Adaptive, Iterative, Long-Term Personalized Therapy Management in a Case of Stage IV Refractory NSCLC


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patient and Methods
2.1. Patient
2.2. Tissue Collection
2.3. Histopathology and Immunohistochemistry
2.4. Blood Collection and Processing
2.5. Tumor DNA Isolation
2.6. Cell-Free DNA (ctDNA) Isolation
2.7. Tumor RNA Isolation
2.8. Exosomal RNA Isolation
2.9. Whole-Exome Sequencing (WES)
2.10. Cell-Free tumor DNA (ctDNA) Profiling
2.11. mRNA Profiling (Transcriptome Analysis)
2.12. In Vitro Chemosensitivity Profiling of Viable Tumor Cells
3. Results
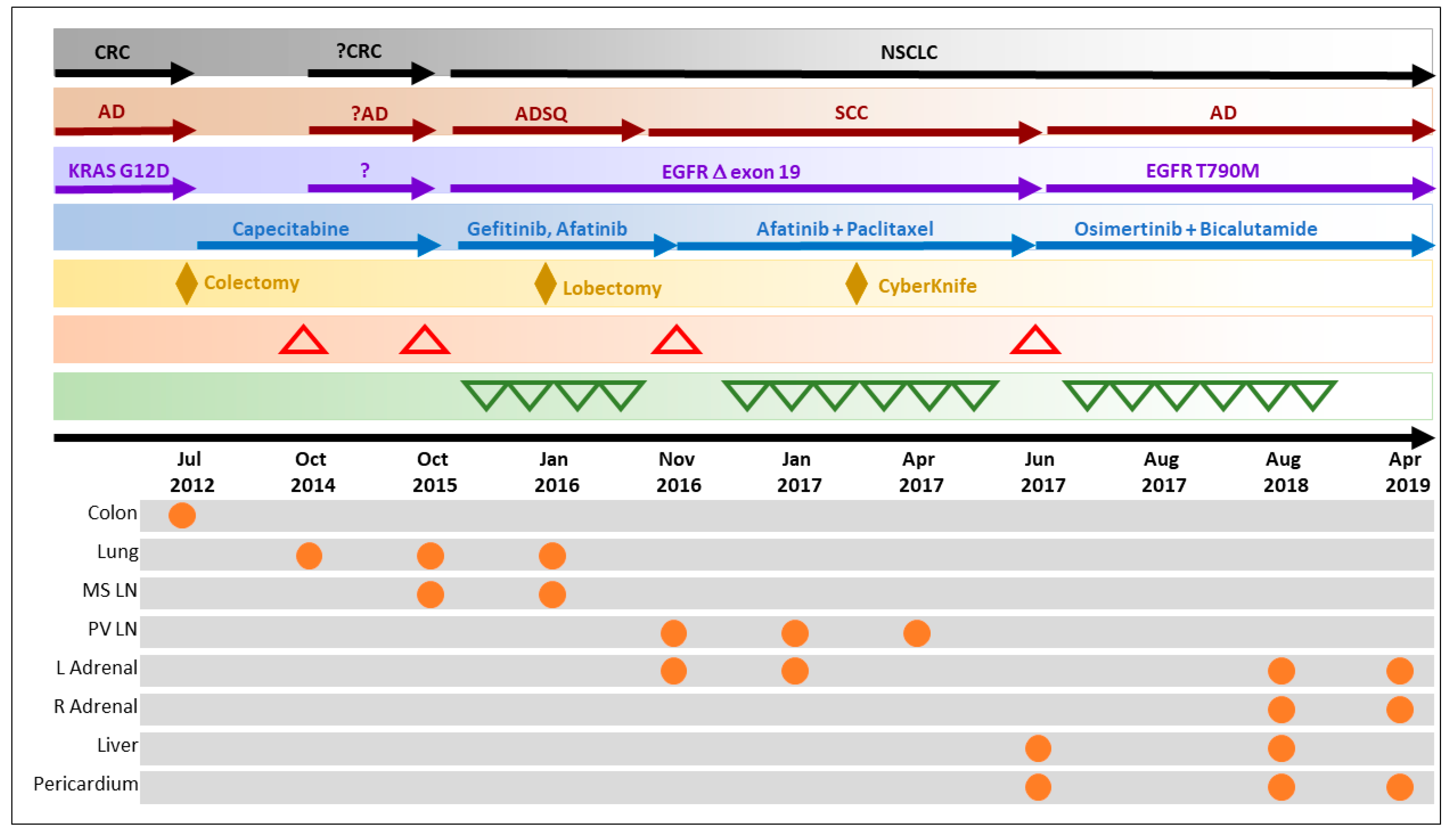
3.1. Overcoming Clinical Conundrum #1: Molecular Investigations Facilitated Accurate Diagnosis and Appropriate Therapy Selection
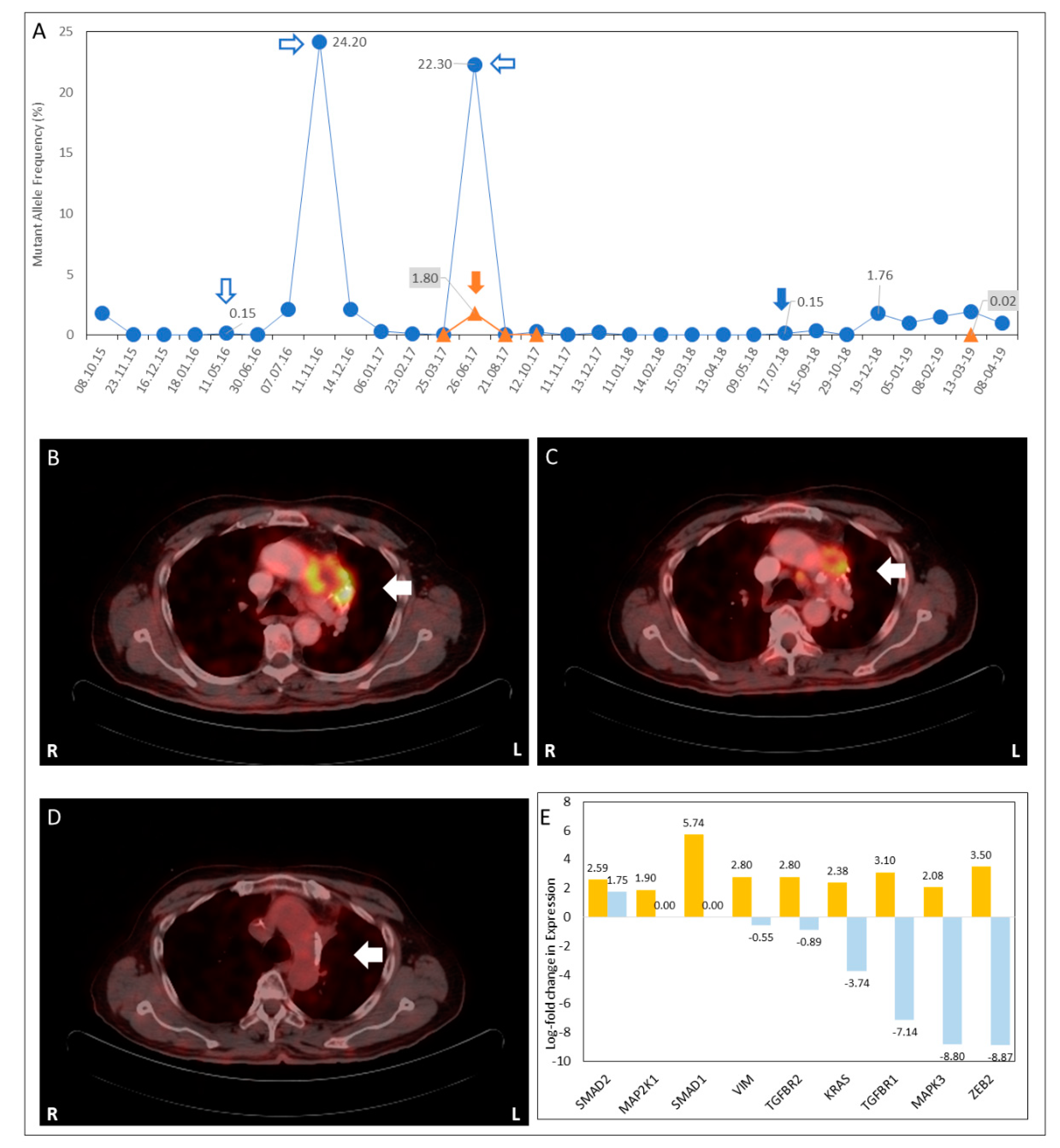
3.2. Overcoming Clinical Conundrum #2: Monitoring for Sub-Radiological Disease and Recurrence
3.3. Overcoming Clinical Conundrum #3: Personalized Treatment Selection when Viable SoC Treatment Options Were Unavailable
3.4. Overcoming Clinical Conundrum #4: Combination of Agents Addresses EGFR Resistance and Target Latent Vulnerability of Tumor
3.5. Recent Status
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability
Conflicts of Interest
References
- Hierro, C.; Matos, I.; Martin-Liberal, J.; Ochoa de Olza, M.; Garralda, E. Agnostic-Histology Approval of new drugs in Oncology: Are we already there? Clin. Cancer Res. 2019, 25, 3694–3707. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Zhang, W. Precision medicine becomes reality—Tumor type-agnostic therapy. Cancer Commun. 2018, 38, 6. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; Dubois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.I.; Wang, H.Y.; Ling, S.; Lu, X. The Ecology and Evolution of Cancer: The Ultra-Microevolutionary Process. Annu. Rev. Genet. 2016, 50, 347–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Deiry, W.S.; Taylor, B.; Neal, J.W. Tumor Evolution, Heterogeneity, and Therapy for Our Patients with Advanced Cancer: How Far Have We Come? Am. Soc. Clin. Oncol. Educ. Book 2017, 37, e8–e15. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Khatami, M. Analyses of repeated failures in cancer therapy for solid tumors: Poor tumor-selective drug delivery, low therapeutic efficacy and unsustainable costs. Clin. Transl. Med. 2018, 7, 11. [Google Scholar] [CrossRef]
