
Theorizing to Improve Mental Health in Multicultural Construction Industries: An Intercultural Coping Model


Abstract
:1. Introduction
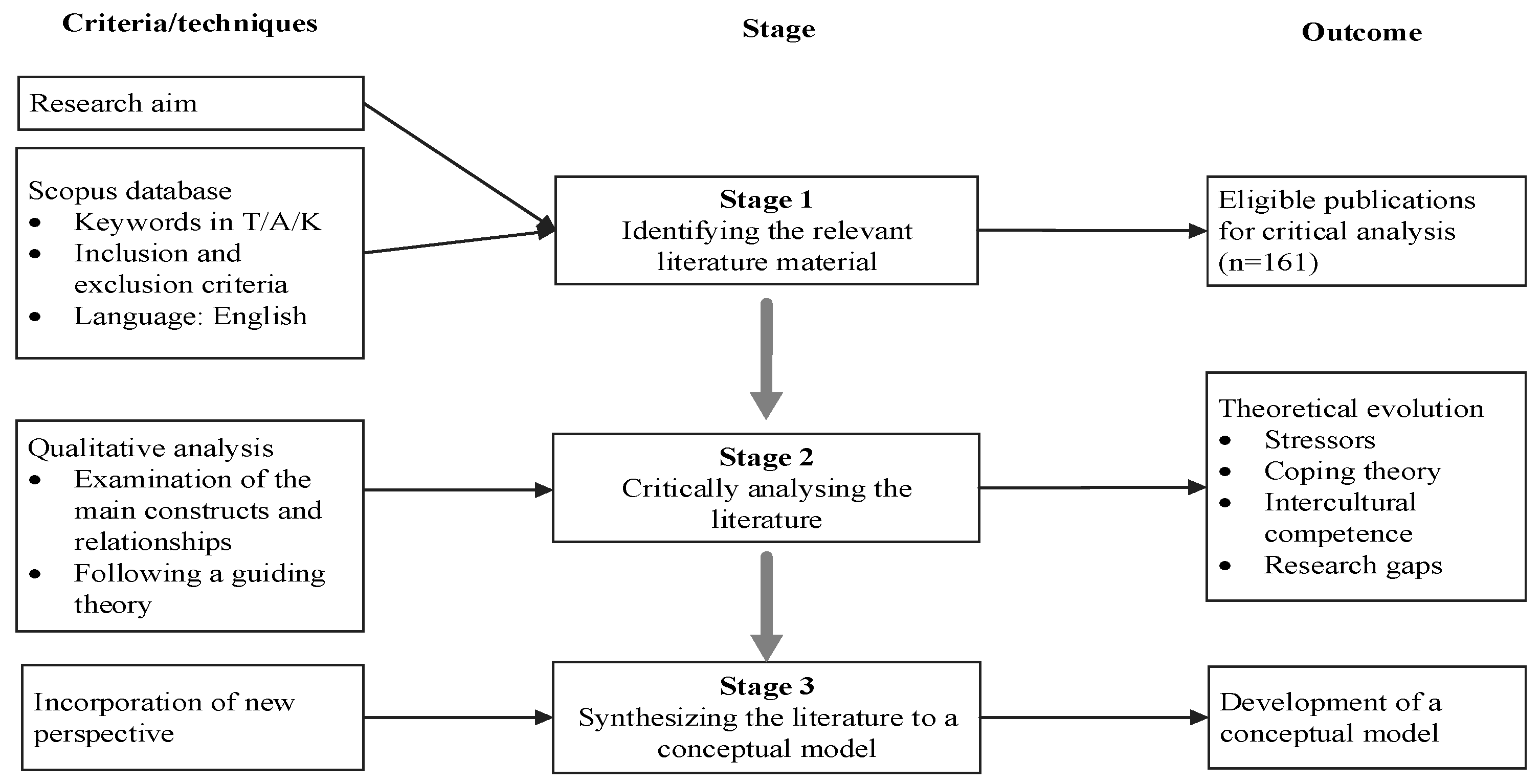
2. Methodology
2.1. Stage 1—Identifying the Relevant Literature Material
2.2. Stage 2—Critically Analyzing the Literature
2.3. Stage 3—Synthesizing the Literature to a Conceptual Model
3. Theoretical Evolution
3.1. Stressors of Construction Workers’ Mental Health
3.1.1. Work Stressors
3.1.2. Personal Stressors
3.1.3. Cultural Stressor
3.2. Coping
3.2.1. The Concept of Coping
3.2.2. Coping in Construction
3.2.3. Proactive Coping
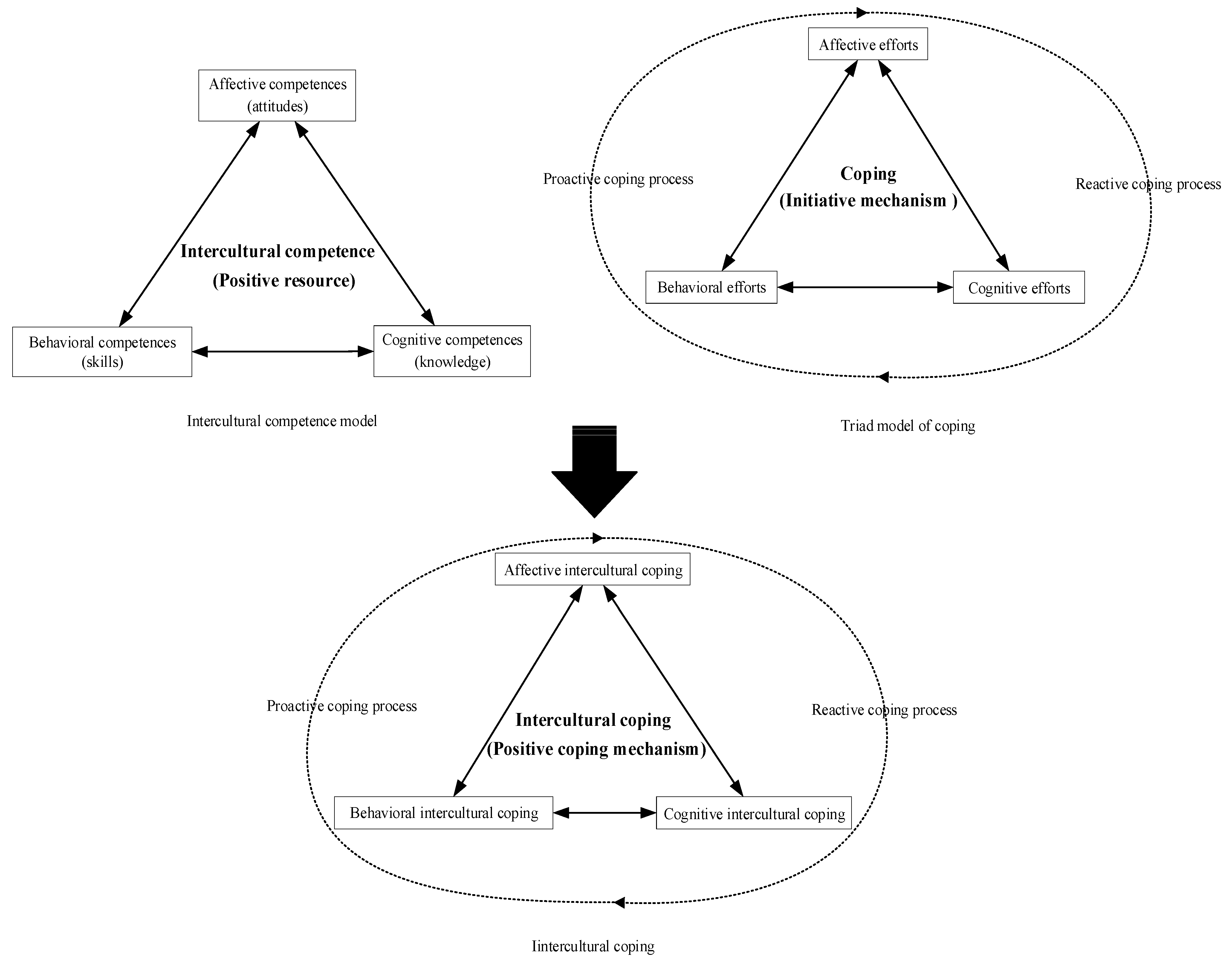
3.3. Intercultural Coping
3.3.1. Intercultural Competence
3.3.2. Incorporating Intercultural Competence into Coping
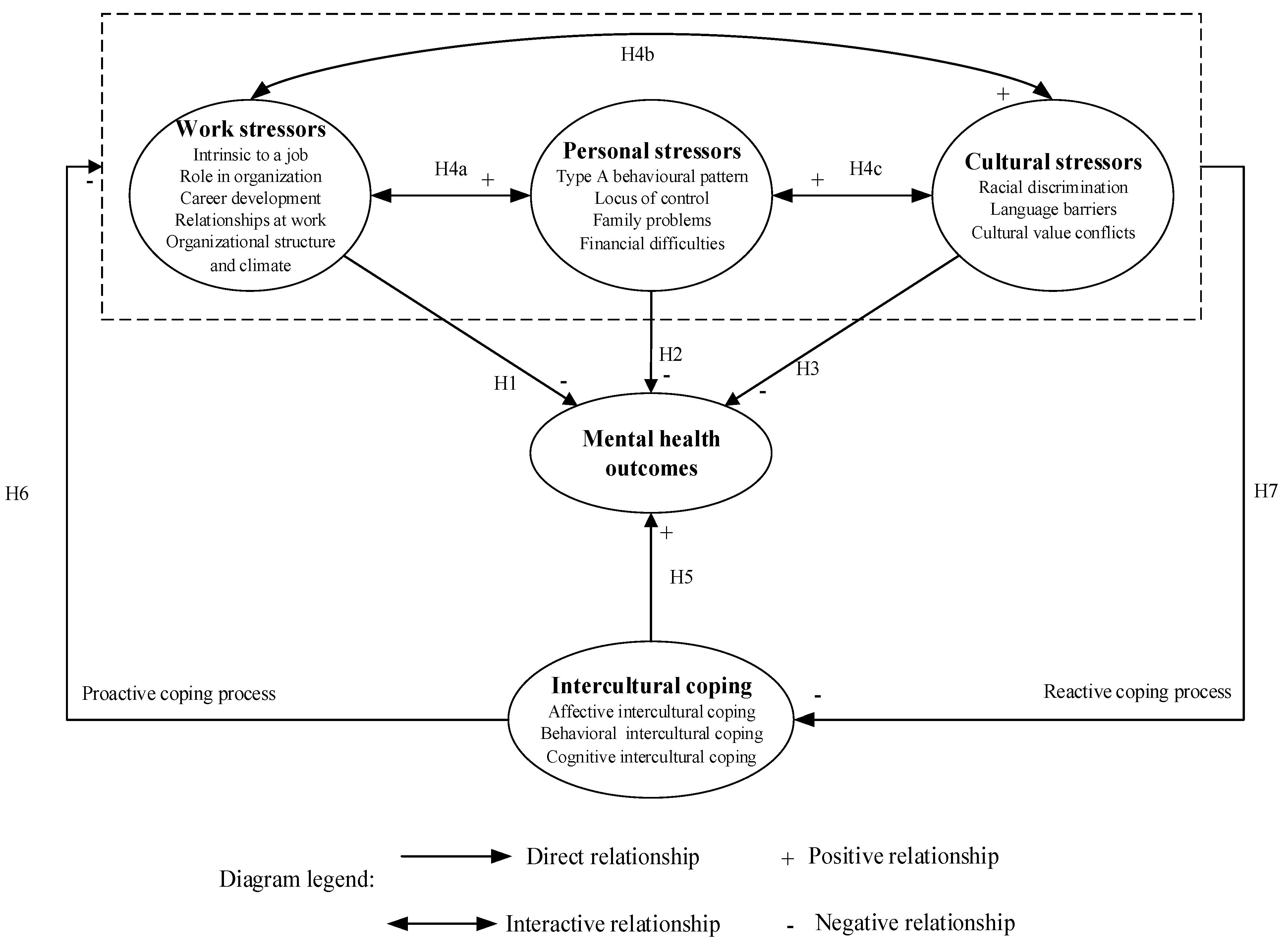
4. Conceptual Model
