
Myopericarditis Associated with COVID-19 in a Pediatric Patient with Kidney Failure Receiving Hemodialysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Case Presentation
3. Discussions
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verity, R.; Okell, L.C.; Dorigatti, I. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Qiu, H.; Wu, J.; Hong, L. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus Response Team, Centers for Disease Control and Prevention. Coronavirus disease 2019 in children—United States, 12 February–2 April, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [Green Version]
- CDC. Certain Medical Conditions and Risk for Severe COVID-19 Illness. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 21 March 2021).
- Parri, N.; Lenge, M.; Buonsenso, D. Coronavirus Infection in Pediatric Emergency Departments (CONFIDENCE) Research Group. Children with Covid-19 in Pediatric Emergency Departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef]
- Yu, C.M.; Wong, R.S.; Wu, E.B.; Kong, S.L.; Wong, J.; Yip, G.W.; Sung, J.J. Cardiovascular complications of severe acute respiratory syndrome. Postgrad. Med. J. 2006, 82, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Dabbagh, M.F.; Aurora, L.; D’Souza, P.; Weinmann, A.J.; Bhargava, P.; Basir, M.B. Cardiac tamponade secondary to COVID-19. JACC Case Rep. 2020, 2, 1326–1330. [Google Scholar] [CrossRef]
- Hua, A.; O’Gallagher, K.; Sado, D.; Byrne, J. Life-threatening cardiac tamponade complicating myo-pericarditis in COVID-19. Eur. Heart J. 2020, 41, 2130. [Google Scholar] [CrossRef] [Green Version]
