
Rotavirus Strain Distribution before and after Introducing Rotavirus Vaccine in India


 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
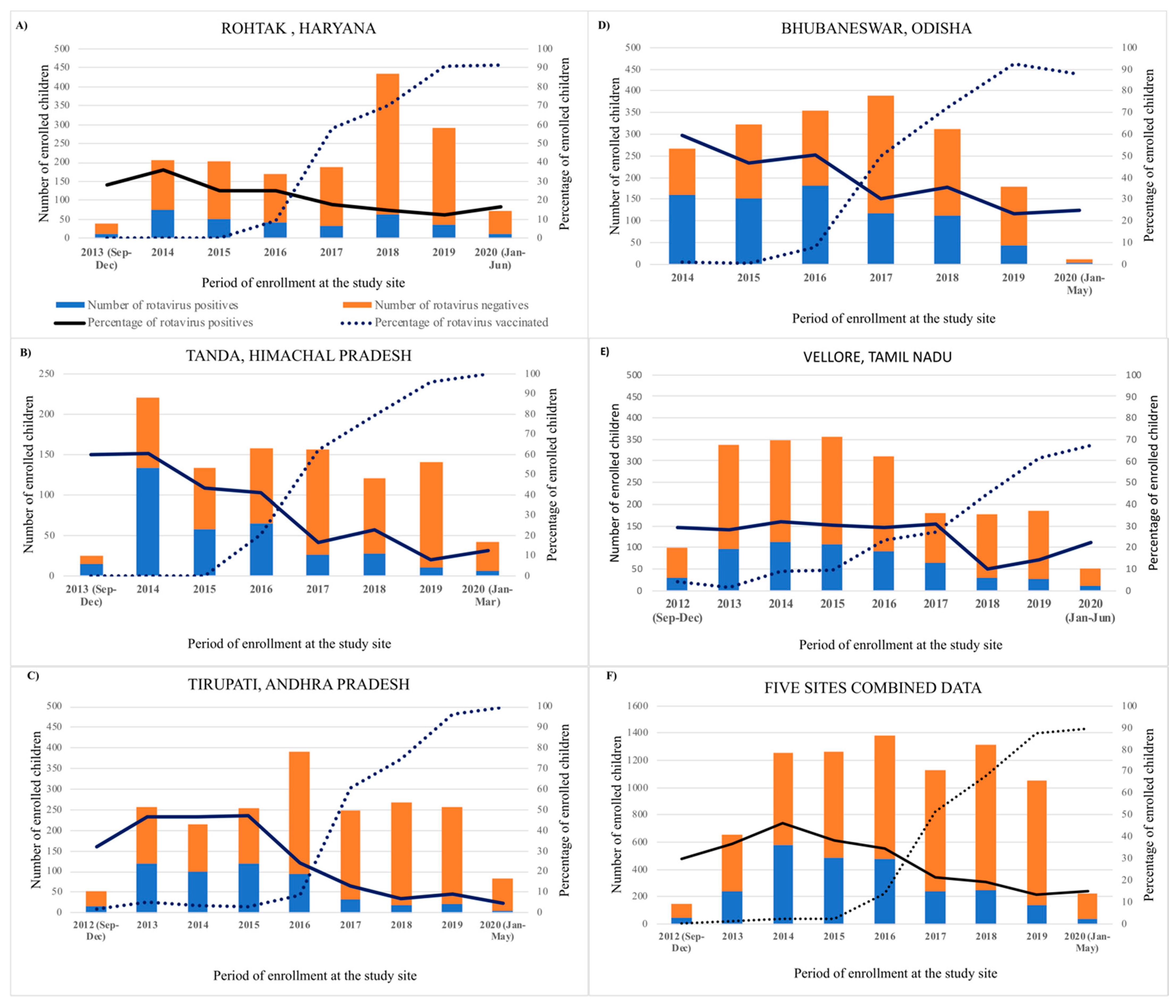
2.1. Prevalence of Rotavirus Diarrhea
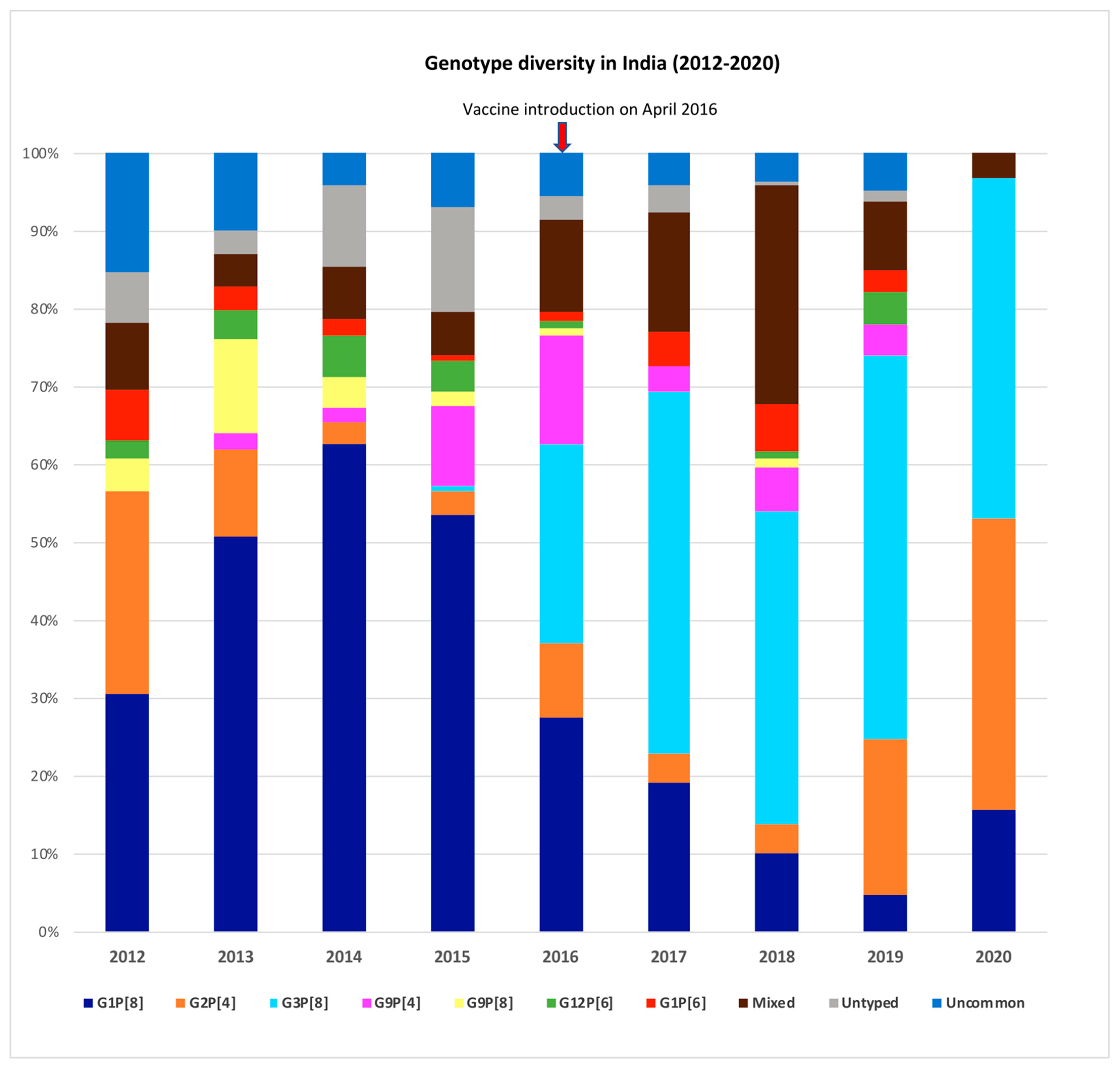
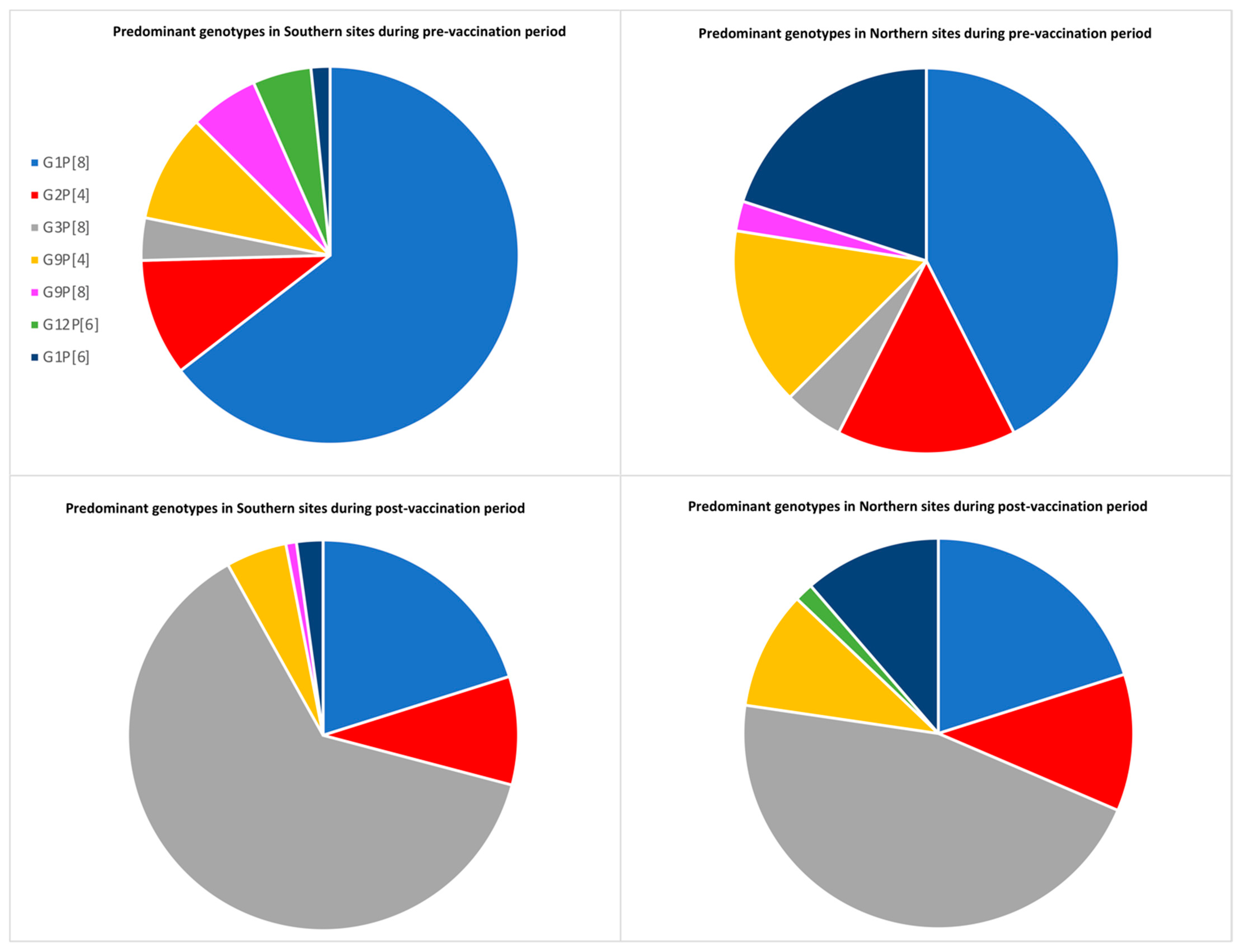
2.2. Rotavirus Genotype Distribution in India
3. Discussion
4. Materials and Methods
4.1. Study Sites
4.2. Sample Collection and Laboratory Testing
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Parashar, U.D.; Gibson, C.J.; Bresee, J.S.; Glass, R.I. Rotavirus and Severe Childhood Diarrhea. Emerg. Infect. Dis. 2006, 12, 304–306. [Google Scholar] [CrossRef] [Green Version]
- Nair, N.P.; Giri, S.; Mohan, V.R.; Parashar, U.; Tate, J.; Shah, M.P.; Arora, R.; Gupte, M.; Mehendale, S.M. Rotavirus vaccine impact assessment surveillance in India: Protocol and methods. BMJ Open 2019, 9, e024840. [Google Scholar] [CrossRef]
- Santos, N.; Hoshino, Y. Global distribution of rotavirus serotypes/genotypes and its implication for the development and implementation of an effective rotavirus vaccine. Rev. Med Virol. 2004, 15, 29–56. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.M.; Tate, J.E.; Kirkwood, C.D.; Steele, A.D.; Parashar, U.D. Current and new rotavirus vaccines. Curr. Opin. Infect. Dis. 2019, 32, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Zeller, M.; Rahman, M.; Heylen, E.; De Coster, S.; De Vos, S.; Arijs, I.; Novo, L.; Verstappen, N.; Van Ranst, M.; Matthijnssens, J. Rotavirus incidence and genotype distribution before and after national rotavirus vaccine introduction in Belgium. Vaccine 2010, 28, 7507–7513. [Google Scholar] [CrossRef]
- Hungerford, D.; Allen, D.J.; Nawaz, S.; Collins, S.; Ladhani, S.; Vivancos, R.; Iturriza-Gómara, M. Impact of rotavirus vaccination on rotavirus genotype distribution and diversity in England, September 2006 to August 2016. Eurosurveillance 2019, 24, 1700774. [Google Scholar] [CrossRef]
