
Meta-Analysis of Parent Training Programs Utilizing Behavior Intervention Technologies


Abstract
:1. Introduction
2. Materials and Methods
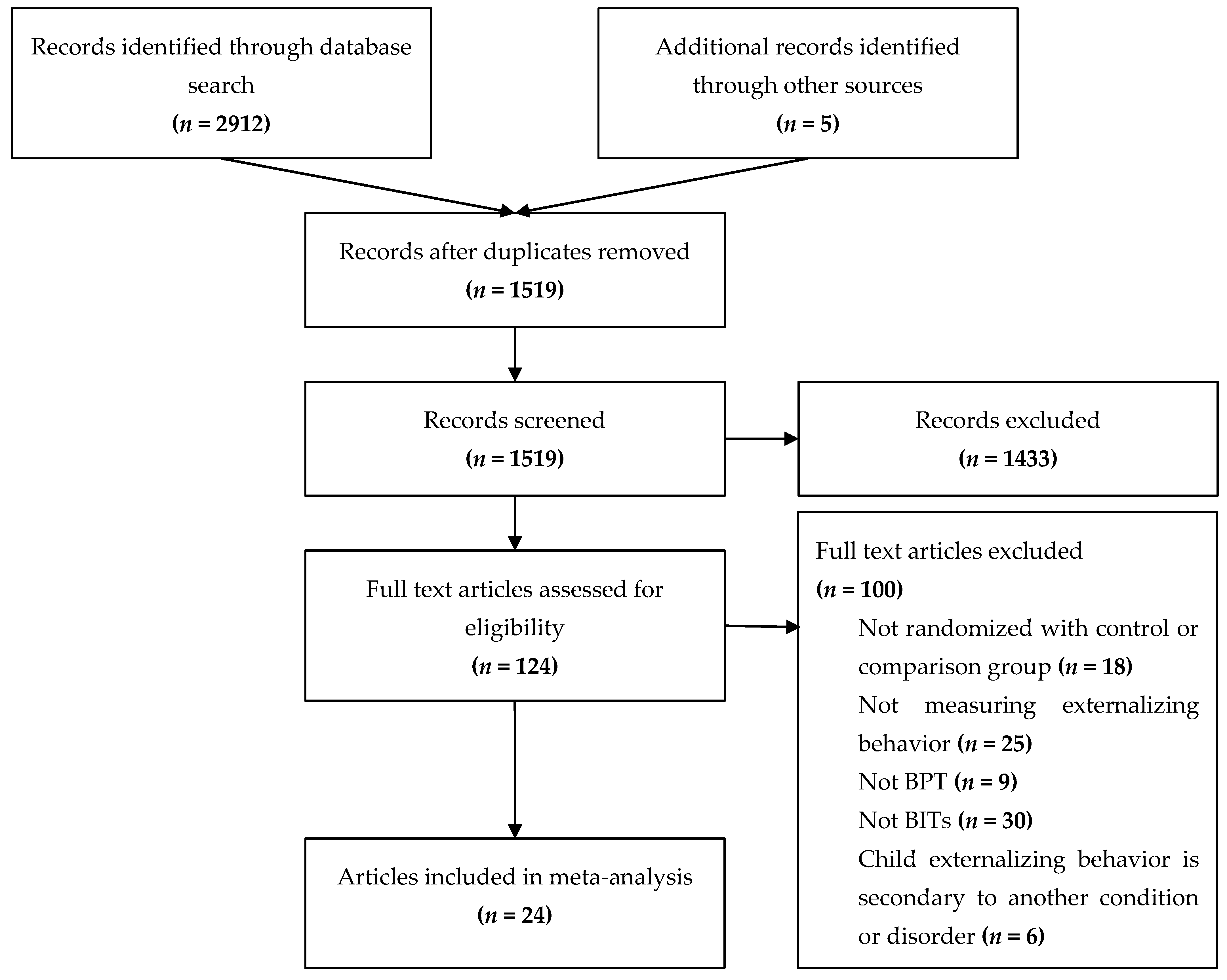
2.1. Selection Process of Articles
2.1.1. Classification of Behavioral Parent Trainings Programs
2.1.2. Methodological Quality
2.2. Measures
2.3. Data Synthesis
3. Results
3.1. Methodological Quality
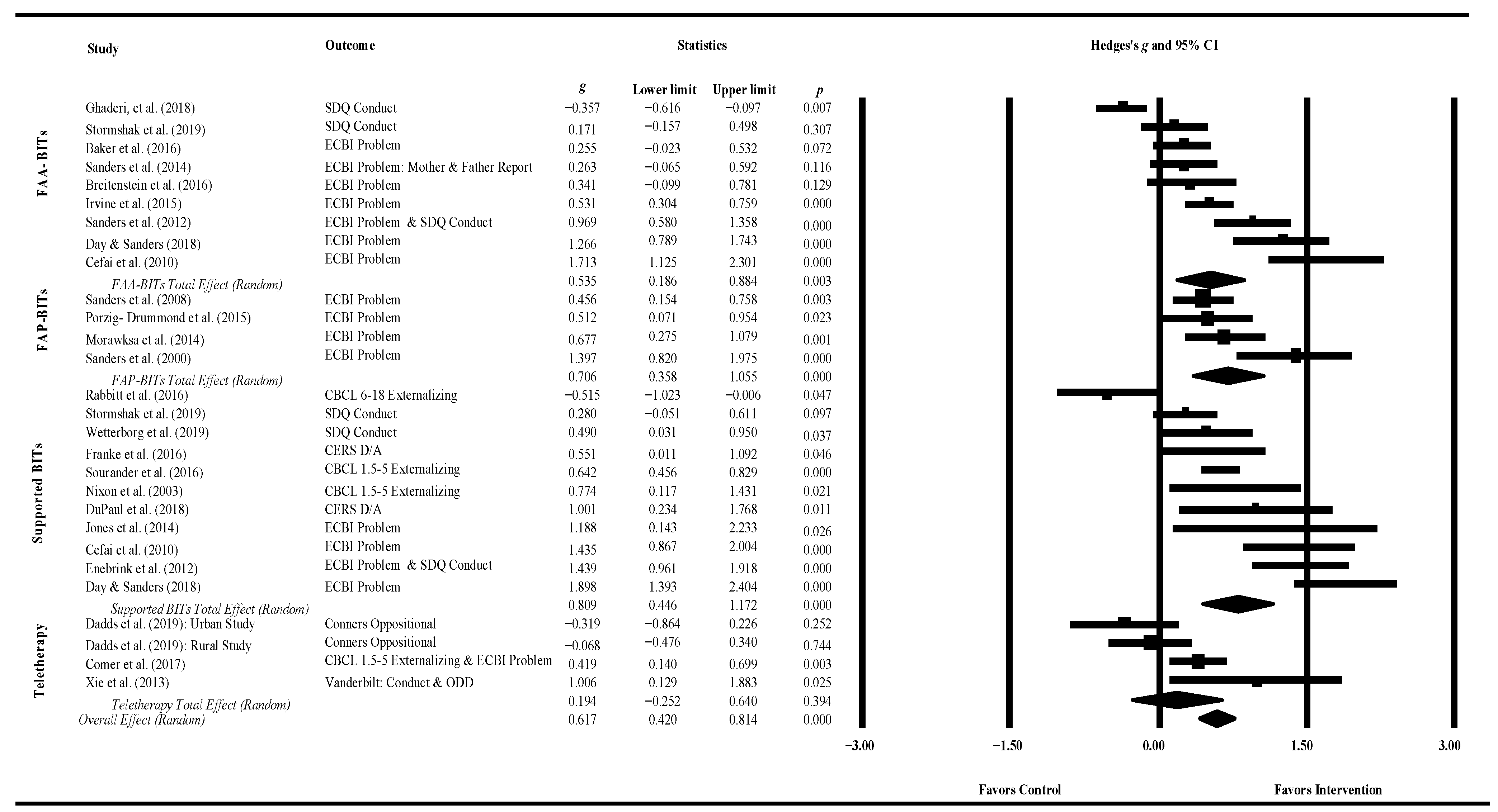
3.2. Primary Comparison
3.2.1. All Studies
3.2.2. Waitlist Control Studies
3.2.3. Active Control Studies
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Methodological Quality Rating

{kind=link}
{kind=link}
{kind=link}
| Item Number | Topic | Item Description |
|---|---|---|
| TITLE and ABSTRACT | ||
| 1 | Title | Identify the research as a single-case experimental design in the title |
| 2 | Abstract | Summarize the research question, population, design, methods including intervention/s (independent variable/s) and target behavior/s and any other outcome/s (dependent variable/s), results, and conclusions |
| INTRODUCTION | ||
| 3 | Scientific background | Describe the scientific background to identify issue/s under analysis, current scientific knowledge, and gaps in that knowledge base |
| 4 | Aims | State the purpose/aims of the study, research question/s, and, if applicable, hypotheses |
| METHOD | ||
| 5 | Design | Identify the design (e.g., withdrawal/reversal, multiple-baseline, alternating-treatments, changing-criterion, some combination thereof, or adaptive design) and describe the phases and phase sequence (whether determined a priori or data-driven) and, if applicable, criteria for phase change |
| 6 | Procedural Changes | Describe any procedural changes that occurred during the course of the investigation after the start of the study |
| 7 | Replication | Describe any planned replication |
| 8 | Randomization | State whether randomization was used, and if so, describe the randomization method and the elements of the study that were randomized |
| 9 | Blinding | State whether blinding/masking was used, and if so, describe who was blinded/masked |
| PARTICIPANT/S or UNITS | ||
| 10 | Selection criteria | State the inclusion and exclusion criteria, if applicable, and the method of recruitment |
| 11 | Participant characteristics | For each participant, describe the demographic characteristics and clinical (or other) features relevant to the research question, such that anonymity is ensured |
| CONTEXT | ||
| 12 | Setting | Describe characteristics of the setting and location where the study was conducted |
| APPROVALS | ||
| 13 | Ethics | State whether ethics approval was obtained and indicate if and how informed consent and/or assent were obtained |
| MEASURES and MATERIALS | ||
| 14 | Measures | Operationally define all target behaviors and outcome measures, describe reliability and validity, state how they were selected, and how and when they were measured |
| 15 | Equipment | Clearly describe any equipment and/or materials (e.g., technological aids, biofeedback, computer programs, intervention manuals or other material resources) used to measure target behavior/s and other outcome/s or deliver the interventions |
| INTERVENTIONS | ||
| 16 | Intervention | Describe the intervention and control condition in each phase, including how and when they were actually administered, with as much detail as possible to facilitate attempts at replication |
| 17 | Procedural fidelity | Describe how procedural fidelity was evaluated in each phase |
| ANALYSIS | ||
| 18 | Analyses | Describe and justify all methods used to analyze data |
| RESULTS | ||
| 19 | Sequence completed | For each participant, report the sequence actually completed, including the number of trials for each session for each case. For participant/s who did not complete, state when they stopped and the reasons |
| 20 | Outcomes and estimation | For each participant, report results, including raw data, for each target behavior and other outcome/s |
| 21 | Adverse events | State whether or not any adverse events occurred for any participant and the phase in which they occurred |
| DISCUSSION | ||
| 22 | Interpretation | Summarize findings and interpret the results in the context of current evidence |
| 23 | Limitations | Discuss limitations, addressing sources of potential bias and imprecision |
| 24 | Applicability | Discuss applicability and implications of the study findings |
| DOCUMENTATION | ||
| 25 | Protocol | If available, state where a study protocol can be accessed |
| 26 | Funding | Identify source/s of funding and other support; describe the role of funders |
References
