2. Materials and Methods
The study was reviewed and approved by the Institutional Review Board (No. 01/14) and was conducted in accordance with the declaration of Helsinki at the Orthodontic Department Healthcare Centre. Informed consent approval was obtained from each patient or their parents.
Inclusion criteria were growing patients with bilateral Class II malocclusion (ANB > 4°) due to mandibular retrognathia (SNB < 78°) with overjet (>4 mm) and deep bite (>4 mm), with no previous orthodontic treatment. Patients with developmental syndromes and anomalies (alveolar cleft and/or palate), mandibular fracture or deformities were also excluded from the study. A Class II malocclusion due to retrognathic mandible was identified through cephalographic analysis, so before-treatment (T0) and after-treatment (T1) lateral cephalograms (LC) were mandatory for all the patients. All lateral cephalograms (LC) were taken using the same equipment (Planmeca Promax, Helsinki, Finland) by an experienced dental radiology engineer under standard conditions: subjects were in the standing position and adequately protected, the Frankfort horizontal plane parallel to the floor, with the teeth in the maximal intercuspation (centric occlusion) and relaxed lips and tongue and with identical distances for each patient from the focus to the median sagittal plane of the subject’s head and to the film. Cephalometric analysis was performed for each patient before (T0) and after (T1) treatment. Definitions of the used (clinically important) angular and linear measurements are described and shown in
Figure 1 and
Figure 2. The linear and angular measurements were measured to the nearest of 0.1 mm and 0.1 degrees, respectively. Only the data with statistically significant changes before and after treatment are presented.
Legends: SNB: the angle formed between the SN plane and the point B indicates the relationship of the mandibular basal arch to the anterior cranial base; SNPg: the angle formed between the SN plane and the point Pg; ANB: the difference between SNA and SNB angle relates jaws to anterior cranial base; Wits appraisal: linear distance between the projecting points A and B perpendicular on the functional occlusal plane (AO and BO) indicates the skeletal sagittal jaw relationship; Gonial angle: the angle between the posterior tangent line of the ramus and the mandibular plane; LAFH: Lower anterior face height is the distance between points Sna and Me; CoGn: the linear distance between the condylion and the gnathion points indicates the mandibular length.
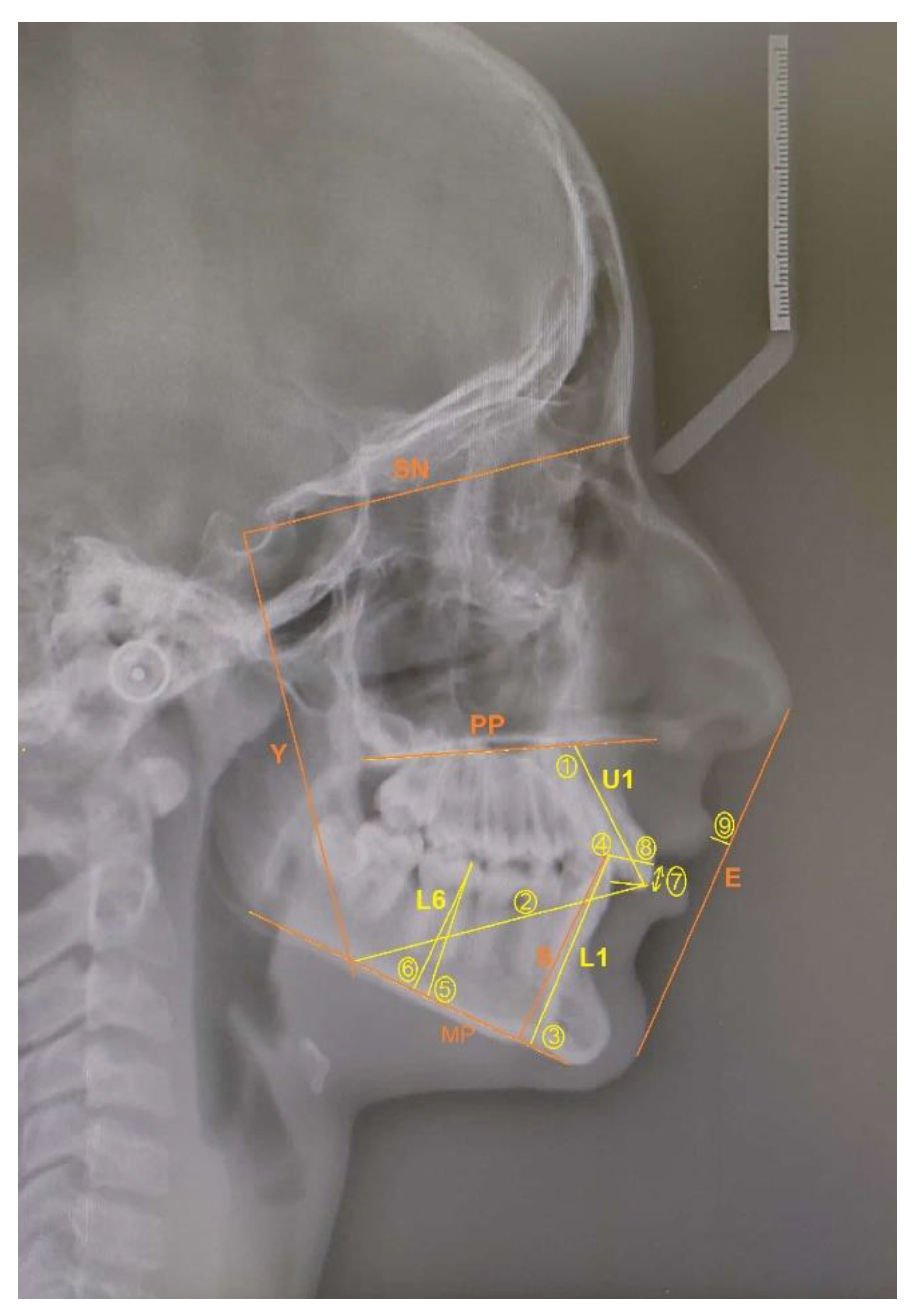
