
Biofilm Formation of Clinical Klebsiella pneumoniae Strains Isolated from Tracheostomy Tubes and Their Association with Antimicrobial Resistance, Virulence and Genetic Diversity

Abstract
:1. Introduction
2. Results
2.1. Patients’ Clinical Characteristics
2.2. Antimicrobial Resistance Pattern
2.3. ESβL Gene Detection
2.4. PCR Detection of Fimbrial Genes
2.5. Biofilm Production
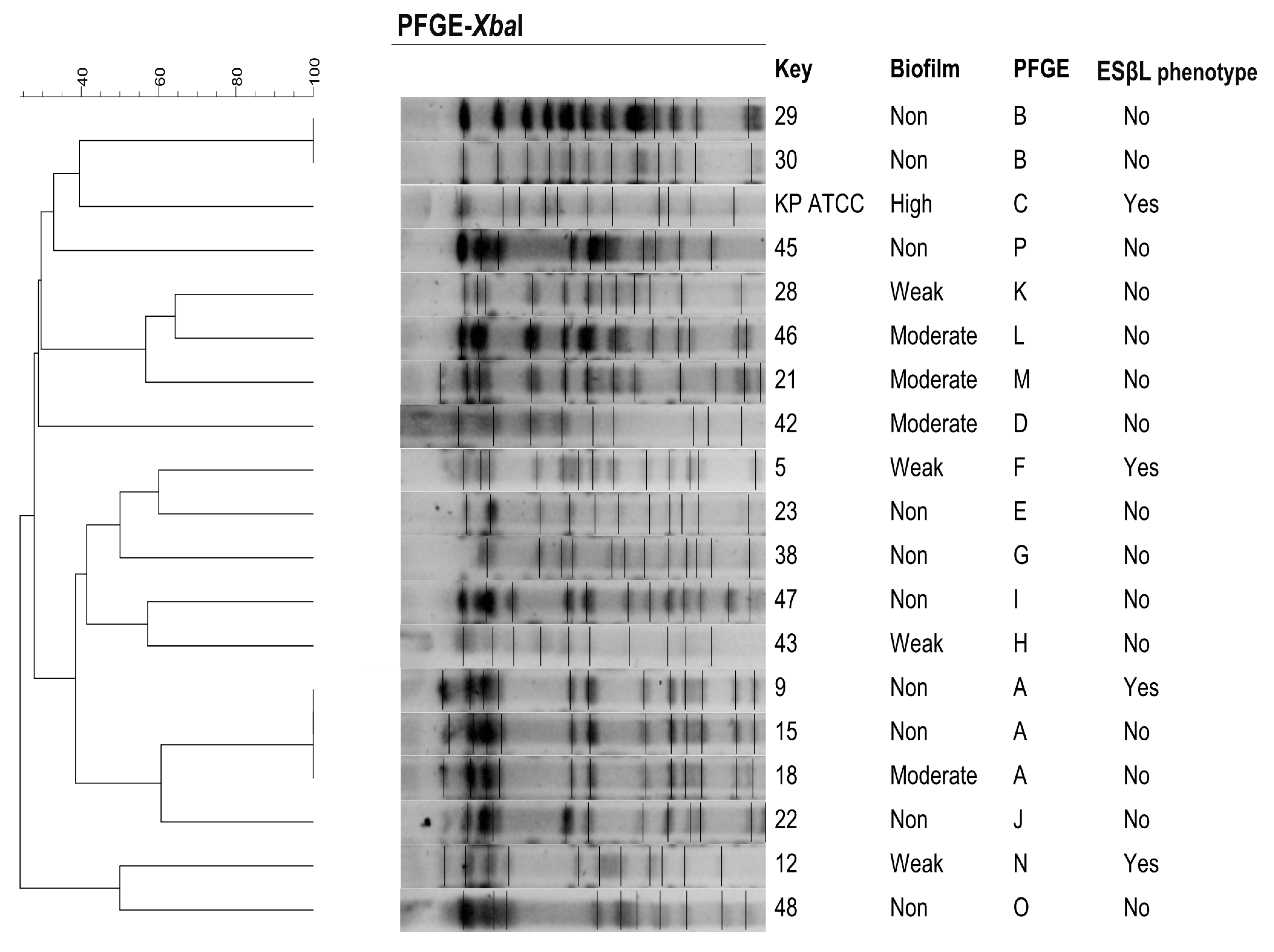
2.6. PFGE
2.7. SEM
3. Discussion
4. Materials and Methods
4.1. Ethical Approval
4.2. Bacterial Strains, Identification and Growth Conditions
4.3. Antibiotic Susceptibility Testing
4.4. Biofilm Production Assay
4.5. Multiplex PCRs for β-Lactamase Encoding Genes (blaSHV, blaTEM and blaCTX-M-type)
4.6. PCR Detection of Fimbrial Genes
4.7. Genotyping by Pulsed-Field Gel Electrophoresis (PFGE)
4.8. Scanning Electron Microscopy (SEM)
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cader, S.H.A.; Shah, F.A.; Nair, S.K.G.R. Tracheostomy colonisation and microbiological isolates of patients in intensive careunits—A retrospective study. World J. Otorhinolaryngol.-Head Neck Surg. 2020, 6, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Weissbrod, P.A.; Merati, A.L. Is percutaneous dilational tracheotomy equivalent to traditional open surgical tracheotomy with regard to perioperative and postoperative complications? Laryngoscope 2012, 122, 1423–1424. [Google Scholar] [CrossRef] [PubMed]
- Szmuk, P.; Ezri, T.; Evron, S.; Roth, Y.; Katz, J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the Space Age. Intensive Care Med. 2008, 34, 222–228. [Google Scholar] [CrossRef]
- Percival, S.L.; Suleman, L.; Vuotto, C.; Donelli, G. Healthcare-Associated infections, medical devices and biofilms: Risk, tolerance and control. J. Med. Microbiol. 2015, 64, 323–334. [Google Scholar] [CrossRef] [Green Version]
- El Cheikh, M.R.; Barbosa, J.M.; Caixêta, J.A.S.; Avelino, M.A.G. Microbiology of tracheal secretions: What to expect with children and adolescents with tracheostomies. Int. Arch. Otorhinolaryngol. 2018, 22, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Rouzé, A.; Jaillette, E.; Poissy, J.; Préau, S.; Nseir, S. Tracheal tube design and ventilator-associated pneumonia. Respir. Care. 2017, 62, 1316–1323. [Google Scholar] [CrossRef] [Green Version]
- Chastre, J.; Fagon, J. State of the Art Ventilator-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef]
- Lepainteur, M.; Ogna, A.; Clair, B.; Dinh, A.; Tarragon, C.; Prigent, H.; Davido, B.; Barbot, F.; Vaugier, I.; Afif, M.; et al. Risk factors for respiratory tract bacterial colonization in adults with neuromuscular or neurological disorders and chronic tracheostomy. Respir. Med. 2019, 152, 32–36. [Google Scholar] [CrossRef]
