
Potential Parasitic Causes of Epilepsy in an Onchocerciasis Endemic Area in the Ituri Province, Democratic Republic of Congo

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Site
2.2. Study Population
2.3. Diagnosis of O. volvulus Infection
2.4. Testing for Other Parasites
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Description of the Population
3.2. Seroprevalence of O. volvulus, T. solium, T. canis and S. stercoralis in Persons with Epilepsy
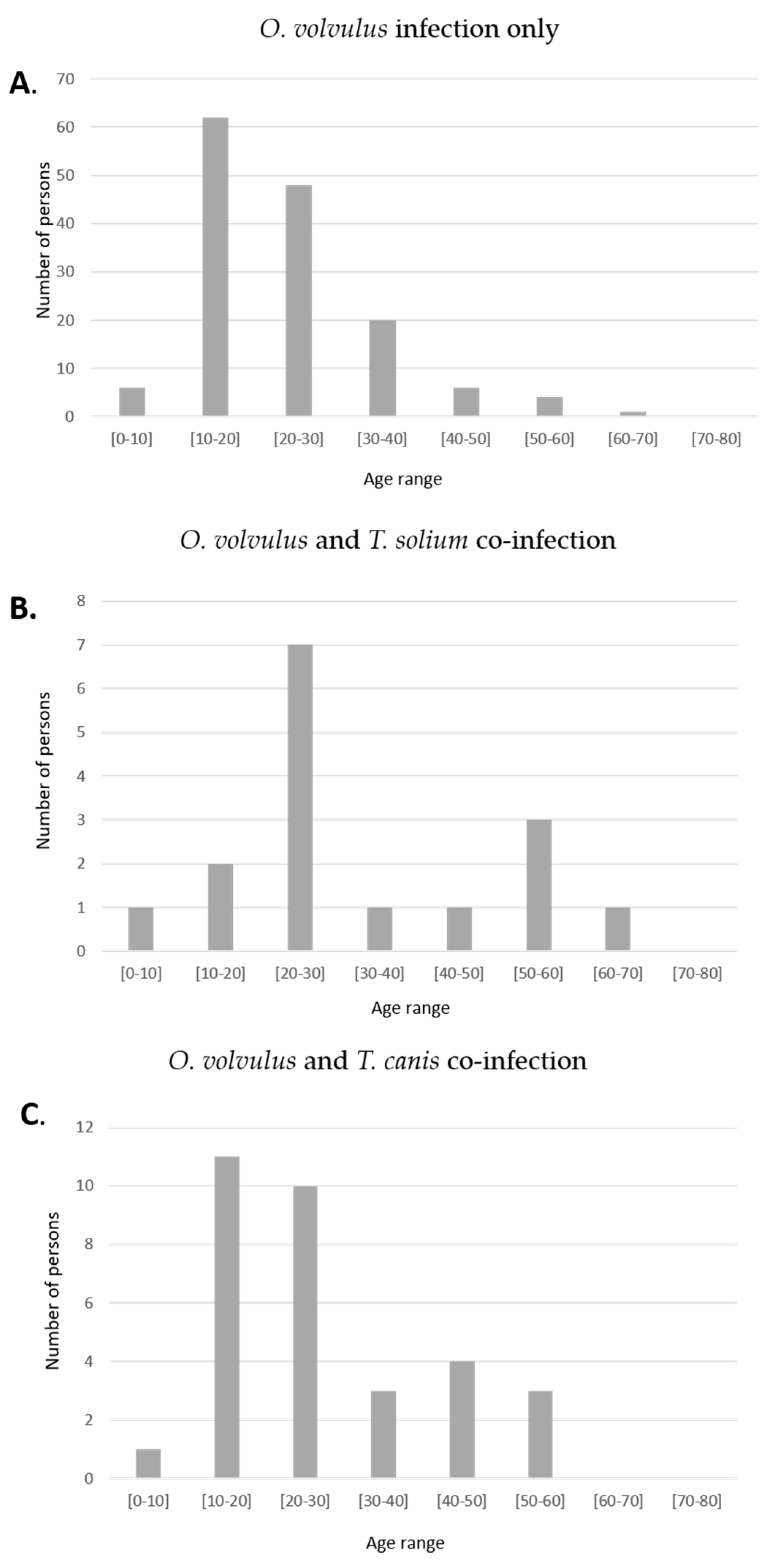
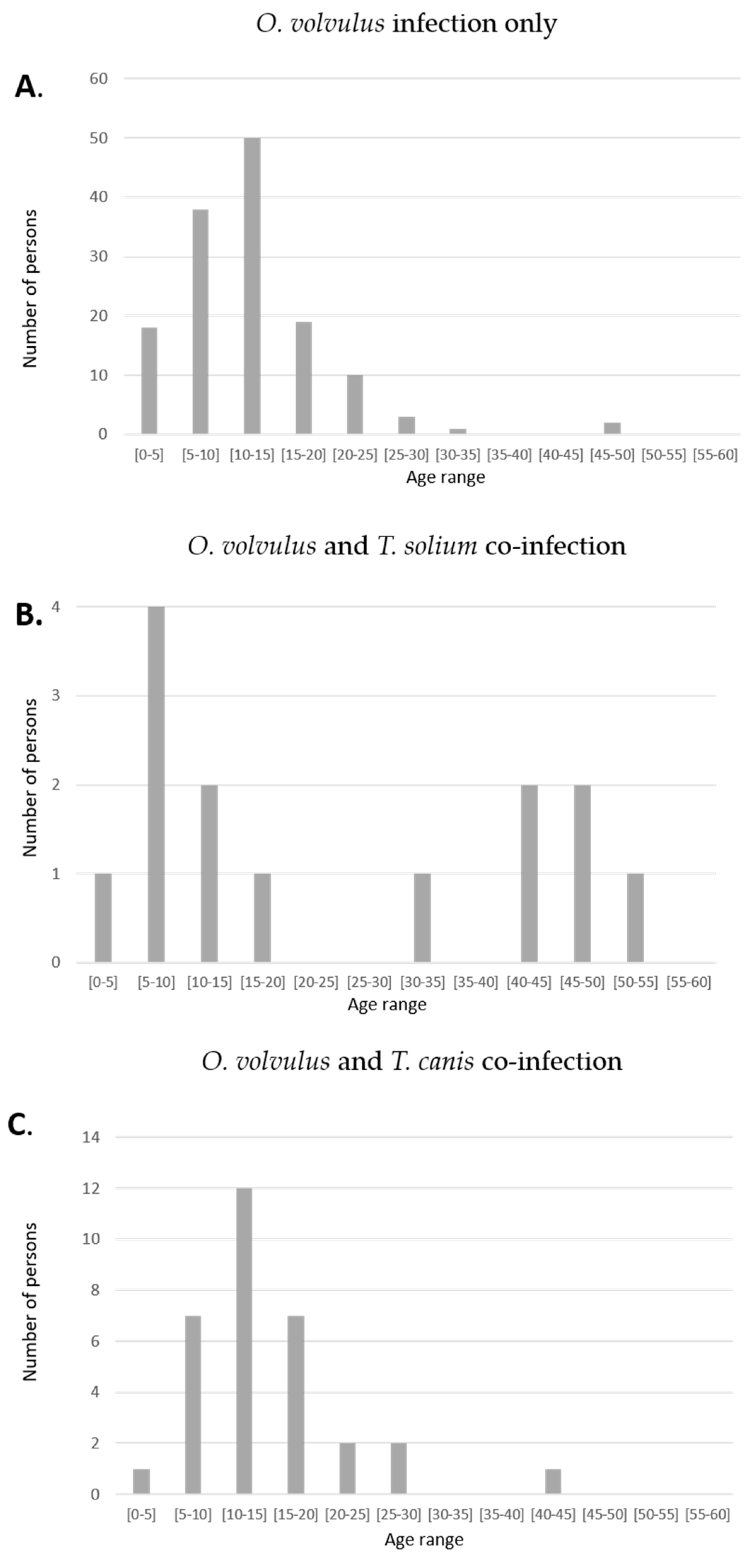
3.3. Characteristic of Co-Infected Persons with Epilepsy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Angwafor, S.A.; Bell, G.S.; Njamnshi, A.K.; Singh, G.; Sander, J.W. Parasites and epilepsy: Understanding the determinants of epileptogenesis. Epilepsy Behav. 2019, 92, 235–244. [Google Scholar] [CrossRef]
- Ngoungou, E.B.; Preux, P.M. Cerebral malaria and epilepsy. Epilepsia 2008, 49 (Suppl. 6), 19–24. [Google Scholar] [CrossRef]
- Winkler, A.S. Neurocysticercosis in sub-Saharan Africa: A review of prevalence, clinical characteristics, diagnosis, and management. Pathog. Glob. Health 2012, 106, 261–274. [Google Scholar] [CrossRef] [Green Version]
- Boussinesq, M.; Pion, S.D.; Demanga, N.; Kamgno, J. Relationship between onchocerciasis and epilepsy: A matched case-control study in the Mbam Valley, Republic of Cameroon. Trans. R. Soc. Trop. Med. Hyg. 2002, 96, 537–541. [Google Scholar] [CrossRef]
- Pion, S.D.S.; Kaiser, C.; Boutros-Toni, F.; Cournil, A.; Taylor, M.M.; Meredith, S.E.O.; Stufe, A.; Bertocchi, I.; Kipp, W.; Preux, P.-M.; et al. Epilepsy in Onchocerciasis Endemic Areas: Systematic Review and Meta-analysis of Population-Based Surveys. PLoS Negl. Trop. Dis. 2009, 3, e461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, C.; Kipp, W.; Asaba, G.; Mugisa, C.; Kabagambe, G.; Rating, D.; Leichsenring, M. The prevalence of epilepsy follows the distribution of onchocerciasis in a west Ugandan focus. Bull. World Health Organ. 1996, 74, 361–367. [Google Scholar]