- Able, Stephen L., Joseph A. Johnston, Lenard A. Adler, and Ralph W. Swindle. 2007. Functional and psychosocial impairment in adults with undiagnosed ADHD. Psychological Medicine 37: 97–107. [Google Scholar] [CrossRef]
- Achenbach, Thomas M. 1991. Child Behavior Checklist/4–18. Burlington: University of Vermont. [Google Scholar]
- Achenbach, Thomas M., and Leslie A. Rescorla. 2000. Manual for the ASEBA Preschool Forms and Profiles. Burlington: Department of Psychiatry, University of Vermont. [Google Scholar]
- Aiken, Leona S., Stephen G. West, and Raymond R. Reno. 1991. Multiple Regression: Testing and Interpreting Interactions. Thousand Oaks: Sage. [Google Scholar]
- Andersson, Gerhard, and Pim Cuijpers. 2009. Internet-Based and Other Computerized Psychological Treatments for Adult Depression: A Meta-Analysis. Cognitive Behaviour Therapy 38: 196–205. [Google Scholar] [CrossRef]
- Baker, Sabine, Matthew R. Sanders, Karen M. T. Turner, and Alina Morawska. 2017. A randomized controlled trial evaluating a low-intensity interactive online parenting intervention, Triple P Online Brief, with parents of children with early onset conduct problems. Behaviour Research and Therapy 91: 78–90. [Google Scholar] [CrossRef] [Green Version]
- Bard, David E., Mark L. Wolraich, Barbara Neas, Melissa Doffing, and Laoma Beck. 2013. The psychometric properties of the Vanderbilt Attention-Deficit Hyperactivity Disorder Diagnostic Parent Rating Scale in a community population. Journal of Developmental and Behavioral Pediatrics 34: 72–82. [Google Scholar] [CrossRef]
- Baumeister, Harald, Lars Reichler, Marie Munzinger, and Jiaxi Lin. 2014. The impact of guidance on Internet-based mental health interventions: A systematic review. Internet Interventions 1: 205–15. [Google Scholar] [CrossRef] [Green Version]
- Baumel, Amit, Aditya Pawar, John M. Kane, and Christoph U. Correll. 2016. Digital parent training for children with disruptive behaviors: Systematic review and meta-analysis of randomized trials. Journal of Child and Adolescent Psychopharmacology 26: 740–49. [Google Scholar] [CrossRef] [PubMed]
- Bolier, Linda, Cristina Majo, Filip Smit, Gerben J. Westerhof, Merel Haverman, Jan A. Walburg, Heleen Riper, and Ernst Bohlmeijer. 2014. Cost-effectiveness of online positive psychology: Randomized controlled trial. The Journal of Positive Psychology 9: 460–71. [Google Scholar] [CrossRef]
- Borenstein, Michael. 2005. Software for publication bias. In Publication Bias in Meta-Analysis: Prevention, Assessment, and Adjustments. Edited by Hannah R. Rothstein, Alexander J. Sutton and Michael Borenstein. Chichester: John Wiley & Sons, pp. 193–220. [Google Scholar]
- Borenstein, Michael, Harris Cooper, Larry V. Hedges, and Jeffrey C. Valentine. 2009. Effect sizes for continuous data. In The Handbook of Research Synthesis and Meta-Analysis. New York: Russell Sage Foundation, vol. 2, pp. 221–35. [Google Scholar]
- Borenstein, Michael, Larry Hedges, Julian P. T. Higgins, and Hannah Rothstein. 2014. Comprehensive Meta-Analysis. Computer Program. Version 3. Englewood: Biostat. [Google Scholar]
- Borenstein, Michael, Larry V. Hedges, Julian P. T. Higgins, and Hannah Rothstein. 2015. Regression in meta-analysis. In Comprehensive Meta Analysis Manual. Englewood: Biostat Inc. [Google Scholar]
- Breitenstein, Susan M., Louis Fogg, Edith V. Ocampo, Diana I. Acosta, and Deborah Gross. 2016. Parent use and efficacy of a self-administered, tablet-based parent training intervention: A randomized controlled trial. JMIR mHealth and uHealth 4: e36. [Google Scholar] [CrossRef]
- Card, Noel A. 2012. Applied Meta-Analysis for Social Science Research. New York: The Guilford Press. [Google Scholar]
- Cefai, Josie, David Smith, and Robert E. Pushak. 2010. Parenting wisely: Parent training via CD-ROM with an Australian sample. Child and Family Behavior Therapy 32: 17–33. [Google Scholar] [CrossRef]
- Chacko, Anil, Scott A. Jensen, Lynda S. Lowry, Melinda Cornwell, Alyssa Chimklis, Elizabeth Chan, Daniel Lee, and Brenda Pulgarin. 2016. Engagement in behavioral parent training: Review of the literature and implications for practice. Clinical Child and Family Psychology Review 19: 204–15. [Google Scholar] [CrossRef]
- Anil Chacko, Carla Counts Allan, Simone S. Moody, Trista Perez Crawford, Cy Nadler, and Alyssa Chimiklis. 2017. Behavioral interventions. In Handbook of DSM–5 Disorders in Children and Adolescents. Edited by Sam Goldstein and Melissa DeVries. Cham: Springer, pp. 617–36. [Google Scholar]
- Chorpita, Bruce F., Eric L. Daleiden, Chad Ebesutani, John Young, Kimberly D. Becker, Brad J. Nakamura, Lisa Phillips, Alyssa Ward, Roxanna Lynch, Lindsay Trent, and et al. 2011. Evidence-based treatments for children and adolescents: An updated review of indicators of efficacy and effectiveness. Clinical Psychology: Science and Practice 18: 154–72. [Google Scholar] [CrossRef]