- Bejiqi, R.; Retkoceri, R.; Maloku, A.; Mustafa, A.; Bejiqi, H.; Bejiqi, R. The Diagnostic and Clinical Approach to Pediatric Myocarditis: A Review of the Current Literature. Open Access Maced. J. Med. Sci. 2019, 7, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Tung-Chen, Y. Acute pericarditis due to COVID-19 infection: An underdiagnosed disease? Med. Clin. 2020, 155, 44–45. [Google Scholar] [CrossRef]
- Li, M.; Chen, S.; Xiang, X.; Wang, Q.; Liu, X. Effects of SARS-CoV-2 and its functional receptor ACE2 on the cardiovascular system. Effekte von SARS-CoV-2 und seinem funktionalen Rezeptor ACE2 auf das Herz-Kreislauf-System. Herz 2020, 45, 659–662. [Google Scholar] [CrossRef]
- Gu, J.; Gong, E.; Zhang, B.; Zheng, J.; Gao, Z.; Zhong, Y.; Zou, W.; Zhan, J.; Wang, S.; Xie, Z.; et al. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005, 202, 415–424. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotta, V.; Marsenic, O.; Atkinson, A.; Pfister, M. Hemodialysis (HD) dose and ultrafiltration rate are associated with survival in pediatric and adolescent patients on chronic HD—A large observational study with follow-up to young adult age. Pediatric Nephrol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, M.R.; Guglin, M.E.; Saltzberg, M.T.; Jessup, M.L.; Bart, B.A.; Teerlink, J.R.; Jaski, B.E.; Fang, J.C.; Feller, E.D.; Haas, G.J.; et al. Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure. J. Am. Coll. Cardiol. 2007, 49, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Burns, J.P. Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to us and canadian pediatric intensive care units. JAMA Pediatrics 2020. [Google Scholar] [CrossRef]