- Mwanga, M.J.; Owor, B.E.; Ochieng, J.B.; Ngama, M.H.; Ogwel, B.; Onyango, C.; Juma, J.; Njeru, R.; Gicheru, E.; Otieno, G.P.; et al. Rotavirus group A genotype circulation patterns across Kenya before and after nationwide vaccine introduction, 2010–2018. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Markkula, J.; Hemming-Harlo, M.; Salminen, M.T.; Savolainen-Kopra, C.; Pirhonen, J.; Al-Hello, H.; Vesikari, T. Rotavirus epidemiology 5–6 years after universal rotavirus vaccination: Persistent rotavirus activity in older children and elderly. Infect. Dis. 2017, 49, 388–395. [Google Scholar] [CrossRef]
- Verberk, J.; Bruijning-Verhagen, P.; de Melker, H.E. Rotavirus in the Netherlands: Background information for the Health Council; National Institute for Public Health and the Environment; RIVM: Bilthoven, The Netherlands, 2017. [Google Scholar] [CrossRef]
- Kaplon, J.; Grangier, N.; Pillet, S.; Minoui-Tran, A.; Vabret, A.; Wilhelm, N.; Prieur, N.; Lazrek, M.; Alain, S.; Mekki, Y.; et al. Predominance of G9P[8] rotavirus strains throughout France, 2014–2017. Clin. Microbiol. Infect. 2018, 24, 660.e1–660.e4. [Google Scholar] [CrossRef] [Green Version]
- Malik, A.; Haldar, P.; Ray, A.; Shet, A.; Kapuria, B.; Bhadana, S.; Santosham, M.; Ghosh, R.S.; Steinglass, R.; Kumar, R. Introducing rotavirus vaccine in the Universal Immunization Programme in India: From evidence to policy to implementation. Vaccine 2019, 37, 5817–5824. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.; Arora, R.; Chitambar, S.D.; Deshpande, J.; Gupte, M.D.; Kulkarni, M.; Naik, T.N.; Mukherji, D.; Venkatasubramaniam, S.; Gentsch, J.R.; et al. Multicenter, Hospital-Based Surveillance of Rotavirus Disease and Strains among Indian Children Aged. J. Infect. Dis. 2009, 200 (Suppl. 1), S147–S153. [Google Scholar] [CrossRef] [Green Version]
