Determination of Risk Factors for Venous Thromboembolism by an Adapted Caprini Scoring System in Surgical Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Adapted Caprini Risk Scoring System
2.4. Study Procedure
2.5. Ethics Approval and Consent to Participate
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Data Availability
Conflicts of Interest
Abbreviations
| VTE | Venous thromboembolism |
| PE | Pulmonary embolism |
| CT | Computed tomography scan |
| MRI | Magnetic resonance imaging |
| RAM | Risk assessment model |
| V/Q | Ventilation-perfusion scan |
References
- Gesta, S.; Tseng, Y.H.; Kahn, C.R. Developmental origin of fat: tracking obesity to its source. Cell 2007, 131, 242–256. [Google Scholar] [CrossRef] [PubMed]
- Naess, I.A.; Christiansen, S.C.; Romundstad, P.; Cannegieter, S.C.; Rosendaal, F.R.; Hammerstrøm, J. Incidence and mortality of venous thrombosis: a population-based study. J. Thromb. Haemost. 2007, 5, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.H.; Gu, K.Q.; Heng, D. Deep vein thrombosis is not rare in Asia-the Singapore General Hospital experience. Ann. Acad. Med. Singap. 2002, 31, 761–764. [Google Scholar] [PubMed]
- Sakon, M.; Maehara, Y.; Yoshikawa, H.; Akaza, H. Incidence of venous thromboembolism following major abdominal surgery: a multi-center, prospective epidemiological study in Japan. J. Thromb. Haemost. 2006, 4, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Nakamura, M.; Sakuma, M.; Yamada, N.; Sakon, M.; Fujita, S.; Seo, N. Incidence of pulmonary thromboembolism (PTE) and new guidelines for PTE prophylaxis in Japan. Clin. Hemorheol. Microcirc. 2006, 35, 257–259. [Google Scholar]
- Kim, J.; Chun, E.; Choi, S.; Park, D.; Kim, H.; Bang, S.; Kim, Y.J. A prospective study on the incidence of postoperative venous thromboembolism in Korea Gastric cancer patients: an inquiry into the application of Western guidelines to Asian cancer patients. PLoS ONE 2013, 8, e61968. [Google Scholar]
- Martino, R.R.D.; Goodney, P.P.; Spangler, E.L.; Wallaert, J.B.; Corriere, M.A.; Rzucidlo, E.M.; Stone, D.H. Variation in thromboemboli complications among patients undergoing commonly performed cancer operations. J. Vasc. Surg. 2012, 55, 1035–1040. [Google Scholar] [CrossRef]
- Leizorovicz, A.; Turpie, A.G.; Cohen, A.T.; Wong, L.; Yoo, M.C.; Dans, A. Epidemiology of venous thromboembolism in Asian patients undergoing major orthopedic surgery without thromboprophylaxis. The SMART study. J. Thromb. Haemost. 2005, 3, 28–34. [Google Scholar] [CrossRef]
- Caprini, J.A. Thrombosis risk assessment as a guide to quality patient care. Dis. Mon. 2005, 51, 70–78. [Google Scholar] [CrossRef]
- Schiff, R.L.; Kahn, S.R.; Shrier, I. Identifying orthopedic patients at high risk for venous thromboembolism despite thromboprophylaxis. Chest 2005, 128, 3364–3371. [Google Scholar] [CrossRef]
- Venous Thromboembolism in Adult Admitted to Hospital: Reducing the Risk. Available online: https://www.nice.org.uk/guidance/cg92 (accessed on 15 January 2010).