- Chesnais, C.B.; Bizet, C.; Campillo, J.T.; Njamnshi, W.Y.; Bopda, J.; Nwane, P.; Pion, S.D.; Njamnshi, A.K.; Boussinesq, M. A Second Population-Based Cohort Study in Cameroon Confirms the Temporal Relationship Between Onchocerciasis and Epilepsy. Open Forum Infect. Dis. 2020, 7, ofaa206. [Google Scholar] [CrossRef]
- Chesnais, C.B.; Nana-Djeunga, H.C.; Njamnshi, A.K.; Lenou-Nanga, C.G.; Boulle, C.; Bissek, A.Z.; Kamgno, J.; Colebunders, R.; Boussinesq, M. The temporal relationship between onchocerciasis and epilepsy: A population-based cohort study. Lancet Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Colebunders, R.; Siewe Fodjo, J.N.; Hopkins, A.; Hotterbeekx, A.; Lakwo, T.L.; Kalinga, A.; Logora, M.Y.; Basanez, M.G. From river blindness to river epilepsy: Implications for onchocerciasis elimination programmes. PLoS Negl. Trop. Dis. 2019, 13, e0007407. [Google Scholar] [CrossRef] [Green Version]
- Idro, R.; Opoka, R.O.; Aanyu, H.T.; Kakooza-Mwesige, A.; Piloya-Were, T.; Namusoke, H.; Musoke, S.B.; Nalugya, J.; Bangirana, P.; Mwaka, A.D.; et al. Nodding syndrome in Ugandan children—clinical features, brain imaging and complications: A case series. BMJ Open 2013, 3, e002540. [Google Scholar] [CrossRef] [Green Version]
- Colebunders, R.; Nelson Siewe, F.J.; Hotterbeekx, A. Onchocerciasis-Associated Epilepsy, an Additional Reason for Strengthening Onchocerciasis Elimination Programs. Trends Parasitol. 2018, 34, 208–216. [Google Scholar] [CrossRef]
- Föger, K.; Gora-Stahlberg, G.; Sejvar, J.; Ovuga, E.; Jilek-Aall, L.; Schmutzhard, E.; Kaiser, C.; Winkler, A.S. Nakalanga Syndrome: Clinical Characteristics, Potential Causes, and Its Relationship with Recently Described Nodding Syndrome. PLoS Negl. Trop. Dis. 2017, 11, e0005201. [Google Scholar] [CrossRef]
- Hotterbeekx, A.; Raimon, S.; Abd-Elfarag, G.; Carter, J.Y.; Sebit, W.; Suliman, A.; Siewe Fodjo, J.N.; De Witte, P.; Logora, M.Y.; Colebunders, R.; et al. Onchocerca volvulus is not detected in the cerebrospinal fluid of persons with onchocerciasis-associated epilepsy. Int. J. Infect. Dis. Off. Publ. Int. Soc. Infect. Dis. 2019, 91, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotterbeekx, A.; Lammens, M.; Idro, R.; Akun, P.R.; Lukande, R.; Akena, G.; Nath, A.; Taylor, J.; Olwa, F.; Kumar-Singh, S.; et al. Neuroinflammation and Not Tauopathy Is a Predominant Pathological Signature of Nodding Syndrome. J. Neuropathol. Exp. Neurol. 