Legends: 1: U1/PP (°) is the angle formed between the maxillary central incisor (U1) long axis and the palatal plane (PP) and indicates maxillary incisor inclination; 2: U1/Y axis (mm) is the distance between the incisal edge of maxillary central incisor perpendicular to the Y axis (formed by dropping a line from the sella perpendicular to the SN line) indicates horizontal maxillary incisor distance; 3: L1/MP (°) is the angle formed between the mandibular central incisor (L1) long axis and the mandible plane (MP) and indicates mandibular incisor inclination; 4: L1/S axis (mm) is the distance between the incisal edge of the mandibular central incisor perpendicular to the S axis (formed by dropping a line through the posterior conture of symphysis perpendicular to the MP line) and indicates horizontal mandibular incisor distance to S axis; 5: L6/MP (°) is the angle between the mandibular first molar (L6) long axis (line passing through the mesial cusp tip and the mesial root tip) and the mandibular plane, and indicates mandibular first molar inclination; 6: L6/MP (mm) is the distance between the mesial cusp tip of the mandibular first molar perpendicular to the mandibular plane and indicates vertical mandibular first molar distance; 7: overjet is the horizontal distance from the maxillary incisor tip to the labial surface of the mandibular incisor; 8: overbite is the vertical distance from the mandibular incisor tip to the maxillary incisor tip; 9: U1/E line is the horizontal distance from the labial surface of the maxillary incisor perpendicular to the E line.
The fixed sagittal guidance (FSG) appliance is a fixed orthodontic appliance bonded on both upper molars, manufactured of a crown (cobalt-chromium alloy) and the occlusal inclined plane of SR Chromasit material (pressure/heat-curing micro filled veneer material) (
Figure 3). Crowns (
Figure 4) were produced using a scanner (to import physical data about the teeth into the computer) and 3D computer design and a specific method of selective laser melting (SLM) (MLab, Concept Laser, Treatstock, Newark, DE, USA) manufacturing technology (adding a layer on top of the layer) [
5]. Special small hooks were added to the crowns for bondage and safety of the appliance (
Figure 4). The inclination was oriented individually to the occlusal plane (angle), thereby actively guiding the mandible anteriorly during jaw closure; it was individually manufactured in a laboratory using an articulator. A construction wax bite was necessary in designing an inclined plane. In order to register the bite for FSG manufacturing, the patient was asked to close his/her mouth in proper sagittal and vertical dimensions. The inclination was adjusted in the laboratory on a case-to-case bias (depending on the severity of the Class II relationship, deep bite) [
11]. The vertical distance of the inclined plane was temporarily reflected in a posterior open bite which enabled easier leveling of the mandibular teeth and correction (flattening) of the curve of Spee. Additionally, all the patients were treated with the same 0.22˝ slot Roth prescription brackets (Dentaurum) and consistent straight (arch) wire sequencing (SWA) (
Figure 3). In leveling and aligning, the arch wire sequence was 0.012, 0.014, 0.018, 0.016 × 0.022, 0.018 × 0. 025 inch rectangular nickel-titanium wire. The FSG was placed at the same time as the fixed orthodontic straight-wire appliance (SWA) (
Figure 3).