- Pranata, R.; Huang, I.; Lukito, A.A.; Raharjo, S.B. Elevated N-terminal pro-brain natriuretic peptide is associated with increased mortality in patients with COVID-19: Systematic review and meta-analysis. Postgrad. Med. J. 2020, 96, 387–391. [Google Scholar] [CrossRef]
- Gao, L.; Jiang, D.; Wen, X.S.; Cheng, X.C.; Sun, M.; He, B.; Zhang, D.Y. Prognostic value of NT-proBNP in patients with severe COVID-19. Respir. Res. 2020, 21, 83. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Gonzalez, M.; Castellano-Martinez, A.; Cascales-Poyatos, H.M.; Perez-Reviriego, A.A. Cardiovascular impact of COVID-19 with a focus on children: A systematic review. World J. Clin. Cases 2020, 8, 5250–5283. [Google Scholar] [CrossRef] [PubMed]
- Tersalvi, G.; Vicenzi, M.; Calabretta, D.; Biasco, L.; Pedrazzini, G.; Winterton, D. Elevated troponin in patients with Coronavirus Disease 2019 (COVID-19): Possible mechanisms. J. Card. Fail. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; She, J.; Wang, Y.; Ma, X. The clinical characteristics of myocardial injury in severe and very severe patients with 2019 novel coronavirus disease. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Huang, Z.; Lin, L.; Lv, J. Coronavirus Disease 2019 (COVID-19) and Cardiovascular Disease: A Viewpoint on the Potential Influence of Angiotensin-Converting Enzyme Inhibitors/Angiotensin Receptor Blockers on Onset and Severity of Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Am. Heart Assoc. 2020, 9, e016219. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yu, J.; Pan, L.Y.; Jiang, H.Y. ACEI/ARB use and risk of infection or severity or mortality of COVID-19: A systematic review and meta-analysis. Pharmacol. Res. 2020, 158, 104927. [Google Scholar] [CrossRef] [PubMed]