2019, 78, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Colebunders, R.; Njamnshi, A.K.; Menon, S.; Newton, C.R.; Hotterbeekx, A.; Preux, P.-M.; Hopkins, A.; Vaillant, M.; Siewe Fodjo, J.N. Onchocerca volvulus and epilepsy: A comprehensive review using the Bradford Hill criteria for causation. PLoS Negl. Trop. Dis. 2021, 15, e0008965. [Google Scholar] [CrossRef]
- Foltz, J.L.; Makumbi, I.; Sejvar, J.J.; Malimbo, M.; Ndyomugyenyi, R.; Atai-Omoruto, A.D.; Alexander, L.N.; Abang, B.; Melstrom, P.; Kakooza, A.M.; et al. An Epidemiologic Investigation of Potential Risk Factors for Nodding Syndrome in Kitgum District, Uganda. PLoS ONE 2013, 8, e66419. [Google Scholar] [CrossRef] [Green Version]
- Lenaerts, E.; Mandro, M.; Mukendi, D.; Suykerbuyk, P.; Dolo, H.; Wonya’Rossi, D.; Ngave, F.; Ensoy-Musoro, C.; Laudisoit, A.; Hotterbeekx, A.; et al. High prevalence of epilepsy in onchocerciasis endemic health areas in Democratic Republic of the Congo. Infect. Dis. Poverty 2018, 7, 68. [Google Scholar] [CrossRef]
- Mandro, M.; Suykerbuyk, P.; Tepage, F.; Rossy, D.; Ngave, F.; Hasan, M.N.; Hotterbeekx, A.; Mambandu, G.; Kashama, J.M.; Laudisoit, A.; et al. Onchocerca volvulus as a risk factor for developing epilepsy in onchocerciasis endemic regions in the Democratic Republic of Congo: A case control study. Infect. Dis. Poverty 2018, 7, 79. [Google Scholar] [CrossRef] [PubMed]
- Mandro, M.; Siewe Fodjo, J.N.; Dusabimana, A.; Mukendi, D.; Haesendonckx, S.; Lokonda, R.; Nakato, S.; Nyisi, F.; Abhafule, G.; Wonya’rossi, D.; et al. Single versus Multiple Dose Ivermectin Regimen in Onchocerciasis-Infected Persons with Epilepsy Treated with Phenobarbital: A Randomized Clinical Trial in the Democratic Republic of Congo. Pathogens 2020, 9, 205. [Google Scholar] [CrossRef] [Green Version]
