
A Cross-Sectional Study of SARS-CoV-2 Seroprevalence between Fall 2020 and February 2021 in Allegheny County, Western Pennsylvania, USA

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Results
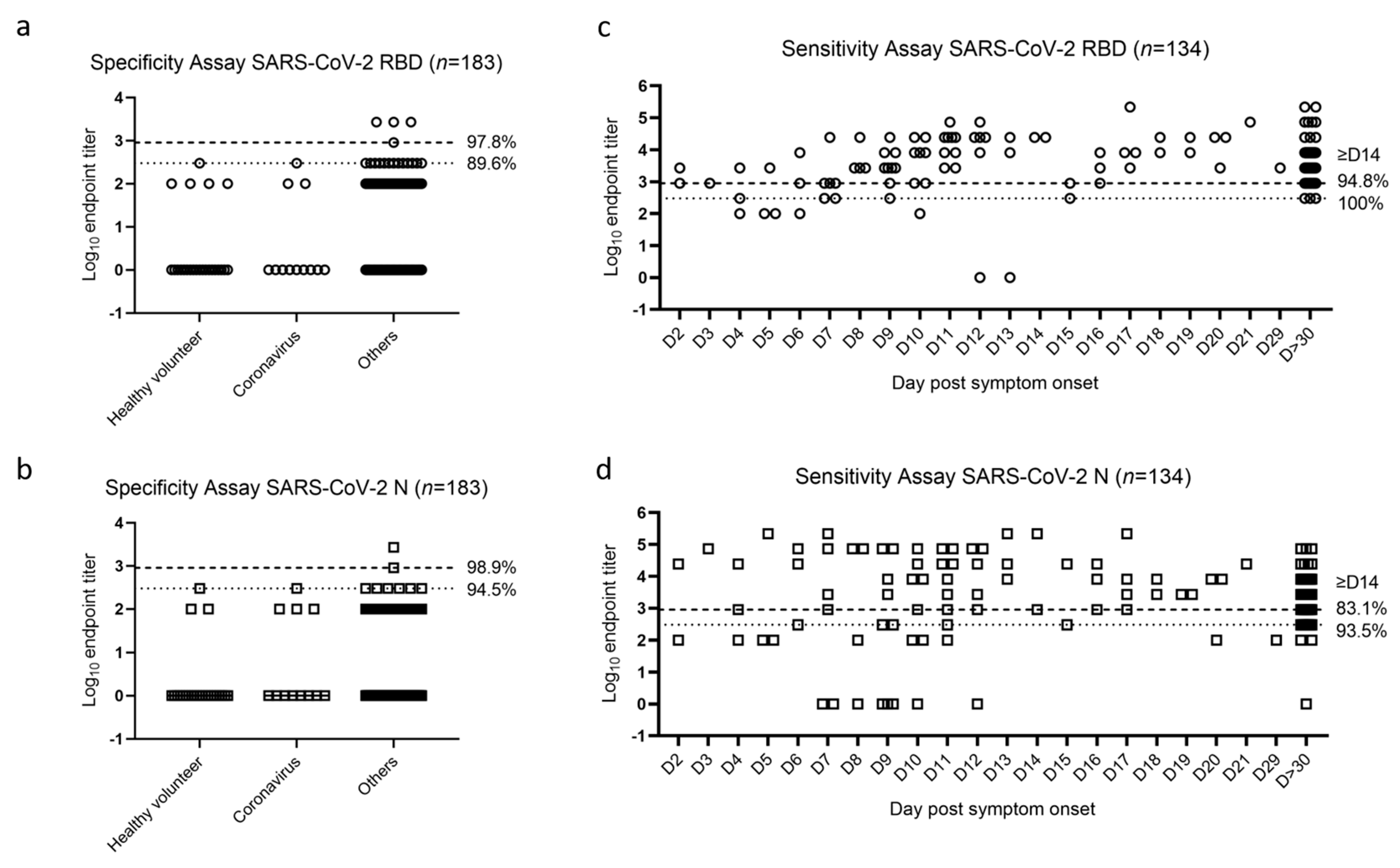
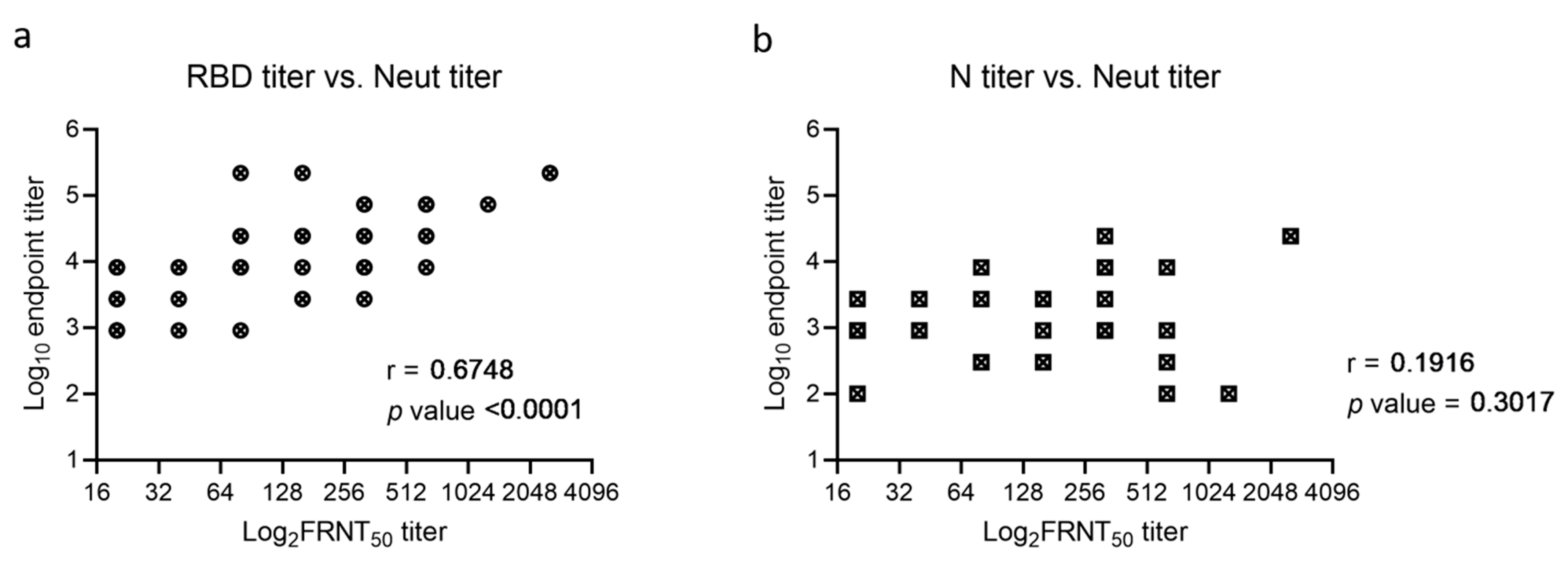
2.1. SARS-CoV-2 RBD and N ELISA Validation
2.2. Seroprevalence of COVID-19 in Allegheny County, Western PA
2.3. Comparison of Income and Race between Infected and Vaccinated Groups
3. Discussion
4. Materials and Methods
4.1. Human Samples
4.2. Enzyme-Linked Immunosorbent Assay (ELISA)
4.3. Focus Reduction Neutralization Test (FRNT)
4.4. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Amanat, F.; Stadlbauer, D.; Strohmeier, S.; Nguyen, T.H.O.; Chromikova, V.; McMahon, M.; Jiang, K.; Arunkumar, G.A.; Jurczyszak, D.; Polanco, J.; et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nat. Med. 2020, 26, 1033–1036. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, K.; Chen, C.J.; Maeda, J.; Makino, S. Nucleocapsid-independent specific viral RNA packaging via viral envelope protein and viral RNA signal. J. Virol. 2003, 77, 2922–2927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, H.L.; Letko, M.; Lasso, G.; Ssebide, B.; Nziza, J.; Byarugaba, D.K.; Navarrete-Macias, I.; Liang, E.; Cranfield, M.; Han, B.A.; et al. The evolutionary history of ACE2 usage within the coronavirus subgenus Sarbecovirus. Virus Evol. 2020. [Google Scholar] [CrossRef]
- Berry, J.D.; Hay, K.; Rini, J.M.; Yu, M.; Wang, L.; Plummer, F.A.; Corbett, C.R.; Andonov, A. Neutralizing epitopes of the SARS-CoV S-protein cluster independent of repertoire, antigen structure or mAb technology. MAbs 2010, 2, 53–66. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.J.; Leng, C.H.; Lien, S.P.; Chi, H.Y.; Huang, C.Y.; Lin, C.L.; Lian, W.C.; Chen, C.J.; Hsieh, S.L.; Chong, P. Immunological characterizations of the nucleocapsid protein based SARS vaccine candidates. Vaccine 2006, 24, 3100–3108. