
I Can Do: Co-Designing a Service with and for People with Dementia to Engage with Volunteering

Abstract
:1. Introduction and Key Concepts
1.1. The Importance of Supporting People Diagnosed with Dementia in Accessing Social Activities
1.2. Co-Designing Services in the Dementia Care Context
1.3. Co-Designing for the IDoService
2. Methodology
2.1. The Workshop Design
2.2. Recruitment of Co-Design Participants and Workshop Settings
2.2.1. Stakeholder Recruitment and Online Setting
- Age UK Salford;
- Age UK Stockport;
- Age UK Trafford;
- Alzheimer’s Society;
- Caribbean African Health Network (CAHN);
- City of Trees;
- Dementia Carers;
- Dementia United;
- Global Brain Health Institute;
- GM Dementia Research Centre;
- Greater Sport (Active aging);
- Health Innovation Manchester;
- Health Watch Manchester;
- HMR Circle;
- Manchester Community Central;
- Manchester Metropolitan University;
- NHS Salford Clinical Commissioning Group;
- Reach Beyond & Open Doors Service, Salford;
- Social Sense;
- Springboard, Oldham;
- Together Dementia Support.
2.2.2. Recruitment of People with Dementia and Workshop Setting
2.3. Results Analysis, Consensus and Decisions Making
- Within the workshops, ideas were openly discussed and, at relevant moments, researchers aimed at leading the discussion towards census relating to the key points discussed, loosely following the idea of the Delphi model (Toepoel and Emerson 2017).
- A purposive review of the outcomes by the researchers after each workshop helped to synthesise key discussion points, ideas and points of consensus for use as source material and to build on in the following workshop(s). This is in line with the iterative nature of the design process. (Jonassen 2008; Sawyer 2021).
- In the final stage, researchers reviewed all the information and outcomes from the workshops in the context of relevant psychosocial and design theory to draw up the specification for the service as a precursor for the design realisation and evaluation in the third phase of the project.
