
Barriers and Enablers to Health-Seeking for People Affected by Severe Stigmatising Skin Diseases (SSSDs): A Scoping Review

Abstract
:1. Introduction
2. Rationale for the Study
3. Materials and Methods
3.1. Stage 1: Identifying the Research Question
3.2. Stage 2: Identifying Relevant Studies
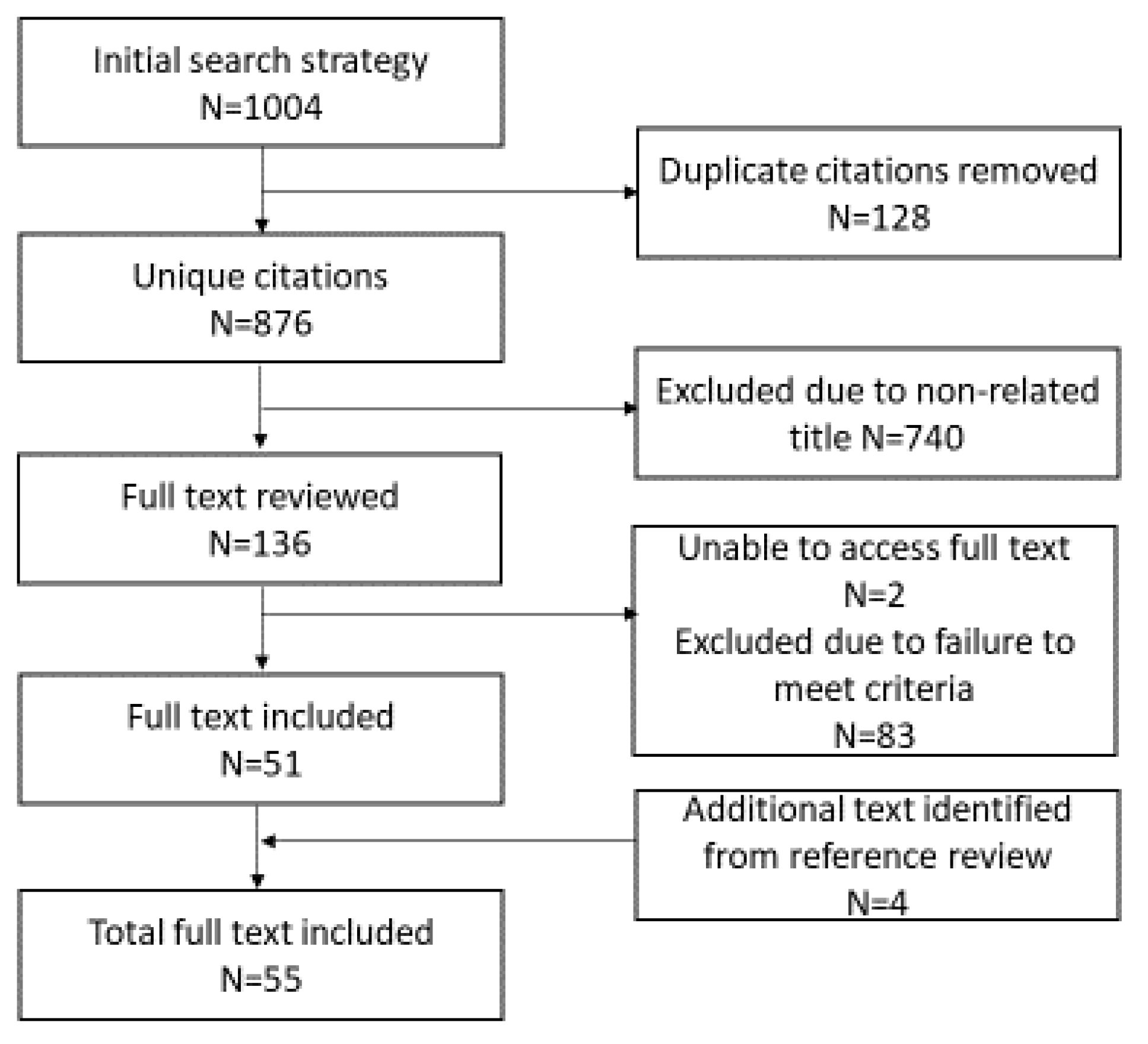
3.3. Stage 3: Study Selection
- Any qualitative, quantitative or mixed methods study or review study. No restrictions were placed on study design.
- Study that includes data about barriers/enablers to accessing care for a SSSD. SSSDs included in this study are leprosy, onchocerciasis, Buruli ulcer, yaws, and clinical presentation of lymphatic filariasis, specifically lymphoedema and hydrocele.
- Studies conducted in Lower Middle-Income Countries (LMIC).
- Study written in English language.
- Studies published between 2010 and 2020.