- McAfee, J.S.; Demarcantonio, M.; Fine, B.R.; Beydoun, H.; Derkay, C. Prevalence of ventilation tubes in children with a tracheostomy tube. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.Y. The emerging problems of infections: Carbapenem resistance and biofilm formation. FEMS Microbiol. Lett. 2016, 363, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryers, J.D. Medical biofilms. Biotechnol. Bioeng. 2008, 100, 1–18. [Google Scholar] [CrossRef]
- Piperaki, E.T.; Syrogiannopoulos, G.A.; Tzouvelekis, L.S.; Daikos, G.L. Klebsiella pneumoniae: Virulence, Biofilm and Antimicrobial Resistance. Pediatr. Infect. Dis. J. 2017, 36, 1002–1005. [Google Scholar] [CrossRef]
- Solomon, D.H.; Wobb, J.; Buttaro, B.A.; Truant, A.; Soliman, A.M.S. Characterization of bacterial biofilms on tracheostomy tubes. Laryngoscope 2009, 119, 1633–1638. [Google Scholar] [CrossRef] [Green Version]
- Alcántar-Curiel, M.D.; Ledezma-Escalante, C.A.; Jarillo-Quijada, M.D.; Gayosso-Vázquez, C.; Morfín-Otero, R.; Rodríguez-Noriega, E.; Cedillo-Ramirez, M.L.; Santos-Preciado, J.I.; GirÓn, J.A. Association of Antibiotic Resistance, Cell Adherence, and Biofilm Production with the Endemicity of Nosocomial Klebsiella pneumoniae. BioMed Res. Int. 2018, 2018, 7012958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifi, K.; Kazemian, H.; Heidari, H.; Rezagholizadeh, F.; Saee Shirvani, F.; Houri, H. Evaluation of biofilm formation among Klebsiella pneumoniae isolates and molecular characterization by ERIC-PCR. Jundishapur J. Microbiol. 2016, 9, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Córdova, A.; Esteban-Kenel, V.; Espinosa-Mazariego, K.; Ochoa, S.A.; Espinosa, M.; de la Garza, D.; Fenández RendÓn, E.; LÓpez Villegas, E.O.; Xicothencotl-Cortes, J. Hospital Infantil de México Pathogenic determinants of clinical Klebsiella pneumoniae strains. Bol. Med. Hosp. Infant. Mex. 2014, 71, 15–24. [Google Scholar]
- Samia, B.; Hafida, H.; Damien, B.; Nicolas, C.; Imane, M.H.; Ibtissem, K.T.; Merieme, L.; Wafae, D.; Christiane, F. Evaluation of biofilm formation of Klebsiella pneumoniae isolated from medical devices at the University Hospital of Tlemcen, Algeria. African J. Microbiol. Res. 2013, 7, 5558–5564. [Google Scholar] [CrossRef] [Green Version]
- Inglis, T.J.J.; Millar, M.R.; Jones, J.G.; Robinson, D.A. Tracheal tube biofilm as a source of bacterial colonization of the lung. J. Clin. Microbiol. 1989, 27, 2014–2018. [Google Scholar] [CrossRef] [Green Version]
- LeChevallier, M.W.; Cawthon, C.D.; Lee, R.G. Inactivation of biofilm bacteria. Appl. Environ. Microbiol. 1988, 54, 2492–2499. [Google Scholar] [CrossRef] [Green Version]