5. Implications for Future Research
5.1. Investigation of Different Types of Psychological Problems
5.2. Interactive Effects of Stressors on Mental Health Outcomes
5.3. Development of Positive Interventions
5.4. Mental Health Management from Different Levels of Cultural Diversity
5.5. Empirical Examinations on the Conceptual Model
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loosemore, M.; Phua, F.; Dunn, K.; Ozguc, U. Operatives’ experiences of cultural diversity on Australian construction sites. Constr. Manag. Econ. 2010, 28, 177–188. [Google Scholar] [CrossRef]
- Lingard, H.; Turner, M. Promoting construction workers’ health: A multi-level system perspective. Constr. Manag. Econ. 2017, 35, 239–253. [Google Scholar] [CrossRef]
- PricewaterhouseCoopers. Creating a Mentally Healthy Workplace: Return on Investment Analysis; PricewaterhouseCoopers: Australia, 2014. Available online: http://www.headsup.org.au/docs/default-source/resources/beyondblue_workplaceroi_finalreport_may-2014.pdf (accessed on 17 December 2021).
- Campbell, F. Occupational Stress in the Construction Industry; Chartered Institute of Building: Berkshire, UK, 2006. [Google Scholar]
- Alderson, L. Uncovered: The Truth behind Construction’s Mental Health. Available online: https://www.constructionnews.co.uk/agenda/mind-matters/uncovered-the-truth-behind-constructions-mental-health-27-04-2017/ (accessed on 7 October 2021).
- BCBuildingTrades. 83% of Construction Workers Have Experienced a Mental Health Issue. Available online: https://bcbuildingtrades.org/83-of-construction-workers-have-experienced-a-mental-health-issue/ (accessed on 28 July 2021).
