COVID-19: Research Directions for Non-Clinical Aerosol-Generating Facilities in the Built Environment



Abstract
:1. Introduction
2. Methods and Materials
3. Aerosol Transmission and Aerosol-Rich Facilities
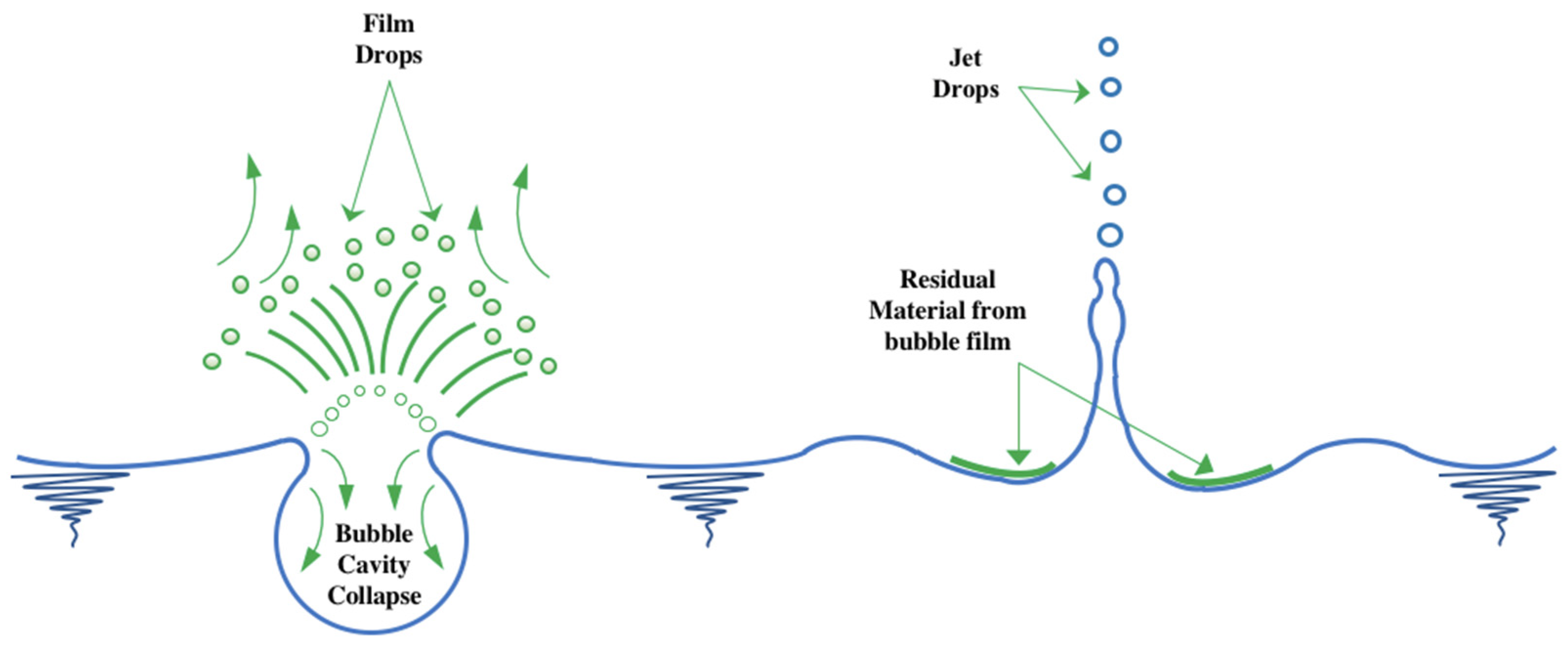
3.1. Mechanism of Aerosol Transmission
3.2. Aerosol-Rich Facilities
3.3. Virus Spread Containment Measures
3.3.1. Water Disinfection
3.3.2. Ventilation-Aided Operation
4. Recent Research Efforts
4.1. Spread and New Variants
4.2. Critical Factors
4.3. Control and Certification
5. Future Research Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. World Health Organization COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 28 April 2021).
