1. Introduction
Construction work, albeit a vital source of employment worldwide, is known to cause significant psychological distress—general signs of stress, fatigue, anxiety, anger, and moodiness, etc.—and consequently, poor mental health among many young workers [
1,
2]. It has been identified in Australia, for example, that although construction workers, in general, have a higher suicide risk as compared to the general male population, young construction workers aged 15 to 24 years have an unusually high suicide risk (about twice that of young workers in other industries) [
3]. There is also a very high prevalence of harmful substance use among young construction workers compared with other categories of young workers [
4]. These problems have been attributed to the direct and indirect effects of young workers’ exposure to psychosocial risk factors (PRFs), both within and outside the construction environment [
5,
6]. PRFs broadly refer to a combination of psychological and social “attributes, characteristics or exposures” that interact to make it more likely for a person to develop a mental health problem or illness [
7]. In the context of the construction industry, PRFs have often been associated with stressful workplace conditions that interact through a person’s experience and perceptions to affect their work output, job satisfaction, and eventually their mental well-being [
8].
Although the broader construction mental health literature is still emerging, a wide range of PRFs, such as existing chronic diseases [
9,
10], young age [
11,
12], weak family support [
13,
14], long working hours [
15], and other industry related risks [
16,
17,
18], have been explored. The extant research, although providing vital insights, such as highlighting the strong connection between PRFs and poor mental health, remains largely fragmented. Additionally, a comprehensive review of the literature on the PRFs specific to young construction workers is still lacking, with the few reviews available (e.g., [
19,
20]) focusing on the case of the general construction workforce. As a result, issues such as the relationships between different PRFs, as well as how they influence psychological distress and poor mental health among young construction workers, are yet to be fully understood. This has posed challenges in developing appropriate mental health interventions for young workers. Furthermore, the limitations of the current literature are yet to be identified to provide directions for future research on the topic. Therefore, we sought to undertake a comprehensive literature review with the objective of answering the following questions:
- (1)
what are the domains of psychosocial risk factors that affect young construction workers’ mental health?
- (2)
what is the relationship between the domains of psychosocial risk factors, psychological distress, and poor mental health in young construction workers?
The outcome of this review has the potential to provide researchers and practitioners with an in-depth understanding of the specific PRFs to which young construction workers are exposed to and inform strategic decisions about the management of young workers’ mental health and safety in the construction industry. Furthermore, this review can provide directions for future research.
2. Methods and Materials
The primary objective of the review was to identify and synthesize categories of a certain phenomena (PRFs and mental health). Accordingly, the first research question was developed in line with the PICo framework, i.e., Population (young workers); Phenomena of Interest (domains of PRFs and mental health); Context (construction) [
21,
22]. The secondary objective of the review was to determine the association between particular independent variables (PRFs) and dependent variables or outcomes (psychological distress and poor mental health). The second research question was, thus, framed in line with the PEO framework, i.e., Population (young construction workers); Exposure (domains of PRFs); Outcomes (psychological distress and poor mental health) [
23].
The PICo and PEO frameworks also helped to determine the types of keywords that were used in the literature search (see
Section 2.1), the formulation of inclusion criteria for retrieved articles (see
Section 2.2), and the approach to data analysis (see
Section 2.3). In line with the research questions of this review, data synthesis using meta-aggregation (narratives, tables, and visuals) [
21,
23] was preferred to a meta-analysis. This was primarily because our review did not seek to statistically explore the effects associated with PRFs, nor to estimate path coefficients between independent and dependent variables. Furthermore, the significant variations in the characteristics of the included studies (i.e., specific samples, contexts, outcomes, and methodologies) violated the condition of “heterogeneity”, thus making the use of meta-analysis inappropriate [
23,
24].
After the analysis, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) approach [
25] was chosen as the framework for reporting of the results.
2.1. Search Terms and Strategies
The electronic databases that were searched include Scopus, ISI Web of Science (WoS), PubMed, CINDAHL, and Google Scholar. We also searched a range of occupational health websites to obtain information on the topic. These included websites for the Australian Institute for Suicide Research and Prevention (AISRAP), Mates in Construction, and the Victorian Health Promotion Foundation. We did not limit the search to any time period. Searching multiple sources increased the chance of obtaining sufficient publications of good quality within the scope of the review topic.
The databases were searched using specific keywords (used individually or combined as search strings) that reflected the components of the PICo and PEO frameworks viz.:
Population: “construction professional*”, “construction labo*”, “construction workforce*”, “construction staff”, “construction personnel*”, “young construction”, “youth”.
Phenomena of interest: “mental health”, “psychiatr*”, “psychosocial*”, “coping*”, “psychological health”.
Context: “construction industry”, “construction sector”.
Exposure: “construction work*”, “construction activit*”, “stress*”.
Outcomes: “psychological well-being”, “psychological ill*”, “psychological disorder*”, “psychological injur*”, “anxiety”, “depress*”, “distress*”.
This search strategy was augmented by a cursory check of the references section of articles to identify additional records that could be of relevance but had not been captured within the scope of the initial search. Through this, additional research articles were obtained directly from their authors. The systematic search yielded a total of 235 articles.