- Wong, J.; Teo, M.; Cheung, Y.K.F. Cultural determinants of stress in the construction industry. In Proceedings of the 2010 International Conference On Construction & Real Estate Management, Brisbane, Australia, 1–3 December 2010; pp. 44–49. [Google Scholar]
- Milner, A.; Law, P.C.F. Summary Report: Mental Health in the Construction Industry; University of Melbourne: Melbourne, Australia, 2017. [Google Scholar]
- Stevenson, D. Thriving at Work: The Stevenson/Farmer Review of Mental Health and Employers; Department for Work and Pensions: London, UK; Department of Health: London, UK, 2017.
- WHO. Strengthening Mental Health Promotion: Mental Health Is Not just the Absence of Mental Disorder; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Pidd, K.; Duraisingam, V.; Roche, A.; Trifonoff, A. Young construction workers: Substance use, mental health, and workplace psychosocial factors. Adv. Dual Diagn. 2017, 10, 155–168. [Google Scholar] [CrossRef]
- Park, H.; Sprince, N.L.; Lewis, M.Q.; Burmeister, L.F.; Whitten, P.S.; Zwerling, C. Risk factors for work-related injury among male farmers in Iowa: A prospective cohort study. J. Occup. Environ. Med. 2001, 43, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Langdon, R.R.; Sawang, S. Construction Workers’ Well-Being: What Leads to Depression, Anxiety, and Stress? J. Constr. Eng. Manag. 2018, 144, 04017100. [Google Scholar] [CrossRef] [Green Version]
- Love, P.E.D.; Edwards, D.J.; Irani, Z. Work stress, support, and mental health in construction. J. Constr. Eng. Manag. 2010, 136, 650–658. [Google Scholar] [CrossRef]
- Sunindijo, R.Y.; Kamardeen, I. Work Stress Is a Threat to Gender Diversity in the Construction Industry. J. Constr. Eng. Manag. 2017, 143, 04017073. [Google Scholar] [CrossRef]
- Rosewarne, S.; Shin, J.S.; McGrath-Champ, S.; Toner, P. The globalisation of the construction work force: The impact on the Australian building and construction industry. In Proceedings of the 4th Asia-Pacific Building Unions Seminar, Beijing, China, 23 August 2006. [Google Scholar]
- Loosemore, M. Work Force Diversity is Key to Construction Innovation. Sourceable. 12 October 2015. Available online: https://sourceable.net/workforce-diversity-is-key-to-construction-innovation/ (accessed on 30 May 2021).
- Statista. Number of Foreign Construction Workers Employed in Singapore from 2013 to 2019. Available online: https://www.statista.com/statistics/1054354/singapore-foreign-construction-workers-employed/ (accessed on 30 May 2021).
- NAHB, E. Immigrant Workers in the Construction Labor Force. Available online: https://www.nahbclassic.org/fileUpload_details.aspx?contentTypeID=3&contentID=272199&subContentID=738700 (accessed on 30 May 2021).
- Office for National Statistics. Migrant Labour Force within the UK’s Construction Industry: August 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/internationalmigration/articles/migrantlabourforcewithintheconstructionindustry/august2018 (accessed on 18 December 2021).
- DeSimone, R.L.; Harris, D.M. Human Resource Development; The Dryden Press: Orlando, FL, USA, 1998. [Google Scholar]
- Berry, J.W. Immigration, acculturation, and adaptation. Appl. Psychol. 1997, 46, 5–34. [Google Scholar] [CrossRef]
- Redfield, R.; Linton, R.; Herskovits, M. Memorandum for the study of acculturation. Am. Anthropol. 1936, 38, 149–152. [Google Scholar] [CrossRef]
- Matsudaira, T. Measures of psychological acculturation: A review. Transcult. Psychiatry 2006, 43, 462–487. [Google Scholar] [CrossRef]
- Cano, M.Á.; Schwartz, S.J.; Castillo, L.G.; Romero, A.J.; Huang, S.; Lorenzo-Blanco, E.I.; Unger, J.B.; Zamboanga, B.L.; Des Rosiers, S.E.; Baezconde-Garbanati, L. Depressive symptoms and externalizing behaviors among Hispanic immigrant adolescents: Examining longitudinal effects of cultural stress. J. Adolesc. 2015, 42, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega, W.A.; Alegría, M. Latino mental health and treatment in the United States. Health Issues Lat. Community 2001, 7, 179–208. [Google Scholar]
- Torres, L.; Rollock, D. Acculturative distress among Hispanics: The role of acculturation, coping, and intercultural competence. J. Multicult. Couns. Dev. 2004, 32, 155–167. [Google Scholar] [CrossRef]
- Torraco, R.J. Writing integrative literature reviews: Guidelines and examples. Hum. Resour. Dev. Rev. 2005, 4, 356–367. [Google Scholar] [CrossRef]