- Poelaert, J.; Pieter Depuydt, P.; De Wolf, A.; Van de Velde, S.; Herck, I.; Blot, S. Polyurethane cuffed endotracheal tubes to prevent early postoperative pneumonia after cardiac surgery: A pilot study. J. Thorac. Cardiovasc. Surg. 2008, 135, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmodiyeh, B.; Kamali, A.; Zarinfar, N.; Mohammadi Joushani, M. The Effect Of Silver-Coated Endotracheal Tube On The Incidence Of Ventilator-Induced Pneumonia In Intubated Patients Admitted To The Intensive Care Unit (ICU). Syst. Rev. Pharm. 2021, 12, 254–262. [Google Scholar]
- Kollef, M.H.; Afessa, B.; Anzueto, A.; Veremakis, C.; Kerr, K.M.; Margolis, B.D.; Craven, D.E.; Roberts, P.R.; Arroliga, A.C.; Hubmayr, R.D.; et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: The NASCENT randomized trial. JAMA 2008, 300, 805–813. [Google Scholar] [CrossRef] [Green Version]
- Thorarinsdottir, H.R.; Kander, T.; Holmberg, A.; Petronis, S.; Klarin, B. Biofilm formation on three different endotracheal tubes: A prospective clinical trial. Crit. Care 2020, 24, 382. [Google Scholar] [CrossRef]
- Mann, E.E.; Magin, C.M.; Mettetal, M.R.; May, R.M.; Henry, M.M.; Deloid, H.; Prater, J.; Sullivan, L.; Thomas, J.G.; Twite, M.D.; et al. Micropatterned Endotracheal Tubes Reduce Secretion-Related Lumen Occlusion. Ann. Biomed. Eng. 2016, 44, 3645–3654. [Google Scholar] [CrossRef] [Green Version]
- Pinciroli, R.; Mietto, C.; Piriyapatsom, A.; Chenelle, C.T.; Thomas, J.G.; Pirrone, M.; Bry, L.; Wojtkiewicz, G.R.; Nahrendorf, M.P.; Kacmarek, R.M.; et al. Endotracheal Tubes Cleaned With a Novel Mechanism for Secretion Removal: A Randomized Controlled Clinical Study. Respir. Care. 2016, 61, 1431–1439. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.K.; Basukala, P.; Basukala, O.; Parajuli, K.; Pokhrel, B.M.; Rijel, B.P. Detection of Biofilm Production and Antibiotic Resistance Pattern in Clinical Isolates from Indwelling Medical Devices. Curr. Microbiol. 2014, 70, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Lin, Z.W.; Chen, C.; Chen, Z.; Lin, F.J.; Wu, Y.; Yang, S.-Y.; Sun, X.; Yao, W.-M.; Li, D.-Y.; et al. Biofilm formation in Klebsiella pneumoniae bacteremia strains was found to be associated with CC23 and the presence of wcaG. Front. Cell Infect. Microbiol. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latifpour, M.; Gholipour, A.; Damavandi, M.S. Prevalence of extended-spectrum beta-lactamase-producing Klebsiella pneumoniae isolates in nosocomial and community-acquired urinary tract infections. Jundishapur J. Microbiol. 2016, 9, e31179. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Ensor, V.; Gossain, S.; Nye, K.; Hawkey, P. Rapid and simple detection of bla CTX-M genes by multiplex PCR assay. J. Med. Microbiol. 2005, 54, 1183–1187. [Google Scholar] [CrossRef]