- Mehendale, S.; Venkatasubramanian, S.; Kumar, C.P.G.; Kang, G.; Gupte, M.D.; Arora, R. Expanded Indian national rotavirus surveillance network in the context of rotavirus vaccine introduction. Indian Pediatr. 2016, 53, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, N.; Rongsen-Chandola, T.; Bavdekar, A.; John, J.; Antony, K.; Taneja, S.; Goyal, N.; Kawade, A.; Kang, G.; Rathore, S.S.; et al. Efficacy of a monovalent human-bovine (116E) rotavirus vaccine in Indian infants: A randomised, double-blind, placebo-controlled trial. Lancet 2014, 383, 2136–2143. [Google Scholar] [CrossRef] [Green Version]
- Debellut, F.; Jaber, S.; Bouzya, Y.; Sabbah, J.; Barham, M.; Abu-Awwad, F.; Hjaija, D.; Ramlawi, A.; Pecenka, C.; Clark, A.; et al. Introduction of rotavirus vaccination in Palestine: An evaluation of the costs, impact, and cost-effectiveness of ROTARIX and ROTAVAC. PLoS ONE 2020, 15, e0228506. [Google Scholar] [CrossRef] [Green Version]
- Giri, S.; Kumar, C.P.G.; Khakha, S.A.; Chawla-Sarkar, M.; Gopalkrishna, V.; Chitambar, S.D.; Ray, P.; Venkatasubramanian, S.; Borkakoty, B.J.; National Rotavirus Surveillance Network investigators; et al. Diversity of rotavirus genotypes circulating in children <5 years of age hospitalized for acute gastroenteritis in India from 2005 to 2016: Analysis of temporal and regional genotype variation. BMC Infect. Dis. 2020, 20, 740. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Thakur, N.; Vashistt, J.; Grover, N.; Krishnan, T.; Changotra, H. Predominance of unusual rotavirus G1P[6] strain in North India: An evidence from hospitalized children and adult diarrheal patients. Infect. Genet. Evol. 2016, 46, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Babji, S.; Arumugam, R.; Priyahemavathy, R.; Sriraman, A.; Sarvanabhavan, A.; Manickavasagam, P.; Simon, A.; Aggarwal, I.; Moses, P.D.; Arora, R.; et al. Genotype distribution of Group A rotavirus from southern India, 2005–2016. Vaccine 2018, 36, 7816–7819. [Google Scholar] [CrossRef]
- Giri, S.; Nair, N.P.; Mathew, A.; Manohar, B.; Simon, A.; Singh, T.; Kumar, S.S.; Mathew, M.A.; Babji, S.; Arora, R.; et al. Rotavirus gastroenteritis in Indian children < 5 years hospitalized for diarrhoea, 2012 to 2016. BMC Public Health 2019, 19, 69. [Google Scholar] [CrossRef]
- Tiku, V.R.; Sharma, S.; Verma, A.; Kumar, P.; Raghavendhar, S.; Aneja, S.; Paul, V.K.; Bhan, M.K.; Ray, P. Rotavirus diversity among diarrheal children in Delhi, India during 2007–2012. Vaccine 2014, 32, A62–A67. [Google Scholar] [CrossRef] [Green Version]
- Carvalho-Costa, F.A.; Volotão, E.D.M.; de Assis, R.M.S.; Fialho, A.M.; Andrade, J.D.S.R.D.; Rocha, L.N.; Tort, L.F.L.; da Silva, M.F.M.; Gómez, M.M.; de Souza, P.M.; et al. Laboratory-based Rotavirus Surveillance During the Introduction of a Vaccination Program, Brazil, 2005–2009. Pediatr. Infect. Dis. J. 2011, 30, S35–S41. [Google Scholar] [CrossRef]
- Hull, J.J.; Teel, E.N.; Kerin, T.K.; Freeman, M.M.; Esona, M.D.; Gentsch, J.R.; Cortese, M.M.; Parashar, U.D.; Glass, R.I.; Bowen, M.D. United States Rotavirus Strain Surveillance from 2005 to 2008. Pediatr. Infect. Dis. J. 2011, 30, S42–S47. [Google Scholar] [CrossRef] [PubMed]
- Bányai, K.; László, B.; Duque, J.; Steele, A.D.; Nelson, E.A.S.; Gentsch, J.R.; Parashar, U.D. Systematic review of regional and temporal trends in global rotavirus strain diversity in the pre rotavirus vaccine era: Insights for understanding the impact of rotavirus vaccination programs. Vaccine 2012, 30, A122–A130. [Google Scholar] [CrossRef] [PubMed]