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA vaccine against SARS-CoV-2-preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- Eckerle, I.; Meyer, B. SARS-CoV-2 seroprevalence in COVID-19 hotspots. Lancet 2020, 396, 514–515. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, J.H.; Hsueh, P.R. Population-based seroprevalence surveys of anti-SARS-CoV-2 antibody: An up-to-date review. Int. J. Infect. Dis. 2020, 101, 314–322. [Google Scholar] [CrossRef]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M.; Nourollahpour Shiadeh, M.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Bajema, K.L.; Wiegand, R.E.; Cuffe, K.; Patel, S.V.; Iachan, R.; Lim, T.; Lee, A.; Moyse, D.; Havers, F.P.; Harding, L.; et al. Estimated SARS-CoV-2 seroprevalence in the US as of September 2020. JAMA Intern. Med. 2021, 181, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Rapsinski, G.J.; Zilla, M.L.; Wheeler, S.E. Immunocompromised seroprevalence and course of illness of SARS-CoV-2 in one pediatric quaternary care center. J. Pediatric Infect. Dis. Soc. 2021, 10, 426–431. [Google Scholar] [CrossRef]
- Wheeler, S.E.; Shurin, G.V.; Keetch, C.; Mitchell, G.; Kattel, G.; McBreen, J.; Shurin, M.R. Evaluation of SARS-CoV-2 prototype serologic test in hospitalized patients. Clin. Biochem. 2020, 86, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Azar, K.M.J.; Shen, Z.; Romanelli, R.J.; Lockhart, S.H.; Smits, K.; Robinson, S.; Brown, S.; Pressman, A.R. Disparities in outcomes among COVID-19 patients in a large health care system in California. Health Aff. (Millwood) 2020, 39, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Webb Hooper, M.; Napoles, A.M.; Perez-Stable, E.J. COVID-19 and racial/ethnic disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W. COVID-19 and African Americans. JAMA 2020, 323, 1891–1892. [Google Scholar] [CrossRef] [Green Version]