- Boscolo, M.; Gobbo, M.; Mantovani, W.; Degani, M.; Anselmi, M.; Monteiro, G.B.; Marocco, S.; Angheben, A.; Mistretta, M.; Santacatterina, M.; et al. Evaluation of an indirect immunofluorescence assay for strongyloidiasis as a tool for diagnosis and follow-up. Clin. Vaccine Immunol. 2007, 14, 129–133. [Google Scholar] [CrossRef] [Green Version]
- van Doorn, H.R.; Koelewijn, R.; Hofwegen, H.; Gilis, H.; Wetsteyn, J.C.; Wismans, P.J.; Sarfati, C.; Vervoort, T.; van Gool, T. Use of enzyme-linked immunosorbent assay and dipstick assay for detection of Strongyloides stercoralis infection in humans. J. Clin. Microbiol. 2007, 45, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic accuracy of five serologic tests for Strongyloides stercoralis infection. PLoS Negl. Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [Green Version]
- López-Hernández, A.; Garaizar, C. Childhood Cerebral Cysticercosis: Clinical Features and Computed Tomographic Findings in 89 Mexican Children. Can. J. Neurol. Sci. 1982, 9, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, L.; Nunes, B.; Mendonça, D.; Lopes, J. Spectrum of epilepsy in neurocysticercosis: A long-term follow-up of 143 patients. Acta Neurol. Scand. 1995, 92, 33–40. [Google Scholar] [CrossRef]
- Singhi, P. Neurocysticercosis. Ther. Adv. Neurol. Disord. 2011, 4, 67–81. [Google Scholar] [CrossRef]
- Tsang, V.C.; Brand, J.A.; Boyer, A.E. An enzyme-linked immunoelectrotransfer blot assay and glycoprotein antigens for diagnosing human cysticercosis (Taenia solium). J. Infect. Dis. 1989, 159, 50–59. [Google Scholar] [CrossRef]
- Del Brutto, O.H. Diagnostic criteria for neurocysticercosis, revisited. Pathog. Glob. Health 2012, 106, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, H.H.; O’Neal, S.E.; Noh, J.; Handali, S. Laboratory Diagnosis of Neurocysticercosis (Taenia solium). J. Clin. Microbiol. 2018, 56, e00424-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montano, S.M.; Villaran, M.V.; Ylquimiche, L.; Figueroa, J.J.; Rodriguez, S.; Bautista, C.T.; Gonzalez, A.E.; Tsang, V.C.; Gilman, R.H.; Garcia, H.H. Neurocysticercosis: Association between seizures, serology, and brain CT in rural Peru. Neurology 2005, 65, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Garcia, H.H.; Gonzalez, A.E.; Gilman, R.H.; Palacios, L.G.; Jimenez, I.; Rodriguez, S.; Verastegui, M.; Wilkins, P.; Tsang, V.C. Short report: Transient antibody response in Taenia solium infection in field conditions-a major contributor to high seroprevalence. Am. J. Trop. Med. Hyg. 2001, 65, 31–32. [Google Scholar] [CrossRef]
