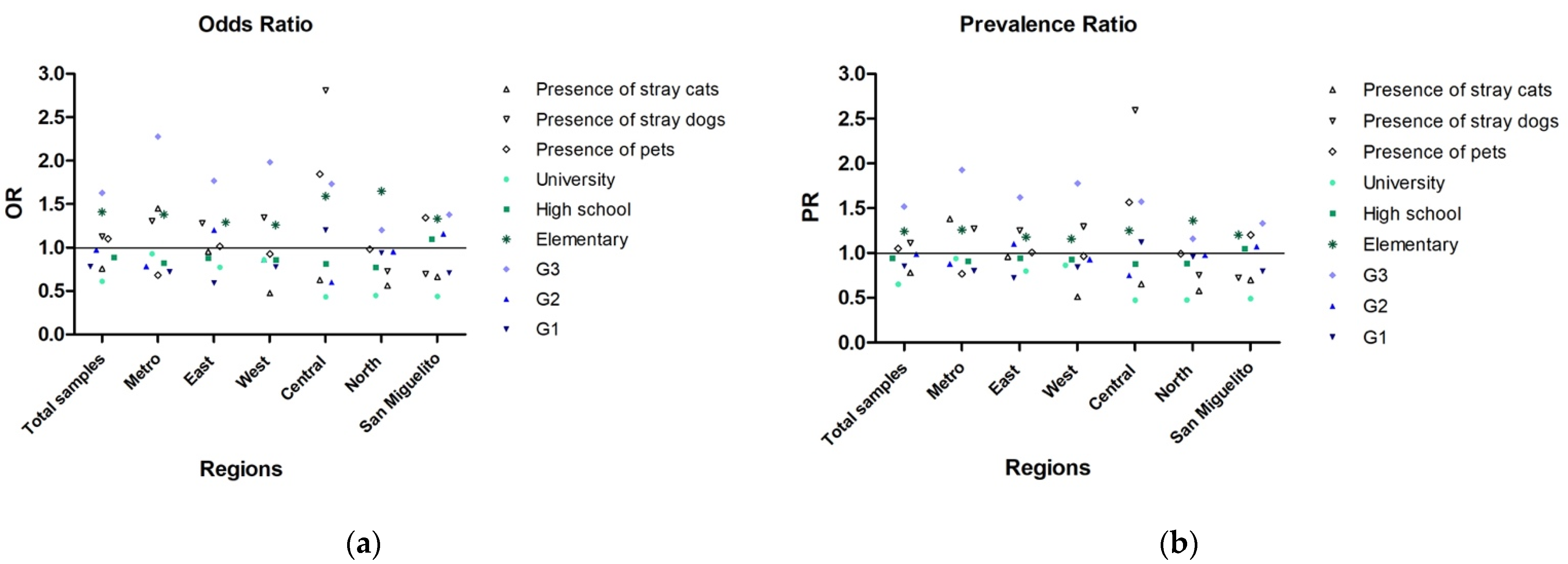
2.3. Association between Exposure to a Risk Factor and the Occurrence of the Disease
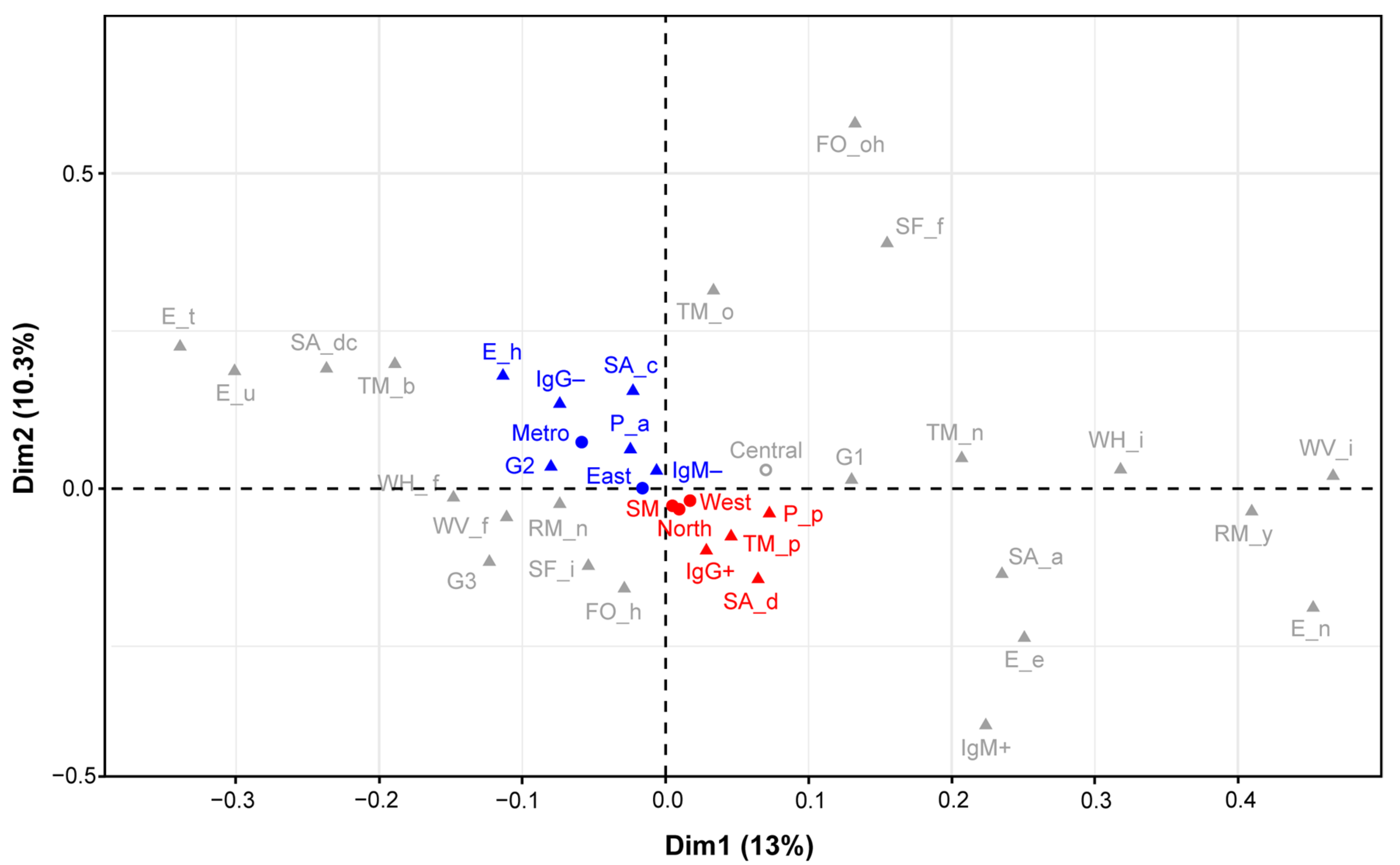
2.4. Relationship Patterns between Different Risk Factors and T. gondii Infection
3. Discussion
4. Materials and Methods
4.1. The Ethics Statement
4.2. Experimental Design
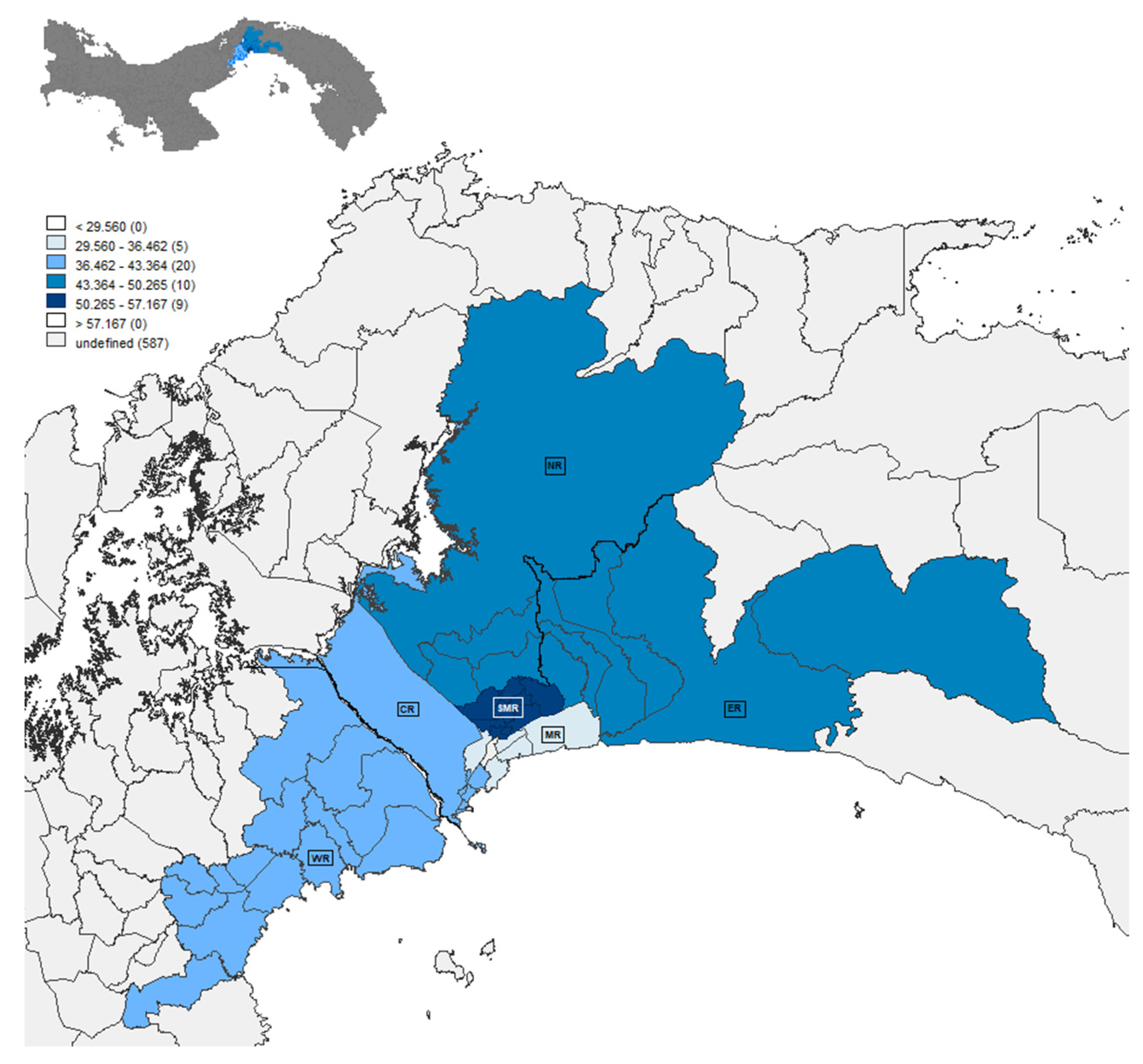
4.3. Geographical Area Studied
4.4. Data Collection and Survey Application
4.5. Sample Collection
4.5.1. Peripheral Blood
4.5.2. Placental Samples
4.5.3. Cerebrospinal Fluid in the Newborns
4.6. Serological and Molecular Diagnosis
4.6.1. Detection of anti-T. gondii Antibodies in Serum Samples
4.6.2. Detection of T. gondii Infection in Placental Samples
4.6.3. Detection of T. gondii Infection in Cerebrospinal Fluid Samples from Newborns