- Anaele, B.I.; Doran, C.; McIntire, R. Visualizing COVID-19 mortality rates and African-American populations in the USA and Pennsylvania. J. Racial. Ethn. Health Disparities 2021. [Google Scholar] [CrossRef]
- Grifoni, A.; Sidney, J.; Zhang, Y.; Scheuermann, R.H.; Peters, B.; Sette, A. A sequence homology and bioinformatic approach can predict candidate targets for immune responses to SARS-CoV-2. Cell Host Microbe 2020, 27, 671–680. [Google Scholar] [CrossRef]
- Cohen, J.I.; Burbelo, P.D. Reinfection with SARS-CoV-2: Implications for vaccines. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.H.; Michlmayr, D.; Gubbels, S.M.; Mølbak, K.; Ethelberg, S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: A population-level observational study. Lancet 2021, 397, 1204–1212. [Google Scholar] [CrossRef]
- Hurlburt, N.K.; Seydoux, E.; Wan, Y.H.; Edara, V.V.; Stuart, A.B.; Feng, J.; Suthar, M.S.; McGuire, A.T.; Stamatatos, L.; Pancera, M. Structural basis for potent neutralization of SARS-CoV-2 and role of antibody affinity maturation. Nat. Commun. 2020, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Shan, C.; Duan, X.; Chen, Z.; Liu, P.; Song, J.; Song, T.; Bi, X.; Han, C.; Wu, L.; et al. A human neutralizing antibody targets the receptor-binding site of SARS-CoV-2. Nature 2020, 584, 120–124. [Google Scholar] [CrossRef]
- Starr, T.N.; Greaney, A.J.; Hilton, S.K.; Ellis, D.; Crawford, K.H.D.; Dingens, A.S.; Navarro, M.J.; Bowen, J.E.; Tortorici, M.A.; Walls, A.C.; et al. Deep mutational scanning of SARS-CoV-2 receptor binding domain reveals constraints on folding and ACE2 binding. Cell 2020, 182, 1295–1310. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, E.N.; Devlin, J.C.; Buus, T.B.; Koide, A.; Cornelius, A.; Samanovic, M.I.; Herrera, A.; Zhang, C.; Desvignes, L.; Odum, N.; et al. Discrete immune response signature to SARS-CoV-2 mRNA vaccination versus infection. medRxiv 2021. [Google Scholar] [CrossRef]