3. Outcomes of the Workshops and Concept Development
3.1. Co-Design Workshop 1: Understanding Experiences, Expertise and Interests
- Sports and physical activities, such as walking, cycling, ball games, swimming, dancing, parachuting training and others.
- Arts and Crafts such as painting, illustration, making paper wreaths, mosaic laying, joinery and making a barrel organ.
- Other creative and leisure activities, such as reading, writing, storytelling, singing and playing music together, learning languages, cake making as well as playing various games.
- Leisure and travel activities, including days out, visiting museums or galleries, camping or holidays and weekends away.
- Socialising and friendships were important to people, such as regularly meeting friends at a pub, cooking and inviting family or friends at home, helping each other.
3.2. Co-Design Workshops 2, 3 and 4: Determining the Purpose of the IDoService in Relation to Existing Provisions
- Participating in ‘usual’ social and cultural activities;
- One-to-one support to help develop personal interests/activities;
- Opportunities and support for people to be able to volunteer.
- To share skills and talents;
- To benefit from one-to-one support for personal activities (e.g., traveling, practice a sport);
- To support each other in reciprocity;
- To do/find existing activities in Greater Manchester with their (care) partners.
- What volunteering opportunities are there in GM for people living with dementia?
- How is it possible to connect people with relevant opportunities?
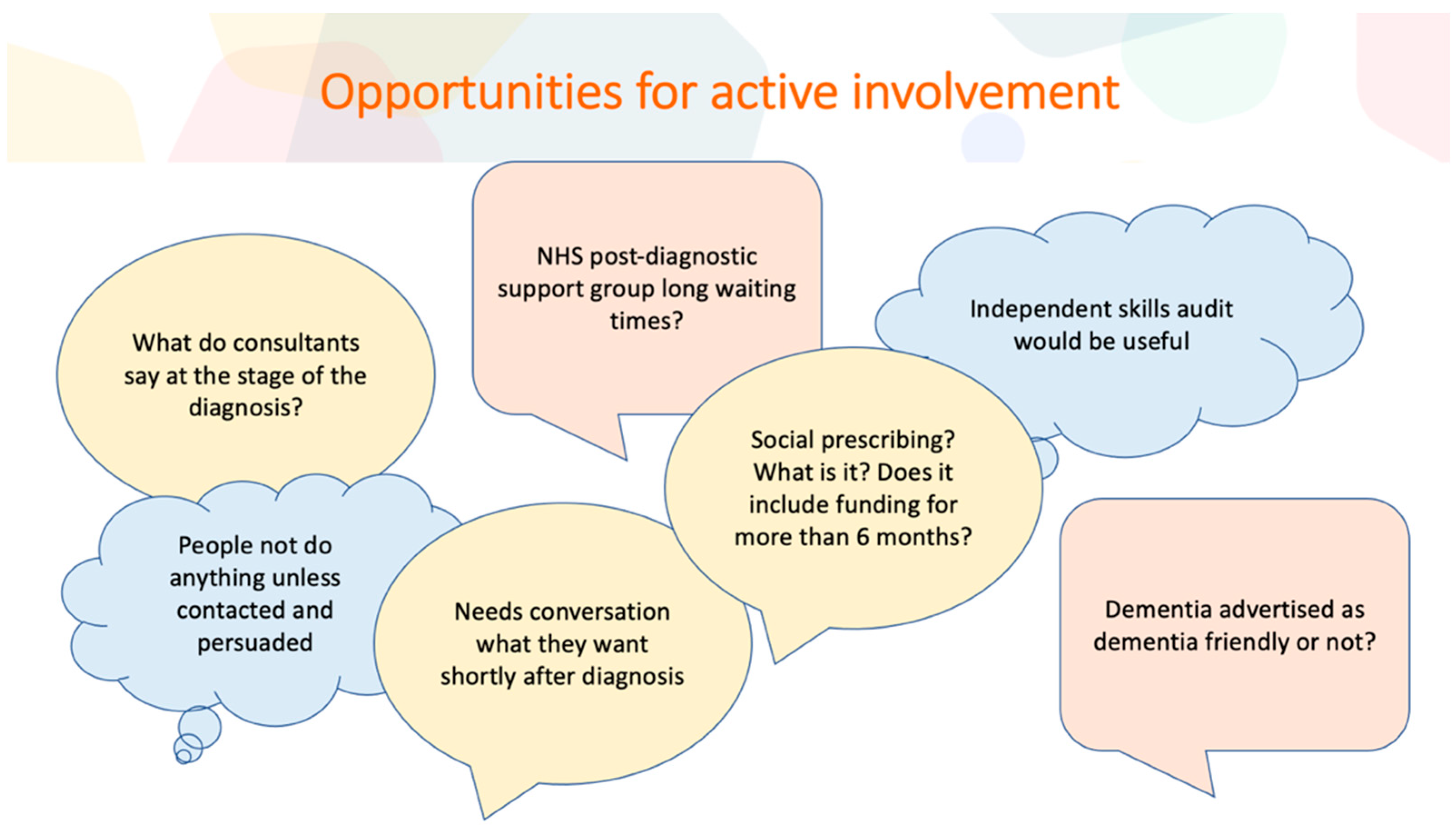
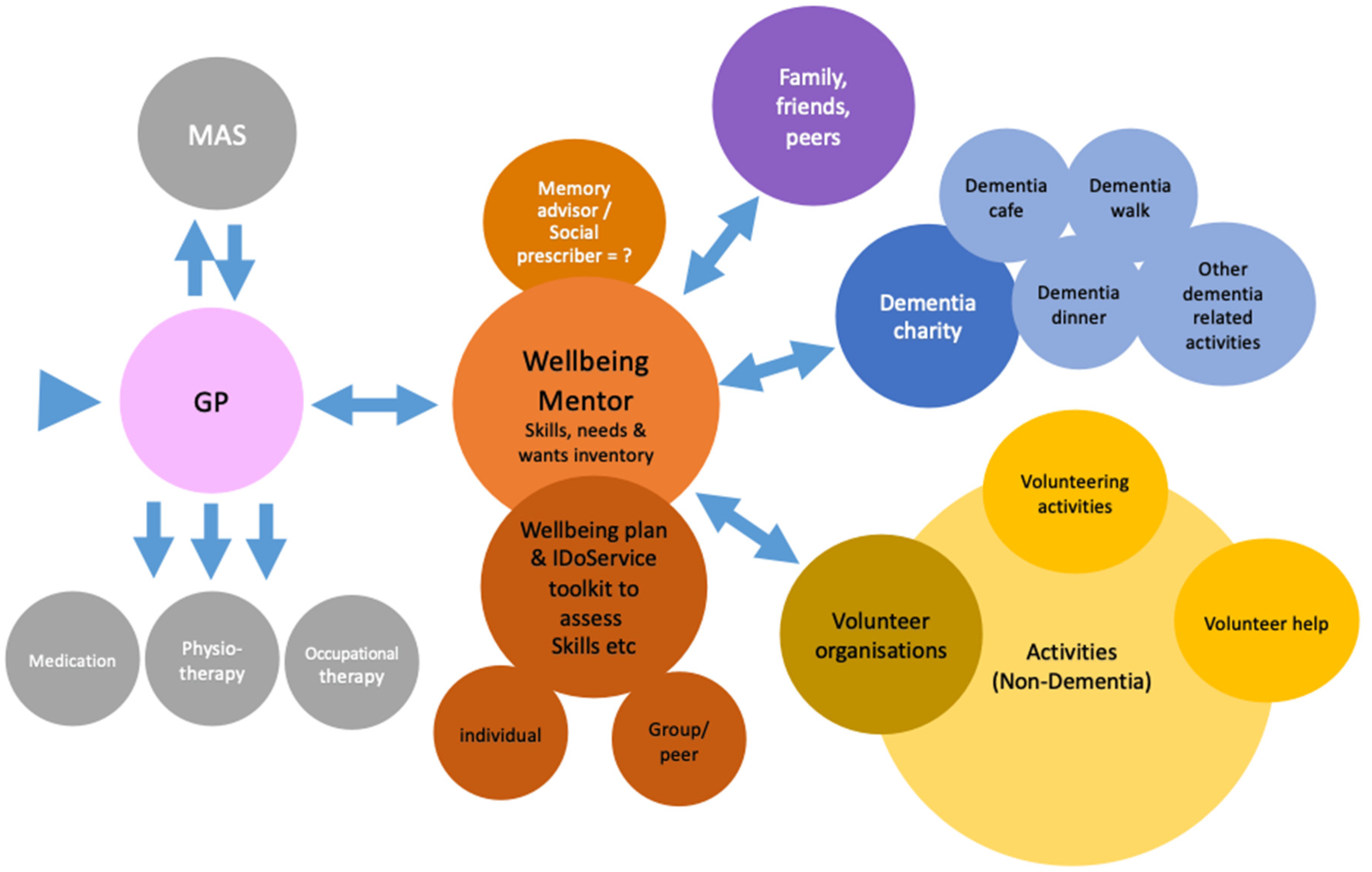
3.3. Co-Design Workshops 5, 6 and 7: Determining the Content and Delivery Format of the IDoService in Relation to Existing Services
- Where and at which point should it be delivered?