2.2. Eligibility Criteria and Final Article Selection
After the comprehensive literature search, we developed criteria to only include articles most relevant to this review. We were particularly interested in articles that had been published in English and met two main criteria. First, studies had to be exclusively focused on young construction workers (i.e., those aged 35 years or younger). Otherwise, study results had to be stratified according to different age groups or report a sample mean age of 35 years or less. Second, the PRFs reported in a study had to be associated with mental health (e.g., general psychological distress and mental disorders such as depression, anxiety, etc.) and/or workers’ positive mental health (e.g., wellbeing, resilience, etc.).
We screened each article’s title, abstract, and keywords to identify those that were relevant for the review. A total of 192 articles (i.e.,
n = 48 duplicates and
n = 144 found to be irrelevant to the study) were removed in the screening process. Those that met the pre-determined criteria were retained for a further assessment of eligibility. Next, we examined the full texts of each of the retained articles. Studies that focused mainly on general physical health (ergonomic risks, chemical hazards, etc.) (
n = 1) were excluded. Studies with a sample mean age above 35, as well as those that had not categorized results by age groups (
n = 11), were also excluded. A final verification of the quality and eligibility of the articles for inclusion in the review was done based on the consensus of all the research team members. Overall, 31 articles were finally retained for the review (included in the references section of this paper and details provided in
supplementary material). The sample size (
n = 31) is well above what has been used in published systematic reviews on different issues associated with young construction workers’ mental health ([
26]:
n = 22,
n = 21,
n = 4; [
27]:
n = 24). Therefore, it is adequate for informing a thorough review of the research topic. A flowchart of the literature search and selection strategy employed is shown in
Figure 1.
2.3. Data Analysis
The study results were synthesized through meta-aggregation [
21]. Synthesized findings obtained through meta-aggregation are only an amalgamation of findings (presented as overarching statements, categories, or themes) from all of the studies included in a review [
28], and not a “re-interpretation” or “re-conceptualization” of extant evidence [
29].
First, we extracted information to provide an overview of each article. Information extracted included author names and background, year of publication, and country of origin, as well as the focus, purpose of the study, setting of the study, sample details, study design, and key findings (
Supplementary Material). The second step involved getting a detailed picture of the study contents. We read each article multiple times to get a clearer and overall picture of what it contained. Each study was assigned a unique code to enhance tracking and analysis. Next, using the overview information (e.g., country of focus and key findings), we identified initial categories of PRFs that formed the basis on which study data were extracted and summarized. Fifty different initial categories were identified.
The next stage involved developing themes (i.e., the central ideas) under which to group the initial categories. This was done through thematic content analysis [
30]. We deductively developed a provisional list of 47 themes using keywords that reflected the identified categories and specific terminology from research articles. We refined the list by retaining unique themes and merging similar ones. This resulted in a reduction of the themes to 30. Subsequently, we undertook a categorization of the 30 themes, leading to the creation of ten domains of PRFs. The 10 domains were further classified into personal, socio-economic, and organizational/industrial factors. A final revision and validation of the appropriateness of domains, themes, and their respective categories was done through consensus among the research team. Next, we examined the interactions among the different PRF domains through inductive reasoning [
31]. Inductive analysis was undertaken by observing the relationships among the different PRFs to identify emergent interactions. Next, a cross-comparison of the observed interactions was done to identify their differences and similarities. Subsequently, each interaction was refined to ensure that they were distinct from the other. Each interaction was then supported with illustrative quotes from the research articles.
A further abstraction of the identified interactions was undertaken to specify propositions on the patterns of influence of the different PRFs on poor mental health. The final stage involved reporting the data from individual studies under each domain and its associated themes. This involved extracting, summarizing, and associating each relevant sentence and idea with a corresponding theme and component.
3. Results
3.1. Overview of the Selected Articles
The 31 studies were either published as peer reviewed journal articles (n = 26: 83.9%) or industry reports (n = 5: 16.1%). Only nine articles (29%) had focused exclusively on young construction workers. The studies were conducted between 1993 and 2020.
The majority (n = 14: 45.2%) of the articles focused on the Australian construction industry. This was followed by three studies (9.7%) each from the UK and the US. Two studies (6.5%) focused on China and Pakistan. One study (3.2%) each examined the cases of South Africa, Nepal, India, Canada, Hong-Kong, and Germany. The remaining studies (3.2%) had a global focus. In terms of the authors’ academic background, the majority of the studies (n = 18: 58%) were conducted by authors solely from health-related disciplines (e.g., medicine, psychology, etc.). Ten studies (32.3%) were from authors with a built environment background (civil engineering, construction management, etc.), while one study (3.2%) was a collaboration between authors from social sciences and a built environment. Of the remaining two studies, one each (3.2%) was from business management and social sciences.
With respect to gender, almost half of the studies (n = 15: 48.4%) gave attention to both male and female workers. However, in all cases, males formed an overwhelming majority of respondents. Twelve studies (38.7%) focused exclusively on male construction workers, whereas only one study (3.2%) focused on females only. Three studies (9.7%) did not state the gender of the respondents. In terms of occupational background, most of the studies (n = 25: 80.65%) focused on site-based, blue-collar construction workers (e.g., bricklayers, masons, and apprentices), whereas only three studies (9.7%) looked at the case of construction professionals (architects, civil engineers, construction managers, etc.). The three remaining studies (9.7%) examined the case of both blue-collar and professional workers. In terms of the cultural background of the respondents/sample, only three studies (9.7%) specifically focused on migrant workers from the Global South.