- Quattrocchi, G.; Nicoletti, A.; Marin, B.; Bruno, E.; Druet-Cabanac, M.; Preux, P.-M. Toxocariasis and Epilepsy: Systematic Review and Meta-Analysis. PLoS Negl. Trop. Dis. 2012, 6, e1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luna, J.; Cicero, C.E.; Rateau, G.; Quattrocchi, G.; Marin, B.; Bruno, E.; Dalmay, F.; Druet-Cabanac, M.; Nicoletti, A.; Preux, P.-M. Updated evidence of the association between toxocariasis and epilepsy: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006665. [Google Scholar] [CrossRef] [PubMed]
- Kamuyu, G.; Bottomley, C.; Mageto, J.; Lowe, B.; Wilkins, P.P.; Noh, J.C.; Nutman, T.B.; Ngugi, A.K.; Odhiambo, R.; Wagner, R.G.; et al. Exposure to multiple parasites is associated with the prevalence of active convulsive epilepsy in sub-Saharan Africa. PLoS Negl. Trop. Dis. 2014, 8, e2908. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| O. volvulus and T. solium Infection (N = 16) | O. volvulus and T. canis Infection (N = 32) 2 | O. volvulus Only 1 (N = 147) | p-Value * | p-Value ** | |
|---|---|---|---|---|---|
| Age, Median (IQR) | 27 (21–51) | 23.5 (16-35) | 22 (16–30) | 0.021 | 0.130 |
| Men, N (%) 3 | 13 (81.3%) | 19 (59.4%) | 71 (48.3%) | 0.012 | 0.26 |
| Age at onset of the epilepsy, Median (IQR) | 14 (9–45) | 13.5 (10–19.5) | 12 (8–15) | 0.122 | 0.051 |
| Generalised tonic–clonic seizures, N (%) | 14 (87.5%) | 32 (100%) | 131 (89.1%) | 0.845 | NA |
| Nodding seizures, N (%) | 1 (6%) | 2 (6.3%) | 24 (16.3%) | 0.288 | 0.143 |
| Absences, N (%) | 7 (43.7%) | 9 (28.2%) | 63 (42.9%) | 0.945 | 0.123 |
| Focal seizures with loss of consciousness, N (%) | 2 (12.5%) | 0(0%) | 25 (17%) | 0.523 | <0.0001 |
| Focal seizures without loss of consciousness, N (%) | 2 (12.5%) | 1 (3.1%) | 3 (2%) | 0.021 | 0.707 |
| Skin snip, N (%) | 13 (81.3%) | 28 (87.5%) | 115 (78.23%) | 0.78 | 0.236 |