- Cohen, Mark A. 1998. The monetary value of saving a high-risk youth. Journal of Quantitative Criminology 14: 5–33. [Google Scholar] [CrossRef]
- Comer, Jonathan S., and Kathleen Myers. 2016. Future directions in the use of telemental health to improve the accessibility and quality of children’s mental health services. Journal of Child and Adolescent Psychopharmacology 26: 296–300. [Google Scholar] [CrossRef] [PubMed]
- Comer, Jonathan S., Candice Chow, Priscilla T. Chan, Christine Cooper-Vince, and Lianna A. S. Wilson. 2013. Psychosocial treatment efficacy for disruptive behavior problems in very young children: A meta-analytic examination. Journal of the American Academy of Child and Adolescent Psychiatry 52: 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comer, Jonathan S., Jami M. Furr, Elizabeth M. Miguel, Christine E. Cooper-Vince, Aubrey L. Carpenter, R. Meredith Elkins, Caroline E. Kerns, Danielle Cornacchio, Tommy Chou, Stefany Coxe, and et al. 2017. Remotely delivering real-time parent training to the home: An initial randomized trial of Internet-delivered parent–child interaction therapy (I-PCIT). Journal of Consulting and Clinical Psychology 85: 909. [Google Scholar] [CrossRef] [PubMed]
- Conners, Keith. 2009. Conners Early Childhood. New York: Multi-Health Systems. [Google Scholar]
- Conners, Keith. 2018. Conners Early Childhood. Edited by Conners E. C. Brochure. New York: Multi-Health Systems. [Google Scholar]
- Conners, C. Keith, Gill Sitarenios, James D. A. Parker, and Jeffery N. Epstein. 1998. The revised Conners’ Parent Rating Scale (CPRS-R): Factor structure, reliability, and criterion validity. Journal of Abnormal Child Psychology 26: 257–68. [Google Scholar] [CrossRef]
- Corralejo, Samantha M., and Melanie M. Domenech Rodríguez. 2018. Technology in parenting programs: A systematic review of existing interventions. Journal of Child and Family Studies 27: 2717–31. [Google Scholar] [CrossRef]
- Dadds, Mark R., Christina Thai, Antonio Mendoza Diaz, Joshua Broderick, Caroline Moul, Lucy A. Tully, David J. Hawes, Suzanne Davies, Katherine Burchfield, and Lindsay Cane. 2019. Therapist-assisted online treatment for child conduct problems in rural and urban families: Two randomized controlled trials. Journal of Consulting and Clinical Psychology 87: 706–19. [Google Scholar] [CrossRef]
- Day, Jamin J., and Matthew R. Sanders. 2017. Mediators of parenting change within a web-based parenting program: Evidence from a randomized controlled trial of Triple P Online. Couple and Family Psychology: Research and Practice 6: 154. [Google Scholar] [CrossRef]
- Day, Jamin J., and Matthew R. Sanders. 2018. Do parents benefit from help when completing a self-guided parenting program online? A randomized controlled trial comparing Triple P Online with and without telephone support. Behavior Therapy 49: 1020–38. [Google Scholar] [CrossRef] [Green Version]
- Desatnik, Alex, Charlotte Jarvis, Nisha Hickin, Lara Taylor, David Trevatt, Pia Tohme, and Nicolas Lorenzini. 2021. Preliminary Real-World Evaluation of an Intervention for Parents of Adolescents: The Open Door Approach to Parenting Teenagers (APT). Journal of Child and Family Studies 30: 38–50. [Google Scholar] [CrossRef]
- DuPaul, George J., Lee Kern, Georgia Belk, Beth Custer, Molly Daffner, Andrea Hatfield, and Daniel Peek. 2018. Face-to-face versus online behavioral parent training for young children at risk for ADHD: Treatment engagement and outcomes. Journal of Clinical Child and Adolescent Psychology 47: 369–83. [Google Scholar] [CrossRef]
- Egger, Helen Link, and Adrian Angold. 2006. Common emotional and behavioral disorders in preschool children: Presentation, nosology, and epidemiology. Journal of Child Psychology and Psychiatry 47: 313–37. [Google Scholar] [CrossRef] [PubMed]
- Egger, Matthias, George Davey Smith, Martin Schneider, and Christoph Minder. 1997. Bias in meta-analysis detected by a simple, graphical test. BMJ 315: 629–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enebrink, Pia, Jens Högström, Martin Forster, and Ata Ghaderi. 2012. Internet-based parent management training: A randomized controlled study. Behaviour Research and Therapy 50: 240–49. [Google Scholar] [CrossRef]
- Eyberg, Sheila M., and Arthur W. Ross. 1999. ECBI and SESBI-R: Eyberg child behavior inventory and Sutter-Eyberg student behavior inventory-revised: Professional manual. Psychological Assessment Resources. Available online: https://www.parinc.com/products/pkey/97 (accessed on 21 August 2021).
