Evaluation of the Impact of the Envelope System on Thermal Energy Demand in Hospital Buildings


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Selection of a Representative Case of Study and Building Description
2.2. Methods—Monitoring Process
2.3. Simulation
3. Results and Discussion
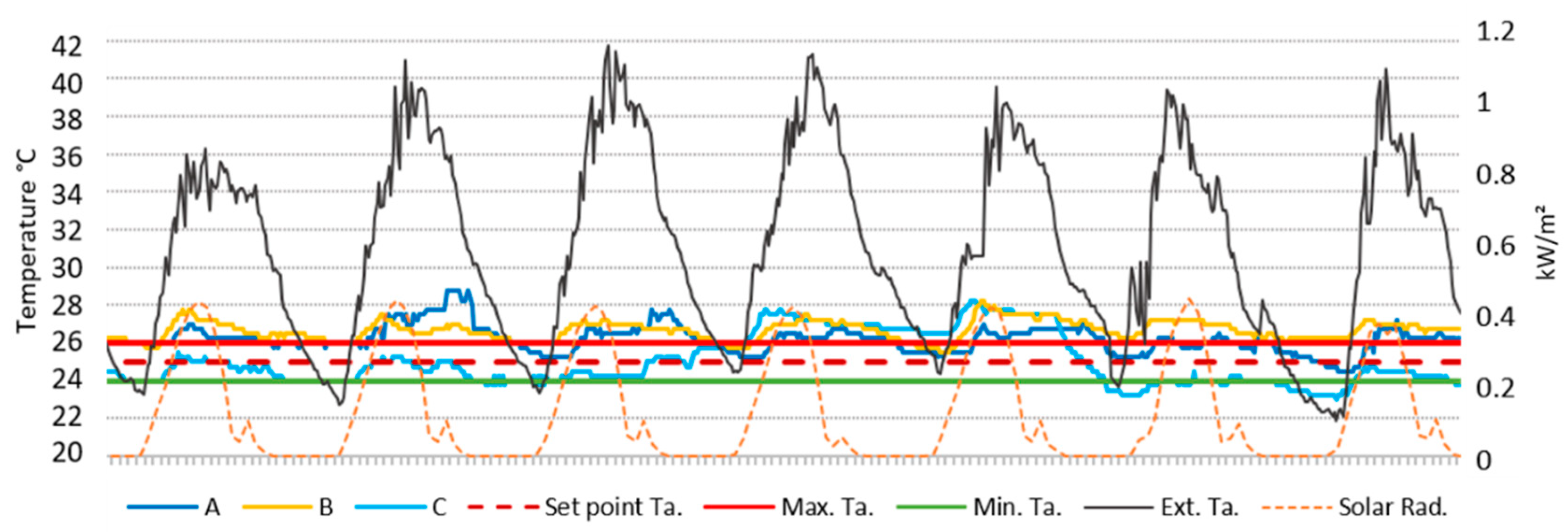
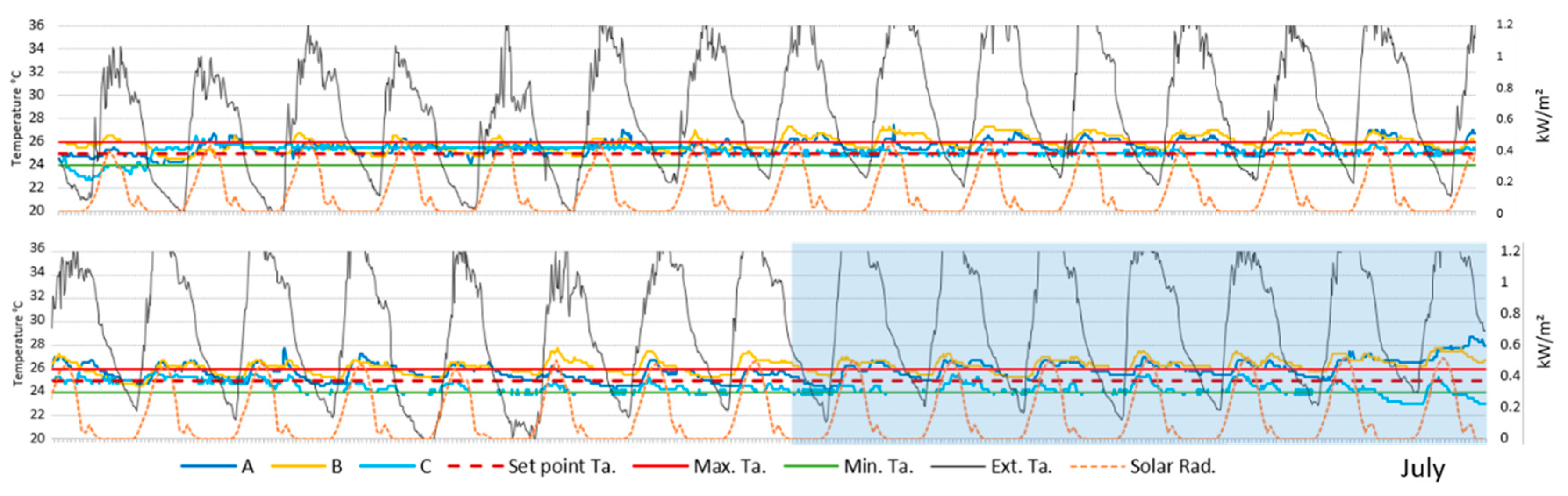
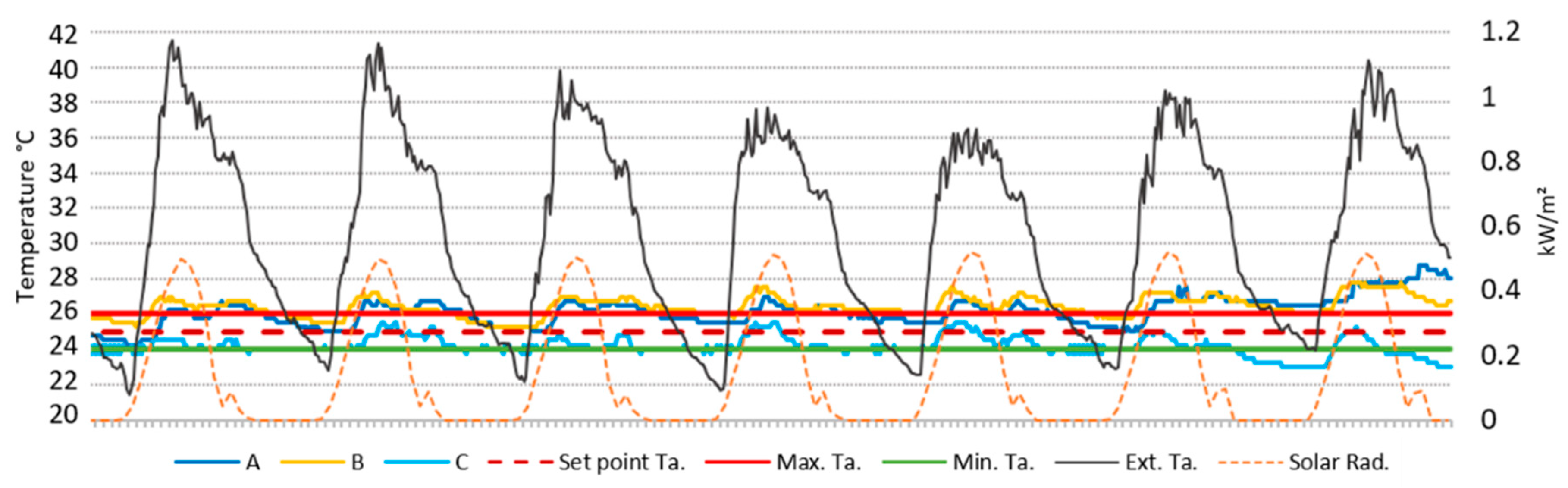
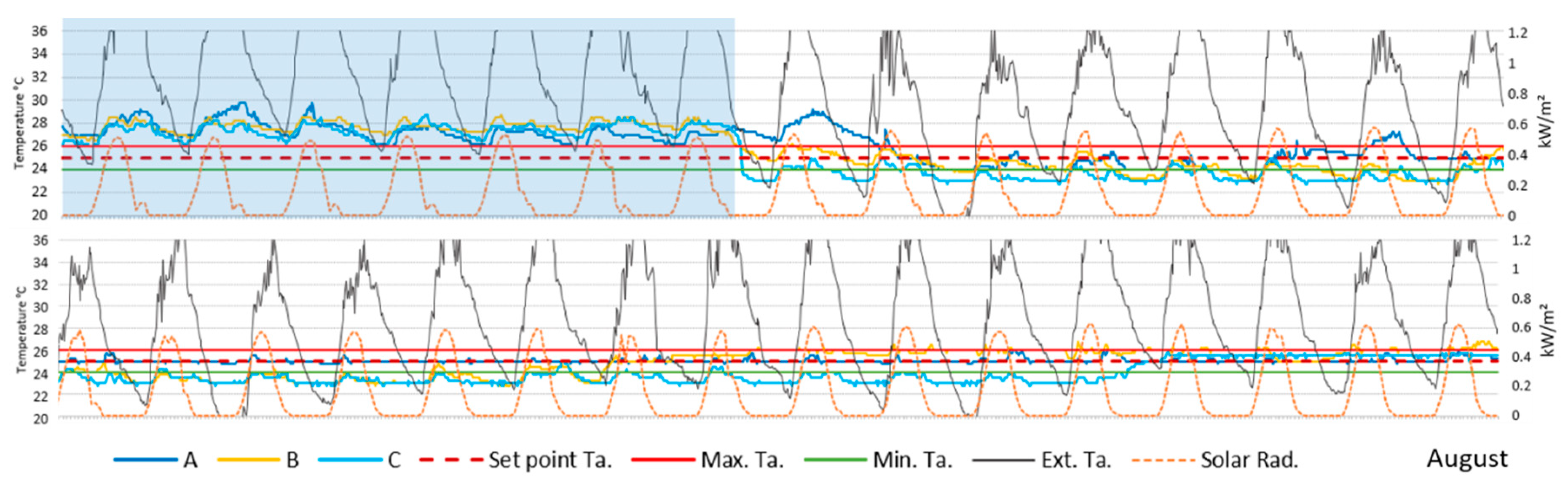
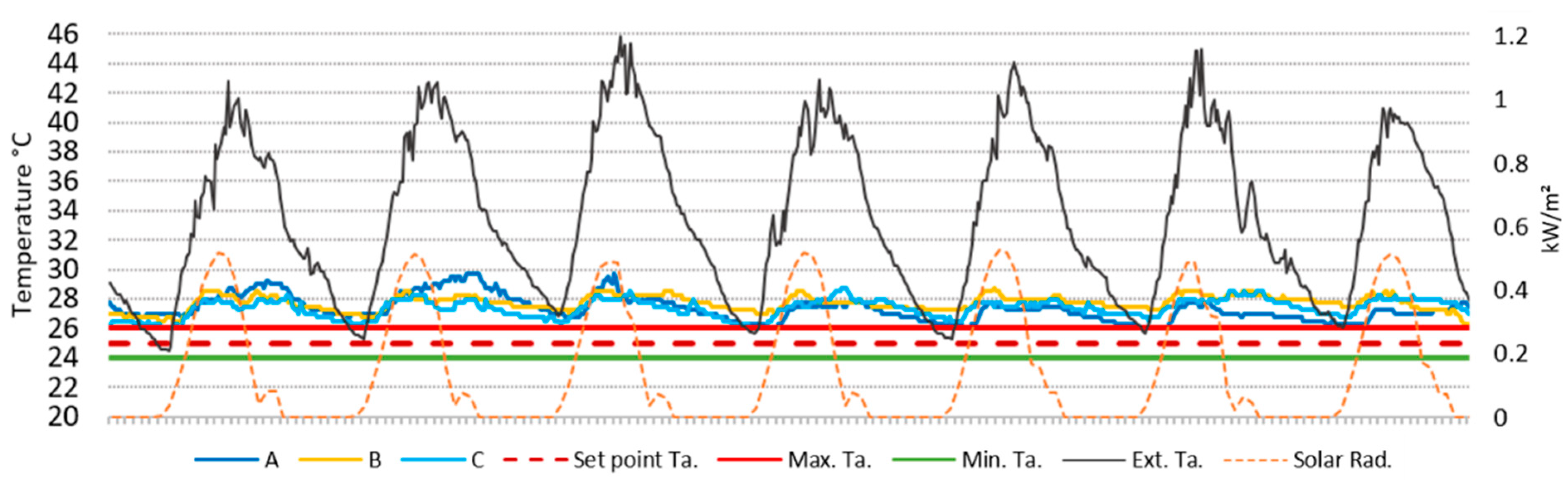
3.1. Measurements Results
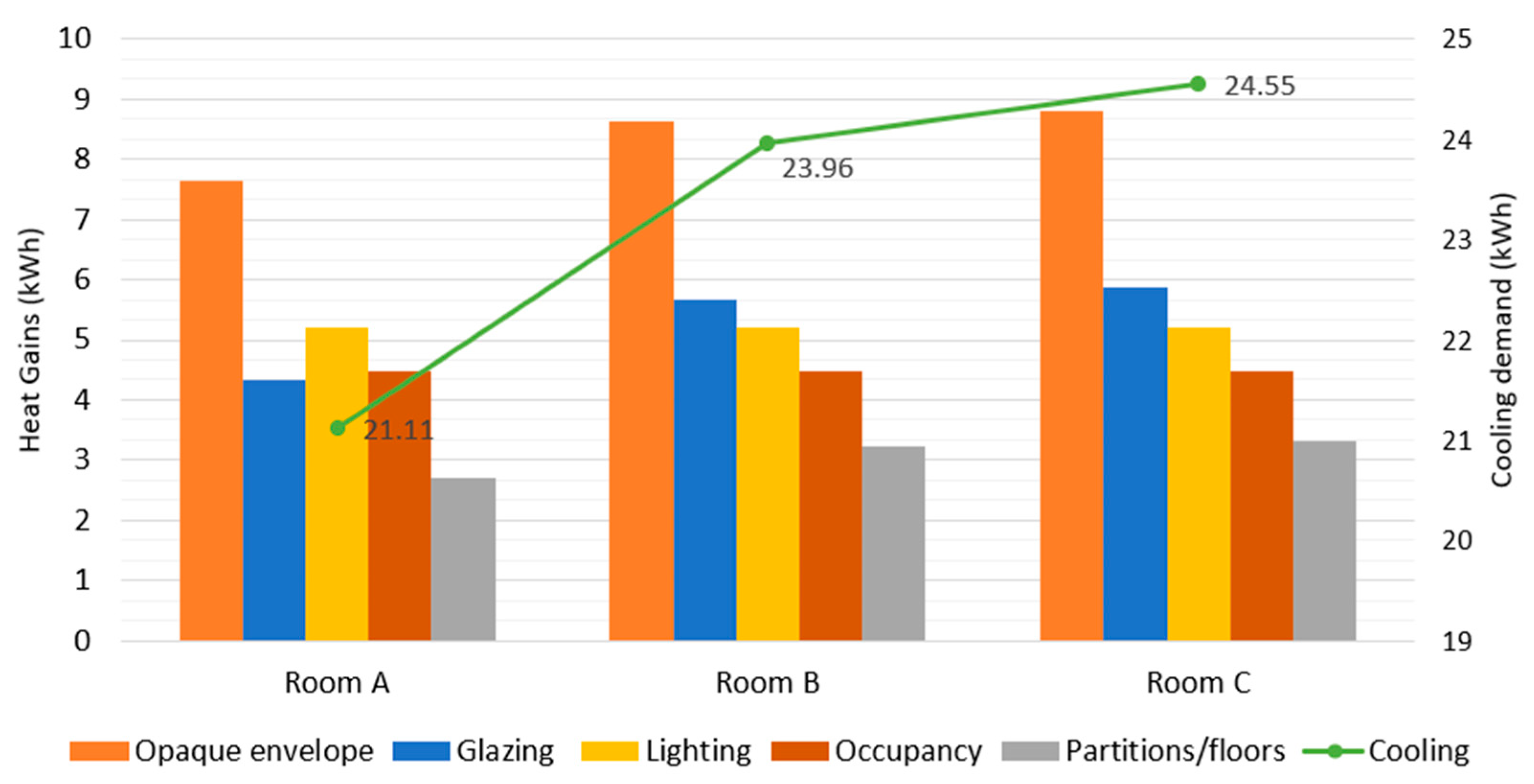
3.2. Simulation Results
4. Conclusions and Future Work
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2014: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014. [Google Scholar]
- Allen, M.R.; Dube, O.P.; Solecki, W.; Aragon-Durand, F.; Cramer, W.; Humphreys, S.; Zickfeld, K. Framing and Context in: Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C Above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; Technical Report; IPCC: Geneva, Switzerland, 2018. [Google Scholar]
- Climate Signals. European Heat Wave. 2003. Available online: https://www.climatesignals.org/events/european-heat-wave-2003 (accessed on 16 June 2020).