- Zhou, H.X.; Peng, L.Q.; Yan, Y.; Yi, Q.; Tang, Y.J. Validation of the Caprini risk assessment model in Chinese hospitalized patients with venous thromboembolism. Thromb. Res. 2012, 130, 735–740. [Google Scholar] [CrossRef]
- Kearon, C.; Akl, E.A.; Comerota, Ạ; Prandoni, P.; Bounameaux, H. Antithrombotic therapy for VTE disease: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012, 141, e419S–e496S. [Google Scholar] [CrossRef]
- Bahl, V.; Hu, H.M.; Henke, P.K.; Wakefield, T.W.; Campbell, D.A., Jr.; Caprini, J.A. A validation study of a retrospective venous thromboembolism risk scoring method. Ann. Surg. 2010, 251, 344–350. [Google Scholar] [CrossRef]
- Lobastov, K.; Barinov, V.; Schastlivtsev, I.; Laberko, L.; Rodoman, G.; Boyarintsev, V. Validation of the Caprini risk assessment model for venous thromboembolism in high-risk surgical patients in the background of standard prophylaxis. J. Vasc. Surg. Venous. Lymphat. Disord. 2016, 4, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Pannucci, C.J.; Bailey, S.H.; Dreszer, G.; Wachtman, C.F.; Zumsteg, J.W.; Jaber, R.M.; Kalliainen, L.K. Valiadation of the Caprini risk assessment model in plastic and reconstructive surgery patients. J. Am. Coll. Surg. 2011, 212, 105–112. [Google Scholar] [CrossRef]
- Yarlagadda, B.B.; Brook, C.D.; Stein, D.J.; Jalisi, S. Venous thromboembolism in otolaryngology surgical impatients receiving chemoprophylaxis. Head Neck 2013, 36, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Kanchan, B.; Anitha, M.; Mohsina, S.; Sanjeev, S.; Arun, K. Assessing the risk for development of Venous Thromboembolism (VTE) in surgical patients using Adapted Caprini scoring system. Int. J. Surg. 2016, 30, 68–73. [Google Scholar]
- Cassidy, M.R.; Rosenkranz, P.; McAneny, D. Reducing postoperative venous thromboembolism complications with a standardized risk-stratified prophylaxis protocol and mobilization program. J. Am. Coll. Surg. 2014, 218, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.A., Jr.