- Sodickson, A.; Baeyens, P.F.; Andriole, K.P.; Prevedello, L.M.; Nawfel, R.D.; Hanson, R.; Khorasani, R. Recurrent CT, Cumulative Radiation Exposure, and Associated Radiation-induced Cancer Risks from CT of Adults. Radiology 2009, 251, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S. Tumor markers in clinical practice: General principles and guidelines. Indian J. Med. Paediatr. Oncol. 2009, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Renfro, L.A.; An, M.-W.; Mandrekar, S.J. Precision oncology: A new era of cancer clinical trials. Cancer Lett. 2017, 387, 121–126. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Delord, J.P.; Gonçalves, A.; Gavoille, C.; Dubot, C.; Isambert, N.; Campone, M.; Trédan, O.; Massiani, M.A.; Mauborgne, C.; et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): A multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015, 16, 1324–1334. [Google Scholar] [CrossRef]
- Tsimberidou, A.-M.; Iskander, N.G.; Hong, D.S.; Wheler, J.J.; Falchook, G.S.; Fu, S.; Piha-Paul, S.; Naing, A.; Janku, F.; Luthra, R.; et al. Personalized Medicine in a Phase I Clinical Trials Program: The MD Anderson Cancer Center Initiative. Clin. Cancer Res. 2012, 18, 6373–6383. [Google Scholar] [CrossRef] [PubMed]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Schwaederle, M.; Hahn, M.E.; Williams, C.B.; De, P.; Krie, A.; Piccioni, D.E.; Miller, V.A.; et al. Molecular profiling of cancer patients enables personalized combination therapy: The I-PREDICT study. Nat. Med. 2019, 25, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Saiyed, M.M.; Ong, P.S.; Chew, L. Off-label drug use in oncology: A systematic review of literature. J. Clin. Pharm. Ther. 2017, 42, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Marquart, J.; Ruby, J.; Lammers, A.; Mailankody, S.; Kaestner, V.; Prasad, V. Frequency and level of evidence used in recommendations by the National Comprehensive Cancer Network guidelines beyond approvals of the US Food and Drug Administration: Retrospective observational study. BMJ 2018, 360, k668. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chang, S.; Li, G.; Sun, Y. Application of liquid biopsy in precision medicine: Opportunities and challenges. Front. Med. 2017, 11, 522–527. [Google Scholar] [CrossRef]