- Who could or should deliver it?
- What should the content of the service be and how should it be delivered?
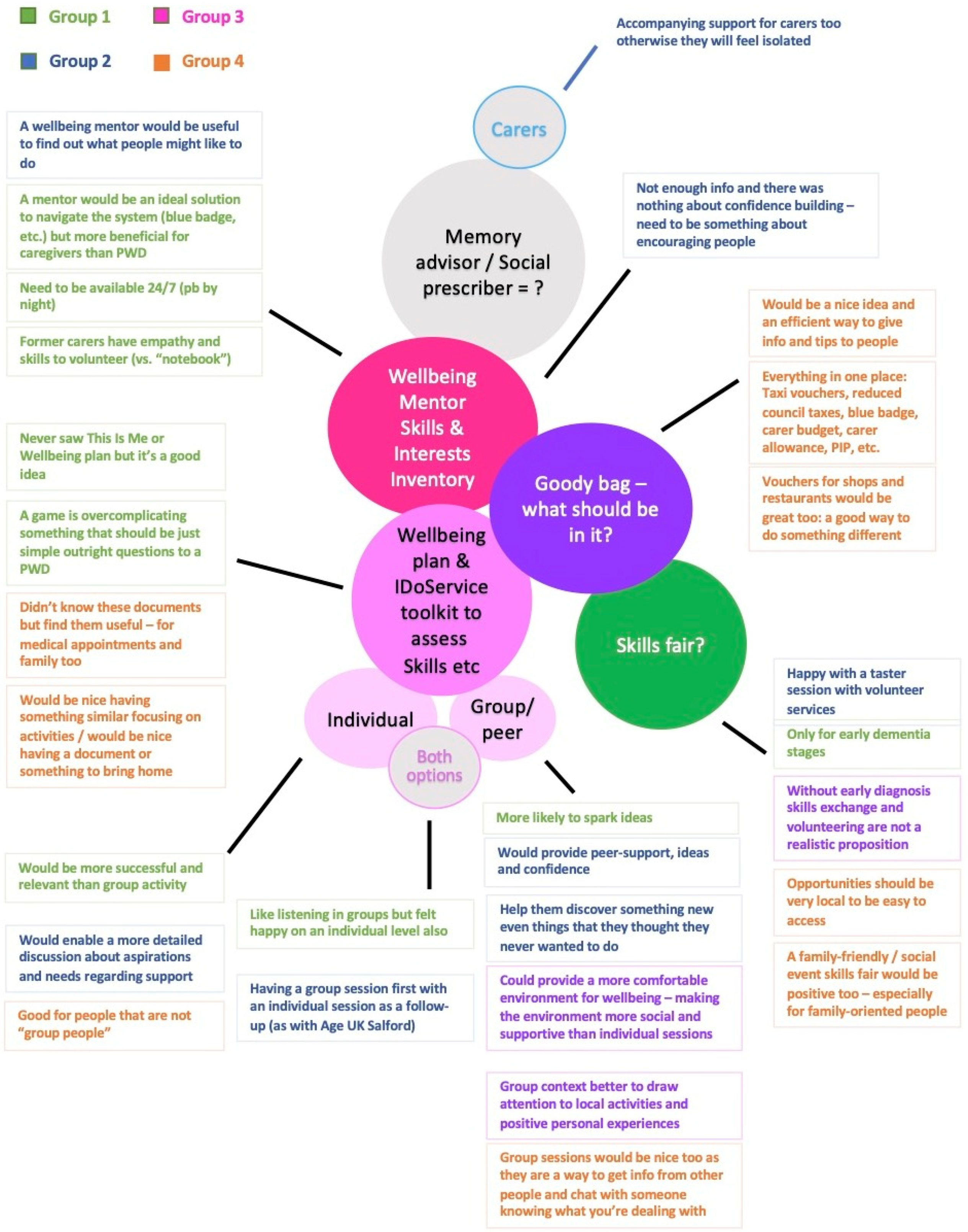
…obviously keep it simple when it comes to actually asking the questions, but I think it’s something that you’ll probably keep going back to. I’m just thinking. So, you’d have whether your wellbeing plan or some form of assessment and you’ll look at what people’s skills are and so on and then how they can develop those or volunteering and volunteer somewhere else. I think it is something that you’d keep going back to because people, as they get more confident, will want to do more so it’s going to change as time goes on so there will be a lot of dipping in and out. […] I think if we had a specific toolkit so that we could explore it further where we could work either as a one to one or whether it would work within a group setting, I think that would be something we would use and would be helpful.(W5, P8)
I like the idea […] of it being at the point of a wellbeing mentor being the person that shares your inventory […] because it’s not labelled as something for people living with dementia either because I was just thinking about your IDoService. I know obviously this project is specifically for people living with dementia but there could be people diagnosed with other health conditions that could equally benefit from the IDoService as well. If the implementation or sharing of what the inventory is and raising awareness sat with the wellbeing mentor, they could share it with more people, including people who have recently been diagnosed with dementia.(W6, P9)