- Christensen, G.D.; Simpson, W.A.; Younger, J.J.; Baddour, L.M.; Barrett, F.F.; Melton, D.M.; Beachey, E.H. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: A quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbiol. 1985, 22, 996–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepanović, S.; Vuković, D.; Hola, V.; Di Bonaventura, G.; Djukić, S.; Ćirković, I.; Ruzicka, F. Quantification of biofilm in microtiter plates: Overview of testing conditions and practical recommendations for assessment of biofilm production by staphylo-484 cocci. Apmis 2007, 115, 891–899. [Google Scholar] [CrossRef]
- Hassan, A.; Usman, J.; Kaleem, F.; Omair, M.; Khalid, A.; Iqbal, M. Evaluation of different detection methods of biofilm formation in the clinical isolates. Braz. J. Infect. Dis. 2011, 15, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Kuinkel, S.; Acharya, J.; Dhungel, B.; Adhikari, S.; Adhikari, N.; Thapa Shrestha, U.; Megha Raj Banjara, M.; Raj Rijal, K.; Ghimire, P. Biofilm Formation and Phenotypic Detection of ESBL, MBL, KPC and AmpC Enzymes and Their Coexistence in Klebsiella spp. Isolated at the National Reference Laboratory, Kathmandu, Nepal. Microbiol. Res. 2021, 12, 683–697. [Google Scholar] [CrossRef]
- Silva, B.S.N.; Alves, G.V.P.; de Andrade Marques, L.; Silva, S.F.S.; de Oliveira Faria, G.; de Araújo, B.L.; dos Santos Pedroso, R.; Penatti, A.P.M.; de Paula Menezes, R.; von Dolinger de Brito, R. ‘Duantification of biofilm produced by clinical, environment and hands’ isolates Klebsiella species using colorimetric and classical methods. J. Microbiol. Methods 2021, 185, 106231. [Google Scholar] [CrossRef] [PubMed]
- Alcántar- Curiel, M.D.; Blackburn, D.; Saldaña, Z.; Gayosso-Vázquez, C.; Iovine, N.; De la Cruz, M.A.; GirÓn, J.A. Multifunctional analysis of Klebsiella pneumoniae fimbrial types in adherence and biofilm formation. Virulence 2013, 4, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Zhou, H.; Li, H.; Gao, Y.; Lu, Z.; Hu, K. Optimization of Pulse-Field Gel Electrophoresis for Subtyping of Klebsiella pneumoniae. Int. J. Enviromental Res. Public Health 2013, 10, 2720–2731. [Google Scholar] [CrossRef] [Green Version]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Björling, G.; Axelsson, S.; Johansson, U.B.; Lysdahl, M.; Markström, A.; Schedin, U.; Aune, R.E.; Frostell, C.; Karlsson, S. Clinical use and material wear of polymeric tracheostomy tubes. Laryngoscope 2007, 117, 1552–1559. [Google Scholar] [CrossRef]
- EUCAST. European Committee on Antimicrobial Susceptibility Testing Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 9.0, Valid from 2019-01-01. Available online: http//www.eucast.org (accessed on 1 January 2019).