- Roczo-Farkas, S.; Kirkwood, C.D.; Cowley, D.; Barnes, G.L.; Bishop, R.F.; Bogdanovic-Sakran, N.; Boniface, K.; Donato, C.M.; Bines, J.E. The Impact of Rotavirus Vaccines on Genotype Diversity: A Comprehensive Analysis of 2 Decades of Australian Surveillance Data. J. Infect. Dis. 2018, 218, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, A.; Bostan, N.; Bokhari, H.; Matthijnssens, J.; Yinda, K.C.; Raza, S.; Nawaz, T. Molecular characterization of human group A rotavirus genotypes circulating in Rawalpindi, Islamabad, Pakistan during 2015–2016. PLoS ONE 2019, 14, e0220387. [Google Scholar] [CrossRef] [Green Version]
- Umair, M.; Salman, M.; Alam, M.M.; Rana, M.S.; Zaidi, S.S.Z.; Bowen, M.D.; Aamir, U.B.; Abbasi, B.H. Rotavirus surveillance in Pakistan during 2015-2016 reveals high prevalence of G12P[6]. J. Med Virol. 2018, 90, 1272–1276. [Google Scholar] [CrossRef] [PubMed]
- Nyaga, M.M.; Jere, K.C.; Esona, M.D.; Seheri, M.L.; Stucker, K.M.; Halpin, R.A.; Akopov, A.; Stockwell, T.B.; Peenze, I.; Diop, A.; et al. Whole genome detection of rotavirus mixed infections in human, porcine and bovine samples co-infected with various rotavirus strains collected from sub-Saharan Africa. Infect. Genet. Evol. 2015, 31, 321–334. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Kamiya, H.; Asada, K.; Suga, S.; Ido, M.; Umemoto, M.; Ouchi, K.; Ito, H.; Kuroki, H.; Nakano, T.; et al. Changes in Rotavirus Genotypes before and after Vaccine Introduction: A Multicenter, Prospective Observational Study in Three Areas of Japan. Jpn. J. Infect. Dis. 2017, 70, 448–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Manual of Rotavirus Detection and Characterization Methods. (2009)WHO_IVB_08.17_eng.Pdf. Available online: https://apps.who.int/iris/bitstream/handle/10665/70122/WHO_IVB_08.17_eng.pdf?sequence=1 (accessed on 19 March 2021).