The majority of the studies (n = 27: 87%) were cross-sectional in nature, with the methodology employed in the different studies being largely determined by the specific research objectives. Most of the studies employed a quantitative approach (n = 19: 61.3%), with qualitative methodologies being used in only five studies (12.5%) and a mixed methods approach used in six studies (16.7%). The remaining two studies (8.3%) were systematic literature reviews.
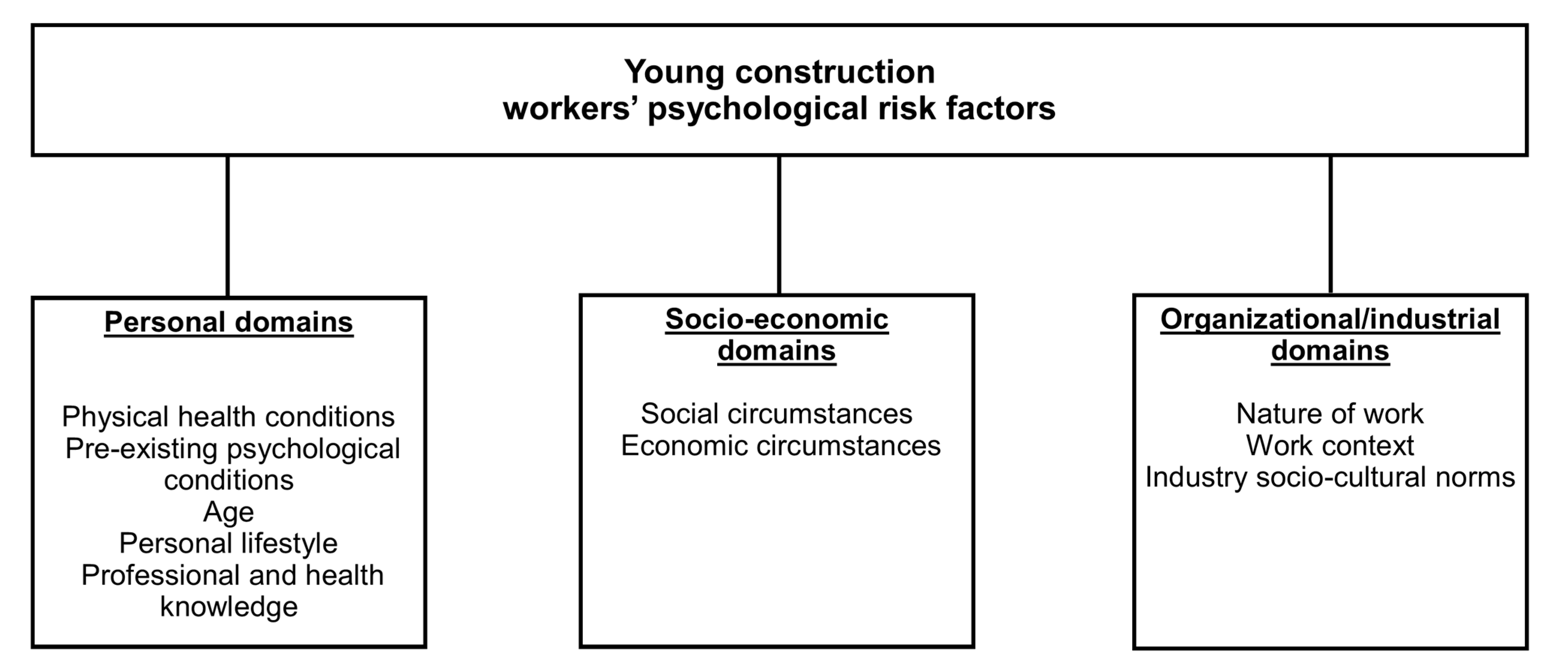
3.2. Domains of Young Construction Workers’ PRFs
A total of 10 domains of PRFs were derived from the included studies (
Figure 2). These domains, altogether, account for 30 individual PRFs common to young construction workers. The frequencies, as shown in
Table 1, indicate the total number of studies that reported the individual PRFs in each domain. The frequencies were used to rank each domain according to how often they were identified in the included studies.
4. Discussion
We present the ten PRF domains as personal (
Table 2), socio-economic (
Table 3), and organizational/industrial (
Table 4) factors. Personal PRFs are individual-level risk factors that mainly stem from a worker’s personal attributes or lifestyle [
32,
33]. Socio-economic PRFs are those associated with a worker’s “social relationship” [
20], such as family and the wider social community [
33], as well as the economic environment. Organizational/industrial PRFs originate from a task or a person’s work or industrial environment [
8,
34].
4.1. Personal Psychosocial Risk Factors
Five personal PRF domains were identified. These are physical health conditions, pre-existing psychological conditions, age, personal lifestyle, and professional and health knowledge. A total of ten risk factors were captured under the five domains.
4.1.1. Domain 1: Physical Health Conditions
The physical health conditions identified were both poor general physical health (e.g., chronic diseases) and pre-existing injuries (e.g., workplace injury). Poor general physical health has been observed as an underlying cause of high levels of psychosocial distress and, consequently, a host of secondary psychological problems that are strongly linked with mortality among young construction workers [
35]. Poor general physical health is usually manifested as “chronic illness” and has been noted as a common PRF among male construction workers in countries such as Australia [
36], China [
13], and Pakistan [
8]. The young workers’ need to deal with poor general physical health has been identified as having a strong link with maladaptive coping practices such as the illicit use of cannabis and cocaine. This has, in turn, been linked strongly with significant mental health problems (e.g., addiction disorders) among young male construction workers in Australia [
35].