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; CLSI supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; p. 282. [Google Scholar]
- Jarrett, W.A.; Ribes, J.; Manaligod, J.M. Biofilm formation on tracheostomy tubes. Ear Nose Throat J. 2002, 81, 659–661. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No. | Patient ID/Isolate No. | Age (Years)/Sex | Hospital Ward(s) | Lenght of Stay in the Ward | Final Diagnosis. ICD9 Treatments/Procedures/Consultation | Antibiotic Treatment |
|---|---|---|---|---|---|---|
| 1. | 5 | 98/M | ORL | 31.07–03.08.2017 | Dyspnoea. A tumor in the larynx. Endoscopic laryngeal biopsy. Emergency tracheostomy. Laryngeal microsurgery using the Kleinsasser instrument set. | Amoxicillin + Clavulanic acid |
| 2. | 9 | 68/M | ORL | 11.12–15.12.2018 | Laryngeal cancer (Carcinoma planoepitheliale GII). Dyspnoea. Permanent tracheostomy. | Amoxicillin + Clavulanic acid |
| 3. | 12 | 77/M | ORL | 20.11–22.12.2018 | Laryngeal cancer (Squamous cell carcinoma GIII, Carcinoma planoepitheliale laryngis GIII). Extended excision of regional lymph nodes. Excision of the larynx and pharynx. Esophageal repair procedures. | Amoxicillin + Clavulanic acid, Ciprofloxacin |
| 4. | 15 | 93/F | OAIT | 18.10–29.11.2018 | Gastrointestinal obstruction. Exploratory laparotomy. Sigmoid tumor excision (adenocarcinoma of the colon). Peroration of the ascending colon in the course of surgery. Relaparotomy. Necrosis of the caecum due to ischemia. Diffuse peritonitis. Acute circulatory and respiratory failure. Multiple organ failure. Dementia syndrome. Chronic respiratory failure. Temporary tracheostomy. Sepsis. Death. | Ampicillin + Sulbactam, Ciprofloxacin, Fluconzole, Gentamicin, Meropenem |
| 5. | 18 | 90/F | OAIT | 15.11.2018–03.01.2019 | Septic shock. Acute respiratory failure. State after aspiration of gastric contents. Aspiration pneumonia. Status after a stroke of the right hemisphere of the brain. Left-sided hemiparesis. Epilepsy of vascular aetiology. Type 2 diabetes. Goiter of the thyroid gland with displacement of the trachea. Ischemic heart disease. Persistent atrial fibrillation. Coaulopa thy resulting from acenocoumarol overdose. Hypertension. Condition after left femoral neck fracture. State after amputation of the lower right limb. Temporary tracheostomy. Death. | Ampicillin + Sulbactam, Clindamycin, Piperacillin + Tazobactam, Vancomycin |
| 6. | 21 | 75/M | ORL | 21.01–08.02.2019 | Squamous cell carcinoma of the larynx GII. Status after right-sided pneumectomy due to squamous cell carcinoma of the lung followed by radiotherapy due to cancer infiltration in the bronchial stump. Hypertension. Complete removal of the larynx with simultaneous reconstruction of the cervical esophagus. Tracheostomy. | Amoxicillin + Clavulanic acid, Metronidazole |
| 7. | 22 | 61/M | ORL | 23.01–25.01.2019 | Carcinoma planoepitheliale laryngis GII. | |
| 8. | 23 | 65/M | ORL | 17.01–20.01.2019 | Suspicion of recurrence of laryngeal cancer. Status after radiotherapy for laryngeal cancer. Permanent tracheostomy. | Amoxicillin + Clavulanic acid |
| 9. | 28 | 69/M | ORL | 01.03–12.03.2019 | Carcinoma planoepitheliale laryngis GI. Condition after duodenal ulcer bleeding. Acute haemorrhagic anemia. Hyperten sion. Type 2 diabetes. Condition after myocardial infarction. Total laryngectomy. Removal of the neck lymph nodes on the right side. Esophageal surgery. | Amoxicillin + Clavulanic acid |
| 10. | 29 | 89/M | ORL | 06.03–27.03.2019 | Recurrence of laryngeal squamous cell carcinoma GII. Condition after radiotherapy and partial surgery. Total laryngectomy. Esophageal surgery. | Amoxicillin + Clavulanic acid |
| 11. | 30 | 74/M | OAIT | 15.03–07.04.2019 | Acute respiratory failure. Hypercapnia. Respiratory acidosis. Persistent atrial fibrillation. Hypertension. Condition after cholecystectomy. Condition after myocardial infarction. Pulmonary hypertension. Tracheostomy. Puncture of the pleural cavities. Blood transfusion. Respirator therapy. | Colistin, Imipenem, Vancomycin |