- Finfgeld-Connett, D. Use of content analysis to conduct knowledge-building and theory-generating qualitative systematic reviews. Qual. Res. 2014, 14, 341–352. [Google Scholar] [CrossRef]
- Snyder, H. Literature review as a research methodology: An overview and guidelines. J. Bus. Res. 2019, 104, 333–339. [Google Scholar] [CrossRef]
- Hong, Y.; Chan, D.W. Research trend of joint ventures in construction: A two-decade taxonomic review. J. Facil. Manag. 2014, 12, 118–141. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, web of science, and Google scholar: Strengths and weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H.W. Psychosocial work environment and mental health among construction workers. Appl. Ergon. 2013, 44, 748–755. [Google Scholar] [CrossRef]
- Bhagat, R.S.; McQuaid, S.J.; Lindholm, H.; Segovis, J. Total life stress: A multimethod validation of the construct and its effects on organizationally valued outcomes and withdrawal behaviors. J. Appl. Psychol. 1985, 70, 202. [Google Scholar] [CrossRef]
- Leung, M.Y.; Ng, S.T.; Skitmore, M.; Cheung, S.O. Critical stressors influencing construction estimators in Hong Kong. Constr. Manag. Econ. 2005, 23, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Cooper, C.L.; Marshall, J. Occupational sources of stress: A review of the literature relating to coronary heart disease and mental ill health. J. Occup. Organ. Psychol. 1976, 49, 11–28. [Google Scholar] [CrossRef]
- Yip, B.; Rowlinson, S.; Siu, O.L. Coping strategies as moderators in the relationship between role overload and burnout. Constr. Manag. Econ. 2008, 26, 869–880. [Google Scholar] [CrossRef] [Green Version]
- Sang, K.; Dainty, A.; Ison, S. Warning: Working in Construction May Be Harmful to Your Psychological Well-Being! In People and Culture in Construction: A Reader; Taylor & Francis Group: London, UK, 2007; pp. 127–143. [Google Scholar]
- Tijani, B.; Jin, X.; Osei-kyei, R. A systematic review of mental stressors in the construction industry. Int. J. Build. Pathol. Adapt. 2021, 39, 433–460. [Google Scholar] [CrossRef]
- Leung, M.Y.; Chan, Y.S.; Yu, J. Integrated model for the stressors and stresses of construction project managers in Hong Kong. J. Constr. Eng. Manag. 2009, 135, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Chen, C.W.; Chen, C.J.; Chiang, T.L. Job insecurity and its association with health among employees in the Taiwanese general population. Soc. Sci. Med. 2005, 61, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.Y.; Liang, Q.; Chan, I.Y.S. Development of a Stressors-Stress-Performance-Outcome Model for Expatriate Construction Professionals. J. Constr. Eng. Manag. 2017, 143, 04016121. [Google Scholar] [CrossRef]
- Joiner, T.A. The influence of national culture and organizational culture alignment on job stress and performance: Evidence from Greece. J. Manag. Psychol. 2001, 16, 229–242. [Google Scholar] [CrossRef]
- Leung, M.Y.; Skitmore, M.; Chan, Y.S. Subjective and objective stress in construction cost estimation. Constr. Manag. Econ. 2007, 25, 1063–1075. [Google Scholar] [CrossRef] [Green Version]
- Leung, M.Y.; Chan, I.Y.S. Exploring stressors of Hong Kong expatriate construction professionals in Mainland China: Focus group study. J. Constr. Eng. Manag. 2012, 138, 78–88. [Google Scholar] [CrossRef]
- Loosemore, M.; Lam, A.S.Y. The locus of control: A determinant of opportunistic behaviour in construction health and safety. Constr. Manag. Econ. 2004, 22, 385–394. [Google Scholar] [CrossRef]
- Chan, A.P.; Nwaogu, J.M.; Naslund, J.A. Mental ill-health risk factors in the construction industry: Systematic review. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- Liang, Q.; Leung, M.Y.; Cooper, C. Focus Group Study to Explore Critical Factors for Managing Stress of Construction Workers. J. Constr. Eng. Manag. 2018, 144, 04018023. [Google Scholar] [CrossRef] [Green Version]
- Al-Maskari, F.; Shah, S.M.; Al-Sharhan, R.; Al-Haj, E.; Al-Kaabi, K.; Khonji, D.; Schneider, J.D.; Nagelkerke, N.J.; Bernsen, R.M. Prevalence of depression and suicidal behaviors among male migrant workers in United Arab Emirates. J. Immigr. Minor. Health 2011, 13, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Luo, X.; Wang, T.; Wang, Y.; Sapkota, B. Safety challenges and improvement strategies of ethnic minority construction workers: A case study in Hong Kong. Int. J. Occup. Saf. Ergon. 2018, 26, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.P.C.; Wong, F.K.W.; Hon, C.K.H.; Javed, A.A.; Lyu, S. Construction safety and health problems of ethnic minority workers in Hong Kong. Eng. Constr. Archit. Manag. 2017, 24, 901–919. [Google Scholar] [CrossRef]