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torgerson, P.R.; Mastroiacovo, P. The global burden of congenital toxoplasmosis: A systematic review. Bull. World Heal. Organ. 2013, 91, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Mareze, M.; Benitez, A.D.N.; Brandão, A.P.D.; Pinto-Ferreira, F.; Miura, A.C.; Martins, F.D.C.; Caldart, E.T.; Biondo, A.W.; Freire, R.L.; Mitsuka-Breganó, R.; et al. Socioeconomic vulnerability associated to Toxoplasma gondii exposure in southern Brazil. PLoS ONE 2019, 14, e0212375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reátegui, C.B.; Vela, L.G. The relation between socioeconomic-epidemiologic factors and seroprevalence of Toxoplasmosis in pregnant women at the Hospital. Neotrop. Helminthol. 2011, 5, 31–40. [Google Scholar]
- Redmond, E.C.; Griffith, C.J. Consumer food handling in the home: A review of food safety studies. J. Food. Prot. 2003, 66, 130–161. [Google Scholar] [CrossRef]
- Thrane, N.; Søndergaard, C.; Schønheyder, H.C.; Sørensen, H.T. Socioeconomic factors and risk of hospitalization with infectious diseases in 0- to 2-year-old Danish children. Eur. J. Epidemiol. 2005, 20, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Unicomb, E.L. Food safety: Pathogen transmission routes, hygiene practices and prevention. J. Heal. Popul. Nutr. 2009, 27, 599–601. [Google Scholar] [CrossRef] [Green Version]
- Alvarado-Esquivel, C.; Terrones-Saldívar, M.d.C.; Hernández-Tinoco, J.; Muñoz-Terrones, M.D.E.; Gallegos-González, R.O.; Sánchez-Anguiano, L.F.; Reyes-Robles, M.E.; Jaramillo-Juárez, F.; Liesenfeld, O.; Estrada-Martínez, S. Seroepidemiology of Toxoplasma gondii in pregnant women in Aguascalientes City, Mexico: A cross-sectional study. BMJ Open 2016, 6, e012409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J.L.; Dubey, J.P. Foodborne Toxoplasmosis. Clin. Infect. Dis. 2012, 55, 845–851. [Google Scholar] [CrossRef]
- CDC. Parasites Toxoplasmosis (Toxoplasma Infection). Epidemiology & Risk Factors. Available online: https://www.cdc.gov/parasites/toxoplasmosis/epi.html (accessed on 15 December 2020).
- Macpherson, C.N.L.; Bidaisee, S. 4-Role of Society and Culture in the Epidemiology and Control of Foodborne Parasites. In Foodborne Parasites in the Food Supply Web, 1st ed.; Gajadhar, A.A., Ed.; Woodhead Publishing: Oxford, UK, 2015; pp. 49–73. [Google Scholar]
- Tenter, A.M. Toxoplasma gondii in animals used for human consumption. Mem. Inst. Oswaldo Cruz 2009, 104, 364–369. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO’s First Ever Global Estimates of Foodborne Diseases Find Children under 5 Account for almost One Third of Deaths. Available online: https://www.who.int/news/item/03-12-2015-who-s-first-ever-global-estimates-of-foodborne-diseases-find-children-under-5-account-for-almost-one-third-of-deaths (accessed on 15 December 2020).