| 2. | 38 | 88/F | OAIT | 14.05–19.06.2019 | Stroke. Chronic respiratory failure. Chronic heart failure. Persistent atrial fibrillation. Condition after ICD implantation. Status after PCI LAD. Hypertension. Pulmonary hypertension. Insulin-dependent type 2 diabetes mellitus. Tracheostomy. Craniotomy for a subarachnoid hematoma. | Ciprofloxacin, Meropenem |
| 13. | 42 | 84/F | OAIT | 03.10–28.11.2018 | Chronic respiratory failure. Tracheostomy. Acute postoperative respiratory failure. Condition after fronto-temporo-parital craniotomy due to acute subdural hematoma over the right hemisphere. Status after iatrogenic gastrointestinal perforation. Hypertension. Digestive tract cancer (area of the ma jor duodenal papilla). Cancer cachexia. Hypoalbuminemia. History of gastric polyp. Dysphagia. Type 2 diabetes mellitus. | Amoxicillin + Clavulanic acid, Gentamicin, Piperacillin + Tazobactam |
| 14. | 43 | 65/F | ORL | 27.11–17.12.2018 | Cancer of the middle throat and left side of the tongue (recurrent). State after RTH-CHTH in 2012. Partial pharygetomy. Exploring the neck area through the incision. One-sided radical neck dissection. Throat repair operations other. | Amoxicillin + Clavulanic acid, Ceftazidime, Cefuroxime, Metronidazole |
| 15. | 45 | 95/F | OAIT | 23.08–20.09.2019 | Oedema pulmonalis, COPD, brain infarction, insulin-dependent type 2 diabetes mellitus. Hypertension. Ischemic heart disease. Alcohol dependence syndrome. Liver damage. Tra cheostomy. Respirator therapy. | Ceftriaxone, Cefuroxime, Levofloxacin |
| 16. | 46 | 70/M | ORL | 12.09–14.09.2019 | Acute respiratory failure in the course of laryngeal cancer. End-stage renal failure during renal replacement therapy. Hypertension. Ischemic heart disease. Status after STEMI. Secondary hypoparathyroidism. Tracheostomy. | Ampicillin |
| 17. | 47 | 65/M | ORL | 26.11–17.12.2019 | Recurrence of laryngeal squamous cell carcinoma GII. Condition after partial laryngectomy. Total laryngectomy. Purulent fistula starting 4 days after surgery (K. pneumoniae in swab). | Clindamycin, Ceftriaxone, Ciprofloxacin |
| 18. | 48 | 61/M | ORL | 27.10–20.11.2019 | Laryngeal squamous cell carcinoma GII. Excision of the larynx and pharynx. Bilateral lymph node removal. Esophageal surgery. | Amoxicillin + Clavulanic acid, Ciprofloxacin |
| Microorganism Klebsiella pneumoniae | n (%) 18 (100) | Resistance (%) |
|---|---|---|
| Penicillins | ||
| Piperacillin | 4 | 22.2 |
| Cephalosporins | ||
| Cefepime | 3 | 16.7 |
| Cefotaxime | 3 | 16.7 |
| Ceftazidime | 3 | 16.7 |
| Ceftriaxone | 4 | 22.2 |
| Cefuroxime | 6 | 33.3 |
| Monobactams | ||
| Aztreonam | 3 | 16.7 |
| Fluoroquinolones | ||
| Ciprofloxacin | 4 | 22.2 |
| Levofloxacin | 4 | 22.2 |
| Moxifloksaxin | 4 | 22.2 |
| Ofloxacin | 4 | 22.2 |
| Aminoglicosides | ||
| Gentamycin | 1 | 5.5 |
| Netylmycin | 2 | 11 |
| Tobramycin | 3 | 16.7 |
| Miscellaneous agents | ||
| Trimethoprim-sulfamethoxazole | 5 | 27.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochońska, D.; Ścibik, Ł.; Brzychczy-Włoch, M. Biofilm Formation of Clinical Klebsiella pneumoniae Strains Isolated from Tracheostomy Tubes and Their Association with Antimicrobial Resistance, Virulence and Genetic Diversity. Pathogens 2021, 10, 1345. https://doi.org/10.3390/pathogens10101345
Ochońska D, Ścibik Ł, Brzychczy-Włoch M. Biofilm Formation of Clinical Klebsiella pneumoniae Strains Isolated from Tracheostomy Tubes and Their Association with Antimicrobial Resistance, Virulence and Genetic Diversity. Pathogens. 2021; 10(10):1345. https://doi.org/10.3390/pathogens10101345
Chicago/Turabian StyleOchońska, Dorota, Łukasz Ścibik, and Monika Brzychczy-Włoch. 2021. "Biofilm Formation of Clinical Klebsiella pneumoniae Strains Isolated from Tracheostomy Tubes and Their Association with Antimicrobial Resistance, Virulence and Genetic Diversity" Pathogens 10, no. 10: 1345. https://doi.org/10.3390/pathogens10101345