- Wong, J.K.W.; Lin, A.H.Q. Construction workplace discrimination: Experiences of ethnic minority operatives in Hong Kong construction sites. Eng. Constr. Archit. Manag. 2014, 21, 403–420. [Google Scholar] [CrossRef]
- Loosemore, M.; Phua, F.T.T.; Dunn, K.; Ozguc, U. The politics of sameness in the Australian construction industry: Comparing operative and manager attitudes towards cultural diversity. Eng. Constr. Archit. Manag. 2011, 18, 363–380. [Google Scholar] [CrossRef]
- Ling, F.Y.Y.; Dulaimi, M.F.; Chua, M. Strategies for managing migrant construction workers from China, India, and the Philippines. J. Prof. Issues Eng. Educ. Pr. 2013, 139, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Spector, P.E. Employee control and occupational stress. Curr. Dir. Psychol. Sci. 2002, 11, 133–136. [Google Scholar] [CrossRef]
- Love, P.E.D.; Edwards, D.J. Taking the pulse of UK construction project managers’ health: Influence of job demands, job control and social support on psychological wellbeing. Eng. Constr. Archit. Manag. 2005, 12, 88–101. [Google Scholar] [CrossRef]
- Johnson, S.; Cooper, C.; Cartwright, S.; Donald, I.; Taylor, P.; Millet, C. The experience of work-related stress across occupations. J. Manag. Psychol. 2005, 20, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Haynes, N.S.; Love, P.E.D. Psychological adjustment and coping among construction project managers. Constr. Manag. Econ. 2004, 22, 129–140. [Google Scholar] [CrossRef]
- Cooper, C.L. Group training for individual and organizational development. Interpers. Dev. 1972, 3, 174. [Google Scholar]
- Ng, S.T.; Skitmore, R.M.; Leung, T.K.C. Manageability of stress among construction project participants. Eng. Constr. Archit. Manag. 2005, 12, 264–282. [Google Scholar] [CrossRef] [Green Version]
- French, J.R.; Caplan, R.D. Organizational stress and individual strain. Fail. Success 1972, 30, 66. [Google Scholar]
- Friedman, M.; Rosenman, R.H. Type A Behavior and Your Heart; Fawcett: Greenwich, CT, USA, 1974. [Google Scholar]
- Ganster, D.C. Type A Behavior and Occupational Stress. J. Organ. Behav. Manag. 1987, 8, 61–84. [Google Scholar] [CrossRef]
- Leung, M.Y.; Zhang, H.; Skitmore, M. Effects of organizational supports on the stress of construction estimation participants. J. Constr. Eng. Manag. 2008, 134, 84–93. [Google Scholar] [CrossRef]
- MacDonald, A.P. Internal-external locus of control. In Measures of Social Psychological Attitudes; Robinson, J.P., Shaver, P.R., Eds.; Institute for Social Research, The University of Michigan: Ann Arbor, MI, USA, 1973. [Google Scholar]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Sycholog. Monogr. Gen. Appl. Adhes. Sci. 1966, 80, 1. [Google Scholar] [CrossRef] [Green Version]
- Hendrix, W.H.; Ovalle, N.K.; Troxler, R.G. Behavioral and physiological consequences of stress and its antecedent factors. J. Appl. Psychol. 1985, 70, 188. [Google Scholar] [CrossRef]
- Kamardeen, I.; Sunindijo, R.Y. Personal Characteristics Moderate Work Stress in Construction Professionals. J. Constr. Eng. Manag. 2017, 143, 04017072. [Google Scholar] [CrossRef]
- Riedel, J.; Wiesmann, U.; Hannich, H.-J. An integrative theoretical framework of acculturation and salutogenesis. Int. Rev. Psychiatry 2011, 23, 555–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, J.W.; Kim, U.; Minde, T.; Mok, D. Comparative studies of acculturative stress. Int. Migr. Rev. 1987, 21, 491–511. [Google Scholar] [CrossRef]
- Joiner, T.E., Jr.; Walker, R.L. Construct validity of a measure of acculturative stress in African Americans. Psychol. Assess. 2002, 14, 462. [Google Scholar] [CrossRef] [PubMed]
- Zvolensky, M.J.; Jardin, C.; Garey, L.; Robles, Z.; Sharp, C. Acculturative stress and experiential avoidance: Relations to depression, suicide, and anxiety symptoms among minority college students. Cogn. Behav. Ther. 2016, 45, 501–517. [Google Scholar] [CrossRef] [PubMed]
- Aveiga, F.; Valverde, O.; Jaselskis, E.J.; Strong, K.C. Integration-communications training for improving productivity and conflict resolution strategies among culture and language diverse construction sites. Int. J. Hum. Resour. Dev. Manage. 2011, 11, 16–37. [Google Scholar] [CrossRef]