- Correa, R.; Cedeño, I.; De Escobar, C.; Fuentes, I. Increased urban seroprevalence of Toxoplasma gondii infecting swine in Panama. Veter Parasitol. 2008, 153, 9–11. [Google Scholar] [CrossRef]
- Pappas, G.; Roussos, N.; Falagas, M.E. Toxoplasmosis snapshots: Global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int. J. Parasitol. 2009, 39, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Dubey, J.P.; Lago, E.G.; Gennari, S.M.; Su, C.; Jones, J.L. Toxoplasmosis in humans and animals in Brazil: High preva-lence, high burden of disease, and epidemiology. Parasitology 2012, 139, 1375–1424. [Google Scholar] [CrossRef] [Green Version]
- Sroka, S.; Bartelheimer, N.; Winter, A.; Queiroz, A.J.N.; Alencar, C.H.; Heukelbach, J.; Ariza, L.; Liesenfeld, O.; Ribeiro, H.; Oliveira, F.A. Prevalence and Risk Factors of Toxoplasmosis among Pregnant Women in Fortaleza, Northeastern Brazil. Am. J. Trop. Med. Hyg. 2010, 83, 528–533. [Google Scholar] [CrossRef]
- Angel-Müller, E.; Hougton, M.P.; Eslava, C.; Riaño, J.; Rey, G.E.; Gómez-Marín, J.E. Gestational and congenital toxo-plasmosis in two hospitals in Bogota, Colombia. Rev. Fac. Med. 2014, 62, 179–185. [Google Scholar] [CrossRef]
- Rosso, F.; Remington, J.S.; Tunubala, G.A.; Chaves, J.A.; Agudelo, A.; Montoya, J.G.; Villalobos, C.; Messa, A.; Les, J.T. Prevalence of infection with Toxoplasma gondii among pregnant women in Cali, Colombia, South America. Am. J. Trop. Med. Hyg. 2008, 78, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Silva-Díaz, H.; Arriaga-Deza, E.V.; Failoc-Rojas, V.E.; Alarcón-Flores, Y.R.; Rojas-Rojas, S.Y.; Becerra-Gutiérrez, L.K.; Mera-Villasis, K.M.; Aguilar-Gamboa, F.R.; Silva-García, T. Seroprevalence of toxoplasmosis in pregnant women and its as-sociated factors among hospital and community populations in Lambayeque. Peru. Rev. Soc. Bras. Med. Trop 2020, 53, 1–6. [Google Scholar]
- Ruiz, A.; Manuel, C.F.; Kotcher, E. The prevalence of Toxoplasma antibodies in Costa Rican postpartum women and their neonates. Am. J. Obstet. Gynecol. 1966, 95, 817–819. [Google Scholar] [CrossRef]
- Sinibaldi, J.; De Ramirez, I. Incidence of congenital toxoplasmosis in live Guatemalan newborns. Eur. J. Epidemiol. 1992, 8, 516–520. [Google Scholar] [CrossRef]
- Alvarado-Esquivel, C.; Sifuentes-Alvarez, A.; Narro-Duarte, S.G.; Estrada-Martínez, S.; Díaz-García, J.H.; Liesenfeld, O.; Martínez-García, S.A.; Canales-Molina, A. Seroepidemiology of Toxoplasma gondii infection in pregnant women in a public hospital in northern Mexico. BMC Infect. Dis. 2006, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Montoya, J.G.; Liesenfeld, O. Toxoplasmosis. Lancet 2004, 363, 1965–1976. [Google Scholar] [CrossRef]
- Wallon, M.; Peyron, F. Congenital Toxoplasmosis: A Plea for a Neglected Disease. Pathogens 2018, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Dunn, D.; Wallon, M.; Peyron, F.; Petersen, E.; Peckham, C.; Gilbert, R. Mother-to-child transmission of toxoplasmosis: Risk estimates for clinical counselling. Lancet 1999, 353, 1829–1833. [Google Scholar] [CrossRef]
- Robbins, J.R.; Zeldovich, V.B.; Poukchanski, A.; Boothroyd, J.C.; Bakardjiev, A.I. Tissue Barriers of the Human Placenta to Infection with Toxoplasma gondii. Infect. Immun. 2011, 80, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Avelino, M.M.; Campos, D., Jr.; do Carmo Barbosa de Parada, J.; de Castro, A.M. Pregnancy as a risk factor for acute toxoplasmosis seroconversion. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 108, 19–24. [Google Scholar] [CrossRef]
- Daunter, B. Immunology of pregnancy: Towards a unifying hypothesis. Eur. J. Obstet. Gynecol. Reprod. Biol. 1992, 43, 81–95. [Google Scholar] [CrossRef]