- Billah, A.; Miah, M.; Khan, N. Reproductive number of coronavirus: A systematic review and meta-analysis based on global level evidence. PLoS ONE 2020, 15, e0242128. [Google Scholar] [CrossRef]
- Biggerstaff, M.; Cauchemez, S.; Reed, C.; Gambhir, M.; Finelli, L. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: A systematic review of the literature. BMC Infect. Dis. 2014, 14, 480. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Jackson, C.B.; Mou, H.; Ojha, A.; Peng, H.; Quinlan, B.D.; Rangarajan, E.S.; Pan, A.; Vanderheiden, A.; Suthar, M.S.; et al. SARS-CoV-2 spike-protein D614G mutation increases virion spike density and infectivity. Nat. Commun. 2020, 11, 6013. [Google Scholar] [CrossRef]
- Pachetti, M.; Marini, B.; Benedetti, F.; Giudici, F.; Mauro, E.; Storici, P.; Masciovecchio, C.; Angeletti, S.; Cicozzi, M.; Gallo, R.C.; et al. Emerging SARS-CoV-2 mutation hot spots include a novel RNA-dependent-RNA polymerase variant. J. Transl. Med. 2020, 18, 179. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Wu, C.; Li, X.; Song, Y.; Yao, X.; Wu, X.; Duan, Y.; Zhang, H.; Wang, Y.; Qian, Z.; et al. On the origin and continuing evolution of SARS-CoV-2. Natl. Sci. Rev. 2020, 7, 1012–1023. [Google Scholar] [CrossRef] [Green Version]
- Dawood, A. Mutated COVID-19 may foretell a great risk for mankind in the future. New Microbes New Infect. 2020, 35, 100673. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.Y.; For the Singapore 2019 Novel Coronavirus Outbreak Research Team; Coleman, K.K.; Tan, Y.K.; Ong, S.W.X.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; et al. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Milton, D.K. It Is Time to Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kohanski, M.A.; Lo, L.J.; Waring, M.S. Review of indoor aerosol generation, transport, and control in the context of COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- WHO. Roadmap to Improve and Ensure Good Indoor Ventilation in the Context of COVID-19. 2021. Available online: https://www.who.int/publications/i/item/9789240021280 (accessed on 1 March 2021).
- Zhao, J.-Y.; Yan, J.-Y.; Qu, J.-M. Interpretations of “Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7)”. Chin. Med. J. 2020, 133, 1347–1349. [Google Scholar] [CrossRef]
- Stilianakis, N.I.; Drossinos, Y. Dynamics of infectious disease transmission by inhalable respiratory droplets. J. R. Soc. Interface 2010, 7, 1355–1366. [Google Scholar] [CrossRef] [Green Version]
- Somsen, G.A.; van Rijn, C.; Kooij, S.; A Bem, R.; Bonn, D. Small droplet aerosols in poorly ventilated spaces and SARS-CoV-2 transmission. Lancet Respir. Med. 2020, 8, 658–659. [Google Scholar] [CrossRef]
- Hadei, M.; Hopke, P.K.; Jonidi, A.; Shahsavani, A. A Letter about the Airborne Transmission of SARS-CoV-2 Based on the Current Evidence. Aerosol Air Qual. Res. 2020, 20, 911–914. [Google Scholar] [CrossRef] [Green Version]
- Morawska, L. Droplet fate in indoor environments, or can we prevent the spread of infection? Indoor Air 2006, 16, 335–347. [Google Scholar] [CrossRef] [Green Version]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef]
- Lee, S.-A.; Grinshpun, S.A.; Reponen, T. Respiratory Performance Offered by N95 Respirators and Surgical Masks: Human Subject Evaluation with NaCl Aerosol Representing Bacterial and Viral Particle Size Range. Ann. Occup. Hyg. 2008, 52, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Lloyd-Smith, J.O.; De Wit, E.; Munster, V.J.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Bescos, R.; Casas-Agustench, P.; Belfield, L.; Brookes, Z.; Gabaldón, T. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 1113. [Google Scholar] [CrossRef]