- Von Bubnoff, N. Liquid Biopsy: Approaches to Dynamic Genotyping in Cancer. Oncol. Res. Treat. 2017, 40, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Enderle, D.; Spiel, A.; Coticchia, C.M.; Berghoff, E.; Mueller, R.; Schlumpberger, M.; Sprenger-Haussels, M.; Shaffer, J.M.; Lader, E.; Skog, J.; et al. Characterization of RNA from Exosomes and Other Extracellular Vesicles Isolated by a Novel Spin Column-Based Method. PLoS ONE 2015, 10, e0136133. [Google Scholar] [CrossRef]
- Sukhai, M.A.; Craddock, K.J.; Thomas, M.; Hansen, A.R.; Zhang, T.; Siu, L.; Bedard, P.; Stockley, T.L.; Kamel-Reid, S. A classification system for clinical relevance of somatic variants identified in molecular profiling of cancer. Genet. Med. 2016, 18, 128. [Google Scholar] [CrossRef]
- Politi, K.; Lynch, T.J.; Lynch, T.; Lynch, T.J. Two sides of the same coin: EGFR exon 19 deletions and insertions in lung cancer. Clin. Cancer Res. 2012, 18, 1490–1492. [Google Scholar] [CrossRef]
- Heist, R.S.; Sequist, L.V.; Engelman, J.A. Genetic Changes in Squamous Cell Lung Cancer: A Review. J. Thorac. Oncol. 2012, 7, 924–933. [Google Scholar] [CrossRef] [Green Version]
- Saikali, Z.; Singh, G. Doxycycline and other tetracyclines in the treatment of bone metastasis. Anti-Cancer Drugs 2003, 14, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, J.; Pulkoski-Gross, A.; Cao, J. Targeting matrix metalloproteinases in cancer: Bringing new life to old ideas. Genes Dis. 2015, 2, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, H.; Fan, Z.; Wang, Z.; Qu, J. Atorvastatin partially inhibits the epithelial-mesenchymal transition in A549 cells induced by TGF-β1 by attenuating the upregulation of SphK1. Oncol. Rep. 2016, 36, 1016–1022. [Google Scholar]
- Chen, J.; Bi, H.; Hou, J.; Zhang, X.; Zhang, C.; Yue, L.; Wen, X.; Liu, D.; Shi, H.; Yuan, J.; et al. Atorvastatin overcomes gefitinib resistance in KRAS mutant human non-small cell lung carcinoma cells. Cell Death Dis. 2013, 4, e814. [Google Scholar] [CrossRef] [PubMed]