- Eyberg, Sheila M., and Arthur W. Ross. 1978. Assessment of child behavior problems: The validation of a new inventory. Journal of Clinical Child and Adolescent Psychology 7: 113–16. [Google Scholar] [CrossRef]
- Eyberg, Sheila M., Stephen R. Boggs, and James Algina. 1995. Parent-child interaction therapy: A psychosocial model for the treatment of young children with conduct problem behavior and their families. Psychopharmacology Bulletin 31: 83–91. [Google Scholar]
- Farmer, Elizabeth M. Z., Scott N. Compton, J. Barbara Burns, and Elizabeth Robertson. 2002. Review of the evidence base for treatment of childhood psychopathology: Externalizing disorders. Journal of Consulting and Clinical Psychology 70: 1267–302. [Google Scholar] [CrossRef]
- Forehand, Rex Lloyd, and Robert Joseph McMahon. 1981. Helping the Noncompliant Child: A Clinician’s Guide to Parent Training. New York: Guilford Press. [Google Scholar]
- Forgatch, Marion S., and Gerald R. Patterson. 2010. Parent Management Training—Oregon Model: An intervention for antisocial behavior in children and adolescents. In Evidence-Based Psychotherapies for Children and Adolescents, 2nd ed. Edited by John R. Weisz and Alan E. Kazdin. New York: Guilford, pp. 159–78. [Google Scholar]
- Foster, E. Michael, Damon E. Jones, and Conduct Problems Prevention Research Group. 2005. The high costs of aggression: Public expenditures resulting from conduct disorder. American Journal of Public Health 95: 1767–72. [Google Scholar] [CrossRef]
- Franke, Nike, Louise J. Keown, and Matthew R. Sanders. 2016. An RCT of an online parenting program for parents of preschool-aged children with ADHD symptoms. Journal of Attention Disorders 24: 1716–26. [Google Scholar] [CrossRef] [PubMed]
- Fu, Rongwei, Gerald Gartlehner, Mark Grant, Tatyana Shamliyan, Art Sedrakyan, Timothy J. Wilt, Lauren Griffith, Mark Oremus, Parminder Raina, Afisi Ismaila, and et al. 2011. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. Journal of Clinical Epidemiology 64: 1187–97. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, María C., Antonio Alarcón, Fernando García, and Enrique Gracia. 2015. Use of alcohol, tobacco, cannabis and other drugs in adolescence: Effects of family and neighborhood. Anales de Psicologia 31: 1000–7. [Google Scholar] [CrossRef]
- Fuentes, María C., Oscar F. Garcia, and Fernando Garcia. 2020. Protective and risk factors for adolescent substance use in Spain: Self-esteem and other indicators of personal well-being and ill-being. Sustainability 12: 5962. [Google Scholar] [CrossRef]
- Garcia, Oscar F., Maria C. Fuentes, Enrique Gracia, Emilia Serra, and Fernando Garcia. 2020. Parenting warmth and strictness across three generations: Parenting styles and psychosocial adjustment. International Journal of Environmental Research and Public Health 17: 7487. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, Ata, Christina Kadesjö, Annika Björnsdotter, and Pia Enebrink. 2018. Randomized effectiveness trial of the family check-up versus internet-delivered parent training (iComet) for families of children with conduct problems. Scientific Reports 8: 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gimenez-Serrano, Sofia, Fernando Garcia, and Oscar F. Garcia. 2021. Parenting styles and its relations with personal and social adjustment beyond adolescence: Is the current evidence enough? European Journal of Developmental Psychology, 1–21. [Google Scholar] [CrossRef]
- Goodman, Robert. 1997. The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry 38: 581–86. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Robert. 2001. Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry 40: 1337–45. [Google Scholar] [CrossRef]
- Grolnick, Wendy S., Madeline R. Levitt, Alessandra J. Caruso, and Rachel E. Lerner. 2021. Effectiveness of a Brief Preventive Parenting Intervention Based in Self-Determination Theory. Journal of Child and Family Studies 30: 905–20. [Google Scholar] [CrossRef]
- Hallgren, Kevin A. 2012. Computing inter-rater reliability for observational data: An overview and tutorial. Tutorials in Quantitative Methods for Psychology 8: 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedges, Larry V., and Ingram Olkin. 1985. Statistical Methods for Meta-Analysis. San Diego: Academic Press. [Google Scholar]
- Higgins, Julian P. T., Simon G. Thompson, Jonathan J. Deeks, and Douglas G. Altman. 2003. Measuring inconsistency in meta-analyses. BMJ 327: 557–60. [Google Scholar] [CrossRef] [Green Version]
- Higgins, Julian P. T., James Thomas, Jacqueline Chandler, Miranda Cumpston, Tianjing Li, Matthew J. Page, and Vivian A. Welch, eds. 2019. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions. Version 6.0 (Updated July 2019). London: Cochrane. [Google Scholar]
- Hunter, John E., and Frank L. Schmidt. 2004. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings. London: Sage Publications. [Google Scholar]
- IBM Corporation. 2019. IBM SPSS Statistics for Mac. Version 26.0. Armonk: IBM Corporation. [Google Scholar]
- Irvine, A. Blair, Vicky A. Gelatt, Michael Hammond, and John R. Seeley. 2015. A randomized study of internet parent training accessed from community technology centers. Prevention Science 16: 597–608. [Google Scholar] [CrossRef]
- Jones, Deborah J., Rex Forehand, Jessica Cuellar, Justin Parent, Amanda Honeycutt, Olga Khavjou, Michelle Gonzalez, Margaret Anton, and Greg A. Newey. 2014. Technology-enhanced program for child disruptive behavior disorders: Development and pilot randomized control trial. Journal of Clinical Child and Adolescent Psychology 43: 88–101. [Google Scholar] [CrossRef] [Green Version]
- Kazak, Anne E., Kimberly Hoagwood, John R. Weisz, Korey Hood, Thomas R. Kratochwill, Luis A. Vargas, and Gerard A. Banez. 2010. A meta-systems approach to evidence-based practice for children and adolescents. American Psychologist 65: 85–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kling, Åsa, Martin Forster, Knut Sundell, and Lennart Melin. 2010. A randomized controlled effectiveness trial of parent management training with varying degrees of therapist support. Behavior Therapy 41: 530–42. [Google Scholar] [CrossRef] [PubMed]