- Mick, P.; Murphy, R. Aerosol-generating otolaryngology procedures and the need for enhanced PPE during the COVID-19 pandemic: A literature review. J. Otolaryngol. 2020, 49, 1–10. [Google Scholar] [CrossRef]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Feng, G.; Bi, Y.; Cai, Y.; Zhang, Z.; Cao, G. Distribution of droplet aerosols generated by mouth coughing and nose breathing in an air-conditioned room. Sustain. Cities Soc. 2019, 51, 101721. [Google Scholar] [CrossRef]
- Zhang, N.; Huang, H.; Su, B.; Ma, X.; Li, Y. A human behavior integrated hierarchical model of airborne disease transmission in a large city. Build. Environ. 2018, 127, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]
- Valeriani, F.; Margarucci, L.M.; Spica, V.R. Recreational Use of Spa Thermal Waters: Criticisms and Perspectives for Innovative Treatments. Int. J. Environ. Res. Public Health 2018, 15, 2675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchard, D.C.; Syzdek, L.D. Water-to-Air Transfer and Enrichment of Bacteria in Drops from Bursting Bubbles. Appl. Environ. Microbiol. 1982, 43, 1001–1005. [Google Scholar] [CrossRef] [Green Version]
- Bouwknegt, M.; Schijven, J.; Schalk, J.A.; Husman, A.M.D.R. Quantitative Risk Estimation for aLegionella pneumophilaInfection Due to Whirlpool Use. Risk Anal. 2013, 33, 1228–1236. [Google Scholar] [CrossRef]
- Moore, G.; Hewitt, M.; Stevenson, D.; Walker, J.T.; Bennett, A. Aerosolization of Respirable Droplets from a Domestic Spa Pool and the Use of MS-2 Coliphage and Pseudomonas aeruginosa as Markers for Legionella pneumophila. Appl. Environ. Microbiol. 2014, 81, 555–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poor, B.M.; Dalimi, A.; Ghafarifar, F.; Khoshzaban, F.; Abdolalizadeh, J. Contamination of swimming pools and hot tubs biofilms with Acanthamoeba. Acta Parasitol. 2018, 63, 147–153. [Google Scholar] [CrossRef]
- Luo, C.; Yao, L.; Zhang, L.; Yao, M.; Chen, X.; Wang, Q.; Shen, H. Possible Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a Public Bath Center in Huai’an, Jiangsu Province, China. JAMA Netw. Open 2020, 3, e204583. [Google Scholar] [CrossRef] [Green Version]
- Mizumoto, K.; Chowell, G. Transmission potential of the novel coronavirus (COVID-19) onboard the diamond Princess Cruises Ship, 2020. Infect. Dis. Model. 2020, 5, 264–270. [Google Scholar] [CrossRef]
- Almilaji, O.; Thomas, P. Air recirculation role in the infection with COVID-19, lessons learned from Diamond Princess cruise ship. medRxiv 2020. [Google Scholar] [CrossRef]
- Parham, A.; Zahra, K.; Jose, G.C.L.; Brent, R.S.; Joseph, G.A. Mechanistic Transmission Modeling of COVID-19 on the Diamond Princess Cruise Ship Demonstrates the Importance of Aerosol Transmission. medRxiv 2020. [Google Scholar] [CrossRef]
- Darnell, M.E.; Subbarao, K.; Feinstone, S.M.; Taylor, D.R. Inactivation of the coronavirus that induces severe acute respiratory syndrome, SARS-CoV. J. Virol. Methods 2004, 121, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-H.; Wu, U.-I.; Tai, H.-M.; Sheng, W.-H. Effectiveness of an ultraviolet-C disinfection system for reduction of healthcare-associated pathogens. J. Microbiol. Immunol. Infect. 2019, 52, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.K.; Lee, J. Prevalence and Antimicrobial-Resistance of Pseudomonas aeruginosa in Swimming Pools and Hot Tubs. Int. J. Environ. Res. Public Health 2011, 8, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Cahill, N.; Morris, D. Recreational waters—A potential transmission route for SARS-CoV-2 to humans? Sci. Total Environ. 2020, 740, 140122. [Google Scholar] [CrossRef] [PubMed]