- Gul, R.; Kim, U.H.; Alfadda, A.A. Renin-angiotensin system at the interface of COVID-19 infection. Eur. J. Pharmacol. 2021, 890, 173656. [Google Scholar] [CrossRef]
- Laycock, J.; Baum, M.; Rees, L. KDIGO nomenclature glossary for Pediatric Nephrology. Pediatric Nephrol. 2020, 35, 2201–2203. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Normal Range | Before COVID-19 (30 June 2020) | Confirmed COVID-19 Infection (9 July 2020) | Early Post-COVID-19 Infection (30 July 2020) | Late Post-COVID-19 Infection (22 July 2020) |
|---|---|---|---|---|---|
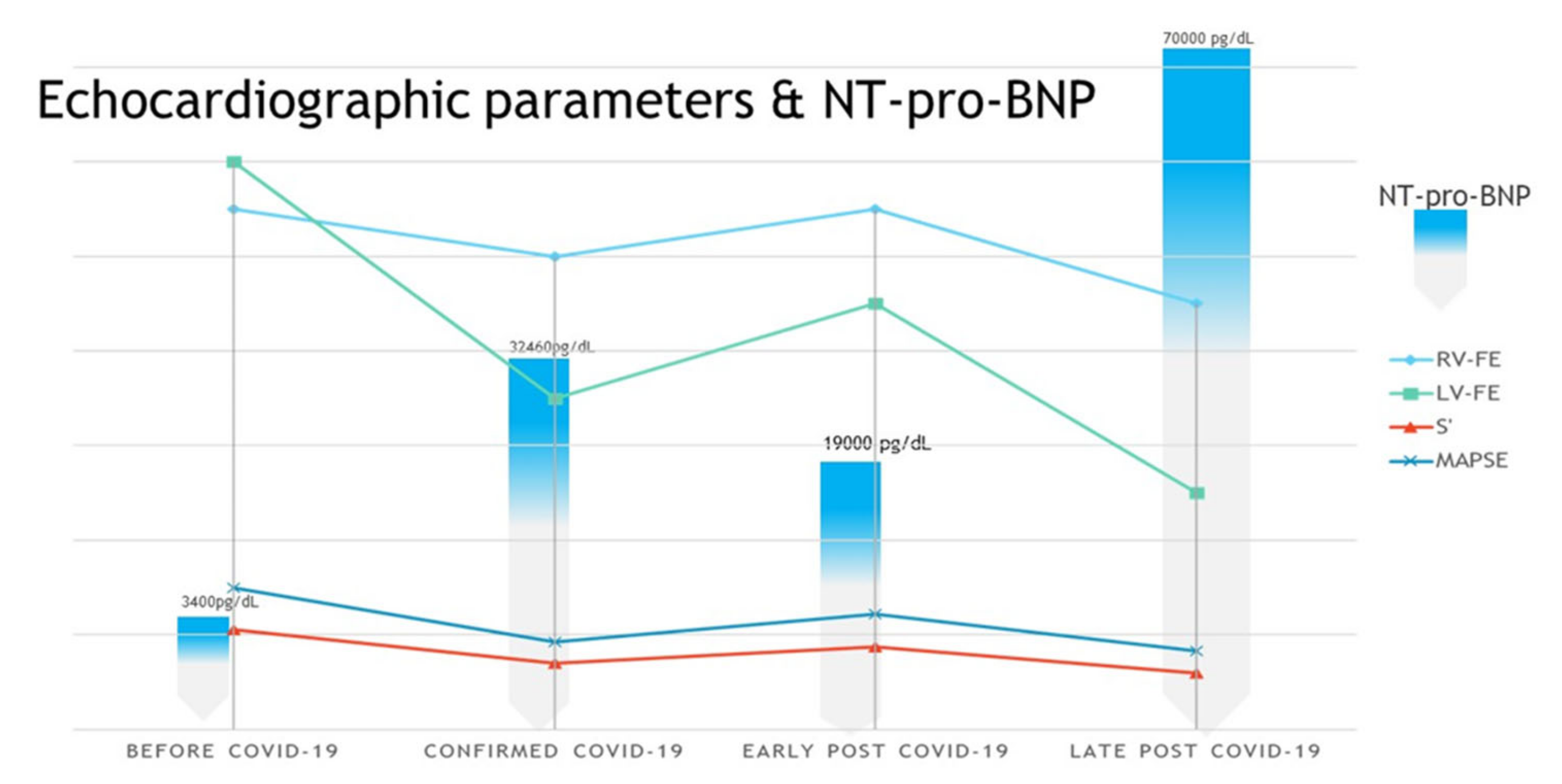
| Right ventricular ejection fraction RV EF (%) | >60 | 55 | 50 | 55 | 45 |
| Left ventricular ejection fraction LV EF (%) | >60 | 60 | 35 | 45 | 25 |
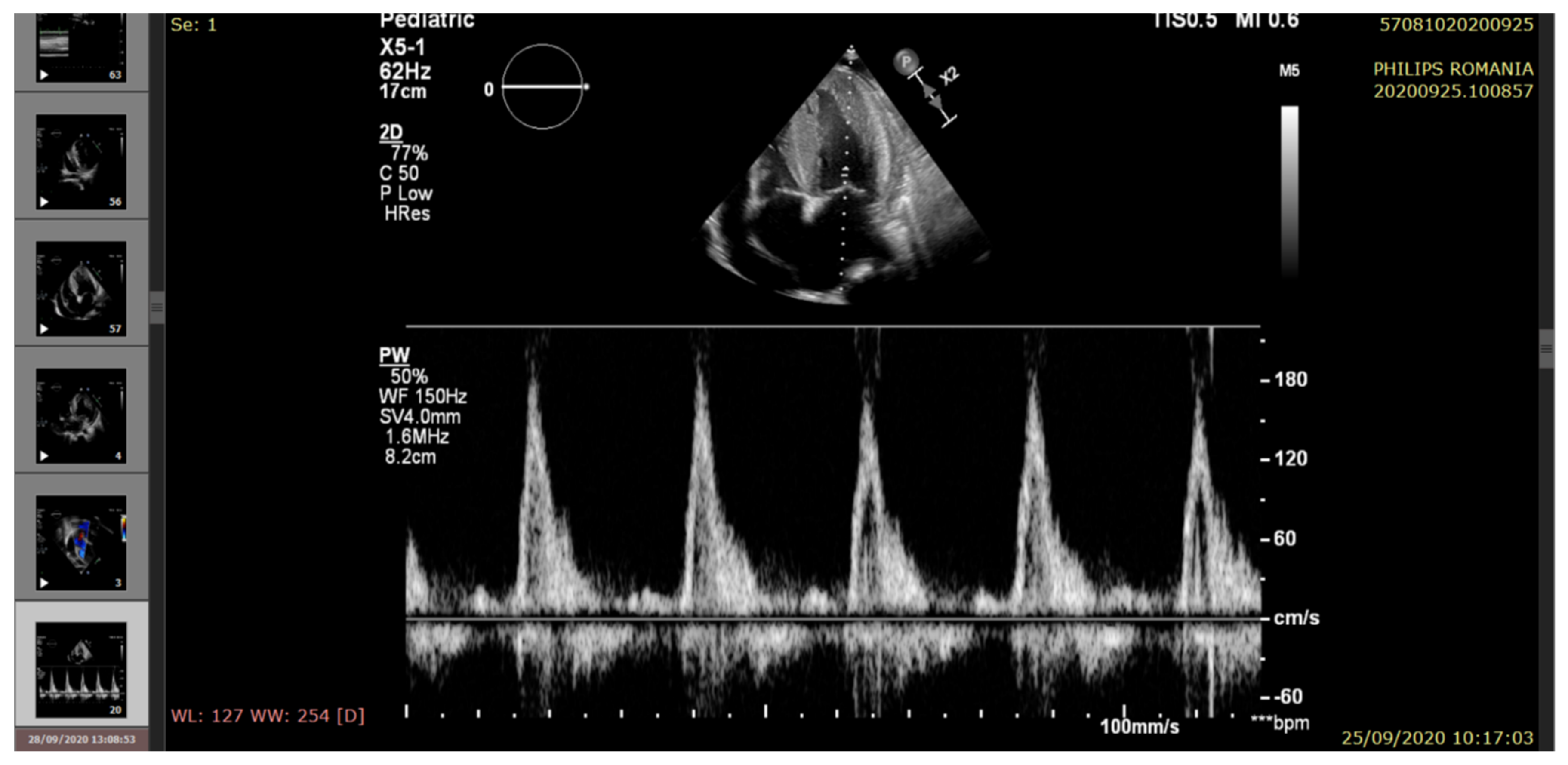
| (S’) Lateral systolic myocardial velocity (cm/s) tissue doppler imaging (TDI) | 8.43 ± 1.06 | 10.5 | 7 | 8.7 | 5.9 |
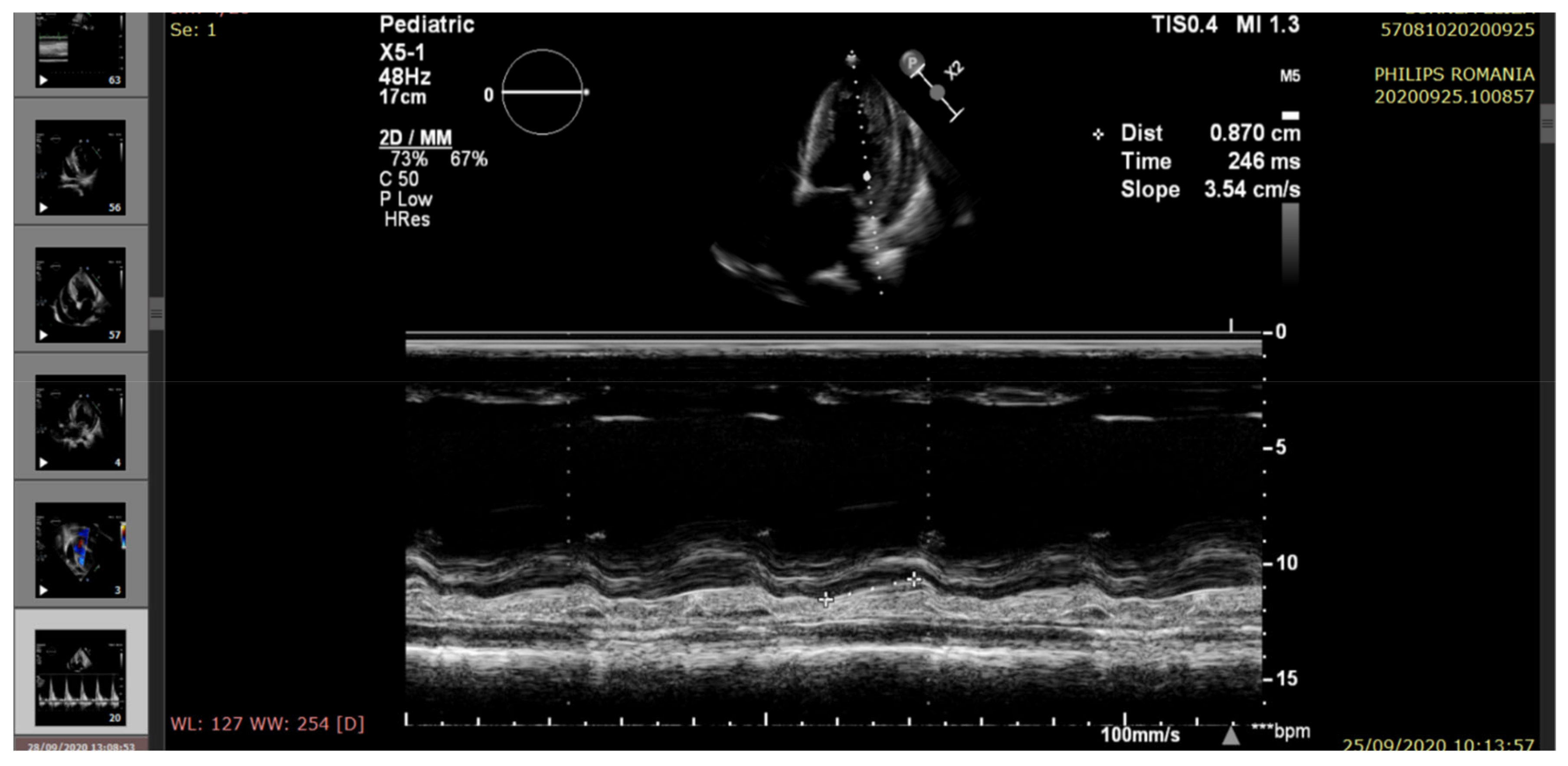
| Mitral annular plane systolic excursion (MAPSE) (mm) (M-mode) | 16.4 ± 2.4 | 15 | 9.2 | 12.2 | 8.3 |
| Mitral diastolic pattern | Normal | Impaired relaxation | Pseudonormal filling | Impaired relaxation | Restrictive filling |
| Pericardial fluid (edge) | <5 mm | Small (6 mm) | Raised (20 mm) | Moderate (14 mm) | Large (22 mm) |
| Pulmonary hypertension (echocardiographic criteria) | Normal | Mild | Moderate | Mild | Moderate/severe |
| Blood pressure (mmHg) | Systolic (90–120)/diastolic (50–80) | 150/90 | 160/110 | 160/90 | 145/95 |
| O2 %saturation | 95–100 | 99 | 80–85 | 90 | 80 |
| Heart rate (beats/min) | 60–100 | 78 | 120 | 90 | 120 |
| Diuresis (mL/24 h) | 500–1200 | 1500 | 500 | 1500 | 1000 |
| Na (mmol/L) | 138–144 | 132 | 129.9 | 122 | 126.7 |