- Lee, Pei-chin, Wern-ing Niew, Hao-jan Yang, Vincent Chin-hung Chen, and Keh-chung Lin. 2012. A meta-analysis of behavioral parent training for children with attention deficit hyperactivity disorder. Research in Developmental Disabilities 33: 2040–49. [Google Scholar] [CrossRef]
- Leijten, Patty, Maartje A. J. Raaijmakers, Bram Orobio de Castro, and Walter Matthys. 2013. Does socioeconomic status matter? A meta-analysis on parent training effectiveness for disruptive child behavior. Journal of Clinical Child and Adolescent Psychology 42: 384–92. [Google Scholar] [CrossRef] [Green Version]
- Liu, Jianghong. 2004. Childhood externalizing behavior: Theory and implications. Journal of Child and Adolescent Psychiatric Nursing 17: 93–103. [Google Scholar] [CrossRef] [Green Version]
- Lobo, Michele A., Mariola Moeyaert, Andrea Baraldi Cunha, and Iryna Babik. 2017. Single-case design, analysis, and quality assessment for intervention research. Journal of Neurologic Physical Therapy 41: 187. [Google Scholar] [CrossRef]
- Lundahl, Brad, Heather J. Risser, and M. Christine Lovejoy. 2006. A meta-analysis of parent training: Moderators and follow-up effects. Clinical Psychology Review 26: 86–104. [Google Scholar] [CrossRef]
- Maughan, Denita R., Elizabeth Christiansen, William R. Jenson, Daniel Olympia, and Elaine Clark. 2005. Behavioral parent training as a treatment for externalizing behaviors and disruptive behavior disorders: A meta-analysis. School Psychology Review 34: 267. [Google Scholar] [CrossRef]
- Merikangas, Kathleen Ries, Jian-ping He, Marcy Burstein, Sonja A. Swanson, Shelli Avenevoli, Lihong Cui, Corina Benjet, Katholiki Georgiades, and Joel Swendsen. 2010. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry 49: 980–89. [Google Scholar] [CrossRef] [Green Version]
- Mingebach, Tanja, Inge Kamp-Becker, Hanna Christiansen, and Linda Weber. 2018. Meta-meta-analysis on the effectiveness of parent-based interventions for the treatment of child externalizing behavior problems. PLoS ONE 13: e0202855. [Google Scholar] [CrossRef] [Green Version]
- Mohr, David C., Michelle Nicole Burns, Stephen M. Schueller, Gregory Clarke, and Michael Klinkman. 2013. Behavioral intervention technologies: Evidence review and recommendations for future research in mental health. General Hospital Psychiatry 35: 332–338. [Google Scholar] [CrossRef] [Green Version]
- Morawska, Alina, Helen Tometzki, and Matthew R. Sanders. 2014. An evaluation of the efficacy of a triple P-positive parenting program podcast series. Journal of Developmental & Behavioral Pediatrics 35: 128–137. [Google Scholar]
- Morris, Scott B. 2008. Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods 11: 364–86. [Google Scholar] [CrossRef]
- Muñoz, Ricardo F. 2017. The efficiency model of support and the creation of digital apothecaries. Clinical Psychology: Science and Practice 24: 46–49. [Google Scholar] [CrossRef]
- Musitu Ochoa, Gonzalo, Clara Maria Isabel Martinez Sanchez, Santiago Yubero, and Jose Fernando GarcÍa Pérez. 2012. Family socialization practices: Factor confirmation of the Portuguese version of a scale for their measurement. Revista de Psicodidactica 17: 159–178. [Google Scholar]
- Mytton, Julie, Jenny Ingram, Sarah Manns, and James Thomas. 2014. Facilitators and barriers to engagement in parenting programs: A qualitative systematic review. Health Education and Behavior 41: 127–37. [Google Scholar] [CrossRef] [PubMed]
- Nieuwboer, Christa C., Ruben G. Fukkink, and Jo M. A. Hermanns. 2013. Online programs as tools to improve parenting: A meta-analytic review. Children and Youth Services Review 35: 1823–29. [Google Scholar] [CrossRef] [Green Version]
- Nixon, Reginald D. V., Lynne Sweeney, Deborah B. Erickson, and Stephen W. Touyz. 2003. Parent-child interaction therapy: A comparison of standard and abbreviated treatments for oppositional defiant preschoolers. Journal of Consulting and Clinical Psychology 71: 251. [Google Scholar] [CrossRef] [Green Version]
- Nock, Matthew K., and Caitlin Ferriter. 2005. Parent management of attendance and adherence in child and adolescent therapy: A conceptual and empirical review. Clinical Child and Family Psychology Review 8: 149–66. [Google Scholar] [CrossRef] [PubMed]
- Pelham, William E., E. Michael Foster, and Jessica A. Robb. 2007. The economic impact of attention-deficit/hyperactivity disorder in children and adolescents. Journal of Pediatric Psychology 32: 711–27. [Google Scholar] [CrossRef] [PubMed]
- Porzig-Drummond, Renata, Richard J. Stevenson, and Caroline Stevenson. 2015. Preliminary evaluation of a self-directed video-based 1–2-3 Magic parenting program: A randomized controlled trial. Behaviour Research and Therapy 66: 32–42. [Google Scholar] [CrossRef]
- Rabbitt, Sarah M., Erin Carrubba, Bernadette Lecza, Emily McWhinney, Jennifer Pope, and Alan E. Kazdin. 2016. Reducing therapist contact in parenting programs: Evaluation of internet-based treatments for child conduct problems. Journal of Child and Family Studies 25: 2001–20. [Google Scholar] [CrossRef] [PubMed]
- Robinson, Elizabeth A., Sheila M. Eyberg, and A. William Ross. 1983. Conduct problem behavior: Standardization of a behavior rating scale with adolescents. Journal of Clinical Child Psychology 12: 347–54. [Google Scholar]
- Rosenthal, Robert. 1979. The file drawer problem and tolerance for null results. Psychological Bulletin 86: 638. [Google Scholar] [CrossRef]
- Sanders, Matthew R. 1999. Triple p-positive parenting program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavioral and emotional problems in children. Clinical Child and Family Psychology Review 2: 71–90. [Google Scholar] [CrossRef]