In terms of pre-existing injuries, although general injuries have been examined, most research has focused on work-related injuries, specifically, musculoskeletal disorders (MSDs) among young male manual workers [
9,
37], with research on the link between general bodily injuries and mental health being scarce. The literature shows that young, male, blue-collar construction workers who sustain work-related injuries have poor long-term mental health outcomes. In the US, for example, young workers who suffered major MSDs (e.g., broken bones, pain, etc.) had poorer mental health [
9]. Among this group, those who were absent from work for a significant period due to prior major MSDs suffered much higher levels of depression and emotional problems (e.g., “feeling calm and peaceful”) than workers with no record of occupational injuries. The specific location of MSDs can also determine their impact on workers’ mental health. Among young masonry apprentices in the US, for example, work-related MSDs that caused pain in the upper body and knees resulted in poorer mental health, while workers without pain in these areas had better mental health [
37].
Whether anticipated or experienced, bodily pains from MSDs have two main linkages (i.e., direct and indirect) with young construction workers’ mental health [
6]. In the first instance, pain from MSDs can directly result in reduced mental health. In the second, MSD-related pain can be the basis of several stressors for workers, leading to poor mental health. Specifically, poor mental health manifests as a secondary psychological injury that results from MSDs. This occurs as a result of stresses related to concerns about the pressure to work despite pain, “feeling trapped in a job that causes pain and distress” without alternative employment, preventing further injury, staying fit for work, and future planning [
6].
4.1.2. Domain 2: Pre-Existing Psychological Conditions
This domain focuses on psychological conditions, both diagnosed and undiagnosed, that workers had before taking up construction employment. A study by the Australian Institute of Suicide Research and Prevention [AISRAP] [
38] that focused on young construction workers above 14 years of age observed pre-existing depression as a direct predisposing risk factor for suicide among the study population. The majority (90.9%) of the sample for the study was between the ages of 15 to 24 years, and the suicide rate for this group was unusually high (58.6 deaths per 100,000 population)—a number twice above the suicide rate for working-aged males in Australia. The high rate of suicide was also observed to have a link with a past history of attempted suicide. More recently, a study [
36] that examined the work and non-work-related influences on suicide among male construction workers in Australia reported similar findings. This study specifically identified that 64.7% of the sample with a high suicide rate had pre-existing depression. Additionally, 11.76% of the sample had a pre-existing diagnosis of schizophrenia and attention deficit disorder, while 5.88% had bipolar disorder, and one unspecified mental illness. Other studies have reported post-traumatic stress disorder (PTSD) as a major predisposing factor for psychological distress, and an accordingly high suicide rate among on-site male construction workers in China [
39].
4.1.3. Domain 3: Age
Past studies (e.g., [
11,
40]) have confirmed age as a critical determinant of the “strain effects of occupational stress” on young construction workers. In one dimension, age, as a personal PRF, has been reported as a mediating variable between the influence of the workplace environment PRFs on poor mental health. [
4] and [
35], for example, have confirmed age to be a key predictor of substance abuse—as influenced by the workplace norms—among young construction workers in Australia, with age having a negative correlation with significant use of illicit drugs and alcohol. In most cases, however, age has been identified as a moderator of the influence of socio-economic and organizational/industrial PRFs on psychological distress and poor mental health [
11]. For instance, it was reported that younger construction professionals in South Africa who experienced high job demands and poor support at work were more likely to experience high levels of psychological distress and, thus, poor mental health. This was because of the need they felt to “prove themselves” and their uncertainties in relation to their organizational role, place, and available support.
Being young increases a worker’s susceptibility to exposure and harm from other major risk factors such as PTSD [
39], bullying [
12], and illicit drug use [
38]. In line with this, workers between the ages of 15 to 24 years have been identified as having an elevated risk of suicide as an outcome of poor mental health [
38]. Furthermore, it has been found, for instance, that being young is enough to determine whether or not a worker will be bullied at the workplace [
12]. For example, it has been reported that workers between the ages of 18 and 25 years are the most likely to be bullied, whereas those under 17 years of age are the least likely to be bullied.
Age also has a bearing on a worker’s decision authority, which in turn directly affects job satisfaction, a key determinant of mental health [
18]. Through an examination of the interaction between age, decision authority, and mental health among construction workers in the US [
18], it was found that, although age was not significantly correlated with job satisfaction or mental health, it affected the relationship between job satisfaction and decision authority, such that decision authority was more positively related to job satisfaction for older construction workers than younger ones. This meant that younger workers had less decision authority and, thus, less job satisfaction, which is a strong predictor of poor mental health.