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.O., Jr.; Kilaru, R.K.; Hosokawa, P.; Henderson, W.G.; Zinner, M.J.; Khuri, S.F. Multivariable predictors of postoperative venous thromboembolism events after general and vascular surgery: Results from the patient safety in surgery study. J. Am. Coll. Surg. 2007, 204, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Silverstein, M.D.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Meltron, L.J. Risk factors of deep vein thrombosis and pulmonary embolism: A population-based case-control study. Arch. Intern. 2000, 160, 809–881. [Google Scholar] [CrossRef]
- Edmonds, M.J.; Crichton, T.J.; Runciman, W.B.; Pradhan, M. Evidence-based risk factors for postoperative deep vein thrombosis. ANZ J. Surg. 2004, 74, 1082–1097. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.A.; Kakkar, A.K. Venous thromboembolism prophylaxis for the general surgery patient: Where do we stand? Semin. Respir. Crit. Care Med. 2008, 29, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Clayton, J.K.; Anderson, J.A.; McNicol, G.P. Preoperative prediction of postoperative deep vein thrombosis. Br. Med. J. 1976, 2, 910–912. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. of Patients with VTE (%) | Relative Risk | p Value | |
|---|---|---|---|
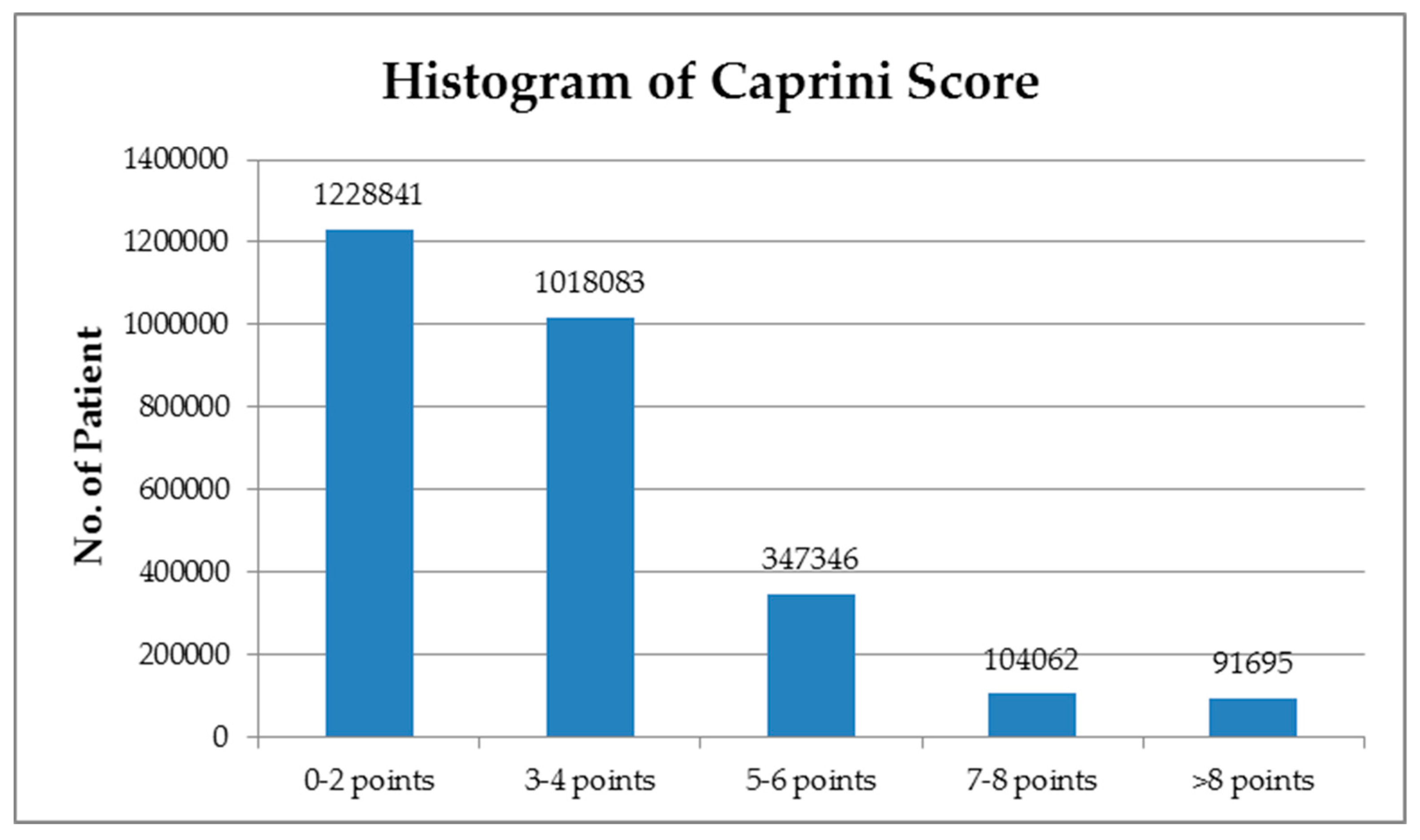
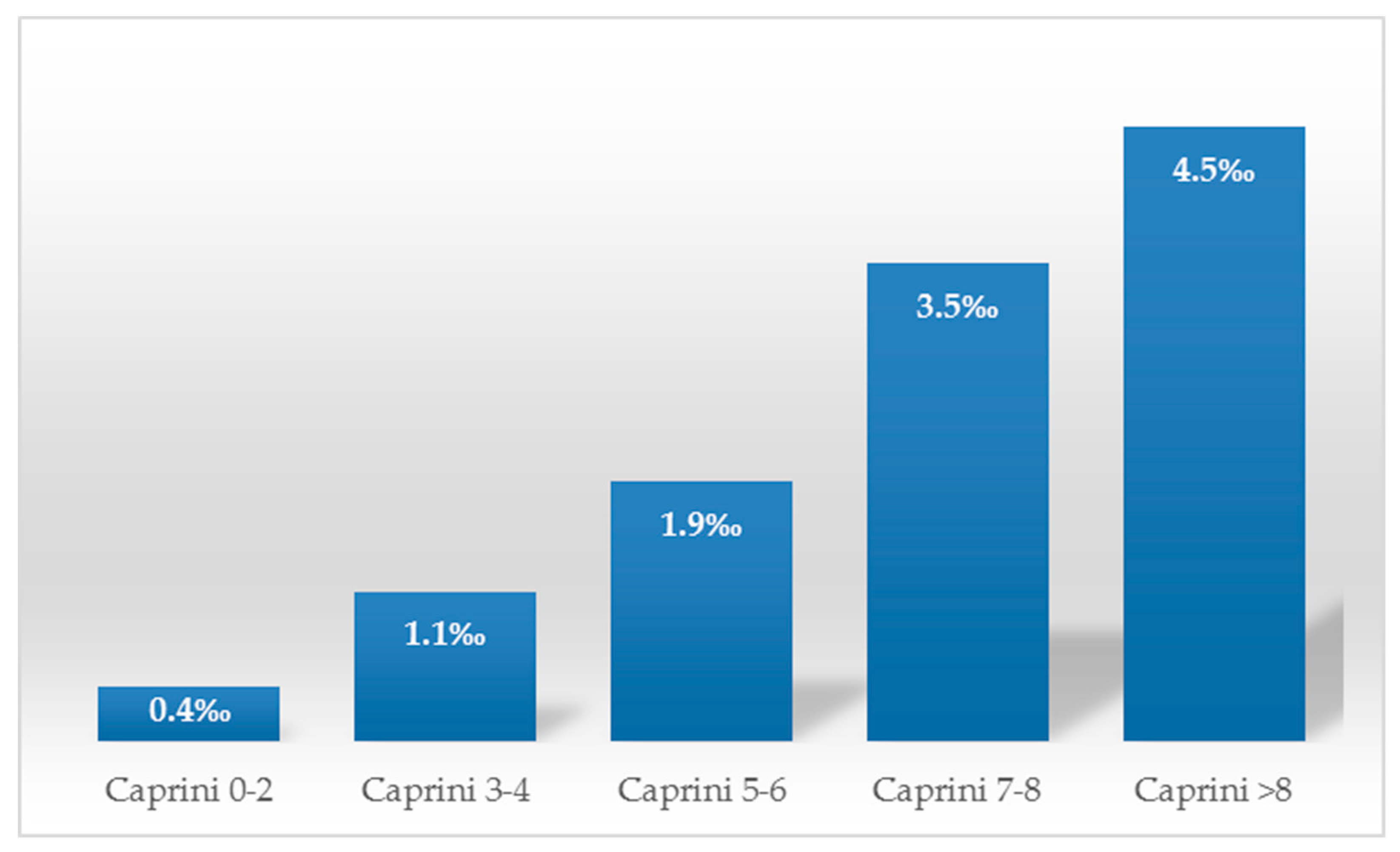
| Caprini 0–2 | 486 (0.04%) | _ | _ |
| Caprini 3–4 | 1141 (0.11%) | 2.83 (2.55–3.15) | <0.001 |
| Caprini 5–6 | 663 (0.19%) | 4.83 (4.29–5.42) | <0.001 |
| Caprini 7–8 | 364 (0.35%) | 8.84 (7.72–10.13) | <0.001 |
| Caprini >8 | 414 (0.45%) | 11.42 (10.02–13.01) | <0.001 |
| Caprini Score | 5–6 Points | 7–8 Points | >8 Points |
|---|---|---|---|
| 3–4 points | 1.7 (1.55–1.88) p < 0.0001 | 3.13 (2.78–3.52) p < 0.0001 | 4.04 (3.61–4.52) p < 0.0001 |
| 5–6 points | - | 1.84 (1.61–2.09) p < 0.0001 | 2.37 (2.10–2.68) p < 0.0001 |
| 7–8 points | - | - | 1.29 (1.12–1.48) p = 0.0004 |
| Risk Factors | RR (95% CI) | Number of Patients | Number of Patients with Postoperative VTE | p |
|---|---|---|---|---|
| Age 41–60 | 2.71 (2.40–3.06) | 980,708 | 1042 | <0.001 |