Final skeletal and dentoalveolar results of the patients treated with FSG were compared with the same results of patients treated with intermaxillary Class II elastics (control group), who matched to the FSG group in age and initial cephalometric characteristics.
Statistical Analysis
Intra-operator error was evaluated by re-digitizing fifteen randomly selected cephalograms two weeks after initial digitization. Error analysis was performed using paired t-tests. Descriptive statistics (mean and standard deviation) for measurements before and after treatment were analyzed using the Statistical Package for Social Sciences version 10.0 (SPSS Inc., Chicago, IL, USA).
An independent t-test was used to compare cephalometric measurements before and after treatment within each group and paired t-test for comparison between groups. The level of significance tested was p < 0.05.
4. Discussion
Digitalization and additive manufacturing have opened many new perspectives in the field of personalized complex medical and dental implant production [
2,
3,
9,
10,
11,
12,
20,
21]. Individualized approach and custom-made implants offer attractive and seem to be almost unlimited options. On the other side we must be aware of concerns about quality and safety assurance control and regulation protocols, particularly in the very sensitive field of medical implants. As these issues seem to play a slightly less important role in temporarily and externally worn implants, the highest ethical and deontological standards should be respected, particularly in permanently inserted and implanted medical devices.
In orthodontics, many corrections can be achieved through the growing and maturation periods and with externally applied devices [
13,
14,
15,
16]. There’s a clear trend, if possible, to achieve similar orthodontic results, to perform this with more convenient and effective methods for patients [
21,
22]. Removable appliances, such as the Fränkel regulator, Bionator, Activator, Twin Block and Class II elastics are effective in the treatment of malocclusions, but often bring inconsistent results, due to the fact that they require high levels of patient’s cooperation [
23,
24,
25,
26]. The major advantage of fixed functional devices such as the Herbst, Jasper Jumper, MARA and Forsus Fatigue Resistant Device lies in their fixed and effective position for 24 h a day with a low impact of patient’s compliance [
23,
24,
25,
26,
27].
The FSG appliance, used in our study, was completely individually designed and fitted perfectly on the upper molars, so no additional correction was needed at the time of bonding; it provided guidance of mandible anteriorly and inferiorly, with the impact in the correction of the sagittal and vertical discrepancy in each closing of the jaw and what is supposed to induce a neuromuscular re-education, while correcting the Class II dentoskeletal relationship [
24]; this approach also prevents the teeth from occluding with antagonists and allows immediate use of a fixed orthodontic appliance in the lower arch, in contrast to for instance Class II elastics, that can be used only after completed alignment of teeth. FSG follows the principle of a bionator, which facilitates the eruption of mandibular posterior teeth by trimming of the acrylic [
23]. In FSG, temporarily achieved posterior teeth space (open bite) with leveling of the mandibular teeth and correction (flattening) of the curve of Spee with avoiding downward and back rotation of mandible, is provided by (individually) inclined plane on FSG.
The above-mentioned concept of treatment also seems to play a role in the reduction of the mean correction time with the appliances. Nelson et al. reported the mean correction time of dental relationship with Class II elastics to be between 6 months and 1.3 years [
28]. Uzel et al. reported about a reduction in the mean correction time of 8.5 ± 2.6 months using Class II elastics comparing with the mean correction time of 4.6 ±1.7 months, using the fixed Reciprocal Mini-Chin Cup (RMCC) appliance [
29]. The mean correction time in our patients, treated with the proposed FSG appliance, was not as short as in the report from Uzel et al. [
29] but comparable to that of Nelson et al. [
28] and there could be several reasons for that, including maturation stage (growing potential) of the patients with their cooperation and possible ability of neuromuscular re-education [
24,
27,
28,
30]; it should be stressed but that the proposed FSG appliance enabled immediate use of SWA, without waiting period, such as with the use of Class II elastics, that could be used only after completed alignment of teeth.
Effective treatment of Class II malocclusions should generate the skeletal (orthopedic) and dentoalveolar (orthodontic) effects; this concept with aligning of teeth and correction of malocclusion has been confirmed in the results of skeletal and dentoalveolar measurements in our study, too. According to several authors, Herbst appliance, Jasper Jumper, Forsus, FMA and intermaxillary elastics have a tendency to procline the mandibular incisors and effect on mandibular molar mesialisation [
26,
31,
32]. We found the mandibular incisor and molar in the FSG group to be statistically significant less proclined as in the control group. As the FSG has no influence on mandibular incisors proclination, such as elastics have, this appliance might be ideal in the situation of proclined mandibular incisors, where there is a great need to control incisor inclination. Similar results with retrusion of the mandibular incisor were reported by Ozbilek et al. [
33] and Celikoglu et al. [
34].