- Sanders, Matthew R., Danielle T. Montgomery, and Margaret L. Brechman-Toussaint. 2000. The mass media and the prevention of child behavior problems: The evaluation of a television series to promote positive outcomes for parents and their children. The Journal of Child Psychology and Psychiatry and Allied Disciplines 41: 939–48. [Google Scholar] [CrossRef]
- Sanders, Matthew, Rachel Calam, Marianne Durand, Tom Liversidge, and Sue Ann Carmont. 2008. Does self-directed and web-based support for parents enhance the effects of viewing a reality television series based on the Triple P–Positive Parenting Programme? Journal of Child Psychology and Psychiatry 49: 924–32. [Google Scholar] [CrossRef]
- Sanders, Matthew R., Sabine Baker, and Karen M.T. Turner. 2012. A randomized controlled trial evaluating the efficacy of Triple P Online with parents of children with early-onset conduct problems. Behaviour Research and Therapy 50: 675–84. [Google Scholar] [CrossRef]
- Sanders, Matthew R., Cassandra K. Dittman, Susan P. Farruggia, and Louise J. Keown. 2014. A comparison of online versus workbook delivery of a self-help positive parenting program. The Journal of Primary Prevention 35: 125–33. [Google Scholar] [CrossRef]
- Schueller, Stephen M., Kathryn Noth Tomasino, and David C. Mohr. 2017. Integrating human support into behavioral intervention technologies: The efficiency model of support. Clinical Psychology: Science and Practice 24: 27–45. [Google Scholar] [CrossRef]
- Serketich, Wendy J., and Jean E. Dumas. 1996. The effectiveness of behavioral parent training to modify antisocial behavior in children: A meta-analysis. Behavior Therapy 27: 171–86. [Google Scholar] [CrossRef]
- Sourander, Andre, Patrick J. McGrath, Terja Ristkari, Charles Cunningham, Jukka Huttunen, Patricia Lingley-Pottie, Susanna Hinkka-Yli-Salomäki, Malin Kinnunen, Jenni Vuorio, Atte Sinokki, and et al. 2016. Internet-assisted parent training intervention for disruptive behavior in 4-year-old children: A randomized clinical trial. JAMA Psychiatry 73: 378–87. [Google Scholar] [CrossRef] [PubMed]
- Spencer, Chelsea M., Glade L. Topham, and Erika L. King. 2019. Do online parenting programs create change? A meta-analysis. Journal of Family Psychology 34: 346. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, Laurence. 2007. Risk taking in adolescence: New perspectives from brain and behavioral science. Current Directions in Psychological Science 16: 55–59. [Google Scholar] [CrossRef]
- Sterne, Jonathan A. C., Alex J. Sutton, John P. A. Ioannidis, Norma Terrin, David R. Jones, Joseph Lau, James Carpenter, Gerta Rücker, Roger M. Harbord, Christopher H. Schmid, and et al. 2011. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 343: d4002. [Google Scholar] [CrossRef] [Green Version]
- Stormshak, Elizabeth A., John R. Seeley, Allison S. Caruthers, Lucia Cardenas, Kevin J. Moore, Milagra S. Tyler, Christopher M. Fleming, Jeff Gau, and Brian Danaher. 2019. Evaluating the efficacy of the Family Check-Up Online: A school-based, eHealth model for the prevention of problem behavior during the middle school years. Development and Psychopathology 31: 1873–86. [Google Scholar] [CrossRef]
- Tate, Robyn L., Michael Perdices, Ulrike Rosenkoetter, William Shadish, Sunita Vohra, David H. Barlow, Robert Horner, Alan Kazdin, Thomas Kratochwill, Skye McDonald, and et al. 2016. The Single-Case Reporting Guideline In BEhavioural Interventions (SCRIBE) 2016: Explanation and elaboration. Archives of Scientific Psychology 4: 10. [Google Scholar] [CrossRef] [Green Version]
- Thongseiratch, Therdpong, Patty Leijten, and G. J. Melendez-Torres. 2020. Online parent programs for children’s behavioral problems: A meta-analytic review. European Child and Adolescent 29: 1555–68. [Google Scholar] [CrossRef] [PubMed]
- Webster-Stratton, Carolyn, and M. Jamila Reid. 2003. The incredible years parents, teachers and children training series: A multifaceted treatment approach for young children with conduct problems. In Evidence-Based Psychotherapies for Children and Adolescents. Edited by Alan E. Kazdin and John R. Weisz. New York: The Guilford Press, pp. 224–40. [Google Scholar]
- Weisenmuller, Chantel, and Dane Hilton. 2020. Barriers to Access, Implementation, and Utilization of Parenting Interventions: Considerations for Research and Clinical Applications. American Psychologist 76: 104. [Google Scholar] [CrossRef]
- Wetterborg, Dan, Pia Enebrink, Kajsa Lönn Rhodin, Martin Forster, Ellen Risto, Johanna Dahlström, Kajsa Forsberg, and Ata Ghaderi. 2019. A pilot randomized controlled trial of Internet-delivered parent training for parents of teenagers. Journal of Family Psychology 33: 764–74. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, Mark L. 2002. NICHQ Vanderbilt Assessment Scale. Boston: National Institute for Children’s Health Quality; American Academy of Pediatrics and National Initiative for Children’s Healthcare Quality. [Google Scholar]
- Xie, Yuhuan, J. Faye Dixon, Ong Min Yee, Junshun Zhang, Y. Ann Chen, Sascha DeAngelo, Peter Yellowlees, Robert Hendren, and Julie B. Schweitzer. 2013. A study on the effectiveness of videoconferencing on teaching parent training skills to parents of children with ADHD. Telemedicine and e-Health 19: 192–99. [Google Scholar] [CrossRef] [PubMed]
- Zisser, Alison, and Sheila M. Eyberg. 2010. Parent-child interaction therapy and the treatment of disruptive behavior disorders. In Evidence-Based Psychotherapies for Children and Adolescents. Edited by John R. Weisz and Alan E. Kazdin. New York: Guilford Press, pp. 179–93. [Google Scholar]



| # | Authors (Date) | Age Range | % Male | RCT Conditions | n | Components | Follow-Up | Primary Outcome Measures | Effect Size (Pre-Post Intervention) | Methodological Quality Rating (Average Score) | BITs Level |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Baker et al. (2017) | 2–9 | 55 | Triple P-Positive Parenting Program (TPOL) Brief vs. WLC | 200 | TPOL Brief is a five-module interactive, self-directed computer program with video modeling and downloadable resources. | 9-month | ECBI, CAPES, PS, Behavior Concerns and Parent Confidence Scale, PCPTOS, PAI, PPC, DASS-2, CSQ | - | 20.5 | FAA-BIT |