- Health, P.C.-VTFPDo. PA Interim Vaccine Plan V8.0. 2021. Available online: https://www.health.pa.gov/topics/Documents/Programs/Immunizations/PA%20Interim%20Vaccine%20Plan%20V.8.pdf (accessed on 6 May 2021).
- Harmon, J.R.; Barbeau, D.J.; Nichol, S.T.; Spiropoulou, C.F.; McElroy, A.K. Rift valley fever virus vaccination induces long-lived, antigen-specific human T cell responses. NPJ Vaccines 2020, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fall 2020 (n = 199) | February 2021 (n = 194) | |
|---|---|---|
| RBD positive (endpoint titer ≥ 900)—No. (%) [95%CI] | 11 (5.5) [3–10] | 48 (24.7) [19–31] |
| N positive (endpoint titer ≥ 300)—No. (%) [95%CI] | 9 (4.5) [2–8] | 29 (14.9) [10–21] |
| RBD and N both positive—No. (%) [95%CI] | 5 (2.5) [1–6] | 25 (12.9) [9–18] |
| Neut positive (FRNT50 ≥ 40)—No. (%) [95%CI] | 4 (2.0) [1–5] | 32 (16.5) [12–22] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, L.; Doyle, J.; Barbeau, D.J.; Le Sage, V.; Wells, A.; Duprex, W.P.; Shurin, M.R.; Wheeler, S.E.; McElroy, A.K. A Cross-Sectional Study of SARS-CoV-2 Seroprevalence between Fall 2020 and February 2021 in Allegheny County, Western Pennsylvania, USA. Pathogens 2021, 10, 710. https://doi.org/10.3390/pathogens10060710
Xu L, Doyle J, Barbeau DJ, Le Sage V, Wells A, Duprex WP, Shurin MR, Wheeler SE, McElroy AK. A Cross-Sectional Study of SARS-CoV-2 Seroprevalence between Fall 2020 and February 2021 in Allegheny County, Western Pennsylvania, USA. Pathogens. 2021; 10(6):710. https://doi.org/10.3390/pathogens10060710
Chicago/Turabian StyleXu, Lingqing, Joshua Doyle, Dominique J. Barbeau, Valerie Le Sage, Alan Wells, W. Paul Duprex, Michael R. Shurin, Sarah E. Wheeler, and Anita K. McElroy. 2021. "A Cross-Sectional Study of SARS-CoV-2 Seroprevalence between Fall 2020 and February 2021 in Allegheny County, Western Pennsylvania, USA" Pathogens 10, no. 6: 710. https://doi.org/10.3390/pathogens10060710