P9: Although people most definitely need support when they’ve been through the memory assessment service and they get a diagnosis, they’re going to be probably reeling from the news that’s been delivered to them so to start saying straight away, for some people it might be important to hear, “Look, just because you’ve got this diagnosis, your life isn’t over. You can still have a good quality of life for many, many years.” I think it’s important to hear that message at the memory clinic and signpost people to the wellbeing mentor for when they’re ready.(W6, P9)
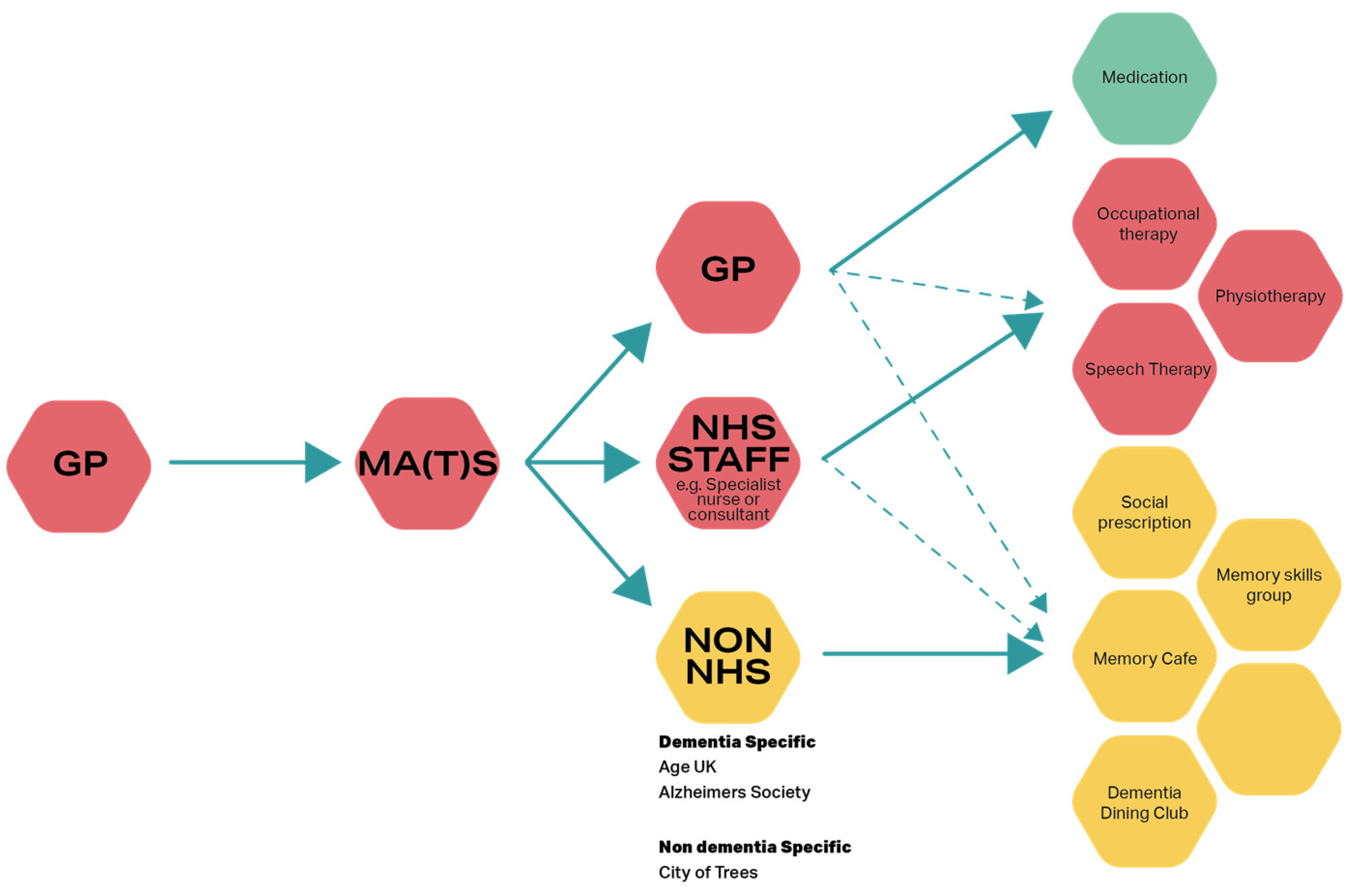
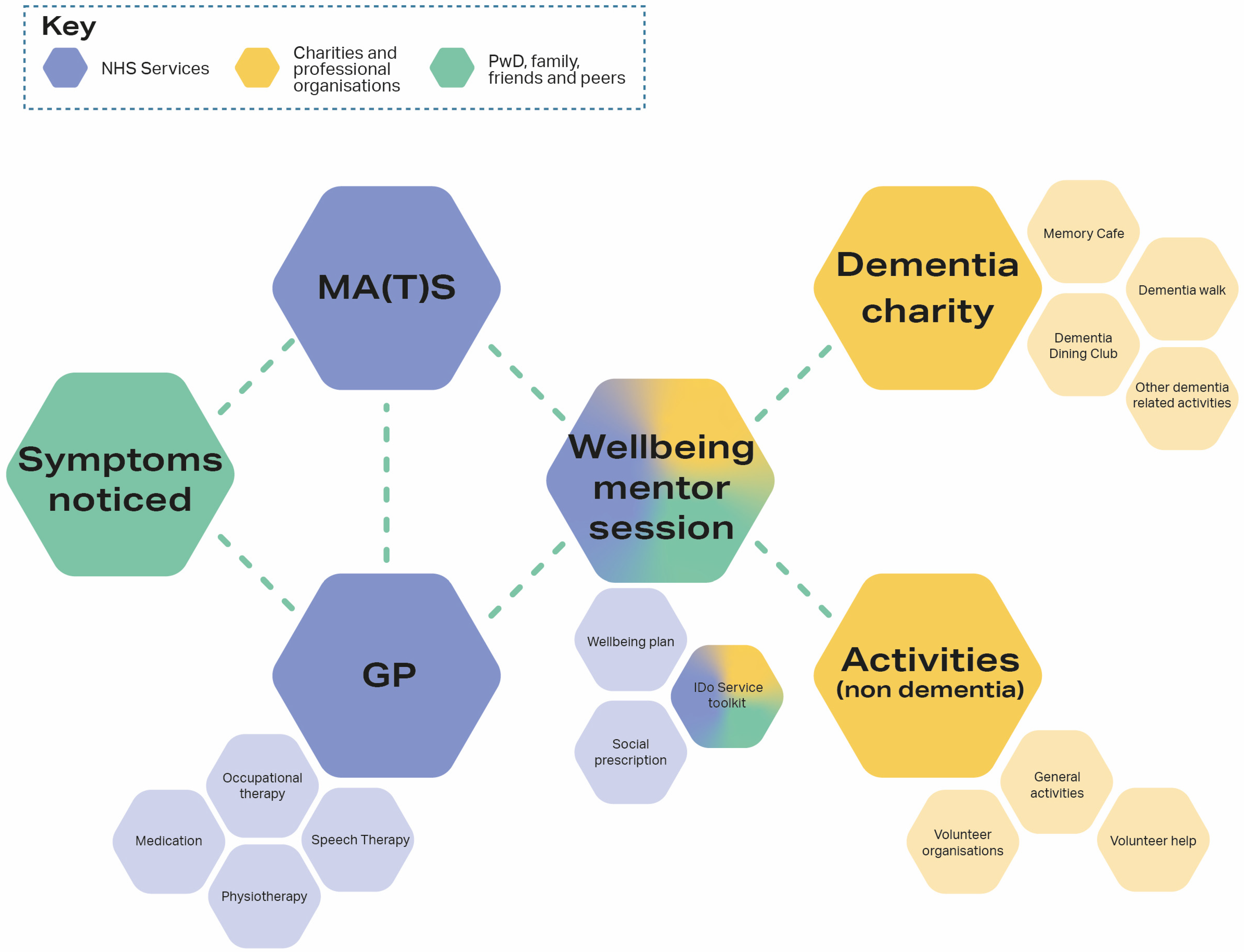
I2: So we could in fact move that arrow, couldn’t we, that blue arrow that goes from the GP to the wellbeing mentor potentially, from the MA(T)S to the wellbeing mentor or add an arrow anyway […] so it’s the next step, once they’ve had their assessment they would meet this wellbeing mentor.(W6, I2)
P9: Just another quick comment. Obviously, the service is called IDo and that’s how you’re funding for IDo but a very common phrase that we hear is ‘can do’, someone has got a ‘can do’ attitude. I really like the idea although obviously you’d have to ask people with dementia as well, if this pathway, this service was called Can Do, is getting the message over that you can still do things, your diagnosis doesn’t have to get in the way.(W6, P9)
4. Discussion: Final Design Concept and Reflection
4.1. I Can Do Pathway Specification
- Delivery through a baseline of three wellbeing mentor sessions, which can be repeated and revisited as required, including:
- ○
- a 1:1 session with the wellbeing mentor to explore strengths and interests in an intimate setting;
- ○