4.1.4. Domain 4: Personal Lifestyle
The main components of this domain are substance use and practicing an alternative lifestyle. An Australian study found substance abuse to be a common lifestyle among young construction workers, with about a quarter of the sample being described as “regular users” of alcohol and illicit drugs [
38]. Pidd et al. [
4] have examined the relationship between alcohol and drug use and psychological well-being among young apprentices in their first year of training in the Australian construction industry. The mean score reported for psychological distress (
M = 17.04) was considerably higher than the national score (
M = 14.9) for Australians of a similar age and gender. Moreover, Pidd et al. [
4] found the use of drugs such as cannabis (44.4% prevalence) and methamphetamine (8.3% prevalence) in the 12 months preceding the study to be significantly above the national prevalence (25.3% for cannabis; 3.3% for methamphetamine). The practice of alternative lifestyles is also beginning to receive attention as a PRF in the literature. Similar to the effect of age, practicing an alternative lifestyle puts young people at a higher risk of exposure to other major psychosocial risk factors. For example, a previous study [
12] has identified that young people who were homosexuals were more likely to face aggressive forms of bullying than those who were not.
Despite being intrinsic, workers’ personal lifestyle has a strong connection with their socio-cultural background, with the literature suggesting a complex relationship between the two. Closely related to this is the effect of construction industry socio-cultural norms (see
Section 4.3.3). In a study that explored the health, beliefs and behaviors that promote alcohol use among young Irish construction workers in London [
41], it was identified that the habit of excessive alcohol drinking was culturally acceptable as part of the Irish lifestyle. This cultural norm was exhibited in four main dimensions—approval of alcohol as a facilitator of social engagement; approval of an alcoholic sub-culture among Irish construction workers; approval of excessive drinking as a demonstration of masculinity; and the use of alcohol as the main coping mechanism among young people dealing with institutional and family abuse. Thus, while young construction workers from Irish backgrounds were fully aware of the potential of alcoholism to cause mental ill-health and suicide, their abuse of alcohol was driven by “the experience of being Irish in London” [
51].
4.1.5. Domain 5: Professional and Health Knowledge
Themes in this domain include low “educational attainment”, having no prior knowledge of the construction environment [
43], and a low level of professional skills [
10,
17]. In terms of educational achievements, studies have shown that young workers with low levels of education tend to have high levels of psychological distress and are more susceptible to self-harm and suicide. This is because of underlying outcomes of lack of education such as poor mental health literacy [
42] and low socio-economic status [
17]. A lack of prior knowledge of the construction environment/work conditions has also been reported to impact young workers’ mental health. Henry et al. [
43] identified that having little to no knowledge of the realities of construction work causes many young workers considerable psychological distress, both before and after taking up construction employment. This is because young workers who do not know what to expect from their work find it difficult to adjust to unexpected work conditions, and sometimes tend to be ignorant or ill-informed about the workplace mental well-being support services available to them. In another dimension, young workers with a low level of professional skills have been found to experience poor mental health, whereas highly skilled construction professionals (e.g., architects, engineers, etc.) tend to have better mental health outcomes [
10,
17].
4.2. Socio-Economic Psychosocial Risk Factors
We identified two socio-economic PRF domains. These include social circumstances and economic circumstances. A total of seven themes of risk factors were captured under the two domains.
4.2.1. Domain 6: Social Circumstances
The themes in this domain are non-work-related and focus on family issues that precipitate poor mental health. Within the broader literature, this domain refers to when family issues interfere with work. In this domain, the issue of relationship/family breakdown has often been mentioned. Past studies of young construction workers in Australia (e.g., [
36,
38]) have reported that workers who experienced a breakdown of relationships in the form of legal separation, divorce, and child custody problems had higher levels of psychological distress and adverse mental health outcomes such as suicide. For example, 75% of the sample—young male suicide victims—in a previous study [
38] had a higher risk of separation or divorce compared with other male suicide victims. They had also experienced relationship problems within three months before their death. These findings are somewhat supported by the fact that a stable marriage has been reported as a protective factor against poor mental health among migrant workers in the Chinese construction industry [
13].
Within this domain, only one study had been conducted on females [
14]. This study explored the relationship between work and family circumstances (i.e., caring for family, spousal support, stress mitigation approaches, and mental health) amongst low-income working mothers living in urban slums across Bangalore, India. It was reported that issues such as having an alcoholic and/or abusive husband, intimate partner violence, raising special needs children, and lack of adequate childcare support were critical PRFs for severe and prolonged depression and suicide attempts. Additionally, concerns about the welfare of pre-school kids and the absence of spousal support were key PRFs for anxiety.
Despite the lack of literature on the construction context, the broader literature provides support for the critical nature of family circumstances as a PRF for poor mental health. Different studies (e.g., [
52,
53,
54]) have indicated that a challenging family environment accounts for mental illness among more than 200 million children below five years of age, and this has been linked with problems such as poor brain development, weak social attachment, substance abuse [
55], and teenage pregnancy [
56], all of which, directly and indirectly, contribute to adverse mental health outcomes in the adult years.
4.2.2. Domain 7: Economic Circumstances
Included in this domain are both work and non-work-related risks such as poor personal and family financial security, lack of adequate employment opportunities leading to long periods of unemployment, and poor home support for personal care, training, and education. These conditions have been linked with high levels of psychological distress among young workers and, consequently, severe depression [
12], substance abuse, and suicide [
57,
58]. In the case of adequate employment, it has been reported that young construction workers who are unemployed for long periods due to living in a challenging economic environment, as well as those partially employed, suffer higher levels of bullying and anxiety [
12].