- Meehl, G.A.; Tebaldi, C. More Intense, More Frequent, and Longer Lasting Heat Waves in the 21st Century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [Green Version]
- Dong, B.; Sutton, R.; Shaffrey, L.; Wilcox, L. The 2015 European Heat Wave. Bull. Am. Meteorol. Soc. 2016, 97, 57–62. [Google Scholar] [CrossRef]
- Black, E.; Blackburn, M.; Harrison, G.; Hoskins, B.; Methven, J. Factors contributing to the summer 2003 European heatwave. Weather 2004, 59, 217–223. [Google Scholar] [CrossRef]
- Habeeb, D.; Vargo, J.; Stone, B. Rising heat wave trends in large US cities. Nat. Hazards 2015, 76, 1651–1665. [Google Scholar] [CrossRef]
- Hardin, A.W.; Liu, Y.; Cao, G.; Vanos, J.K. Urban heat island intensity and spatial variability by synoptic weather type in the northeast U.S. Urban Clim. 2018, 24, 747–762. [Google Scholar] [CrossRef]
- He, B. Potentials of meteorological characteristics and synoptic conditions to mitigate urban heat island effects. Urban Clim. 2018, 24, 26–33. [Google Scholar] [CrossRef]
- The European Espace Agency. Urban Heat Island and Urban Thermography; Techical Report I, DUE (Data User Element); ESA: Bari, Italy, 2011. [Google Scholar]
- Fernández García, F.; Allende Álvarez, F.; Alcaide Muñoz, J.; Rasilla Álvarez, D.; Martilli, A. Estudio de Detalle del Clima Urbano de Madrid; Área de Gobierno de Medio Ambiente y Movilidad, Ayuntamiento de Madrid: Madrid, Spain, 2016. [Google Scholar]
- Ward, K.; Lauf, S.; Kleinschmit, B.; Endlicher, W. Heat waves and urban heat islands in Europe: A review of relevant drivers. Sci. Total Environ. 2016, 569–570, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Martin-Vide, J.; Moreno-Garcia, M.C. Probability values for the intensity of Barcelona’s urban heat island (Spain). Atmos. Res. 2020, 240, 104–877. [Google Scholar] [CrossRef]
- Yagüe, C.; Zurita, E.; Martinez, A. Statistical analysis of the Madrid urban heat island. Atmos. Environment. Part B. Urban Atmos. 1991, 25, 327–332. [Google Scholar] [CrossRef]
- Núñez Peiró, M.; Román López, E.; Sánchez-Guevara Sánchez, C.; Neila González, F. Towards a Dynamic Model for the Urban Heat Island of Madrid. An. Edif. 2016, 2, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Oudin Åström, D.; Bertil, F.; Joacim, R. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Phung, D.; Thai, P.K.; Guo, Y.; Morawska, L.; Rutherford, S.; Chu, C. Ambient temperature and risk of cardiovascular hospitalization: An updated systematic review and meta-analysis. Sci. Total Environ. 2016, 550, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Ormandy, D.; Ezratty, V. Health and thermal comfort: From WHO guidance to housing strategies. Energy Policy 2012, 49, 116–121. [Google Scholar] [CrossRef]
- Xiong, J.; Lian, Z.; Zhou, X.; You, J.; Lin, Y. Effects of temperature steps on human health and thermal comfort. Build. Environ. 2015, 94, 144–154. [Google Scholar] [CrossRef]
- Mapped: How Climate Change Affects Extreme Weather around the World. Available online: https://www.carbonbrief.org/mapped-how-climate-change-affects-extreme-weather-around-the-world (accessed on 9 June 2020).