| Age 61–74 | 4.34 (3.84–4.89) | 617,609 | 1050 | <0.001 |
| Age >74 | 5.37 (4.71–6.12) | 296,650 | 625 | <0.001 |
| Acute MI | 4.51 (3.34–6.09) | 8759 | 43 | <0.001 |
| COPD | 1.03 (0.61–1.75) | 12,304 | 14 | 0.898 |
| Heart failure | 4.58 (4.05–5.18) | 59,169 | 277 | <0.001 |
| Cancer | 1.39 (1.21–1.61) | 135,001 | 207 | <0.001 |
| Varicose vein | 50.26 (46.46–54.36) | 20,338 | 827 | <0.001 |
| Liver disease | 2.29 (1.98–2.64) | 80,812 | 196 | <0.001 |
| Stomach ulcer | 2.62 (2.44–2.82) | 502,953 | 1122 | <0.001 |
| Respiratory failure | 4.01 (2.71–5.94) | 5703 | 25 | <0.001 |
| Lung disease | 3.86 (3.33–4.49) | 44,816 | 182 | <0.001 |
| Acute renal failure | 5.51 (4.82–6.30) | 40,814 | 232 | <0.001 |
| Hypertension | 4.41 (4.11–4.73) | 550,498 | 1596 | <0.001 |
| Immobilizing >3 days | 2.18 (1.34–3.57) | 6685 | 16 | 0.0018 |
| History of DVT/PE | 5.81 (4.79–6.25) | 4901 | 1170 | <0.001 |
| Peripheral vascular disease | 21.43 (18.62–24.66) | 9243 | 204 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanh, B.M.; Cuong, L.Q.; Son, N.T.; Duc, D.T.; Hung, T.T.; Hung, D.D.; Giang, T.B.; Hiep, N.H.; Xuyen, H.T.H.; Nga, N.T.; et al. Determination of Risk Factors for Venous Thromboembolism by an Adapted Caprini Scoring System in Surgical Patients. J. Pers. Med. 2019, 9, 36. https://doi.org/10.3390/jpm9030036
Hanh BM, Cuong LQ, Son NT, Duc DT, Hung TT, Hung DD, Giang TB, Hiep NH, Xuyen HTH, Nga NT, et al. Determination of Risk Factors for Venous Thromboembolism by an Adapted Caprini Scoring System in Surgical Patients. Journal of Personalized Medicine. 2019; 9(3):36. https://doi.org/10.3390/jpm9030036
Chicago/Turabian StyleHanh, Bui My, Le Quang Cuong, Nguyen Truong Son, Duong Tuan Duc, Tran Tien Hung, Duong Duc Hung, Tran Binh Giang, Nguyen Hoang Hiep, Hoang Thi Hong Xuyen, Nguyen Thi Nga, and et al. 2019. "Determination of Risk Factors for Venous Thromboembolism by an Adapted Caprini Scoring System in Surgical Patients" Journal of Personalized Medicine 9, no. 3: 36. https://doi.org/10.3390/jpm9030036