Poor personal and family finances have been found to act together to influence psychological distress and poor mental health in young construction workers. This is because workers with poor finances, often as a result of low wages, face difficulties providing financial support for their families, and families with poor finances have difficulty providing financial support for young workers [
12,
14]. In a study of remote male construction workers in Australia, the majority (62.3%) of the samples were constantly worried about their low wages, making them six times more likely to have very high scores for self-reported poor mental health [
44].
This outcome is not only limited to remote construction workers, but is also common among the general male construction workforce, many of whom are known to suffer the direct impacts of work and home-related financial instability [
38]. In India, for example, young female construction workers who are mothers with low-income backgrounds and experience declining access to support from their extended family have been identified to have high psychological distress as a result of constantly worrying about how to cater for their children’s safety, nutrition, and education [
14]. Thus, this group suffers significant levels of anxiety disorder, depression, and suicidal ideation [
14]. Apart from support for personal care, workers who have weak or no support—from their families or elsewhere—for their academic or occupational training tend to have an elevated risk of high psychological distress, bullying, and suicide [
12].
4.3. Organizational/Industrial Psychosocial Risk Factors
We identified three organizational/industrial PRF domains. These include the nature of work, work context, and industry socio-cultural norms. A total of 13 themes of risk factors were captured under the three domains.
4.3.1. Domain 8: Nature of Work
This domain includes key themes directly related to the characteristics associated with the actual construction tasks undertaken by a worker. They include long working hours [
15], low job control (having no say in how work is structured, i.e., how much work is assigned to a person, how work is executed, the amount of time allocated for tasks, etc.), and tasks that demand “higher psychological” effort [
26]. When young workers undertake tasks that require the use of new technology [
16], specialized knowledge, the provision of consultation, and adapting to constant changes in project conditions and project team members, they are often subjected to high cognitive demands related to being reliable, friendly, assertive, and constantly motivated [
45]. A study of young workers in small German construction firms revealed that high cognitive demand tasks in particular impose a “multi-component strain”, which has a direct impact on the mental health of young construction workers [
45]. Studies from Australia have shown that young workers who are mostly employed in manual occupations are more prone to suicide, whereas those with managerial roles tend to have better mental health [
10,
17]. High work demands, both cognitive and physical, underpinned by the strict timelines typical of construction industry work, cause poor prioritization and utilization of social support and interactions, both at home and at the workplace, thus resulting in a stressful work life for young construction workers, especially those below 30 years of age [
3,
36,
38].
Past studies on young construction managers in the UK have reported the problem of time-pressure overspill into home and the leisure environment [
16]. In terms of work-home interference, a study of the “work-home interface” and family separation among fly-in-fly-out (FIFO) and drive-in-drive-out (DIDO) workers indicated that young FIFO and DIDO workers who were parents reported that separation from their families due to work pressure led to low relationship quality with family and friends, causing them significant psychological distress [
43]. This outcome was significantly lower in the case of those who were not parents. Other workers also reported that the adjustment to long day and night shifts caused sleep disorders and fatigue, which led to significant stress levels. This is similar to the finding that sleep status is a key PRF among migrant workers in China’s construction industry [
13].
4.3.2. Domain 9: Work Context
Work context refers to the features of the work environment within which construction work is undertaken or where workers find themselves. As such, themes in this domain focus on the primary-level (rather than industry) circumstances within which construction work is undertaken. Specific themes include the nature of relationship/interaction between young workers and others (e.g., employers, supervisors, peers, clients, etc.) [
27,
47]. It is common for young workers to have poor relationships with colleagues and superiors, leading to harassment and mostly verbal bullying. Studies from Australia, for example, have reported that many supervisors are aggressive, impatient, and not willing to be questioned by young workers [
38,
42]. Additionally, older workers are less tolerant of young workers’ circumstances and tend to condone their bullying. In spite of these problems being rampant, young workers hardly complain or discuss it with others because of the fear of losing work [
27,
38]. They are also apprehensive about changing jobs due to fear of encountering harsh supervisors elsewhere.
Young workers also experience mental health stigma at work [
44]. The impact of stigmatization on young workers includes the reluctance to go to work, low self-esteem, sleep disorders, psychological distress, panic attacks, anxiety disorder, feelings of isolation, poor concentration and decision-making ability, depression, and suicidal ideation [
27,
38]. In particular, periods of high suicide among young workers coincided with a high prevalence of intense stress, low construction activity, and an increase in the number of lost working days, all of which were strongly connected with workplace disputes arising from poor relationships [
3].
Other themes associated with the physical work environment include unsuitable on-site accommodation and living conditions [
46], as well as the presence of and exposure to on-site physical hazards [
43]. These stressors, whether perceived or real, have a link with the safety climate and have been identified in the Canadian [
46] and Nepalese [
40] construction industries as having a strong correlation with job stress and poor mental health experienced by young workers. In Nepal, for example, workers who perceived their work environment to pose any health risks were three times more likely to experience mental health problems than those who did not [
40]. Other studies (e.g., [
12,
39]) have indicated that working in a poor physical construction environment can increase young workers’ susceptibility to significant psychosocial hazards, such as the exposure to victims of attempted suicide or even witnessing suicide and the serious injuries of other workers. Other issues such as political instability and “wars and natural disasters” have been noted to demoralize young workers, bringing them considerable psychological stress because of the potential of these problems to cause the complete abandonment of work and adversely affect young workers’ employment and long-term career progression [
8].