As the correction time in our study took more than a year, several factors in treatment should also be considered, such as the safety of the treatment and appliance, failure rate, patients’ compliance and the long-term results. With the proposed construction and bonding, there were no complications observed in the treatment of our patients, who all successfully finished the same protocol of treatment. Within the follow-up period of 2 years, there were no observed changes and no clinical, nor subjective worsening of the achieved results after finishing of the treatment.
Author Contributions
Conceptualization, methodology, investigation, data analyses, writing—original draft preparation, writing—review and editing, analysis, A.Č. and A.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Approved by the Institutional Review Board (No. 01/14).
Informed Consent Statement
Informed consent was obtained from all patients’ parents or patients included in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- ISO/ASTM 52900:2015; Standard Terminology for Additive Manufacturing-General Principles-Terminology. American National Standards Institute (ANSI): New York, NY, USA, 2015. Available online: www.astm.org (accessed on 13 August 2022).
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.O.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. B. Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Jimenez, M.; Romero, L.; Dominguez, I.A.; Espinosa, M.M.; Dominguez, M. Additive manufacturing technologies: An overview about 3D printing methods and future prospects. Complexity 2019, 1–30. [Google Scholar] [CrossRef]
- Khorasani, M.; Ghasemi, A.H.; Leary, M.; Sharabian, E.; Gibson, I.; Downing, D.; Bateman, M.; Rolfe, B. The effect of absorption ratio on meltpool features in laser-based powder bed fusion of IN718. Opt. Laser. Technol. 2022, 153, 108263. [Google Scholar] [CrossRef]
- Zhou, Y.; Abbara, E.M.; Jiang, D.; Azizi, A.; Poliks, M.M.; Ning, F. High-cycle fatigue properties of curved-surface AlSi10Mg parts fabricated by powder bed fusion additive manufacturing. Rapid. Prototyp. J. 2022, 28, 1346–1360. [Google Scholar] [CrossRef]
- Giganto, S.; Martinez-Pellitero, S.; Cuesta, E.; Zapico, P.; Joaquin, B. Proposal of design rules for improving the accuracy of Selective Laser Melting (SLM) manufacturing using benchmarks parts. Rapid. Prototyp. J. 2021, 28, 1129–1143. [Google Scholar] [CrossRef]
- Linares, J.M.; Chaves-Jacob, J.; Lopez, Q.; Sprauel, J.M. Fatigue life optimization for 17-4Ph steel produced by selective laser melting. Rapid. Prototyp. J. 2022, 28, 1182–1192. [Google Scholar] [CrossRef]
- Khan, H.M.; Waqar, S.; Koc, E. Evolution of temperature and residual stress behavior in selective laser melting of 316L stainless steel across a cooling channel. Rapid. Prototyp. J. 2021, 28, 1272–1283. [Google Scholar] [CrossRef]
- Fang, C.; Cai, H.; Kuong, E.; Chui, E.; Chuen Siu, Y.; Ji, T.; Drstvenšek, I. Surgical applications of three-dimensional printing in the pelvis and acetabulum: From models and tools to implants. Unfallchirurg 2019, 122, 278–285. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC. Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Fekonja, A.; Zupančič Hartner, T.; Čretnik, A. Mandibular retrognathia correction using a fixed sagittal guidance appliance individually manufactured by selective laser melting manufacturing technology. Rapid. Prototyping J. 2018, 24, 416–423. [Google Scholar] [CrossRef]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 62, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W., Jr.; Ackerman, J.L. (Eds.) Malocclusion and dentofacial deformity in contemporary society. In Contemporary Orthodontics, 6th ed.; Mosby: St. Louis, MO, USA, 2000; pp. 2–22. [Google Scholar]
- McNamara, J.A., Jr. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981, 51, 177–202. [Google Scholar]