- Etheredge, G.D.; Frenkel, J.K. Human Toxoplasma Infection in Kuna and Embera Children in the Bayano and San Blas, Eastern Panama. Am. J. Trop. Med. Hyg. 1995, 53, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Sousa, O.E.; Saenz, R.E.; Frenkel, J.K. Toxoplasmosis in Panama: A 10-Year Study. Am. J. Trop. Med. Hyg. 1988, 38, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, V.A.N.; Escala, M.; Sáenz-Llorens, X. Seroprevalencia de Infección de Toxoplasma gondii en Mujeres Embarazadas por Medio de Detección de Anticuerpos IgG e IgM anti T. gondii y su Impacto en el Recién Nacido, que Asisten a la Maternidad del Hospital Santo Tomás en el Periodo de 1 de junio 30 de Noviembre 2014. Master’s Thesis, Universidad de Panamá, Via Simón Bolívar, Panama, 2014. [Google Scholar]
- Bigna, J.J.; Tochie, J.N.; Tounouga, D.N.; Bekolo, A.O.; Ymele, N.S.; Youda, E.L.; Sime, P.S.; Nansseu, J.R. Global, regional, and country seroprevalence of Toxoplasma gondii in pregnant women: A systematic review, modelling and meta-analysis. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- El Bissati, K.; Levigne, P.; Lykins, J.; Adlaoui, E.B.; Barkat, A.; Berraho, A.; Laboudi, M.; El Mansouri, B.; Ibrahimi, A.; Rhajaoui, M.; et al. Global initiative for congenital toxoplasmosis: An observational and international comparative clinical analysis. Emerg. Microbes Infect. 2018, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rostami, A.; Riahi, S.; Gamble, H.; Fakhri, Y.; Shiadeh, M.N.; Danesh, M.; Behniafar, H.; Paktinat, S.; Foroutan, M.; Mokdad, A.; et al. Global prevalence of latent toxoplasmosis in pregnant women: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 673–683. [Google Scholar] [CrossRef]
- Li, X.; Felin, M.S.; Bodden, L.; Boyer, K.M.; McLeod, R.; Reyes, O. Toxoplasmosis Education for Pregnant Women in Panama [16A]. Obstet. Gynecol. 2016, 127, 15S–16S. [Google Scholar] [CrossRef]
- Gay-Andrieu, F.; Fricker-Hidalgo, H.; Sickinger, E.; Espern, A.; Brenier-Pinchart, M.-P.; Braun, H.-B.; Pelloux, H. Comparative evaluation of the ARCHITECT Toxo IgG, IgM, and IgG Avidity assays for anti-Toxoplasma antibodies detection in pregnant women sera. Diagn. Microbiol. Infect. Dis. 2009, 65, 279–287. [Google Scholar] [CrossRef]
- Prusa, A.-R.; Hayde, M.; Unterasinger, L.; Pollak, A.; Herkner, K.R.; Kasper, D.C. Evaluation of the Roche Elecsys Toxo IgG and IgM electrochemiluminescence immunoassay for the detection of gestational Toxoplasma infection. Diagn. Microbiol. Infect. Dis. 2010, 68, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Naessens, A.; Jenum, P.A.; Pollak, A.; Decoster, A.; Lappalainen, M.; Villena, I.; Lebech, M.; Stray-Pedersen, B.; Hayde, M.; Pinon, J.-M.; et al. Diagnosis of congenital toxoplasmosis in the neonatal period: A multicenter evaluation. J. Pediatr. 1999, 135, 714–719. [Google Scholar] [CrossRef]
- Pomares, C.; Montoya, J.G. Laboratory Diagnosis of Congenital Toxoplasmosis. J. Clin. Microbiol. 2016, 54, 2448–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MINSA. Resolución Nº57. Que adopta las normas técnicas y administrativas y protocolos de atención del programa de salud integral de la mujer. Gaceta Oficial Digital, 4 April 2019. [Google Scholar]
- Liesenfeld, O.; Montoya, J.G.; Kinney, S.; Press, C.; Remington, J.S. Effect of Testing for IgG Avidity in the Diagnosis of Toxoplasma gondiiInfection in Pregnant Women: Experience in a US Reference Laboratory. J. Infect. Dis. 2001, 183, 1248–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Ministry of Health of Peru. Guías de Manejo de las Complicaciones en el Embarazo 2015; The Ministry of Health of Peru: Lima, Peru, 2015.