3.4. Stage 4: Charting the Data
3.5. Stage 5: Collating, Summarising and Reporting the Results
4. Results
4.1. Study Characteristics
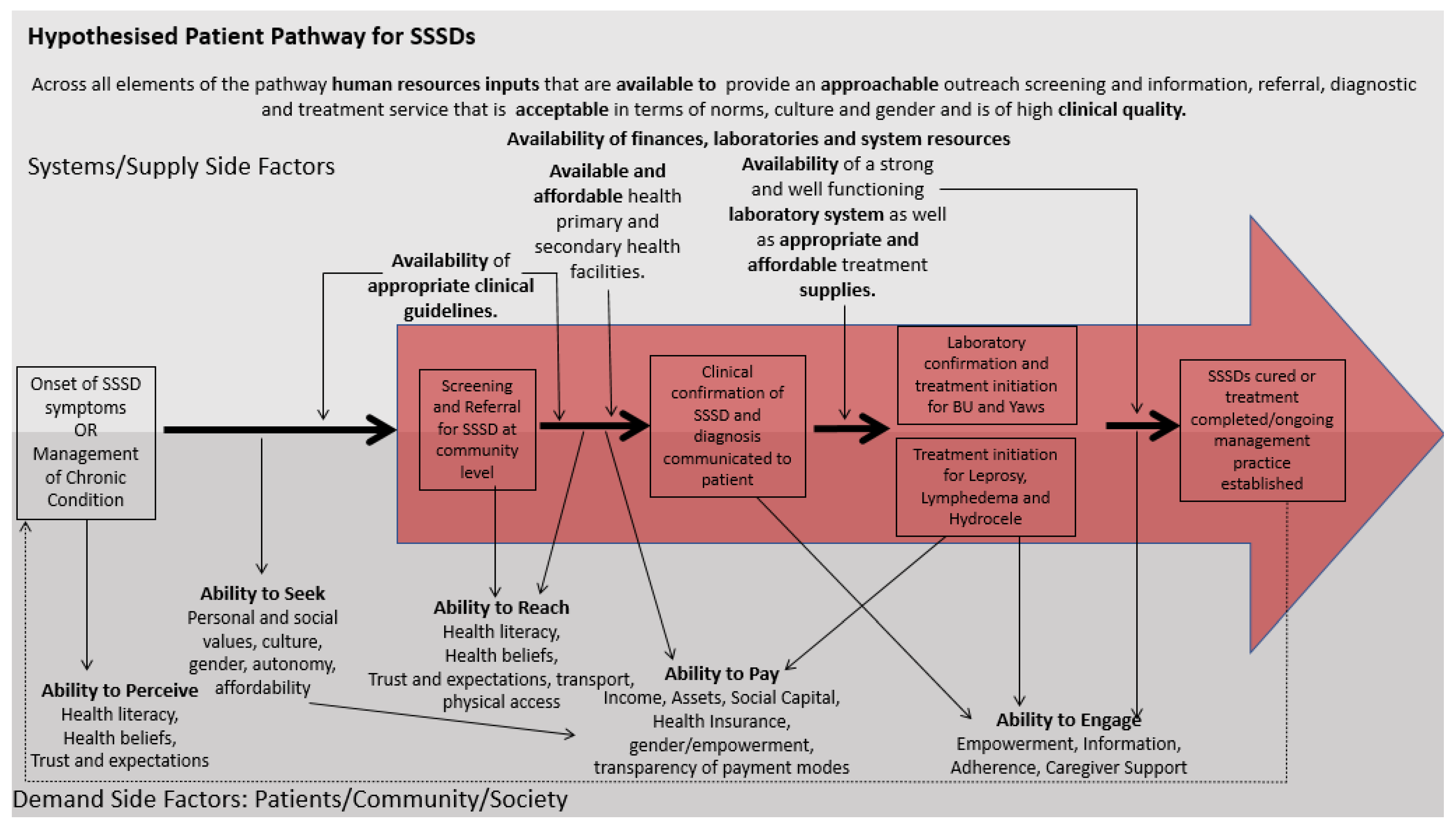
4.2. Demand-Side Factors
4.2.1. Ability to Perceive
4.2.2. Health Beliefs and Their Role in Health-Seeking
4.2.3. Ability to Seek
4.2.4. Ability to Reach
4.2.5. Ability to Pay
4.2.6. Ability to Engage
4.3. Supply-Side Factors
4.3.1. Approachability
4.3.2. Acceptability
4.3.3. Availability and Accommodation
4.3.4. Affordability
4.3.5. Appropriateness
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Topic Specific Key Word | Mesh Term | Free Text Term | |
| OR | Access | Health services accessibility | Health N3 Access |
| OR | Availability | Health N3 Availability | |
| OR | Help | Helping behaviour Help-seeking behaviour Help behaviour | Help* |
| OR | Utilisation | Patient acceptance of health care | Health N3 Utili* Health N3 use |
| OR | Behaviour | health N3 Behaviour health N3 behavior | |
| OR | Seek | Health N3 Seek* Health N3 accept* | |
| OR | Practice | Health knowledge, attitudes, practice | Health N3 practice |
| OR | Perception | Health N3 perception | |
| OR | Attitude | Attitude to health | Health N3 attitude |
| OR | Belief | “health belief*” | |
| OR | Enabler | Enabler or motivator or facilitator | |
| OR | Barrier | Barrier | |
| OR | Demand | Health service needs and demands | Health N3 need Health N3 demand |
| Topic Specific Key Word | Mesh Term | Free Text Term | |
| OR | skin disease | Skin diseases, infectious Skin diseases, parasitic | |
| OR | Neglected Tropical Diseases | Neglected diseases | |
| OR | Leprosy | Leprosy Mycobacterium leprae | Leprosy “Hansen’s disease” “Mycobacterium Leprae” |
| OR | Buruli ulcer | Buruli ulcer | “buruli ulcer” “mycobacterium ulcerans” “skin ulcer” |
| OR | Yaws | Yaws | Yaws Frambesia |
| OR | Lymphoedema | Lymphedema | Lymphedema lymphoedema “Milroy’s disease” |
| OR | Lymphedema | Lymphoedema | Lymphedema lymphoedema “Milroy’s disease” |
| OR | Lymphatic filariasis | Elephantiasis, Filarial | “filarial elephantiasis” “lymphatic filariasis” |
| OR | Hydrocele | Testicular hydrocele | Hydrocele |
| Context Specific Key Word | Mesh Term | Free text terms | |
| OR | Sub Saharan Africa | Africa south of the sahara | “sub-saharan Africa” |
| OR | Africa | Africa | |
| OR | Low-and Middle- Income Countries | LMIC “low and middle income” “low resource” | |
| OR | Liberia | Liberia | Liberia |
| OR | Developing countries | Developing countries | “developing countr*” |
References
- Abdulmalik, Jibril, Emeka Nwefoh, James Obindo, Samuel Dakwak, Motunrayo Ayobola, John Umaru, Elisha Samuel, Christopher Ogoshi, and Julian Eaton. 2018. Emotional Difficulties and Experiences of Stigma among Persons with Lymphatic Filariasis in Plateau State, Nigeria. Health and Human Rights 20: 27–40. [Google Scholar] [PubMed]
- Abedi, Heidarali, Akbar Javadi, and Sayedali Naji. 2013. An exploration of health, family and economic experiences of leprosy patients, Iran. Pakistan Journal of Biological Sciences 16: 927–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackumey, Mercy M., Margaret Gyapong, Matilda Pappoe, and Mitchell G. Weiss. 2011. Help-Seeking for Pre-Ulcer and Ulcer Conditions of Mycobacterium Ulcerans Disease (Buruli Ulcer) in Ghana. American Journal of Tropical Medicine and Hygiene 85: 1106–13. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, Ram Kumar, Jeevan Bahadur Sherchand, Shiva Raj Mishra, Kamal Ranabhat, Amrit Pokharel, Pramila Devkota, Durga Mishra, Yadu Chandra Ghimire, Khageshwor Gelal, Rajan Paudel, and et al. 2015. Health-Seeking Behaviors and Self-Care Practices of People with Filarial Lymphoedema in Nepal: A Qualitative Study. Journal of Tropical Medicine 2015: 260359. [Google Scholar] [CrossRef] [Green Version]
- Alferink, Marike, Tjip S. van der Werf, Ghislain E. Sopoh, Didier C. Agossadou, Yves T. Barogui, Frederic Assouto, Chantal Agossadou, Roy E. Stewart, Ymkje Stienstra, and Adelita V. Ranchor. 2013. Perceptions on the Effectiveness of Treatment and the Timeline of Buruli Ulcer Influence Pre-Hospital Delay Reported by Healthy Individuals. PLoS Neglected Tropical Diseases 7: e2014. [Google Scholar] [CrossRef] [Green Version]