- World Meteorological Organization and World Health Organization Heatwaves and Health. Guidance on Warning System-Development; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Barriopedro, D.; Sousa, P.M.; Trigo, R.M.; García-Herrera, R.; Ramos, A.M. The Exceptional Iberian Heatwave of Summer 2018. Bull. Am. Meteor. Soc. 2020, 101, S29–S34. [Google Scholar] [CrossRef] [Green Version]
- Herring, S.C.; Hoell, A.; Hoerling, M.P.; Kossin, J.P.; Schreck, C.J., III; Stott, P.A. Explaining Extreme Events of 2015 from a Climate Perspective. Bull. Am. Meteor. Soc. 2017, 97, S57–S62. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.; Davies, M.; Mavrogianni, A.; Shrubsole, C.; Hamilton, I.; Das, P.; Jones, B.; Oikonomou, E.; Biddulph, P. Mapping indoor overheating and air pollution risk modification across Great Britain: A modelling study. Build. Environ. 2016, 99, 1–12. [Google Scholar] [CrossRef]
- Pyrgou, A.; Castaldo, V.L.; Pisello, A.L.; Cotana, F.; Santamouris, M. On the effect of summer heatwaves and urban overheating on building thermal-energy performance in central Italy. Sustain. Cities Soc. 2017, 28, 187–200. [Google Scholar] [CrossRef]
- European Commission. Consumption of non-Residential Buildings per m² (Normal Climate). Available online: https://ec.europa.eu/energy/content/energy-consumption-m%C2%B2-2_en (accessed on 18 August 2020).
- Ma, H.; Lu, W.; Yin, L.; Shen, X. Public Building Energy Consumption Level and Influencing Factors in Tianjin. Energy Procedia 2016, 88, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Verheyen, J.; Theys, N.; Allonsius, L.; Descamps, F. Thermal comfort of patients: Objective and subjective measurements in patient rooms of a Belgian healthcare facility. Build. Environ. 2011, 46, 1195–1204. [Google Scholar] [CrossRef]
- Pourshaghaghy, A.; Omidvari, M. Examination of thermal comfort in a hospital using PMV–PPD model. Appl. Ergon. 2012, 43, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Sattayakorn, S.; Ichinose, M.; Sasaki, R. Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals. Energy Build. 2017, 149, 45–57. [Google Scholar] [CrossRef]
- Alotaibi, B.S.; Lo, S.; Southwood, E.; Coley, D. Evaluating the suitability of standard thermal comfort approaches for hospital patients in air-conditioned environments in hot climates. Build. Environ. 2020, 169, 106561. [Google Scholar] [CrossRef]
- Spanish Association for Standardization and Certification (AENOR) Air Conditioning Installations in Hospitals; AENOR: Madrid, Spain, 2005.
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Energy Build. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Azizpour, F.; Moghimi, S.; Salleh, E.; Mat, S.; Lim, C.H.; Sopian, K. Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of University Kebangsaan Malaysia Medical Centre (UKMMC). Energy Build. 2013, 64, 317–322. [Google Scholar] [CrossRef]
- Quiroga, A.; Chattas, G.; Gil, A.; Ramírez, M.; Montes, M.T.; Iglesias, A.; Plasencia, J.; López, I.; Carrera, B. Practical Guide to Thermoregulation in Newborns; SIBEN: Buenos Aires, Argentina, 2010. [Google Scholar]
- Knobel, R.; Guenther, B.D.; Rice, H.E. Thermoregulation and thermography in neonatal physiology and disease. Biol. Res. Nurs. 2011, 13, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Lubkowska, A.; Szymański, S.; Chudecka, M. Surface Body Temperature of Full-Term Healthy Newborns Immediately after Birth-Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 1312. [Google Scholar] [CrossRef] [Green Version]
- Kakkad, K.; Barzaga, M.L.; Wallenstein, S.; Shah Azhar, G.; Sheffield, P.E. Neonates in Ahmedabad, India, during the 2010 Heat Wave: A Climate Change Adaptation Study. J. Environ. Public Health 2014, 2014, 8. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Maternal and Newborn Health/Safe Motherhood Thermal Protection of the Newborn: A Practical Guide; WHO: Geneva, Switzerland, 1997; pp. 11–64. [Google Scholar]
- Jia, Y.S.; Lin, Z.L.; Lv, H.; Li, Y.M.; Green, R.; Lin, J. Effect of delivery room temperature on the admission temperature of premature infants: A randomized controlled trial. J. Perinalology 2013, 33, 264–267. [Google Scholar] [CrossRef] [Green Version]
- ASHRAE. Handbook for HVAC Applications in Health Care Facilities; ASHRAE: Atlanta, GA, USA, 2019; Charpter 9; pp. 1–20. [Google Scholar]
- Number of Public Hospitals in Spain from 2000 to 2017. Available online: https://www.statista.com/statistics/557228/publicly-owned-hospitals-in-spain/ (accessed on 20 August 2020).