- MINSA. Decreto Ejecutivo Nº 1617. Que determina y categoriza los eventos de salud pública de notificación e investigación obligatoria, define los tipos de vigilancia epidemiológica, la vigilancia laboratorial y se señalan los procedimientos para su realización. Gaceta Oficial, 22 October 2014. [Google Scholar]
- Lindsay, D.; Dubey, J.; Butler, J.; Blagburn, B. Mechanical transmission of Toxoplasma gondii oocysts by dogs. Veter- Parasitol. 1997, 73, 27–33. [Google Scholar] [CrossRef]
- Fábrega, L.; Restrepo, C.M.; Torres, A.; Smith, D.; Chan, P.; Pérez, D.; Cumbrera, A.; Caballero E., Z. Frequency of Toxoplasma gondii and Risk Factors Associated with the Infection in Stray Dogs and Cats of Panama. Microorganisms 2020, 8, 927. [Google Scholar] [CrossRef]
- Rengifo-Herrera, C.; Pile, E.; García, A.; Pérez, A.; Pérez, D.; Nguyen, F.K.; de la Guardia, V.; McLeod, R.; Caballero, Z. Seroprevalence of Toxoplasma gondii in domestic pets from metropolitan regions of Panama. Parasite 2017, 24, 9. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Statistics and Census (Panama). Densidad de Población en el Distrito de Panamá, Según Corregimientos, Censos de Población y Vivienda año: Página web de la Contraloría General de la República de Panamá 2010; National Institute of Statistics and Census (Panama): Panama City, Panama, 2010. [Google Scholar]
- National Institute of Statistics and Census (Panama). Superficie, Población y Densidad del Distrito de San Miguelito, Según Corregimiento: Censos de 1990 a 2000. Página web de la Contraloría General de la República de Panamá 2000; National Institute of Statistics and Census (Panama): Panama City, Panama, 2000. [Google Scholar]
- Anselin, L.; Syabri, I.; Kho, Y. GeoDa: An Introduction to Spatial Data Analysis. Geogr. Anal. 2006, 38, 5–22. [Google Scholar] [CrossRef]
- Burg, J.L.; Grover, C.M.; Pouletty, P.; Boothroyd, J.C. Direct and sensitive detection of a pathogenic protozoan, Toxoplasma gondii, by polymerase chain reaction. J. Clin. Microbiol. 1989, 27, 1787–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. 2020. Available online: https://www.r-project.org (accessed on 4 March 2020).
- Tests, Chi-squared (χ2), Odds ratio and Relative risk. GraphPad Prism version 6.1 for Windows, GraphPad Software, San Diego, California USA. Available online: www.graphpad.com (accessed on 7 June 2021).
- Kassambra, A. Factoextra R Package: Easy Multivariate Data Analyses and Elegant Visualization. Version 1.0.5. Available online: http://www.sthda.com/english/wiki/factoextra-r-package-easy-multivariate-dataanalyses-and-elegant-visualization#acknoweledgment (accessed on 24 June 2020).