- Ali, Oumer, Asrat Mengiste, Maya Semrau, Abraham Tesfaye, Abebaw Fekadu, and Gail Davey. 2021. The Impact of Podoconiosis, Lymphatic Filariasis, and Leprosy on Disability and Mental Well-Being: A Systematic Review. PLoS Neglected Tropical Diseases 15: e0009492. [Google Scholar] [CrossRef]
- Arksey, Hilary, and Lisa O’Malley. 2005. Scoping Studies: Towards a Methodological Framework. International Journal of Social Research Methodology: Theory and Practice 8: 19–32. [Google Scholar] [CrossRef] [Green Version]
- Atre, Sachin Ramchandra, Sheela Girish Rangan, Vanaja Prabhakar Shetty, Nilesh Gaikwad, and Nerges Furdoon Mistry. 2011. Perceptions, Health Seeking Behaviour and Access to Diagnosis and Treatment Initiation among Previously Undetected Leprosy Cases in Rural Maharashtra, India. Leprosy Review 82: 222–34. [Google Scholar] [CrossRef]
- Da Silva, Maria Cristina Dias, and Elisabete Pimenta Araújo Paz. 2019. Experiences of People Affected by Leprosy in the Health Services: A Hermeneutic Approach. Leprosy Review 90: 172–82. [Google Scholar] [CrossRef]
- De Kruijff, Arie. 2015. Mozambique Country Profile. Leprosy Review 86: 89–95. [Google Scholar] [CrossRef] [PubMed]
- Dean, Laura, Rachel Tolhurst, Gartee Nallo, Karsor Kollie, Anthony Bettee, and Sally Theobald. 2019. Neglected Tropical Disease as a ‘Biographical Disruption’: Listening to the Narratives of Affected Persons to Develop Integrated People Centred Care in Liberia. PLoS Neglected Tropical Diseases 13: e0007710. [Google Scholar] [CrossRef] [Green Version]
- Dupnik, Kathryn Margaret, Fernando José Ramos Cardoso, Ana Luiza Braga Brito De Macêdo, Igor Leonardo Cardoso De Sousa, Renata Cristina Barros Leite, Selma Maria Bezerra Jerônimo, and Mauricio Lisboa Nobre. 2013. Intolerance to Leprosy Multi-Drug Therapy: More Common in Women? Leprosy Review 84: 209–18. [Google Scholar] [CrossRef] [PubMed]
- Garchitorena, Andrés, Calistus N. Ngonghala, Jean-Francois Guegan, Gaëtan Texier, Martine Bellanger, Matthew Bonds, and Benjamin Roche. 2015. Economic inequality caused by feedbacks between poverty and the dynamics of a rare tropical disease: The case of buruli ulcer in sub-Saharan Africa. Proceedings of the Royal Society B: Biological Sciences 282: 20151426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautham, Melur Sukumar, Munivenkatappa Dayananda, Dhruvarao Gopinath, Nallur Somanna Shivraj, Basha Riyaz, and Sreekantaiah Pruthvish. 2011. Community-Based Needs Assessment of Leprosy Patients in Chamrajanagar District, Karnataka, India. Leprosy Review 82: 286–95. [Google Scholar] [CrossRef] [PubMed]
- Girma, Lisanawork, Kidist Bobosha, Tsegaye Hailu, and Edessa Negera. 2018. Knowledge and self-care practice of leprosy patients at ALERT Hospital, Ethiopia. bioRxiv, 78–87. [Google Scholar] [CrossRef]
- Gómez, Libardo, Alberto Rivera, Yesenia Vidal, Jorge Bilbao, Christa Kasang, Sandra Parisi, Eva Maria Schwienhorst-Stich, and Karl Philipp Puchner. 2018. Factors Associated with the Delay of Diagnosis of Leprosy in North-Eastern Colombia: A Quantitative Analysis. Tropical Medicine and International Health 23: 193–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, Pankaj. 2015. Use of Audio-Visual Aids in Teaching Post Operative Exercises to Person Affected by Leprosy. Leprosy Review 86: 251–53. [Google Scholar] [CrossRef] [PubMed]
- Hameed, Shaffa, Alexander Maddams, Hattie Lowe, Lowri Davies, Rajat Khosla, and Tom Shakespeare. 2020. From Words to Actions: Systematic Review of Interventions to Promote Sexual and Reproductive Health of Persons with Disabilities in Low- And Middle-Income Countries. BMJ Global Health 5: e002903. [Google Scholar] [CrossRef] [PubMed]
- Henry, Mary, Noêmi GalAn, Katherine Teasdale, Renata Prado, Harpreet Amar, Marina S. Rays, Lesley Roberts, Pedro Siqueira, Gilles de Wildt, Marcos Virmond, and et al. 2016. Factors Contributing to the Delay in Diagnosis and Continued Transmission of Leprosy in Brazil—An Explorative, Quantitative, Questionnaire Based Study. PLoS Neglected Tropical Diseases 10: e0004542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heukelbach, Jorg, Olga André Chichava, Alexcian Rodrigues de Oliveira, Kathrin Häfner, Friederike Walther, Carlos Henrique Morais de Alencar, Alberto Novaes Ramos, Adriana Cavalcante Ferreira, and Liana Ariza. 2011. Interruption and Defaulting of Multidrug Therapy against Leprosy: Population-Based Study in Brazil’s Savannah Region. PLoS Neglected Tropical Diseases 5: e1031. [Google Scholar] [CrossRef] [Green Version]