- Suzawa, K.; Toyooka, S.; Sakaguchi, M.; Morita, M.; Yamamoto, H.; Tomida, S.; Ohtsuka, T.; Watanabe, M.; Hashida, S.; Maki, Y.; et al. Antitumor effect of afatinib, as a human epidermal growth factor receptor 2-targeted therapy, in lung cancers harboring HER2 oncogene alterations. Cancer Sci. 2016, 107, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Schuler, M.; Yang, J.C.; Park, K.; Kim, J.H.; Bennouna, J.; Chen, Y.M.; Chouaid, C.; De Marinis, F.; Feng, J.F.; Grossi, F.; et al. Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: Phase III randomized LUX-Lung 5 trial. Ann. Oncol. 2016, 27, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Minari, R.; Bordi, P.; Tiseo, M. Third-generation epidermal growth factor receptor-tyrosine kinase inhibitors in T790M-positive non-small cell lung cancer: Review on emerged mechanisms of resistance. Transl. Lung Cancer Res. 2016, 5, 695–708. [Google Scholar] [CrossRef]
- Munoz, J.; Wheler, J.J.; Kurzrock, R. Androgen receptors beyond prostate cancer: An old marker as a new target. Oncotarget 2015, 6, 592–603. [Google Scholar] [CrossRef]
- Anand, K.; Ensor, J.; Trachtenberg, B.; Bernicker, E. Osimertinib induced cardio-toxicity: A retrospective review of FDA adverse events reporting system (FAERS). J. Clin. Oncol. 2019, 9044. [Google Scholar]
- United States Food and Drug Administration. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-osimertinib-first-line-treatment-metastatic-nsclc-most-common-egfr-mutations (accessed on 19 June 2019).


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranade, A.; Patil, D.; Bhatt, A.; Dhasare, R.; Datta, V.; Datar, R.; Akolkar, D. Adaptive, Iterative, Long-Term Personalized Therapy Management in a Case of Stage IV Refractory NSCLC. J. Pers. Med. 2019, 9, 34. https://doi.org/10.3390/jpm9030034
Ranade A, Patil D, Bhatt A, Dhasare R, Datta V, Datar R, Akolkar D. Adaptive, Iterative, Long-Term Personalized Therapy Management in a Case of Stage IV Refractory NSCLC. Journal of Personalized Medicine. 2019; 9(3):34. https://doi.org/10.3390/jpm9030034
Chicago/Turabian StyleRanade, Anantbhushan, Darshana Patil, Amit Bhatt, Rucha Dhasare, Vineet Datta, Rajan Datar, and Dadasaheb Akolkar. 2019. "Adaptive, Iterative, Long-Term Personalized Therapy Management in a Case of Stage IV Refractory NSCLC" Journal of Personalized Medicine 9, no. 3: 34. https://doi.org/10.3390/jpm9030034