- Matheny, K.B.; Aycock, D.W.; Pugh, J.L.; Curlette, W.L.; Silva Cannella, K.A. Stress coping: A qualitative and quantitative synthesis with implications for treatment. Couns. Psychol. 1986, 14, 499–549. [Google Scholar] [CrossRef]
- Freud, S. Civilization and Its Discontents. Standard Edition; Hogarth Press: London, UK, 1930; Volume 21, pp. 59–145. [Google Scholar]
- Freud, A. The Ego and the Mechanisms of Defense; International Universities Press: New York, NY, USA, 1946. [Google Scholar]
- Livneh, H.; Martz, E. An introduction to coping theory and research. In Coping with Chronic Illness and Disability; Springer: Boston, MA, USA, 2007; pp. 3–27. [Google Scholar]
- Menninger, K. Regulatory devices of the ego under major stress. Int. J. Psycho-Anal. 1954, 35, 412–420. [Google Scholar]
- Haan, N. Coping and Defending: Processes of Self-Environment; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Radnitz, C.L.; Tiersky, L. Psychodynamic and cognitive theories of coping. In Coping with Chronic Illness and Disability; Springer: Boston, MA, USA, 2007; pp. 29–48. [Google Scholar]
- Folkman, S.; Lazarus, R.S.; Dunkel-Schetter, C.; DeLongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Pers. Soc. Psychol. 1986, 50, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Launier, R. Stress-related transactions between person and environment. In Perspectives in Interactional Psychology; Springer: Boston, MA, USA, 1978; pp. 287–327. [Google Scholar]
- Pearlin, L.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [CrossRef] [Green Version]
- Moos, R.H. Coping with Physical Illness 2: New Perspectives; Plenum Press: New York, NY, USA, 1984. [Google Scholar]
- Endler, N.S. Stress, Anxiety and coping: The multidimensional interaction model. Can. Psychol. Psychol. Can. 1997, 38, 136–153. [Google Scholar] [CrossRef]
- Enshassi, A.; Al-Swaity, E.; Abdul Aziz, A.R.; Choudhry, R. Coping behaviors to deal with stress and stressor consequences among construction professionals: A case study at the Gaza Strip, Palestine. J. Financ. Manag. Prop. Constr. 2018, 23, 40–56. [Google Scholar] [CrossRef]
- Chan, I.Y.S.; Leung, M.Y.; Liang, Q. The roles of motivation and coping behaviours in managing stress: Qualitative interview study of Hong Kong expatriate construction professionals in mainland China. Int. J. Environ. Res. Public Health 2018, 15, 561. [Google Scholar] [CrossRef] [Green Version]
- Bowen, P.; Edwards, P.; Lingard, H.; Cattell, K. Workplace stress, stress effects, and coping mechanisms in the construction industry. J. Constr. Eng. Manag. 2014, 140, 04013059. [Google Scholar] [CrossRef]
- Wong, P.T.P.; Reker, G.T.; Peacock, E. The Resource-Congruence Model of Coping and the Development of the Coping Schemas Inventory; Springer: New York, NY, USA, 2006. [Google Scholar]
- Minchin, R.E., Jr.; Glagola, C.R.; Guo, K.; Languell, J.L. Case for drug testing of construction workers. J. Manag. Eng. 2006, 22, 43–50. [Google Scholar] [CrossRef]
- Greenglass, E.; Schwarzer, R.; Jakubiec, D.; Fiksenbaum, L.; Taubert, S. The proactive coping inventory (PCI): A multidimensional research instrument. In Proceedings of the 20th International Conference of the Stress and Anxiety Research Society (STAR), Cracow, Poland, 12–14 July 1999; p. 14. [Google Scholar]
- Schwarzer, R.; Knoll, N. Positive coping: Mastering demands and searching for meaning. In Handbook of Positive Psychological Assessment; American Psychological Association: Washington, DC, USA, 2003. [Google Scholar]
- Aspinwall, L.G.; Taylor, S.E. A stitch in time: Self-regulation and proactive coping. Psychol. Bull. 1997, 121, 417–436. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R. Manage stress at work through preventive and proactive coping. In The Blackwell Handbook of Principles of Organizational Behavior; Blackwell: Oxford, UK, 2000; pp. 342–355. [Google Scholar]
- Taylor, S.E.; Kemeny, M.E.; Reed, G.M.; Bower, J.E.; Gruenewald, T.L. Psychological resources, positive illusions, and health. Am. Psychol. 2000, 55, 99. [Google Scholar] [CrossRef] [PubMed]
- Uskul, A.K.; Greenglass, E. Psychological wellbeing in a Turkish-Canadian sample. Anxiety Stress Coping 2005, 18, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Cruz, J.P.; Cabrera, D.N.C.; Hufana, O.D.; Alquwez, N.; Almazan, J. Optimism, proactive coping and quality of life among nurses: A cross-sectional study. J. Clin. Nurs. 2018, 27, 2098–2108. [Google Scholar] [CrossRef]