- Ibe, Ogochukwu, Obinna Onwujekwe, Benjamin Uzochukwu, Miriam Ajuba, and Paul Okonkwo. 2015. Exploring Consumer Perceptions and Economic Burden of Onchocerciasis on Households in Enugu State, South-East Nigeria. PLoS Neglected Tropical Diseases 9: e0004231. [Google Scholar] [CrossRef] [Green Version]
- John, Annamma Succhanda, Pamidipani Samuel Sundar Rao, and Sonali Das. 2010. Assessment of Needs and Quality Care Issues of Women with Leprosy. Leprosy Review 81: 34–40. [Google Scholar] [CrossRef]
- Kasang, Christa, Sri Nandini Krishnan, Noah Menkor, and Karl Puchner. 2019. Impact of General Health Volunteers on Leprosy Control in Nimba County, Liberia: An Experience from the Ganta Leprosy Rehabilitation Centre over 2013–2015. Leprosy Review 90: 161–66. [Google Scholar] [CrossRef]
- Kok, Maryse C., Marjolein Dieleman, Miriam Taegtmeyer, Jacqueline E. W. Broerse, Sumit S. Kane, Hermen Ormel, Mandy M. Tijm, and Korrie A. M. de Koning. 2014. Which Intervention Design Factors Influence Performance of Community Health Workers in Low- and Middle-Income Countries? A Systematic Review. Health Policy and Planning 30: 1207–27. [Google Scholar] [CrossRef] [PubMed]
- Kouassi, Bernard L., Aboulaye Barry, Kathrin Heitz-Tokpa, Stefanie J. Krauth, Andre Goépogui, Mamadou S. Baldé, Oumar Barry, Marie L. Niamey, Moses J. Bockarie, Benjamin G. Koudou, and et al. 2018. Perceptions, Knowledge, Attitudes and Practices for the Prevention and Control of Lymphatic Filariasis in Conakry, Republic of Guinea. Acta Tropica 179: 109–16. [Google Scholar] [CrossRef] [PubMed]
- Krentel, Alison, Margaret Gyapong, Shruti Mallya, Nana Yaa Boadu, Mary Amuyunzu-nyamongo, Mariana Stephens, and Deborah A. Mcfarland. 2017. Review of the Factors Influencing the Motivation of Community Drug Distributors towards the Control and Elimination of Neglected Tropical Diseases (NTDs). PLoS Neglected Tropical Diseases 11: e0006065. [Google Scholar] [CrossRef] [Green Version]
- Kumar, Ram, Adhikari Jeevan, and Bahadur Sherchand. 2015. Awareness and Coverage of Mass Drug Administration for Elimination of Lymphatic Filariasis: A Community Based Cross Sectional Study in Nepal. Journal of Community Health 40: 34–40. [Google Scholar] [CrossRef]
- Kuper, Hannah. 2019. Neglected Tropical Diseases and Disability-What Is the Link? Transactions of the Royal Society of Tropical Medicine and Hygiene 113: 838–43. [Google Scholar] [CrossRef]
- Kuper, Hannah. 2021. Disability, Mental Health, Stigma and Discrimination and Neglected Tropical Diseases. Transactions of The Royal Society of Tropical Medicine and Hygiene 115: 145–46. [Google Scholar] [CrossRef]
- Lal, Vivek, Sukumar Das, Shyamali Pal, Swadesh Ranjan Dhali, Arup Sarkar, and G. Srinivas. 2017. Improving Quality of Care Using Mobile Technology: Experiences from the Urban Leprosy Project in Kolkata, India. Leprosy Review 88: 270–73. [Google Scholar] [CrossRef]
- Levesque, Jean-Frederic, Mark F. Harris, and Grant Russell. 2013. Patient-Centred Access to Health Care: Conceptualising Access at the Interface of Health Systems and Populations. International Journal for Equity in Health 12: 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lira, Karlisson Bezerra, João Jaime Giffoni Leite, Débora Castelo Branco de Souza Collares Maia, Rafael de Mesquita Ferreira Freitas, and Alexsandra Rodrigues Feijão. 2012. Knowledge of the Patients Regarding Leprosy and Adherence to Treatment. Brazilian Journal of Infectious Diseases 16: 472–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lusli, Mimi, Marjolein B. M. Zweekhorst, Beatriz Miranda-Galarza, Ruth M. H. Peters, Sarah Cummings, Francisia S. S. E. Seda, Joske F. G. Bunders, and Irwanto. 2015. Dealing with Stigma: Experiences of Persons Affected by Disabilities and Leprosy. BioMed Research International 2015: 261329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mani, Suresh, Joydeepa Darlong, Annamma John, and Pitchaimani Govindharaj. 2015. Non-Adherence to Steroid Therapy in Leprosy Reaction and Neuritis. Leprosy Review 86: 356–67. [Google Scholar] [CrossRef] [PubMed]