- a group session where between two and six people with dementia meet with local volunteer service representatives to find out what is on offer, and where people can discuss their interests within their peer support group. In this way, people can consider whether and what they might wish to do individually or together, since discussing and doing activities jointly can support confidence (Rodgers 2018);
- ○
- a 1:1 session with the wellbeing mentor to work out details for realising one or two of the interests identified.
- Provide detailed information about the service to function as a guide for care professionals acting as wellbeing mentors in delivering the service.
- Provide detailed information about the service for people with dementia as well as spaces for notes to function as a workbook.
- Be designed engaging in terms of language, readability, the inclusion of images and other relevant materials to be appropriate and tailored to the cognitive and emotional needs of people with dementia (e.g., DEEP 2022).
- Include a contents list for easy access and overview.
- Provide information on the content of each of the three sessions.
- Structure sessions inclusively and interactively to allow for co-production and provide participants with a sense of ownership and empowerment (Dening et al. 2020).
- Include relaxation and/or ice breaker exercises at the beginning of each session to enable people to mentally arrive and get comfortable (Niedderer et al. 2020).
- Include physical prompts as memory aids and inspiration and storytelling to allow for personal exploration (Ahmed 2015; Niedderer et al. 2020).
- Include spaces for notes to record e.g., interests, or choices agreed in the sessions.
- Include spaces for reflection on the sessions and feelings about them (Niedderer et al. 2020).