- Gundy, P.M.; Gerba, C.P.; Pepper, I.L. Survival of Coronaviruses in Water and Wastewater. Food Environ. Virol. 2009, 1, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Romano-Bertrand, S.; Glele, L.-S.A.; Grandbastien, B.; Lepelletier, D. Preventing SARS-CoV-2 transmission in rehabilitation pools and therapeutic water environments. J. Hosp. Infect. 2020, 105, 625–627. [Google Scholar] [CrossRef] [PubMed]
- Lazzarin, R.M.; Longo, G.A. Comparison of heat recovery systems in public indoor swimming pools. Appl. Therm. Eng. 1996, 16, 561–570. [Google Scholar] [CrossRef]
- Law, R.C.K.; Lai, J.H.K. COVID-19: What’s next for facilities managers, engineers and researchers? Hong Kong Eng. 2020, 48, 15–17. [Google Scholar]
- Amoah, I.D.; Kumari, S.; Bux, F. Coronaviruses in wastewater processes: Source, fate and potential risks. Environ. Int. 2020, 143, 105962. [Google Scholar] [CrossRef]
- WHO. Global Research on Coronavirus Disease (COVID-19). 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov (accessed on 10 February 2021).
- Kang, M.; Wei, J.; Yuan, J.; Guo, J.; Zhang, Y.; Hang, J.; Qu, Y.; Qian, H.; Zhuang, Y.; Chen, X.; et al. Probable Evidence of Fecal Aerosol Transmission of SARS-CoV-2 in a High-Rise Building. Ann. Intern. Med. 2020, 173, 974–980. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Rapid Increase of a SARS-CoV-2 Variant with Multiple Spike Protein Mutations Observed in the United Kingdom; ECDC: Stockholm, Sweden, 2020.
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- Megahed, N.A.; Ghoneim, E.M. Antivirus-built environment: Lessons learned from Covid-19 pandemic. Sustain. Cities Soc. 2020, 61, 102350. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.M.; Xu, P.; Xiao, T.; He, R.; Dai, M.; Miller, S.L. Review and comparison of HVAC operation guidelines in different countries during the COVID-19 pandemic. Build. Environ. 2021, 187, 107368. [Google Scholar] [CrossRef]
- Raj, A.; Velraj, R.; Fariborz, H. The contribution of dry indoor built environment on the spread of Coronavirus: Data from various Indian states. Sustain. Cities Soc. 2020, 62, 102371. [Google Scholar] [CrossRef]
- Leng, J.; Wang, Q.; Liu, K. Sustainable design of courtyard environment: From the perspectives of airborne diseases control and human health. Sustain. Cities Soc. 2020, 62, 102405. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Cheng, P.; Jia, W.; Dung, C.-H.; Liu, L.; Chen, W.; Lei, H.; Kan, C.; Han, X.; Su, B.; et al. Impact of intervention methods on COVID-19 transmission in Shenzhen. Build. Environ. 2020, 180, 107106. [Google Scholar] [CrossRef]
- Xu, C.; Wei, X.; Liu, L.; Su, L.; Liu, W.; Wang, Y.; Nielsen, P.V. Effects of personalized ventilation interventions on airborne infection risk and transmission between occupants. Build. Environ. 2020, 180, 107008. [Google Scholar] [CrossRef] [PubMed]
- Blocken, B.; van Druenen, T.; van Hooff, T.; Verstappen, P.; Marchal, T.; Marr, L. Can indoor sports centers be allowed to re-open during the COVID-19 pandemic based on a certificate of equivalence? Build. Environ. 2020, 180, 107022. [Google Scholar] [CrossRef]