- Marahatta, Sujan Babu, Rakchya Amatya, Srijana Adhikari, Deena Giri, Sarina Lama, Nils Kaehler, Komal Raj Rijal, Suchana Marahatta, and Bipin Adhikari. 2018. Perceived Stigma of Leprosy among Community Members and Health Care Providers in Lalitpur District of Nepal: A Qualitative Study. PLoS ONE 13: e0209676. [Google Scholar] [CrossRef] [PubMed]
- Marega, Abdoulaye, Paulo Das Neves Pires, Jaibo Mucufo, and Artur Muloliwa. 2019. Hansen’s Disease Deformities in a High Risk Area in Mozambique: A Case Study. Revista Da Sociedade Brasileira de Medicina Tropical 52: 2. [Google Scholar] [CrossRef] [PubMed]
- Marks, Michael, Cynthia Kwakye-Maclean, Rachel Doherty, Paul Adwere, Abdul Aziz Abdulai, Fredrick Duah, Sally Ann Ohene, Oriol Mitja, Blanche Oguti, Anthony W. Solomon, and et al. 2017. Knowledge, Attitudes and Practices towards Yaws and Yaws-like Skin Disease in Ghana. PLoS Neglected Tropical Diseases 11: e0005820. [Google Scholar] [CrossRef] [Green Version]
- Mues, Katherine E., Michael Deming, David G. Kleinbaum, Philip J. Budge, Mitch Klein, Juan S. Leon, Aishya Prakash, Jonathan Rout, and Le Anne M. Fox. 2014. Impact of a Community-Based Lymphedema Management Program on Episodes of Adenolymphangitis (ADLA) and Lymphedema Progression—Odisha State, India. PLoS Neglected Tropical Diseases 8: e3140. [Google Scholar] [CrossRef] [Green Version]
- Muthuvel, Thirumugam, Srinivas Govindarajulu, Petros Isaakidis, Hemant Deepak Shewade, Vasudev Rokade, Rajbir Singh, and Sanjeev Kamble. 2017. ‘I Wasted 3 Years, Thinking It’s Not a Problem’: Patient and Health System Delays in Diagnosis of Leprosy in India: A Mixed-Methods Study. PLoS Neglected Tropical Diseases 11: e0005192. [Google Scholar] [CrossRef] [Green Version]
- Nsai, Frankline Sanyuy, Samuel Nambile Cumber, Ngwayu Claude Nkfusai, Vecheusi Zennobia Viyoff, Nkemngu Blake Afutendem, Rosaline Yumumkah Cumber, Joyce Mahlako Tsoka-Gwegweni, and Jane Francis Tata Kihla Akoachere. 2018. Knowledge and Practices of Health Practitioners on Treatment of Buruli Ulcer in the Mbonge, Ekondo Titi and Muyuka Health Districts, South West Region, Cameroon. Pan African Medical Journal 31: 228. [Google Scholar] [CrossRef]
- Nwafor, Charles Chukwunalu, Anthony Meka, Joseph Ngozi Chukwu, Ngozi Ekeke, Chukwuka Alphonsus, Obinna Mbah, Nelson Okechukwu Madichie, Ufuoma Aduh, Matthew Ogbeifo, Bola Olubakin IseOluwa-Adelokiki, and et al. 2019. Assessment of Community Knowledge, Attitude, and Stigma of Buruli Ulcer Disease in Southern Nigeria. African Health Sciences 19: 2100–11. [Google Scholar] [CrossRef] [Green Version]
- Ocaya, A., F. Kironde, and E. I. Odongo-Aginya. 2015. Knowledge and Attitude towards Buruli Ulcer Disease in Adjumani District, Northwestern Uganda. East African Medical Journal 92: 537–41. [Google Scholar]
- Oluwole, Akinola, Laura Dean, Luret Lar, Kabiru Salami, Okefu Okoko, Sunday Isiyaku, Ruth Dixon, Elizabeth Elhassan, Elena Schmidt, Rachael Thomson, and et al. 2019. Optimising the Performance of Frontline Implementers Engaged in the NTD Programme in Nigeria: Lessons for Strengthening Community Health Systems for Universal Health Coverage. Human Resources for Health 17: 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, Georgina. 2018. Understanding Perceptions on ‘Buruli’ in Northwestern Uganda: A Biosocial Investigation. PLoS Neglected Tropical Diseases 12: e0006689. [Google Scholar] [CrossRef] [Green Version]
- Peeters Grietens, Koen, Elizabeth Toomer, Alphonse Um Boock, Susanna Hausmann-Muela, Hans Peeters, Kirezi Kanobana, Charlotte Gryseels, and Joan Muela Ribera. 2012. What Role Do Traditional Beliefs Play in Treatment Seeking and Delay for Buruli Ulcer Disease?-Insights from a Mixed Methods Study in Cameroon. PLoS ONE 7: e36954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochazka, Mateo, Joseph Timothy, Rachel Pullan, Karsor Kollie, Emerson Rogers, Abednego Wright, and Jennifer Palmer. 2020. ‘Buruli Ulcer and Leprosy, They Are Intertwined’: Patient Experiences of Integrated Case Management of Skin Neglected Tropical Diseases in Liberia. PLoS Neglected Tropical Diseases 14: e0008030. [Google Scholar] [CrossRef] [PubMed]
- Pryce, Joseph, Hayley E. Mableson, Ramesh Choudhary, Basu Dev Pandey, Dambar Aley, Hannah Betts, Charles D. Mackenzie, Louise A. Kelly-Hope, and Hugh Cross. 2018. Assessing the Feasibility of Integration of Self-Care for Filarial Lymphoedema into Existing Community Leprosy Self-Help Groups in Nepal. BMC Public Health 18: 201. [Google Scholar] [CrossRef] [Green Version]