| 2 | Breitenstein et al. (2016) | 2–5 | 43 | ezPARENT vs. Attention Control Condition (Health Promotion Group) | 79 | The ezPARENT program is a 12-week, six module self-administered, tablet-based application. It is an adaptation of the Chicago Parent Program. | 6-month | ECBI; TCQ; PQ; PSI-SF | ECBI Problem Scale: d = −0.18 | 20.5 | FAA-BIT |
| 3 | Cefai et al. (2010) | 9–15 | 50.86 | Individual Parenting Wisely CD-Rom vs. Group Parenting Wisely CD-Rom vs. WLC | 125 | One to three session self-administered individual intervention using the Parenting Wisely CD-Rom. The group condition completed Parenting Wisely program FTF as a group during two-sessions with clinician facilitated discussion. | 3-month | PSOC, ECBI | ECBI Problem Scale: Individual d = 0.45 Group d = 0.69 | 15 | FAA-BIT FTF with BITs as adjuncts |
| 4 | Comer et al. (2017) | 3–5 | 82.5 | Internet Parent-Child Interaction Training (iPCIT) vs. FTF PCIT | 40 | Video teleconferencing with a therapist who provides live coaching through a webcam and Bluetooth earpiece. On average, treatment length is 20 sessions and is titrated based on family needs. | 6-month | CBCL; ECBI; K-DBDs diagnostic interview; CGI-S/I; CGAS; BTPS; CSQ-8; TAI | ECBI Problem Scale: d = −1.15 CBCL Externalizing: d = −1.10 | 21 | Teletherapy |
| 5 | Dadds et al. (2019) Study 1: Urban Study 2: Rural | 3–9 3–14 | 79.7 79.6 | AccessEI vs. FTF BPT | 133 73 | AccessEI is an online intervention that includes six to 10 60- to 70-min video conferencing sessions with a clinician paired with six video modules (a total of one-hour and 14-min). FTF is an intensive PMT. In study one, FTF took place over one week (four 1.5-h sessions) with one follow-up call. In study 2, FTF took place in six-10 weekly 1-h sessions. | 3-month | CPRS-R; BSI; SDQ | Conners-Oppositional: η2 = 0.579 η2 = 0.569 | 20 | Teletherapy |
| 6 | Day and Sanders (2018) | 1–8 | 46.5 | TPOL vs. Telephone Supported TPOL (TPOLe) vs. WLC | 183 | TPOL is an eight module parenting intervention that utilizes video, interactive activities, and downloadable resources with optional text reminders. TPOLe included up to eight practitioner support sessions in which participants were able to ask questions, the practitioner reviewed module content and participant goals, and the practitioners created adherence plans if the participant was not engaging with the program. | 5-month | ECBI; PS; DASS; PTC; PPC; RQI; PAI | ECBI Problem Scale: WLC vs. TPOL d = 0.66 WLC vs. TPOLe d = 0.93 TPOL vs. TPOLe d = 0.26 | 21.5 | FAA-BIT BITs with Human Support |
| 7 | DuPaul et al. (2018) | 3–5 | 63.8 | Online BPT vs. FTF BPT vs. WLC | 47 | The online program was a 10 session internet intervention. The first session in the BIT BPT occurred in person, and parents received an overview of the program. The rest of the intervention was delivered online, and parents received weekly calls from research assistants to check on intervention implementation and answer any questions. FTF was a 10 session therapist led manualized BPT program. | - | CERS, PSI-SF, Test of Parent Knowledge | CERS Defiant/Aggressive: ηp2 = 0.07 | 19.5 | BITs with Human Support |
| 8 | Enebrink et al. (2012) | 3–13 | 57.7 | Internet Parent Management Training (PMT) vs. WLC | 104 | The internet-PMT is a seven-session program that is delivered online with feedback from research assistants. It is based off of the Swedish BPT program Comet (Kling et al. 2010). | 6-month | ECBI, SDQ, PPI | ECBI Problem Scale: d = 0.72 SDQ Conduct Problems: d = 0.30 | 21 | BITs with Human Support |
| 9 | Franke et al. (2016) | 3–4 | - | TPOL vs. Delayed Intervention | 53 | TPOL is a self-directed, eight module, internet positive parenting intervention. Participants received two telephone consultations with Triple P facilitators. | 6-month | EC-BEH; EC-BEH-s; CBS; SDQ; PS; PSDQ; DASS-21; PSOC; CSQ | EC-BEH Defiance/Aggression: d = 0.45 | 20.5 | BITs with Human Support |
| 10 | Ghaderi et al. (2018) | 10–13 | - | iComet vs. Family Check-Up (FCU) | 231 | iComet is a seven session parent training program delivered through a secure website. FCU is a parent training model that is catered to the parent’s needs. | 1-year 2-years | SDQ; DBD | SDQ Conduct Problems: d = 0.06 | 21 | FAA-BIT |
| 11 | Irvine et al. (2015) | 11–14 | 52.9 | Parenting Toolkit vs. WLC | 307 | Parenting Toolkit is a nine module online intervention completed entirely on the computer. | - | ECBI, Parenting Scale | ECBI Problem Scale: η2 = 0.009 | 19.5 | FAA-BIT |
| 12 | Jones et al. (2014) | 3–8 | 53 | Standard Helping the Noncompliant Child (HNC) vs. Technology Enhanced HNC (TE-HNC) | 15 | TE-HNC consists of eight to 12 standard, in-person sessions and access to a phone application with video examples, reminders, surveys, and home practice. | - | ECBI; consumer satisfaction scale | ECBI Problem Scale: d = 1.59 | 18.5 | FTF with BITs as Adjuncts |
| 13 | Morawska et al. (2014) | 2–10 | 61.9 | TPOL Podcast vs. WLC | 139 | The TPOL podcast consists of seven episodes that range from nine- to 14-minutes. These podcasts present parent training topics in a conversational manner. | 6-month | ECBI, CAPES, PS, PTC | ECBI Problem Scale: d = 0.39 | 17 | FAP-BIT |
| 14 | Nixon et al. (2003) | 3–5 | 70.4 | Modified Parent-Child Interaction Therapy (PCIT) vs. FTF PCIT vs. WLC | 54 | The modified PCIT condition included videotapes in which PCIT skills were discussed and modelled, along with five face-to-face sessions and five 30-minute telephone consultations. The standard condition included 12 one- to two-hour weekly PCIT sessions. | 6-month | ECBI; CBCL; HSQ-M; PSI; PSOC; PLOC; PS; DPICS-II | CBCL Externalizing: FTF PCIT vs. modified PCIT d = 0.01 Modified PCIT vs. WLC d = 0.59 | 17.5 | FTF with BITs as Adjuncts |
| 15 | Porzig-Drummond et al. (2015) | 2–10 | 50 | 1–2-3 Parenting vs. WLC | 84 | 1–2-3 Parenting is a self-directed, online parenting program where parents learn parenting strategies by watching two videos (totaling four hours) and receive email reminders to complete the lesson and practice. | 6-month | ECBI, PSI, DASS | ECBI Problem Scale: d = 0.70 | 21 | FAP-BIT |