- McKelvey, D.; Foster, K.; Copley, D.; Wilson, A. Overcladding for Thermal Performance and Building Resiliency, Thermal Performance of the Exterior Envelopes of Whole Buildings; American Society of Heating, Refrigeration, and Air-Conditioning Engineers (ASHRAE): Miami, FL, USA, 2016. [Google Scholar]
- Kandya, A.; Mohan, M. Mitigating the Urban Heat Island effect through building envelope modifications. Energy Build. 2018, 164, 266–277. [Google Scholar] [CrossRef]
- MODIFICA Project. Predictive Model of the Behavior of Residential Buildings under the Effects of the Madrid Heat Island. Available online: http://abio-upm.org/project/modifica/ (accessed on 26 August 2020).
- Terés-Zubiaga, J.; Escudero, C.; García-Gafaro, C.; Sala, J.M. Methodology for evaluating the energy renovation effects on the thermal performance of social housing buildings: Monitoring study and grey box model development. Energy Build. 2015, 102, 390–405. [Google Scholar] [CrossRef]
- Cuce, P.M.; Cuce, E. Toward cost-effective and energy-efficient heat recovery systems in buildings: Thermal performance monitoring. Energy 2017, 137, 487–494. [Google Scholar] [CrossRef]
- Madsen, H.; Holst, J. Estimation of continuous-time models for the heat dynamics of a building. Energy Build. 1995, 22, 67–79. [Google Scholar] [CrossRef]
- SIEMENS Building Technology DESIGO-INSIGHT Building Automation & Control System; Zug, Switzerland, 2004.
- Spanish Association of Standardization and Certification (AENOR) UNE-EN 62974-1 Monitoring and Measuring Systems Used for Data Collection, Gathering and Analysis-Part 1: Device Requirements; AENOR: Madrid, Spain, 2017.
- Big Ladder Software. Available online: https://bigladdersoftware.com/epx/docs/8-0/engineering-reference/page-021.html (accessed on October 2020).
- Spain Ministry of Development Regulations of Technical Building Code (CTE). Energy Saving Regulations in Buildings (HE); HE-1; Spain Ministry of Development Regulations of Technical Building Code: Madrid, Spain, 2017. [Google Scholar]
- Spain Ministry of Industry. Tourism and Commerce in collaboration with the Ministry of Housing Thermal Installations in Buildings (RITE); IT 1.2.4.5; Spain Ministry of Industry: Madrid, Spain, 2013. [Google Scholar]
- AHSRAE 90.I Standard; Energy Standards for Buildings except Low-Rise Residential Buildings; ASHRAE: Atlanta, GA, USA, 2010.
- Brás, A.; Rocha, A.; Faustino, P. Integrated approach for school buildings rehabilitation in a Portuguese city and analysis of suitable third party financing solutions in EU. J. Build. Eng. 2015, 3, 79–93. [Google Scholar] [CrossRef]
- Freewan, A. Advances in Passive Cooling Design: An Integrated Design Approach. In Zero and Net Zero Energy; Hailu, G., Ed.; IntechOpen: London, UK, 2019; pp. 187–211. [Google Scholar]
- Aguirre Piña, A.L. Indoor thermal effects of different wall configurations in warm humid climates. In Passive and Low Energy Ecotechniques; Bowen, A., Ed.; Pergamon, Turkey, 1985; pp. 988–993. [Google Scholar]
- Wu, S. 4-Heat energy storage and cooling in buildings. In Materials for Energy Efficiency and Thermal Comfort in Buildings; Hall, M.R., Ed.; Woodhead Publishing: Cambridge, UK, 2010; pp. 101–126. [Google Scholar]
- State Meteorological Agency of Spain (AEMET). Weather Summary-Summer 2018; AEMET: Madrid, Spain, 2018. [Google Scholar]
- Hwang, R.; Lin, T.; Lin, F. Evaluation and mapping of building overheating risk and air conditioning use due to the urban heat island effect. J. Build. Eng. 2020, 32, 101726. [Google Scholar] [CrossRef]