- Rai, Sarju Sing, Irwanto, Ruth M.H. Peters, Elena V. Syurina, Annisa Ika Putri, Altana Mikhakhanova, Denise Naniche, and Marjolein B. M. Zweekhorst. 2020. Qualitative Exploration of Experiences and Consequences of Health-Related Stigma among Indonesians with HIV, Leprosy, Schizophrenia and Diabetes. Kesmas 15: 7–16. [Google Scholar] [CrossRef]
- Ramos, José M., Miguel Martínez-Martín, Francisco Reyes, Deriba Lemma, Isabel Belinchón, and Félix Gutiérrez. 2012. Gender differential on characteristics and outcome of leprosy patients admitted to a long-term care rural hospital in South-Eastern Ethiopia. International Journal for Equity in Health 11: 1–7. [Google Scholar] [CrossRef] [Green Version]
- Renita, Lourdhurajan, Susanne A. Pulimood, Elizabeth Pushpa Eapen, Jayaprakash Muliyil, and K. R. John. 2010. Health Care Utilisation in Indian Leprosy Patients in the Era of Elimination. Leprosy Review 81: 299–305. [Google Scholar] [CrossRef]
- Rogers, Julia H., Lassana Jabateh, Jason Beste, Bradley H. Wagenaar, Ryan McBain, Daniel Palazuelos, Eugene Wickett, Catherine Oswald, Harriet G. Napier, and Julia Toomey-Garbo. 2018. Impact of Community-Based Adherence Support on Treatment Outcomes for Tuberculosis, Leprosy and HIV/AIDS-Infected Individuals in Post-Ebola Liberia. Global Health Action 11: 1522150. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, Jhuma, Aparajita Dasgupta, and Debashis Dutt. 2012. Disability among new leprosy patients, an issue of concern: An institution based study in an endemic district for leprosy in the state of West Bengal, India. Indian Journal of Dermatology, Venereology and Leprology 78: 328–34. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, Rashmi, and Swetalina Pradhan. 2016. Leprosy and Women. International Journal of Women’s Dermatology 2: 117–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sightsavers. 2021. UK Government Cuts Funding for Neglected Tropical Diseases. Available online: https://www.sightsavers.org/news/2021/06/uk-government-cuts-funding-for-neglected-tropical-diseases/ (accessed on 7 February 2022).
- Singh, Harminder, BithikaNel Kumar, Kamalpreet Kaur, PramodKumar Kar, Akash Bansal, and Vinod KumarSingh Chauhan. 2013. A 3 Years Experience of Treating Tribal Leprosy Patients and Its Impact on Various Domains of Patient′s Life. International Journal of Health & Allied Sciences 2: 13. [Google Scholar] [CrossRef]
- Singh, Rakesh, Babita Singh, and Sharika Mahato. 2019. Community knowledge, attitude, and perceived stigma of leprosy amongst community members living in Dhanusha and Parsa districts of Southern Central Nepal. PLoS Neglected Tropical Diseases 13: e0007075. [Google Scholar] [CrossRef]
- Srinivas, Govindarajulu, Shuba Kumar, Rani Mohanraj, Geethalakshmi Sekkizhar, Thirumugam Muthuvel Id, Vivek Lal, Burkard Koemm, and Christa Kasang. 2018. Development and Validation of a Scale to Assess Attitudes of Health Care Providers towards Persons Affected by Leprosy in Southern India. PLoS Neglected Tropical Diseases 6: e0006808. [Google Scholar] [CrossRef] [PubMed]
- Stanton, Michelle C., Abigail Best, Matthew Cliffe, Louise Kelly-Hope, Nana Kwadwo Biritwum, Linda Batsa, and Alex Debrah. 2016. Situational Analysis of Lymphatic Filariasis Morbidity in Ahanta West District of Ghana. Tropical Medicine and International Health 21: 236–44. [Google Scholar] [CrossRef]
- Stanton, Michelle C., Emma L. Smith, Sarah Martindale, Square Z. Mkwanda, and Louise A. Kelly-Hopea. 2015. Exploring Hydrocoele Surgery Accessibility and Impact in a Lymphatic Filariasis Endemic Area of Southern Malawi. Transactions of the Royal Society of Tropical Medicine and Hygiene 109: 252–61. [Google Scholar] [CrossRef] [PubMed]
- Subedi, Madhusudan, and Ulla-Britt Engelbrektsson. 2018. Factors Contributing to Delay in Diagnosis and Start of Treatment of Leprosy: Analysis of Help-Seeking Narratives from a Community Study in Dang District. Dhaulagiri Journal of Sociology and Anthropology 12: 11–17. [Google Scholar] [CrossRef]
- Sun, Nina, and Joseph Amon. 2018. Addressing Inequity: Neglected Tropical Diseases and Human Rights. Health and Human Rights Journa 20: 11–26. Available online: https://cdn2.sph.harvard.edu/wp-content/uploads/sites/125/2018/06/Amon.pdf (accessed on 14 May 2022).