| 16 | Rabbitt et al. (2016) | 6–13 | 67.5 | Full Contact Webcam PMT vs. Reduced Contact PMT | 60 | Full contact PMT included eight 50-minute teletherapy. Reduced contact PMT included 12 weekly prerecorded web sessions and 15- to 20-minute phone calls every 2 weeks with a therapist to address questions or concerns. | - | CBCL; IAB; CGAS; RDI | CBCL d = 0.79 | 18.5 | BITs with Human Support |
| 17 | Sanders et al. (2012) | 2–9 | 67.2 | TPOL vs. Internet As Usual Control Group | 116 | TPOL is an eight-module self-directed, interactive, internet intervention. It includes video modeling, personalized goal setting, content reviews and answer feedback, interactive exercises, downloadable worksheets and podcasts, and automated text and email prompts. | 6-month | ECBI, SDQ, PS, PTC, DASS-21, PAI, PPC, CSQ | ECBI Problem Scale: d = 0.71 SDQ Conduct: d = 0.58 | 18.5 | FAA-BIT |
| 18 | Sanders et al. (2008) | 2–9 | 64.9 | Driving Mum and Dad Mad with Triple P workbook and website vs. Driving Mum and Dad Mad | 174 | Driving Mum and Dad Mad is a six-episode show about parents with young children. The enhanced condition also included Triple P self-directed workbook, weekly emails on parenting topics, reminders, access tip sheets, videos, and the option to email for assistance. | 6-month | ECBI, PS, DASS1, PAI, PPC, RQI | ECBI Problem Scale d = 0.63 | 15 | FAP-BIT |
| 19 | Sanders et al. (2014) | 3–8 | 67 | TPOL vs. Self-Help Workbook | 193 | TPOL is an eight-module self-directed, interactive, internet intervention. It includes video modeling, personalized goal setting, content reviews and answer feedback, interactive exercises, downloadable worksheets and podcasts, and automated text and email prompts. The self-help workbook consists of the same core content as TPOL, but is delivered through a workbook divided into 10 weekly sessions with reading, activities, and homework tasks. | 6-month | ECBI, DASS-21, PSQ | Mother Report ECBI Problem d = 1.44 Father Report ECBI Problem d = 0.73 | 14 | FAA-BIT |
| 20 | Sanders et al. (2000) | 2–8 | 58.9 | Triple P Television Series Families vs. WLC | 56 | Families consists of 12 20- to 30-minute episodes which feature a story regarding family issues along with Triple P guidelines and instructions. Participants also had 12 written self-help Triple P information sheets. | 6-month | ECBI; PS; PSOC; DASS; PPC; AARP | ECBI Problem Scale: p = 0.09 | 17 | FAP-BIT |
| 21 | Sourander et al. (2016) | 4 | 61.9 | Strongest Families Smart Website (SFSW) vs. Education Control Group | 464 | SFSW is a 11 session internet-assisted BPT with weekly telephone coaching. Education control included access to a website on positive parenting strategies with 45-minute weekly coaching calls. | 12-month | CBCL; SDQ | CBCL Externalizing: d = 0.34 | 19 | BITs with Human Support |
| 22 | Stormshak et al. (2019) | 6th–7th grade students | 47.9 | FCU Online (FCU) vs. FCU Online Plus Coach vs. WLC | 322 | FCU online includes at least three online sessions and is adapted to fit participant needs and goals. In the online only version, feedback was provided online. In the online plus coach version, feedback was provided over the telephone or video-conferencing. | - | SDQ | SDQ Conduct Problems: WLC vs. web-only d = −0.13 WLC vs. web + coach d = −0.102 Web-only vs. web + coach d = 0.020 | 18 | FAA-BIT BITs with Human Support |
| 23 | Wetterborg et al. (2019) | 12–17 | 41 | Parent Web vs. WLC | 75 | Parent Web is a six- to nine-week parenting intervention delivered through the internet with five core modules and six optional modules. Each module has text, illustrations and movie clips. A practitioner provides reminders, feedback, and answers questions. | 6-month 9-month | DBD, SDQ, APQ, PSS, HADS | SDQ Conduct: d = 0.34 | 19.5 | BITs with Human Support |
| 24 | Xie et al. (2013) | 6–14 | 68.2 | Videoconference BPT vs. FTF BPT | 22 | Both groups received 10 weekly sessions manualized parent training; however, the videoconference group never met FTF. | - | Vanderbilt Assessment Scales, SSRS, PRQ-CA; CGAS; CGI-s; CGI-I | Vanderbilt Conduct p = 0.33 Vanderbilt ODD p = 0.66 | 18.5 | Teletherapy |
| Problem Behavior Outcomes | nobs | g | 95% Confidence Interval | Z | Test of Homogeneity | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Overall Effect | 28 | 0.62 | 0.42 | 0.81 | 6.14 ** | χ2 (27) = 188.81 ** |
| Subgroup: Treatment Type | ||||||
| Fully Automated Active BIT | 9 | 0.54 | 0.19 | 0.88 | 3.01 ** | χ2 (8) = 77.23 ** |
| Fully Automated Passive BIT | 4 | 0.71 | 0.36 | 1.06 | 3.97 ** | χ2 (3) = 8.38 ** |
| Supported BITs | 11 | 0.81 | 0.45 | 1.17 | 4.37 ** | χ2 (10) = 68.28 ** |
| Teletherapy | 4 | 0.19 | −0.25 | 0.64 | 0.85 | χ2 (3) = 10.72 |
| Subgroup χ2 (3) = 4.94, p = 0.18 (ns) | ||||||
| Problem Behavior Outcomes | nobs | g | 95% Confidence Interval | Z | Test of Homogeneity | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Overall Effect | 28 | 0.62 | 0.42 | 0.81 | 6.14 ** | χ2 (27) = 188.81 ** |
| Subgroup: Control Group Type | ||||||
| Active Control | 9 | 0.14 | −0.17 | 0.45 | 0.90 | χ2 (8) = 40.00 ** |
| Waitlist or Education Control | 19 | 0.82 | 0.61 | 1.03 | 7.68 ** | χ2 (18) = 94.80 ** |
| Subgroup χ2 (1) = 12.90, p = 0.000 (s) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bausback, K.B.; Bunge, E.L. Meta-Analysis of Parent Training Programs Utilizing Behavior Intervention Technologies. Soc. Sci. 2021, 10, 367. https://doi.org/10.3390/socsci10100367
Bausback KB, Bunge EL. Meta-Analysis of Parent Training Programs Utilizing Behavior Intervention Technologies. Social Sciences. 2021; 10(10):367. https://doi.org/10.3390/socsci10100367
Chicago/Turabian StyleBausback, Kimberly B., and Eduardo L. Bunge. 2021. "Meta-Analysis of Parent Training Programs Utilizing Behavior Intervention Technologies" Social Sciences 10, no. 10: 367. https://doi.org/10.3390/socsci10100367