- Lê, S.J.; Husson, J.F. FactoMineR: An R Package for Multivariate Analysis. J. Stat. Softw. 2008, 25, 18. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No. (%), (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Suspected cases of CT | |||||||||
| Region | No. of Patients | Prevalence | Old Infection IgG+ IgM- | Indeterminatecases IgG+ IgM i | Probable Recent Infection IgG+ IgM+ | Recent Infection IgG- IgM+ | At-Risk Group G- IgM- | CT Confirmed by PCR | Age a (Years) |
| Metro | 353 | 107 (30.31) (25.62–35.44) | 100 (28.32) (23.74–33.38) | 1 (0.28) (0.15–1.82) | 5 (1.42) (0.52–3.47) | 1 (0.28) (0.01–1.82) | 246 (69.68) (64.56–74.38) | 0 (0) (0–1.34) | 27.83 ± 0.33 |
| West | 444 | 178 (40.09) (35.52–44.83) | 171 (38.51) (33.99–43.23) | 1 (0.23) (0.01–1.45) | 6 (1.35) (0.55–3.07) | 0 (0) (0–1.07) | 266 (59.91 (55.17–64.47) | 0(0) (0–1.07) | 27.73 ± 0.29 |
| Central | 227 | 94 (41.41) (34.98–48.13) | 90 (39.65) (33.30–46.35) | 0 (0) (0–2.07) | 4 (1.76) (0.56–4.75) | 0 (0) (0–2.07) | 133 (58.59) (51.87–65.01) | 1 (0.44) (0.02–2.81) | 27.34 ± 0.44 |
| North | 296 | 137 (46.28) (40.52–52.14) | 133 (44.93) (39.20–50.80) | 2 (0.68) (0.12–2.69) | 2 (0.68) (0.12–2.69) | 0 (0) (0–1.60) | 159 (53.72) (47.86–59.48) | 0 (0) (0–1.60) | 26.53 ± 0.36 |
| East | 526 | 265 (50.38) (46.02–54.73) | 253 (48.09) (43.76–52.46) | 2 (0.38) (0.06–1.52) | 8 (1.52) (0.71–3.10) | 2 (0.38) (0.06–1.52) | 261 (49.62) (45.27–53.97) | 3 (0.57) (0.15–1.80) | 26.65 ± 0.27 |
| San Miguelito | 480 | 252 (52.50) (47.93–57.03) | 244 (50.83) (46.27–55.38) | 0 (0) (0–0.99) | 6 (1.25) (0.51–2.84) | 2 (0.42) (0.07–1.66) | 228 (47.50) (42.97–52.07) | 5 (1.04) (0.38–2.56) | 27.61 ± 0.27 |
| Total | 2326 | 1033 (44.41) (42.38–46.46) | 991 (42.60) (40.59–44.65) | 6 (0.26) (0.10–0.59) | 31 (1.33) (0.92–1.91) | 5 (0.21) (0.08–0.53) | 1293 (55.58) (53.54–57.62) | 9 (0.38) (0.19–0.76) | 27.28 ± 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores, C.; Villalobos-Cerrud, D.; Borace, J.; Fábrega, L.; Norero, X.; Sáez-Llorens, X.; Moreno, M.T.; Restrepo, C.M.; Llanes, A.; Quijada R., M.; et al. Epidemiological Aspects of Maternal and Congenital Toxoplasmosis in Panama. Pathogens 2021, 10, 764. https://doi.org/10.3390/pathogens10060764
Flores C, Villalobos-Cerrud D, Borace J, Fábrega L, Norero X, Sáez-Llorens X, Moreno MT, Restrepo CM, Llanes A, Quijada R. M, et al. Epidemiological Aspects of Maternal and Congenital Toxoplasmosis in Panama. Pathogens. 2021; 10(6):764. https://doi.org/10.3390/pathogens10060764
Chicago/Turabian StyleFlores, Carlos, Delba Villalobos-Cerrud, Jovanna Borace, Lorena Fábrega, Ximena Norero, X. Sáez-Llorens, María Teresa Moreno, Carlos M. Restrepo, Alejandro Llanes, Mario Quijada R., and et al. 2021. "Epidemiological Aspects of Maternal and Congenital Toxoplasmosis in Panama" Pathogens 10, no. 6: 764. https://doi.org/10.3390/pathogens10060764