- Kang, G.; Desai, R.; Arora, R.; Chitamabar, S.; Naik, T.N.; Krishnan, T.; Deshpande, J.; Gupte, M.D.; Venkatasubramaniam, S.; Gentsch, J.R.; et al. Diversity of circulating rotavirus strains in children hospitalized with diarrhea in India, 2005–2009. Vaccine 2013, 31, 2879–2883. [Google Scholar] [CrossRef]
- Iturriza-Gomara, M.; Green, J.; Brown, D.; Desselberger, U.; Gray, J. Comparison of specific and random priming in the reverse transcriptase polymerase chain reaction for genotyping group A rotaviruses. J. Virol. Methods 1999, 78, 93–103. [Google Scholar] [CrossRef]
- Babji, S.; Arumugam, R.; Sarvanabhavan, A.; Gentsch, J.R.; Kang, G. Approach to molecular characterization of partially and completely untyped samples in an Indian rotavirus surveillance program. Vaccine 2014, 32, A84–A88. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Site Name | Pre- Vaccination Period and Enrollment | Pre- Vaccination Rotavirus Positivity | Post- Vaccination Period and Enrollment | Post- Vaccination Rotavirus Positivity | Percentage Reduction in Rotavirus Positivity |
|---|---|---|---|---|---|
| Rohtak | 489 | 153 (31.2%) | 1103 | 169 (15.3%) | 50.96% |
| Tanda | 423 | 237 (56.0%) | 573 | 104 (18.1%) | 67.67% |
| Tirupati | 930 | 401 (43.1%) | 1089 | 131 (12.0%) | 72.15% |
| Bhubaneswar | 723 | 395 (54.6%) | 1113 | 379 (34.0%) | 37.72% |
| Vellore | 1598 | 470 (29.4%) | 458 | 91 (19.8%) | 32.65% |
| Total | 4163 | 1656 (39.7%) | 4336 | 874 (20.1%) | 49.37% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varghese, T.; Alokit Khakha, S.; Giri, S.; Nair, N.P.; Badur, M.; Gathwala, G.; Chaudhury, S.; Kaushik, S.; Dash, M.; Mohakud, N.K.; et al. Rotavirus Strain Distribution before and after Introducing Rotavirus Vaccine in India. Pathogens 2021, 10, 416. https://doi.org/10.3390/pathogens10040416
Varghese T, Alokit Khakha S, Giri S, Nair NP, Badur M, Gathwala G, Chaudhury S, Kaushik S, Dash M, Mohakud NK, et al. Rotavirus Strain Distribution before and after Introducing Rotavirus Vaccine in India. Pathogens. 2021; 10(4):416. https://doi.org/10.3390/pathogens10040416
Chicago/Turabian StyleVarghese, Tintu, Shainey Alokit Khakha, Sidhartha Giri, Nayana P. Nair, Manohar Badur, Geeta Gathwala, Sanjeev Chaudhury, Shayam Kaushik, Mrutunjay Dash, Nirmal K. Mohakud, and et al. 2021. "Rotavirus Strain Distribution before and after Introducing Rotavirus Vaccine in India" Pathogens 10, no. 4: 416. https://doi.org/10.3390/pathogens10040416