4.2. Reflections on the Co-Design Process and Its Transformative Impact
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
| 1 | Also at times called MATS: Memory Assessment and Treatment Services. |
References
- Ahmed, Anya. 2015. Retiring to Spain: Women’s Narratives of Nostalgia, Belonging and Community. Bristol: Policy Press. [Google Scholar] [CrossRef]
- Arblaster, Kielan, and Sharon Brennan. 2022. Left to Cope Alone: The Unmet Support Needs after a Dementia Diagnosis. London: Alzheimer’s Society, p. 29. Available online: https://www.alzheimers.org.uk/sites/default/files/2022-07/left-to-cope-alone-after-diagnosis-report.pdf (accessed on 2 March 2023).
- Clarkson, Paul, Jane Hughes, Chengqiu Xie, Matthew Larbey, Brenda Roe, Clarissa M. Giebel, David Jolley, David Challis, and HoSt-D (Home Support in Dementia) Programme Management Group. 2017. Overview of systematic reviews: Effective home support in dementia care, components and impacts—Stage 1, psychosocial interventions for dementia. Journal of Advanced Nursing 73: 2845–63. [Google Scholar] [CrossRef] [PubMed]
- DEEP. 2022. Making Things More Accessible. Available online: https://www.dementiavoices.org.uk/deep-resources/making-things-more-accessible/ (accessed on 7 January 2021).
- Dening, Tom, and Malarvizhi Babu Sandilyan. 2014. Dementia: Definitions and types. Nursing Standard 29: 37–42. [Google Scholar] [CrossRef] [PubMed]
- Dening, Tom, Julie Gosling, Michael Craven, and Kristina Niedderer. 2020. Guidelines for Designing with and for People with Dementia. Nottingham: MinD. [Google Scholar] [CrossRef]
- Fernández-Mayoralas, Gloria, Fermina Rojo-Pérez, Pablo Martínez-Martín, Maria-Eugenia Prieto-Flores, Carmen Rodríguez-Blázquez, Salomé Martín-García, José-Manuel Rojo-Abuín, and Maria-Joao Forjaz. 2015. Active ageing and quality of life: Factors associated with participation in leisure activities among institutionalized older adults, with and without dementia. Aging & Mental Health 19: 1031–41. [Google Scholar] [CrossRef] [Green Version]
- Garde, Julia Anne, Mascha Cécile Van Der Voort, and Kristina Niedderer. 2018. Design Probes for People with Dementia. Paper presented at Design as a Catalyst for Change—DRS International Conference 2018, DRS International Conference 2018, Limerick, Ireland, June 25–28; Edited by Cristiano Storni, Keelin Leahy, Muireann McMahon, Peter Lloyd and Erik Bohemia. London: Design Research Society. [Google Scholar]
- Greenhalgh, Trisha. 2009. Patient and public involvement in chronic illness: Beyond the expert patient. BMJ 338: b49. [Google Scholar] [CrossRef] [Green Version]
- Jonassen, David H. 2008. Instructional Design as Design Problem Solving: An Iterative Process. Educational Technology 48: 21–26. Available online: https://www.jstor.org/stable/44429574 (accessed on 7 January 2021).
- Kort, Helianthe S. M., Bas Steunenberg, and Joost Van Hoof. 2019. Methods for Involving People Living with Dementia and Their Informal Carers as Co-Developers of Technological Solutions. Dementia and Geriatric Cognitive Disorders 47: 149–56. [Google Scholar] [CrossRef] [Green Version]
- Low, Lee-Fay, Kate Swaffer, Margaret McGrath, and Henry Brodaty. 2018. Do people with early-stage dementia experience Prescribed Disengagement? A systematic review of qualitative studies. International Psychogeriatrics 30: 807–31. [Google Scholar] [CrossRef]
- Malmberg, Lisa, Vanessa Rodrigues, Linda Lännerström, Katarina Wetter-Edman, Josina Vink, and Stefan Holmlid. 2019. Service Design as a Transformational Driver Toward Person-Centered Care in Healthcare. In Service Design and Service Thinking in Healthcare and Hospital Management: Theory, Concepts, Practice. Edited by Mario A. Pfannstiel and Christoph Rasche. Berlin and Heidelberg: Springer International Publishing, pp. 1–18. [Google Scholar] [CrossRef]
- Marquez, Joe J., and Annie Downey. 2015. Service Design: An Introduction to a Holistic Assessment Methodology of Library Services. Weave: Journal of Library User Experience 1: 201. [Google Scholar] [CrossRef]
- McDougall, Sean. 2012. Co-Production, Co-Design and Co-Creation: What Is the Difference? Available online: https://www.stakeholderdesign.com/co-production-versus-co-design-what-is-the-difference/ (accessed on 10 September 2019).
- Neuhoff, Rike, Nanna Dam Johansen, and Luca Simeone. 2022. Story-centered co-creative methods: A means for relational service design and healthcare innovation. In Service Design Practices for Healthcare Innovation: Paradigms, Principles, Prospects. Edited by Mario A. Pfannstiel, Naaliia Brehmer and Christoph Rasche. Berlin and Heidelberg: Springer, pp. 1–18. [Google Scholar] [CrossRef]
- Niedderer, Kristina, Dew Harrison, Julie Gosling, Michael P. Craven, Alethea Blackler, Raquel Losada Durán, and Teresa Cid. 2020. Working with experts with experience: Charting co-production and codesign in the development of HCI-based design. In HCI and Design in the Context of Dementia. Edited by Rens Brankaert and Gail Kenning. Cham: Springer, pp. 303–20. [Google Scholar] [CrossRef]
- Niedderer, Kristina, Laura Orton, and Isabelle Tournier. 2022a. An overview of current practices and approaches to co-designing services with and for people with dementia towards developing a framework for best practice. In DRS2022: Bilbao, Bilbao, Spain. Edited by Dan Lockton, Sara Lenzi, Paul Hekkert, Arlene Oak, Juan Sádaba and Peter Lloyd. Bilbao: DRS. [Google Scholar] [CrossRef]
- Niedderer, Kristina, Vjera Holthoff-Detto, Thomas J. L. van Rompay, Aarmağan Karahanoğlu, Geke D. S. Ludden, Rosa Almeida, Raquel Losada Durán, Yolanda Bueno Aguado, Jennifer N. W. Lim, Tina Smith, and et al. 2022b. This is Me: Evaluation of a board game to promote social engagement, wellbeing and agency in people with dementia through mindful life-storytelling. Journal of Aging Studies 60: 100995. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics. 2021. Estimates of the Population for the UK, England and Wales, Scotland and Northern Ireland. June 25. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland (accessed on 15 August 2022).