- Susanto, Tantut, Erti Ikhtiarini Dewi, and Iis Rahmawati. 2017. The Experiences of People Affected by Leprosy Who Participated in Self-Care Groups in the Community: A Qualitative Study in Indonesia. Leprosy Review 88: 543–53. [Google Scholar] [CrossRef]
- Tabah, Earnest Njih, Dickson Shey Nsagha, Anne Cécile Zoung Kanyi Bissek, Theophilus Ngeh Njamnshi, Irine Ngani Nformi Njih, Gerd Pluschke, and Alfred Kongnyu Njamnshi. 2018. Community Knowledge, Perceptions and Attitudes Regarding Leprosy in Rural Cameroon: The Case of Ekondotiti and Mbonge Health Districts in the South-West Region. PLoS Neglected Tropical Diseases 12: e0006233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tembei, Ayok M., Jonas A. Kengne-Ouaffo, Elvis A. Ngoh, Bonekeh John, Theobald M. Nji, Kebede Deribe, Peter Enyong, Theresa Nkuo-Akenji, Gail Davey, and Samuel Wanji. 2018. A comparative analysis of economic cost of podoconiosis and leprosy on affected households in the Northwest Region of Cameroon. The American Journal of Tropical Medicine and Hygiene 98: 1075–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ukwaja, Kingsley N., Chukwuka Alphonsus, Chinwe C. Eze, Linda Lehman, Ngozi Ekeke, Charles C. Nwafor, Joy Ikebudu, Moses C. Anyim, and Joseph N. Chukwu. 2020. Investigating Barriers and Challenges to the Integrated Management of Neglected Tropical Skin Diseases in an Endemic Setting in Nigeria. PLoS Neglected Tropical Diseases 14: e0008248. [Google Scholar] [CrossRef] [PubMed]
- Velink, Anita, Rebecca J. Woolley, Richard O. Phillips, Kabiru M. Abass, Tjip S. van der Werf, Emmanuel Agumah, Janine de Zeeuw, Sandor Klis, and Ymkje Stienstra. 2016. Former Buruli Ulcer Patients’ Experiences and Wishes May Serve as a Guide to Further Improve Buruli Ulcer Management. PLoS Neglected Tropical Diseases 10: e0005261. [Google Scholar] [CrossRef] [PubMed]
- Villacorta Linaza, Rocio, Timothy Garner, and Chantelle Genovezos. 2021. Building Supply Chain Capacity for Neglected Tropical Diseases: Experience from the Ascend West and Central Africa Programme. Transactions of the Royal Society of Tropical Medicine and Hygiene 115: 841–46. [Google Scholar] [CrossRef] [PubMed]
- Vouking, Marius Zambou, Violette Claire Tamo, and Lawrence Mbuagbaw. 2013. The Impact of Community Health Workers (CHWs) on Buruli Ulcer in Sub-Saharan Africa: A Systematic Review. The Pan African Medical Journal 15: 19. [Google Scholar] [CrossRef]
- Wharton-Smith, Alexandra, Christian Rassi, Esey Batisso, Giuseppina Ortu, Rebecca King, Misganu Endriyas, Helen Counihan, Prudence Hamade, and Dawit Getachew. 2019. Gender-Related Factors Affecting Health Seeking for Neglected Tropical Diseases: Findings from a Qualitative Study in Ethiopia. PLoS Neglected Tropical Diseases 13: e0007840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. 2008. Closing the Gap in a Generation. Available online: http://www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf (accessed on 14 May 2020).
- WHO. 2020. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. Geneva: World Health Organization, Available online: https://www.who.int/neglected_diseases/revised-draftntd-roadmap-23apr2020.pdf (accessed on 7 July 2020).
- Wijeratne, Monika Priyadarshani, and Truls Østbye. 2017. Knowledge, Attitudes and Practices Relating to Leprosy among Public Health Care Providers in Colombo, Sri Lanka. Leprosy Review 88: 75–84. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=30188095&site=ehost-live (accessed on 7 July 2020). [CrossRef]
- World Health Organization. 2020. Mental Health of People with Neglected Tropical Diseases: Towards a Person-Centred Approach. Available online: https://www.who.int/health-topics/mental-health#tab=tab_2 (accessed on 7 July 2020).