The final theme—organizational management conditions—focuses on organizational-level management issues that affect how work is undertaken. These include poor job security, poor human resource management practices, and workplace discrimination. The project-based nature of construction work, for instance, means that many organizations are unable to guarantee job security for their employees [
59]. Therefore, for young construction employees, there is a constant threat of unemployment and subjection to poor organizational human resource management practices, and these issues cause much stress and anxiety [
11,
26,
36,
38,
48]. This is especially true in the case of young workers who lack knowledge and experience of typical construction project conditions [
43]. Studies specific to the Global South have identified additional organizational conditions such as workplace discrimination, wrong perceptions of organizational expectations [
11] (South Africa), and “career development-related psychosocial factors” including the absence of organizational-level training programs and lack of opportunities for “career mentoring” [
8] (Pakistan).
In another dimension, literature is emerging on the impact of organizational conditions in academic institutions on the psychological condition of construction students because they are also considered to be young construction workers [
60]. Attention has, for instance, been given to the psychological stressors affecting graduate construction students in Australian universities [
49]. It was reported that the pressure from the high academic standards of universities caused students to have “high self-expectations” and to constantly worry about the possibility of poor academic performance. Studies of this nature are not available in the case of the Global South.
4.3.3. Domain 10: Industry Socio-Cultural Norms
This domain includes themes which focus on cultural norms within the industry at large [
42]. Research on the effects of “school-to-work transition” and industry culture, e.g., [
4,
61], indicates that the cultural theme of masculinity and domination by superiors plays a critical role in young apprentices’ patterns of psychosocial distress. The culture of domination encourages workplace bullying and the harassment of young workers [
18]. The prevalence of bullying has been estimated to be about 15% globally and an average of 10% in Australia, rising sharply to 56% in the case of FIFO workers [
27]. The pressure to demonstrate masculinity can make young workers, especially new entrants, resort to the frequent use of illicit drugs [
4].
The abuse of substances is fueled by the construction industry’s culture of open support for substance use as a coping mechanism. Illicit drugs are unfortunately readily available in many construction environments. For example, many young male construction workers in Australia abuse cocaine because of the issue of “workplace availability” [
35]. Alcohol and substance misuse have also been described as an accepted industry “coping behavior” for work pressure [
41,
50]. Reports from psychological autopsies have confirmed that problems related to alcohol use often precede suicide among young workers, especially apprentices [
35].
It can be inferred from the broader mental health literature, especially on the Global South, that a wide range of industry norms may derive from the cultural norms of the wider social environment [
62]. For instance, there is generally a cultural tolerance of physical abuse—a strong contributor to poor mental health—which stems from a misguided sense of appropriate discipline for young people [
63]. In a study of 28 Global South countries [
64], about 83% of the sample (children with mental health problems) had experienced some form of psychological abuse. Additionally, 64% of the sample had experienced a combination of psychological and moderate physical abuse, while 43% had experienced extreme psychological and physical abuse.
4.4. Interactions between the Domains of PRFs and Their Relationship with Poor Mental Health
We examined the interactions between the domains of the PRFs and their relationships with poor mental health. In doing this, we were guided by transaction theory, which indicates that stress emanates from the interaction between environmental and personal factors [
65]. Four key interactions between the domains of PRFs (personal, socio-economic, and organizational/industrial) and their relationships with psychological distress that leads to poor mental health were identified.
Table 5 shows the identified relationships, examples of their supporting quotes, and their respective literature sources.
A conceptual model that shows how the PRF domains influence poor mental health was proposed based on the identified relationships (
Figure 3). Fifteen propositions were derived based on the conceptual framework viz.:
Proposition 1a. Socio-economic risk factors have a direct influence on poor mental health.
Proposition 1b. Socio-economic risk factors have a direct influence on psychological distress.
Proposition 1c. Socio-economic risk factors have a direct influence on personal risk factors.
Proposition 2a. Organizational/industrial risk factors have a direct influence on poor mental health.
Proposition 2b. Organizational/industrial risk factors have a direct influence on psychological distress.
Proposition 2c. Organizational/industrial risk factors have a direct influence on personal risk factors.
Proposition 3a. The influence of socio-economic and organizational/industrial risk factors on psychological distress is mediated by personal risk factors.
Proposition 3b. The influence of socio-economic and organizational/industrial risk factors on poor mental health is mediated by personal risk factors.
Proposition 4. The influence of socio-economic, personal, and organizational/industrial risk factors on poor mental health is mediated by psychological distress.
Proposition 5a. Age moderates the influence of socio-economic risk factors on psychological distress.
Proposition 5b. Age moderates the influence of socio-economic risk factors on personal risk factors.
Proposition 5c. Age moderates the influence of organizational/industrial factors on psychological distress.
Proposition 5d. Age moderates the influence of organizational/industrial factors on personal risk factors.
Proposition 5e. Age moderates the influence of socio-economic risk factors on poor mental health.
Proposition 5f. Age moderates the influence of organizational/industrial factors on poor mental health.
4.5. Future Research Directions
The current review has four main implications for future research. First and foremost is the need to give attention to the issue of positive mental health. The ten PRF domains and the 30 associated themes indicate that most of the studies reviewed framed mental health using a “disease-based model” [
66]. This predominant focus on the “symptomology of poor mental health” has, to a large extent, obscured an understanding of positive mental health and how it can be achieved by construction workers [
66]. This is at odds with the increasing advocacy to give attention to the positive aspects of mental health [
67]. It is argued that a strong focus on understanding and promoting the factors that stimulate positive mental health is a more effective way to helping young people achieve wellbeing as opposed to just mitigating the effects of PRFs. It is, therefore, imperative to build upon the current body of literature by undertaking more research on the personal, socio-economic, and organizational/industrial factors to promote positive mental health among young construction workers.