- Orton, Laura, Isabelle Tournier, Steve Threlfall, and Kristina Niedderer. 2023. Ido Service Project-Work Package Two Data. [Dataset]. Manchester: E-space–Manchester Metropolitan University’s Research Repository. [Google Scholar] [CrossRef]
- Pratt, Rebekah, and Heather Wilkinson. 2001. The Effect of Being Told the Diagnosis of Dementia from the Perspectives of the Person with Dementia. Final Report to the Mental Health Foundation. Stirling: CSRD. [Google Scholar]
- Roberts, Chris. 2019. Living with Dementia (Keynote). Paper presented at MinD International Conference, Dresden, Germany, September 19–20; Available online: https://designingfordementia.eu/news/mind-events/mind-conference-2019/mind-2019-keynote-presentations/chris-roberts-living-with-dementia (accessed on 17 March 2021).
- Rodgers, Paul A. 2018. Co-designing with people living with dementia. CoDesign 14: 188–202. [Google Scholar] [CrossRef] [Green Version]
- Sanders, Elizabeth B.-N., and Pieter Jan Stappers. 2008. Co-creation and the new landscapes of design. Co-Design 4: 5–18. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, R. Keith. 2021. The iterative and improvisational nature of the creative process. Journal of Creativity 31: 100002. [Google Scholar] [CrossRef]
- Steen, Marc, Menno Manschot, and Nicole De Koning. 2011. Benefits of co-design in service design projects. International Journal of Design 5: 53–60. Available online: http://www.ijdesign.org/index.php/IJDesign/article/view/890/346 (accessed on 2 March 2023).
- Stickdorn, Marc, and Jakob Schneider. 2011. This Is Service Design Thinking: Basics, Tools, Cases. Hoboken: Wiley. [Google Scholar]
- Toepoel, Vera, and Hannah Emerson. 2017. Using experts’ consensus (the Delphi method) to evaluate weighting techniques in web surveys not based on probability schemes. Mathematical Population Studies 24: 161–71. [Google Scholar] [CrossRef] [Green Version]
- Tournier, Isbelle, Laura Orton, Tom Dening, Anya Ahmed, Vjera Holthoff-Detto, and Kristina Niedderer. 2023. An investigation of the wishes, needs, opportunities and challenges of accessing meaningful activities for people living with mild to moderate dementia. International Journal of Environmental Research and Public Health 20: 5358. [Google Scholar] [CrossRef]
- Wang, Gubing, Chiara Marradi, Armagan Albayrak, and Tischa J. M. van der Cammen. 2019. Co-designing with people with dementia: A scoping review of involving people with dementia in design research. Maturitas 127: 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. 2021. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 7 January 2021).
- Wilson, Samantha A., Paula Byrne, and Sarah E. Rodgers. 2023. ‘I’d be lost without my smartphone’: A qualitative analysis of the use of smartphones and tablets by people living with dementia, mild cognitive impairment, and their caregivers. Aging & Mental Health, 1–9. [Google Scholar] [CrossRef]
- Zanasi, Michele, Berit Ziebuhr, Yolanda Bueno Aguado, Raquel Losada Durán, Tom Dening, Isabelle Tournier, Kristina Niedderer, Ana Diaz, Diana Druschke, Rosa Almeida, and et al. 2023. Feelings of usefulness and empowerment in people with dementia: A qualitative study. International Journal of Environmental Research and Public Health 20: 6080. [Google Scholar] [CrossRef]