- Ziperstein, Josh, Monique Dorkenoo, Michel Datagni, Naomi Drexler, Monica Murphy, Yao Sodahlon, and Els Mathieu. 2014. Final Program Evaluation Methods and Results of a National Lymphedema Management Program in Togo, West Africa. Journal of Epidemiology and Global Health 4: 125–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Health-Seeking | SSSDs | LMIC |
|---|---|---|
| Access Availability Help Utilisation Behaviour Seek Practice Perception Attitude Belief Enabler Barrier Demand | Skin disease Neglected tropical diseases Leprosy Buruli Ulcer Yaws Lymphoedema Lymphatic filiariasis Hydrocele | Sub-Saharan Africa Africa Low and middle income countries Liberia Developing countries |
| Study | Country of Focus | Geographic Region | Chronic Condition/Disease of Focus | Methodology |
|---|---|---|---|---|
| (Abdulmalik et al. 2018) | Nigeria | SSA | Lymphatic Filariasis | qualitative |
| (Abedi et al. 2013) | Iran | Western Asia | Leprosy | qualitative |
| (Ackumey et al. 2011) | Ghana | SSA | Buruli ulcer | quantitative |
| (Adhikari et al. 2015) | Nepal | Asia | Lymphoedema | qualitative |
| (Alferink et al. 2013) | Benin | SSA | Buruli ulcer | quantitative |
| (John et al. 2010) | India | Asia | Leprosy | quantitative |
| (Atre et al. 2011) | India | Asia | Leprosy | mixed |
| (Dean et al. 2019) | Liberia | SSA | Mixed NTDs-lymphatic filariasis, leprosy, Buruli Ulcer, and onchocerciasis | qualitative |
| (Dupnik et al. 2013) | Brazil | South America | leprosy | quantitative |
| (Garchitorena et al. 2015) | SSA | SSA | Buruli ulcer | modelling |
| (Gautham et al. 2011) | India | Asia | Leprosy | quantitative |
| (Girma et al. 2018) | Ethiopia | SSA | leprosy | quantitative |
| (Gómez et al. 2018) | Colombia | South America | leprosy | quantitative |
| (Henry et al. 2016) | Brazil | South America | leprosy | quantitative |
| (Heukelbach et al. 2011) | Brazil | South America | leprosy | quantitative |
| (Ibe et al. 2015) | Nigeria | SSA | onchocerciasis | quantitative |
| (Kasang et al. 2019) | Liberia | SSA | Leprosy | quantitative |
| (Kouassi et al. 2018) | Guinea | SSA | Lymphatic Filariasis | mixed |
| (De Kruijff 2015) | Mozambique | SSA | Leprosy | quantitative |
| (Kumar et al. 2015) | India | Asia | Leprosy | quantitative |
| (Lira et al. 2012) | Brazil | South America | Leprosy | quantitative |
| (Renita et al. 2010) | Brazil | South America | Leprosy | quantitative |
| (Lusli et al. 2015) | India | Asia | Leprosy | mixed |
| (Marahatta et al. 2018) | Nepal | Asia | Leprosy | qualitative |
| (Marega et al. 2019) | Mozambiqu | SSA | Leprosy | quantitative |
| (Marks et al. 2017) | Ghana | SSA | Yaws | mixed |
| (Mues et al. 2014) | India | Asia | Lymphoedema | quantitative |
| (Nsai et al. 2018) | Cameroon | SSA | Buruli ulcer | quantitative |
| (Nwafor et al. 2019) | Nigeria | SSA | Buruli ulcer | quantitative |
| (Ocaya et al. 2015) | Uganda | SSA | Buruli ulcer | quantitative |
| (Gupta 2015) | India | Asia | Leprosy | report |
| (Pearson 2018) | Uganda | SSA | Buruli ulcer | qualitative |
| (Peeters Grietens et al. 2012) | Cameroon | SSA | Buruli ulcer | mixed |
| (Prochazka et al. 2020) | Liberia | SSA | Buruli ulcer, leprosy | qualitative |
| (Pryce et al. 2018) | Nepal | Asia | Lymphatic Filariasis | quantitative |
| (Rai et al. 2020) | Indonesia | Asia | leprosy | qualitative |
| (Singh et al. 2013) | Nepal | Asia | Leprosy | quantitative |
| (Ramos et al. 2012) | Ethiopia | SSA | leprosy | quantitative |
| (Rogers et al. 2018) | Liberia | SSA | Leprosy | quantitative |
| (Sarkar and Pradhan 2016) | Global | Global | Leprosy | review |
| (Sarkar et al. 2012) | India | Asia | leprosy | review |
| (Da Silva and Paz 2019) | Brazil | South America | Leprosy | qualitative |
| (Stanton et al. 2016) | Ghana | SSA | Lymphatic Filariasis | mixed |
| (Stanton et al. 2015) | Malawi | SSA | Lymphatic Filariasis | quantitative |
| (Subedi and Engelbrektsson 2018) | Nepal | Asia | Leprosy | qualitative |
| (Mani et al. 2015) | India | Asia | Leprosy | quantitative |
| (Susanto et al. 2017) | Indonesia | Asia | Leprosy | qualitative |
| (Tabah et al. 2018) | Cameroon | SSA | Leprosy | quantitative |
| (Tembei et al. 2018) | Cameroon | SSA | Leprosy | quantitative |
| (Muthuvel et al. 2017) | India | Asia | Leprosy | mixed |
| (Velink et al. 2016) | Ghana | SSA | Buruli ulcer | mixed |
| (Lal et al. 2017) | India | Asia | Leprosy | quantitative |
| (Wharton-Smith et al. 2019) | Ethiopia | SSA | Mixed NTDs, including lymphatic filariasis | qualitative |
| (Wijeratne and Østbye 2017) | Sri Lanka | Asia | leprosy | quantitative |
| (Ziperstein et al. 2014) | Togo | SSA | Lymphoedema | qualitative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCollum, R.; Berrian, H.; Theobald, S.; Zaizay, Z.; Kollie, K.; Dean, L. Barriers and Enablers to Health-Seeking for People Affected by Severe Stigmatising Skin Diseases (SSSDs): A Scoping Review. Soc. Sci. 2022, 11, 332. https://doi.org/10.3390/socsci11080332
McCollum R, Berrian H, Theobald S, Zaizay Z, Kollie K, Dean L. Barriers and Enablers to Health-Seeking for People Affected by Severe Stigmatising Skin Diseases (SSSDs): A Scoping Review. Social Sciences. 2022; 11(8):332. https://doi.org/10.3390/socsci11080332
Chicago/Turabian StyleMcCollum, Rosalind, Hannah Berrian, Sally Theobald, Zeela Zaizay, Karsor Kollie, and Laura Dean. 2022. "Barriers and Enablers to Health-Seeking for People Affected by Severe Stigmatising Skin Diseases (SSSDs): A Scoping Review" Social Sciences 11, no. 8: 332. https://doi.org/10.3390/socsci11080332