- Newman, C.; Edwards, D.; Martek, I.; Lai, J.; Thwala, W.D.; Rillie, I. Industry 4.0 deployment in the construction industry: A bibliometric literature review and UK-based case study. Smart Sustain. Built Environ. 2020. [Google Scholar] [CrossRef]
- Sepasgozar, S.M.E.; Shi, A.; Yang, L.; Shirowzhan, S.; Edwards, D.J. Additive Manufacturing Applications for Industry 4.0: A Systematic Critical Review. Buildings 2020, 10, 231. [Google Scholar] [CrossRef]
- Ghansah, F.A.; Owusu-Manu, D.-G.; Ayarkwa, J.; Darko, A.; Edwards, D.J. Underlying indicators for measuring smartness of buildings in the construction industry. Smart Sustain. Built Environ. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| WHO: Guidelines For Safe Recreational Water Environments Volume 2 Swimming Pools and Similar Environments | Centre for Health Protection, HKSARG: Guidelines on Infection Control of Commercial Spa Pools | Queensland Health: Water Quality Guidelines for Public Aquatic Facilities | ANSI/APSP/ICC-11-2019: American National Standard for Water Quality in Public Pools and Spas | HSE, U.K.: The Control of Legionella and Other Infectious Agents in Spa-Pool Systems | Newfoundland and Labrador: Public Pool Standards and Guidelines | ||
|---|---|---|---|---|---|---|---|
| System Disinfection | Turnover Rate (min) | 5–20 | Not Specified | 20–30 | Not Specified | 6–15 | Not Specified |
| Free chlorine (ppm) | 2–3 (Twice daily) | 3–5 (Twice daily) | ≥3 (Five times daily (i)) | 2–5 (Hourly) | 3–5 (Daily at opening and every two hours thereafter) | 1.5 (Class A Pool); 2–3 (Class B Pool) (iii); (1/2 h before opening and every four hours thereafter) | |
| Combined chlorine (ppm) | ideally <0.2 | ≤1 (Twice daily) | ≤1, ideally <0.2 (Five times daily) | ≤0.4 (Hourly) | ≤1 (Ditto) | ≤0.5 (Ditto) | |
| Water balance | pH value | 7.2–7.8 (Several times a day) | 7.2–7.8 (Twice daily) | 7.2–7.8 (Five times daily) | 7.2–7.8 (Twice daily) | 7.0–7.6 (Ditto) | 7.2–7.8 (Ditto) |
| Total alkalinity (mg/L) | Not specified | 80–200 (Not specified) | 80–120 (Weekly) | 60–180 (Once daily) | Not specified | 80–120 (Weekly, Class A; Daily, Class B) | |
| Microbiological quality | Calcium hardness (mg/L) | Not specified | 75–150 (Not specified) | Not specified (Weekly) | 100–800 (Once daily) | Not specified | 200–300 (Weekly) |
| Total bacteria count (CFU/mL) | Not specified | ≤200 (Monthly) | ≤100 (Monthly) | ≤200 (Not specified) | <100 (Monthly) | <250 (Not specified) | |
| Escherichia coli (CFU/100 mL) | <1 (Monthly) | 0 (Monthly) | <1 (Monthly) | <2 (Not specified) | <1 (Monthly) | 0 (Not specified) | |
| Pseudomonas aeruginosa (CFU/100 mL) | <1 (Weekly) | Not specified | <1 (Monthly) | Not specified | <10 (Monthly) | <10 (Not specified) | |
| Legionella (CFU/100 mL) | <1 (Monthly) | Not specified | Not specified | Not specified | <100 (Quarterly) | Not specified | |
| Staphylococcus aureus (CFU/100 mL) | <100 (Not specified) | Not specified | Not specified | Not specified | Not specified | <50 (Not specified) | |
| Clarity | Turbidity (NTU) | ≤0.5 (Not specified) | ≤0.5 (Once daily) | ≤0.5 (Once daily) | Visible | Total dissolved solids (TDS) ≤1000 ppm (Daily) | (Not specified) |
| Notes | - | Drain the pool weekly; backwash filters weekly; cleanse pool, equipment, and pool surrounding daily | Highly recommended to use secondary disinfectant (e.g., UV and ozone) | Recommend complete draining instead of gradual water replacement based on given formula (ii) | Backwashing should be done after the last user of the day; total volume should be drained weekly | - | |