- Starren, A.; Luijters, K.; Drupsteen, L.; Vilkevicius, G.; Stulginskis, A.; Eeckelaert, L.; Elsler, D. Diverse Cultures at Work: Ensuring Safety and Health through Leadership and Participation; European Agency for Safety and Health at Work: Bilbao, Spain, 2013. [Google Scholar]
- Deardorff, D.K. Identification and assessment of intercultural competence as a student outcome of internationalization. J. Stud. Int. Educ. 2006, 10, 241–266. [Google Scholar] [CrossRef]
- Gudykunst, W.B. Applying anxiety\uncertainty management (AUM) Theory to intercultural adjustment training. Int. J. Intercult. Relat. 1998, 22, 227–250. [Google Scholar] [CrossRef]
- Lloyd, S.; Hartel, C. Intercultural competencies for culturally diverse work teams. J. Manag. Psychol. 2010, 25, 845–875. [Google Scholar] [CrossRef]
- Gudykunst, W.B.; Kim, Y.Y. Communicating with Strangers: An Approach to Intercultural Communication; McGraw-Hill: New York, NY, USA, 1997. [Google Scholar]
- Dodd, C. An introduction to intercultural effectiveness skills. In Intercultural Skills for Multicultural Societies; SIETAR International: Washington, DC, USA, 1987; pp. 3–12. [Google Scholar]
- Ayoko, O.B.; Härtel, C.E. Cultural differences at work: How managers deepen or lessen the cross-racial divide in their workgroups. Qld. Rev. 2000, 7, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Torres, L.; Rollock, D. Acculturation and depression among Hispanics: The moderating effect of intercultural competence. Cult. Divers. Ethn. Minor. Psychol. 2007, 13, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [Green Version]
- LaMontagne, A.D.; Martin, A.; Page, K.M.; Reavley, N.J.; Noblet, A.J.; Milner, A.J.; Keegel, T.; Smith, P.M. Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry 2014, 14, 131. [Google Scholar] [CrossRef] [Green Version]
- LaFromboise, T.; Coleman, H.L.; Gerton, J. Psychological impact of biculturalism: Evidence and theory. Psychol. Bull. 1993, 114, 395. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Major Stressors | Key Sub-Factors | Authors |
|---|---|---|
| Work stressors | Factors intrinsic to a job (work overload/work overtime) Role in organization (role conflict/role ambiguity) Career development (job insecurity/under promotion) Relationships at work (with co-workers/managers/subordinates) Organizational structure and climate (involvement in the job/organizational rules and procedures) | Cooper and Marshall [37]; Yip et al. [38]; Campbell [4]; Love et al. [14]; Sang et al. [39]; Tijani et al. [40]; Leung et al. [35]; Sunindijo and Kamardeen [15]; Leung et al. [41]; Cheng et al. [42]; Leung et al. [43]; Joiner [44]. |
| Personal stressors | Behavior pattern of an individual (Type A and Type B behaviors) Locus of control (external and internal locus of control) Family problems Financial difficulties | Leung et al. [45]; Tijani et al. [40]; Leung and Chan [46]; Loosemore and Lam [47]; Chan et al. [48]; Liang et al. [49]; Al-Maskari et al. [50]. |
| Cultural stressors | Racial discrimination Language barriers Cultural value conflicts | Wu et al. [51]; Chan et al. [52]; Wong and Lin [53]; Loosemore et al. [54]; Ling et al. [55]. |
| Classifications of Intercultural Competence [100,102] | Definition | Competences [102] |
|---|---|---|
| Affective competence (Attitudes) | Attitudes, feelings, and personality traits that a person owns in terms of specific cultures and people with whom they interact [103] | Dissimilarity openness Tolerance for ambiguity Cultural empathy |
| Behavioral competence (Skills) | Skills for stressful situations in intercultural interactions [104] | Intercultural communication competence Emotion management skills Conflict management skills |
| Cognitive competence (Knowledge) | Abilities to perceive and understand information [104] | Cognitive complexity Goal orientation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Q.; Feng, Y.; London, K. Theorizing to Improve Mental Health in Multicultural Construction Industries: An Intercultural Coping Model. Buildings 2021, 11, 662. https://doi.org/10.3390/buildings11120662
Liu Q, Feng Y, London K. Theorizing to Improve Mental Health in Multicultural Construction Industries: An Intercultural Coping Model. Buildings. 2021; 11(12):662. https://doi.org/10.3390/buildings11120662
Chicago/Turabian StyleLiu, Qinjun, Yingbin Feng, and Kerry London. 2021. "Theorizing to Improve Mental Health in Multicultural Construction Industries: An Intercultural Coping Model" Buildings 11, no. 12: 662. https://doi.org/10.3390/buildings11120662