| K (mmol/L) | 3.4–4.9 | 4.90 | 4.96 | 5.00 | 5.02 |
| Serum creatinine (mg/dL) | 0.5–1 | 10.24 | 8.20 | 8.40 | 8.16 |
| Serum urea (mg/dL) | <39 | 111.3 | 86.5 | 120 | 99.5 |
| CRP (mg/L) | 0–5.00 | 3.88 | 2.68 | 5.78 | 1.82 |
| Hb (g/dL) | 11.5–15 | 6.8 | 5.6 | 6.00 | 8.6 |
| WBC (×109/L) | 4.5–13.5 | 4.43 | 5.67 | 6.57 | 16.33 |
| Neutrophil (×109/L) | 1.8–8 | 2.5 | 2.65 | 16.00 | 14.14 |
| Lymphocytes (×109/L) | 1.5–6.5 | 0.76 | 1.23 | 1.2 | 1.13 |
| Lymphocytes (%) | 20–55 | 17.20 | 6.1 | 6.00 | 6.9 |
| NT-proBNP (pg/dL) | (<125) | 3400 | 32,460 | 19,000 | 70,000 |
| Troponin T (pg/mL) | 0–14 (negative) >50 (positive) | 23 | 61 | 44 | 66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, M.D.; Balgradean, M.; Cirstoveanu, C.G.; Balgradean, I.; Popa, L.I.; Pavelescu, C.; Capitanescu, A.; Berghea, E.C.; Filip, C. Myopericarditis Associated with COVID-19 in a Pediatric Patient with Kidney Failure Receiving Hemodialysis. Pathogens 2021, 10, 486. https://doi.org/10.3390/pathogens10040486
Ionescu MD, Balgradean M, Cirstoveanu CG, Balgradean I, Popa LI, Pavelescu C, Capitanescu A, Berghea EC, Filip C. Myopericarditis Associated with COVID-19 in a Pediatric Patient with Kidney Failure Receiving Hemodialysis. Pathogens. 2021; 10(4):486. https://doi.org/10.3390/pathogens10040486
Chicago/Turabian StyleIonescu, Marcela Daniela, Mihaela Balgradean, Catalin Gabriel Cirstoveanu, Ioana Balgradean, Loredana Ionela Popa, Carmen Pavelescu, Andrei Capitanescu, Elena Camelia Berghea, and Cristina Filip. 2021. "Myopericarditis Associated with COVID-19 in a Pediatric Patient with Kidney Failure Receiving Hemodialysis" Pathogens 10, no. 4: 486. https://doi.org/10.3390/pathogens10040486