- Tulloch, J.F.; Proffit, W.R.; Phillips, C. Outcomes in a 2-phase randomized clinical trial of early Class II treatment. Am. J. Orthod. Dentofacial. Orthop. 2004, 125, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Falck, F.; Fränkel, R. Clinical relevance of step-by-step mandibular advancement in the treatment of mandibular retrusion using the Fränkel appliance. Am. J. Orthod. Dentofacial. Orthop. 1989, 96, 333–341. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields, H.W., Jr.; Larson, B.E.; Sauer, D.M. Combined surgical and orthodontic treatment. In Contemporary Orthodontics, 6th ed.; Proffit, W.R., Fields, H.W., Jr., Ackerman, J.L., Eds.; Mosby: St. Louis, MO, USA, 2018; pp. 657–709. [Google Scholar]
- Graber, T.M.; Vanarsdall, R.L.J. Orthodontics: Current Principles and Techniques, 2nd ed.; Mosby Year Book: St. Louis, MO, USA, 1994; pp. 383–432. [Google Scholar]
- Sufia, N.R.; Sadat, S.M.A. Growth modification in Class II Malocclusion: A review. Update Dent. Coll. J. 2014, 4, 23–26. [Google Scholar] [CrossRef]
- Jevremović, D.; Kojić, V.; Bogdanović, G.; Puškar, T.; Eggbeer, D.; Thomas, D.; Williams, R. A selective laser melted Co–Cr alloy used for the rapid manufacture of removable partial denture frameworks—Initial screening of biocompatibility. J. Serb. Chem. Soci. 2011, 76, 43–52. [Google Scholar] [CrossRef]
- Marañón-Vásquez, G.A.; Barreto, L.S.C.; Pithon, M.M.; Nojima, L.I.; Nojima, M.C.G.; Araújo, M.T.S.; Souza, M.M.G. Reasons influencing the preferences of prospective patients and orthodontists for different orthodontic appliances. Korean. J. Orthod. 2021, 51, 115–125. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle. Orthod. 2014, 85, 881–889. [Google Scholar] [CrossRef]
- Neves, L.S.; Janson, G.; Cancado, R.H.; de Lima, K.J.; Fernandes, T.M.; Henriques, J.F. Treatment effects of the Jasper Jumper and the Bionator associated with fixed appliance. Prog. Orthod. 2014, 15, 54–59. [Google Scholar]
- Franchi, L.; Baccetti, T. Prediction of individual mandibular changes induced by functional jaw orthopedics followed by fixed appliances in Class II patients. Angle Orthod. 2006, 76, 950–954. [Google Scholar] [CrossRef]
- Sahm, G.; Bartsch, A.; Witt, E. Micro-electronic monitoring of functional appliance wear. Eur. J. Orthod. 1990, 12, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Weiland, F.J.; Ingervall, B.; Bantleon, H.P.; Droacht, H. Initial effects of treatment of Class II malocclusion with the Herren activator, activator-headgear combination and the Jasper Jumper. Am. J. Orthod. Dentofacial. Orthop. 1997, 11, 19–27. [Google Scholar] [CrossRef]
- Pancherz, H. A cephalometric analysis of skeletal and dental changes contributing to Class II correction in activator treatment. Am. J. Orthod. 1984, 85, 125–134. [Google Scholar] [CrossRef]
- Nelson, B.; Hansen, K.; Hägg, U. Overjet reduction and molar correction in fixed appliance treatment of Class II, division 1, malocclusions: Sagittal and vertical components. Am. J. Orthod. Dentofacial. Orthop. 1999, 115, 13–23. [Google Scholar] [CrossRef]
- Uzel, A.; Uzel, I.; Serdar Toroglu, M. Two different applications of Class II elastics with nonextraction segmental techniques. Angle Orthod. 2007, 77, 694–700. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; McNamara, J.A. The Cervical Vertebral Maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Sem. Orthod. 2005, 11, 119–129. [Google Scholar] [CrossRef]
- Kinzinger, G.S.; Lisson, J.A.; Frye, L.; Gross, U.; Hourfar, J. A retrospective cephalometric investigation of two fixed functional orthodontic appliances in class II treatment: Functional mandibular advancer vs. Herbst appliance. Clin. Oral. Investig. 2018, 22, 293–304. [Google Scholar] [CrossRef]
- Karacay, S.; Akin, E.; Olmez, H.; Gurton, A.U.; Sagdic, D. Forsus Nitinol Flat Spring and Jasper Jumper corrections of Class II division 1 malocclusions. Angle Orthod. 2006, 76, 666–672. [Google Scholar]
- Ozbilek, S.; Gungor, A.Y.; Celik, S. Effects of skeletally anchored Class II elastics: A pilot study and new approach for treating Class II malocclusion. Angle. Orthod. 2007, 87, 505–512. [Google Scholar] [CrossRef]
- Celikoglu, M.; Buyuk, S.K.; Ekizer, A.; Unal, T. Treatment effects of skeletally anchored Forsus FRD EZ and Herbst appliances: A retrospective clinical study. Angle. Orthod. 2016, 86, 306–314. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}