- Zeilig, Hannah, Victoria Tischler, Millie van der Byl Williams, Julian West, and Sarah Strohmaier. 2019. Co-creativity, well-being and agency: A case study analysis of a co-creative arts group for people with dementia. Journal of Aging Studies 49: 16–24. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Workshop No., Date & Mode | Content | Participants | Methods |
|---|---|---|---|
| Workshop 1 November 2021 Face-to-face | Explore meaningful/leisure activities and skills people like to do, like help with, or like to offer to others | People with dementia and care/partners 17 participants (6 people with dementia, 6 carers, 5 former carers) | Prompts (Garde et al. 2018): We asked people to bring objects that represented their favourite activities and/or skills. Storytelling (Ahmed 2015): We asked people to tell stories about their activities and skills important to them, using the objects they brought. |
| Workshops 2, 3 & 4 December 2021 Online via MS Teams | Explore services and opportunities based on identified skills and interests | Service providers 3, 6 and 5 participants, respectively | Online focus groups (Kort et al. 2019): For the workshops with service providers, we used a more traditional online focus group format, where we combined questions with storytelling to elicit relevant information about services and examples of their application. |
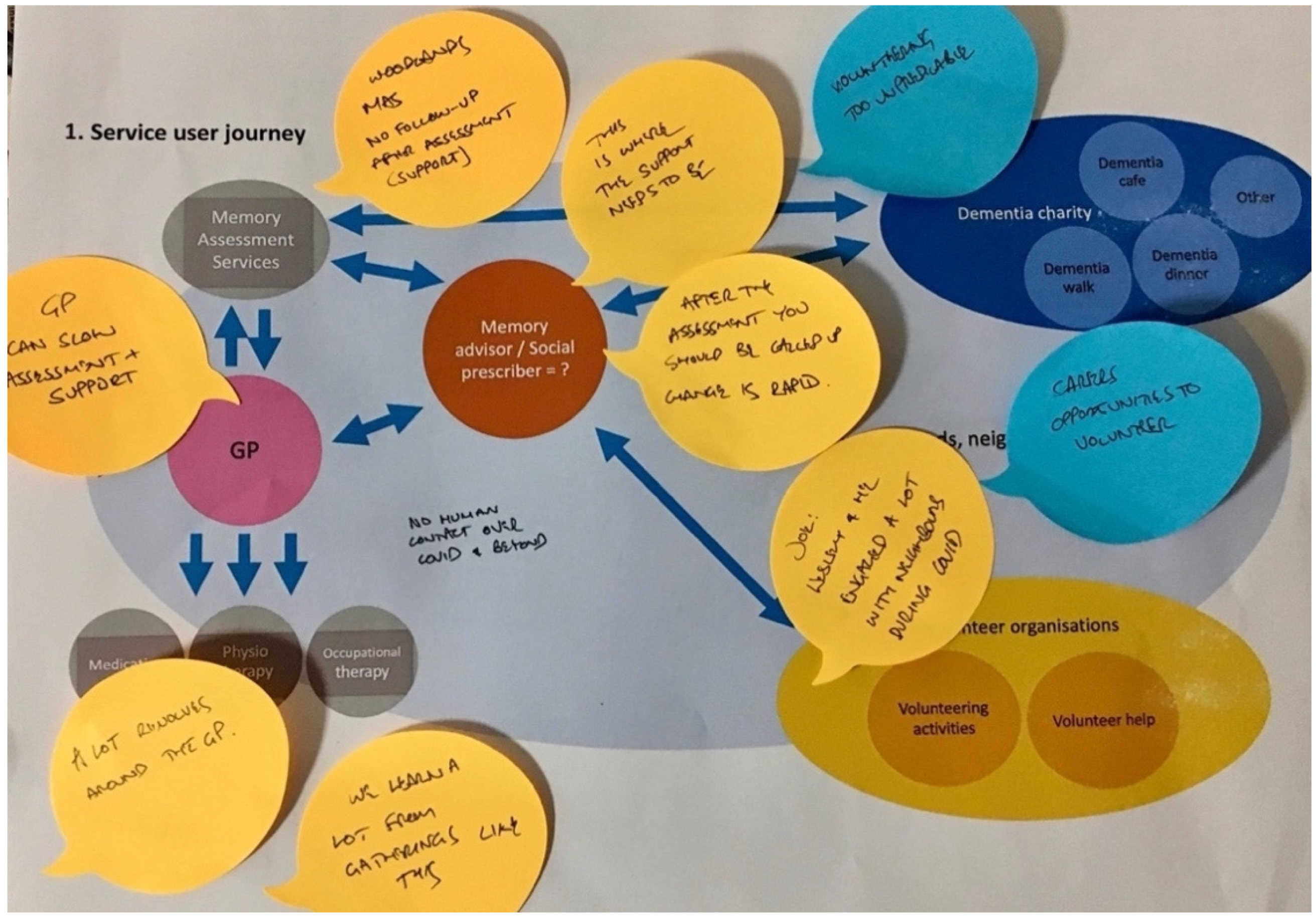
| Workshops 5 & 6 March 2022 Online via MS Teams | Explore and work out how the service could or should work | Service providers 7 and 5 participants, respectively | Service-pathway mapping using visual prompts and storytelling. All sessions followed the same pattern and were used to explore the proposed service pathway intervention—what to offer, how it might work, how to deliver it. A visual map with movable items was used to work imaginatively through what might be involved, and to solicit input and feedback on how a person might need to be supported to enable participation as a volunteer or participant. |
| Workshop 7 March 2022 Face-to-face | Explore and work out how the service could or should work | People with dementia and care/partners 21 participants (8 people with dementia, 8 carers, 5 former carers) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niedderer, K.; Tournier, I.; Orton, L.; Threlfall, S. I Can Do: Co-Designing a Service with and for People with Dementia to Engage with Volunteering. Soc. Sci. 2023, 12, 364. https://doi.org/10.3390/socsci12060364
Niedderer K, Tournier I, Orton L, Threlfall S. I Can Do: Co-Designing a Service with and for People with Dementia to Engage with Volunteering. Social Sciences. 2023; 12(6):364. https://doi.org/10.3390/socsci12060364
Chicago/Turabian StyleNiedderer, Kristina, Isabelle Tournier, Laura Orton, and Steve Threlfall. 2023. "I Can Do: Co-Designing a Service with and for People with Dementia to Engage with Volunteering" Social Sciences 12, no. 6: 364. https://doi.org/10.3390/socsci12060364