- Kendrick, C.; Ogden, R.; Wang, X.; Baiche, B. Thermal mass in new build UK housing: A comparison of structural systems in a future weather scenario. Energy Build. 2012, 48, 40–49. [Google Scholar] [CrossRef]
- Rodriguez, C.M.; D’Alessandro, M. Indoor thermal comfort review: The tropics as the next frontier. Urban Clim. 2019, 29, 100488. [Google Scholar] [CrossRef]
- Elias-Ozkan, S.; Summers, F.; Surmeli, N.; Yannas, S. A Comparative study of the thermal performance of building materials. In Proceedings of the 23rd Conference on Passive and Low Energy Architecture (PLEA), Geneva, Switzerland, 6–8 September 2006. [Google Scholar]
- Ding, Y.; Wang, Z.; Feng, W.; Marnay, C.; Zhou, N. Influence of occupancy-oriented interior cooling load on building cooling load design. Appl. Therm. Eng. 2016, 96, 411–420. [Google Scholar] [CrossRef]
- Yang, Z.; Becerik-Gerber, B. How Does Building Occupancy Influence Energy Efficiency of HVAC Systems? Energy Procedia 2016, 88, 775–780. [Google Scholar] [CrossRef] [Green Version]
- Pacific Northwest National Laboratory. The Influence of Occupancy on Building Energy use Intensity and the Utility of an Occupancy-Adjusted Performance Metric; Pacific Northwest National Laboratory: Richland, WA, USA, 2017. [Google Scholar]
- Shafiee, E.; Faizi, M.; Yazdanfar, S.; Khanmohammadi, M. Assessment of the effect of living wall systems on the improvement of the urban heat island phenomenon. Build. Environ. 2020, 181, 106923. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inputs | Newborn Patient Rooms A, B, C |
|---|---|
| Setpoint temperature | Cooling 26 °C/Heating 24 °C |
| RH% | Humidification 40%/Dehumidification 60% |
| ACPH | 2.7 |
| Workday profile (h) | 0:00–24:00 Mon–Sun |
| Occupancy density (p/m2) | 0.10 |
| Occupancy schedule (h) | 9:00–21:00, 80% Occup. Rate |
| 22:00–8:00, 50% Occup. Rate | |
| Occupancy heat gain (W/M2) | Sens. 63 Lat. 52 |
| Lighting heat gain (W/m2) | 7 |
| Illuminance (lx) | 500 |
| Element | Construction System | U Factor W/(m2)K |
|---|---|---|
| E1. Façade wall |  | 0.42 |
| E2. Flat roof |  | 0.52 |
| E3. Floor |  | 0.47 |
| E4. Ground floor |  | 0.52 |
| Wall/Window Area | Total | North | East | South | West | Rooms (A B C)/East |
|---|---|---|---|---|---|---|
| Wall (m2) | 16,446.06 | 3869.33 | 44,222.78 | 3775.4 | 4378.55 | 13 |
| Window opening (m2) | 4500.17 | 1266.5 | 1070.3 | 1031.96 | 1131.41 | 3.25 |
| Window-Wall Ratio (%) | 27 | 33 | 24 | 27 | 26 | 25 |
| Heat Source | Room A (kWh/Day) | Room B (kWh/Day) | Room C (kWh/Day) |
|---|---|---|---|
| Walls | 5.24 | 6.12 | 6.23 |
| Glazing | 4.32 | 5.68 | 5.88 |
| Solar gains | 1.43 | 2.11 | 2.19 |
| Roof | 2.41 | 2.52 | 2.58 |
| Partitions | 1.16 | 1.34 | 1.35 |
| Floor | 1.56 | 1.90 | 1.97 |
| Light | 5.21 | 5.21 | 5.21 |
| Occupancy | 4.47 | 4.47 | 4.47 |
| Cooling demand | 21.11 | 23.96 | 24.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez Mejía, K.; Barbero-Barrera, M.d.M.; Rodríguez Pérez, M. Evaluation of the Impact of the Envelope System on Thermal Energy Demand in Hospital Buildings. Buildings 2020, 10, 250. https://doi.org/10.3390/buildings10120250
Jiménez Mejía K, Barbero-Barrera MdM, Rodríguez Pérez M. Evaluation of the Impact of the Envelope System on Thermal Energy Demand in Hospital Buildings. Buildings. 2020; 10(12):250. https://doi.org/10.3390/buildings10120250
Chicago/Turabian StyleJiménez Mejía, Katia, María del Mar Barbero-Barrera, and Manuel Rodríguez Pérez. 2020. "Evaluation of the Impact of the Envelope System on Thermal Energy Demand in Hospital Buildings" Buildings 10, no. 12: 250. https://doi.org/10.3390/buildings10120250