| Australia | China | Hong Kong | U.K. | U.S. | U.S. | |
|---|---|---|---|---|---|---|
| Guideline/ Codes | Code of Practice for the Design, Construction, Operation, Management & Maintenance of Aquatic Facilities | GB 37488-2012: Hygienic indicators and limits for public places | Guidelines on Infection Control of Commercial Spa Pools | HSG 282—The control of legionella and other infectious agents in spa-pool systems | ASHRAE 62.1 Ventilation for Acceptable Indoor Air Quality | California Mechanical Code 2016 |
| Ventilation requirement | 10 L/s (per person), or 10 L/s/m2 (of wet area) | Min. outdoor air: 20 m3/h per person (i.e., 5.56 L/s/p), CO2 ≤ 1500 ppm, bacterial concentrations ≤ 4000 CFU/m3 | N.A. (ventilation should be of 6 to 12 air changes per hour) | 10–15 L/s/m2 (of wet area) | 3.2 L/s/m2 (of wet area) (akin to general swimming pool) | Negative pressure, min. outdoor air change: 2 (min.); 6 (for hospital hydrotherapy setting) |
| Measure | Engineering Institutions | Management Institutions | ||||
|---|---|---|---|---|---|---|
| ASHRAE: Guidance for Building Operations during the COVID-19 Pandemic; Position Document on Infectious Aerosols | ISHARE COVID-19 Guidance Document for Air Conditioning and Ventilation | REHVA COVID-19 Guidance | CIBSE COVID-19 Ventilation Guidance | IFMA Pandemic Manual | CPMI: Technical Guidelines for the Operation Management of Air-conditioning Ventilation System in Public Buildings During the COVID-19 Epidemic | |
| ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| ✔ | ✔ | ✔ | ✔ | - | ✔ |
| ✔ | (For quarantine areas and COVID-19 patient area and industrial facilities) | ✔ | ✔ | ✔ | ✔ |
| ✔ | ✔ | - | - | ✔ | ✔ |
| ✔ (24/7 if possible) | ✔ (Fresh air and ventilation system should be kept on throughout the off cycle and on the weekend and holidays in air circulation mode) | ✔ (Start ventilation at nominal speed at least 2 h before the building usage time and switch to lower speed 2 h after the building usage time; keep the ventilation on 24/7 with lower ventilation rates when people are absent) | ✔ | ✔ (Start the AC system 1 or 2 h before the building usage time) | |
| ✔ | - | ✔ | ✔ | - | - |
| ✔ (For high-density spaces such as waiting rooms, prisons, and shelters) | ✔ (For larger ducted units and AHUs) | ✔ (Normally a suitable solution for healthcare facilities) | - | - | |
| ✔ (As applicable to the infectious aerosols of concern) | ✔ (Humidity: 40–70%; Temperature: 24–30 °C) | - | ✔ (Maintain relative humidity above 40% wherever possible) | - | Properly increase supply air temperature and indoor temperature setpoint in summer, etc. |
| - | ✔ | As usual | ✔ | ✔ | |
| ✔ | - | Change CO2 setpoint to lower, 400 ppm value, in order to maintain the operation at nominal speed | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Law, R.C.K.; Lai, J.H.K.; Edwards, D.J.; Hou, H. COVID-19: Research Directions for Non-Clinical Aerosol-Generating Facilities in the Built Environment. Buildings 2021, 11, 282. https://doi.org/10.3390/buildings11070282
Law RCK, Lai JHK, Edwards DJ, Hou H. COVID-19: Research Directions for Non-Clinical Aerosol-Generating Facilities in the Built Environment. Buildings. 2021; 11(7):282. https://doi.org/10.3390/buildings11070282
Chicago/Turabian StyleLaw, Roger C. K., Joseph H. K. Lai, David John Edwards, and Huiying (Cynthia) Hou. 2021. "COVID-19: Research Directions for Non-Clinical Aerosol-Generating Facilities in the Built Environment" Buildings 11, no. 7: 282. https://doi.org/10.3390/buildings11070282