Second is the need to intensify research on young workers with Global South backgrounds. The greater percentage of the evidence base for the PRF domains and themes that have emerged out of this review are studies which have focused on the Global North context, mostly the Australian construction industry. This indicates that within the extant literature, young construction workers with Global South backgrounds constitute an under-researched population who are experiencing impediments to their mental wellbeing because of their socio-cultural background [
68,
69]. While recommendations from existing research can inform the development of mental health interventions, taken alone, the current body of literature is less than fit for the purpose for addressing the needs of young construction workers with Global South backgrounds. This is partly because people with Global South backgrounds tend to have a poor uptake of Westernized mental healthcare interventions [
70] since these types of interventions tend to be incompatible with their socio-cultural backgrounds [
71]. With Global South countries increasingly investing in improving formal training and education of young people for employment into the construction industry [
2,
72] and some Global North countries seeing young migrants from the Global South as crucial for the post-COVID recovery of their construction sectors [
67,
73], it is vital to intensify research into the management of PRFs that are unique to young workers with Global South backgrounds as this will potentially facilitate the design of new interventions and refine existing ones to be compatible with their the specific situation.
Third, despite the well-supported fact within the broader literature (e.g., [
53,
74]) that psychological stress primarily emanates from outside the workplace, and that both socio-economic and organizational/industrial PRFs influence personal PRFs, psychological distress levels, and mental health, the top five ranked domains (see
Table 1) give evidence that extant research has focused mainly on the role of organizational/industrial and personal PRFs on young construction workers’ mental health outcomes. As such, within the construction literature, very little attention has been given to the influence of socio-economic PRFs such as family background and home support. Therefore, it is important for research within the construction sector not to consider organizational/industry and personal PRFs in isolation, but rather to intensify research on the influence of socio-economic PRFs and how they can also be considered when developing interventions that are robust and responsive to the situation of young construction workers.
Finally, there is a need to increase research on young female workers. Only one study gave exclusive attention to the PRFs that are unique to young female workers, with most of the other studies focusing entirely on young males. This suggests that the PRF domains and associated themes identified in the review invariably reflect the masculine nature of the industry. However, emerging research (e.g., [
75]) suggests that significant differences could exist between the PRFs that affect male and female construction workers, as well as how these two groups experience the psychological stress associated with construction work and its effect on their mental health. With the construction industry being male-dominated and struggling to attract females, greater knowledge of the PRFs affecting young females is needed to inform the development and implementation of appropriate workplace interventions and specific treatment programs that are responsive to the needs of young female workers. This will, in turn, help to achieve a healthy workplace for young females and attract more of them into the industry.
4.6. Limitations
This review has four key limitations. First, although the studies included in this review offer valuable contributions to the knowledge on the mental health of young construction workers, it mostly paints a picture of the situation in the Global North. Therefore, the results of this review cannot easily be generalized across different construction industries due to significant contextual variations between the Global North and other regions of the world. Second, due to language limitations, we restricted the review to English articles only. It is possible that this could have led to the omission of some key issues which could have been critical to the outcomes of the review. Third, while we took stringent measures, such as employing a systematic literature search and selection strategies to ensure validity and analyzed results as a team to limit researcher bias, we acknowledge that the discussions in this study represent, in part, our subjective interpretations of the studies reviewed. Therefore, a possibility remains that other researchers might have different viewpoints and derive different conclusions from the studies that we considered in this review. Finally, the proposed research model only demonstrates the relationships among the different variables but does not include their associated path coefficients. This makes it impossible to tell the level of influence that different PRFs have on psychological distress and poor mental health. Future reviews could seek to determine path coefficients using meta-analysis.
5. Conclusions
There is a growing need to address the problem of poor mental health among young construction workers. This review sought to contribute a greater understanding to the fragmented nature of research on the psychosocial risk factors that contribute to young construction workers’ poor mental health. In total, 30 risk factors were identified from 31 studies and grouped into ten different domains. These were further categorized as personal, socio-economic, and organizational/industrial risks. A conceptual framework was proposed—together with 15 testable propositions—which provides a more unified picture of the patterns of interaction among young construction workers’ PRF domains, as well as their impacts on psychological distress and, eventually, poor mental health.
Our systematic review revealed that, although several studies had examined to some extent the PRFs that contribute to poor mental health among young workers, none had given attention to the factors that could potentially promote positive mental health. Furthermore, little research exists on the case of young workers in the Global South, non-workplace PRFs (e.g., socio-cultural factors such as family conditions, marital issues, and religious beliefs), and the case of young females in the construction industry. Future studies will need to give greater attention to these factors, as well as seek to validate the conceptual framework proposed in this review.
The findings of this review are useful to construction firms, mental health practitioners, researchers, and policy makers for prioritizing resources for addressing the impacts of psychosocial risk factors. They are also useful for the design and implementation of effective mental health interventions targeted specifically at young construction workers.








{kind=link}
{kind=link}
{kind=link}