| Mf load, Median (IQR) | 4 (1.25–11.25) | 10 (1–10) | 9 (0–67) | 0.385 | 0.907 |
| Seroprevalence (N = 195) | |
|---|---|
| T. solium (WB), N (%) | 16 (8.2%) |
| T. canis (ELISA), N (%) | 36 (18.5%) |
| Strongyloides (IFAT + ELISA), N (%) | 25 (12.8%) |
| Nr | Age | Sex | Age of Seizures Onset | Generlized TCS | Nodding Seizures | Absences | Focal Seizures |
|---|---|---|---|---|---|---|---|
| 1 | 10 | M | 8 | YES | YES | YES | YES * |
| 2 | 19 | F | 5 | YES | NO | YES | NO |
| 3 | 20 | M | 20 | YES | NO | NO | YES ** |
| 4 | 21 | M | 14 | YES | NO | YES | NO |
| 5 | 22 | F | 9 | YES | NO | NO | NO |
| 6 | 23 | M | 9 | YES | NO | NO | YES *** |
| 7 | 24 | M | 7 | YES | NO | NO | NO |
| 8 | 27 | M | 11 | YES | NO | YES | NO |
| 9 | 27 | M | 12 | YES | NO | YES | NO |
| 10 | 29 | M | 10 | YES | NO | YES | YES * |
| 11 | 34 | M | 31 | YES | NO | NO | NO |
| 12 | 50 | F | 44 | YES | NO | YES | NO |
| 13 | 51 | M | 49 | YES | NO | NO | NO |
| 14 | 52 | M | 45 | YES | NO | NO | NO |
| 15 | 60 | M | 53 | YES | NO | NO | NO |
| 16 | 65 | M | 47 | YES | NO | NO | NO |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vieri, M.K.; Mandro, M.; Cardellino, C.S.; Orza, P.; Ronzoni, N.; Siewe Fodjo, J.N.; Hotterbeekx, A.; Colebunders, R. Potential Parasitic Causes of Epilepsy in an Onchocerciasis Endemic Area in the Ituri Province, Democratic Republic of Congo. Pathogens 2021, 10, 359. https://doi.org/10.3390/pathogens10030359
Vieri MK, Mandro M, Cardellino CS, Orza P, Ronzoni N, Siewe Fodjo JN, Hotterbeekx A, Colebunders R. Potential Parasitic Causes of Epilepsy in an Onchocerciasis Endemic Area in the Ituri Province, Democratic Republic of Congo. Pathogens. 2021; 10(3):359. https://doi.org/10.3390/pathogens10030359
Chicago/Turabian StyleVieri, Melissa Krizia, Michel Mandro, Chiara Simona Cardellino, Pierantonio Orza, Niccolò Ronzoni, Joseph Nelson Siewe Fodjo, An Hotterbeekx, and Robert Colebunders. 2021. "Potential Parasitic Causes of Epilepsy in an Onchocerciasis Endemic Area in the Ituri Province, Democratic Republic of Congo" Pathogens 10, no. 3: 359. https://doi.org/10.3390/pathogens10030359