
Longterm Outcome of Therapeutic Vaccination with a Third Generation Pre-S/S HBV Vaccine (PreHevbrioR) of Chronically HBV Infected Patients

Abstract
:1. Introduction and Rational
1.1. Development of Vaccines for Protection against Hepatitis B Virus Infection
1.2. Development of Therapeutic Vaccines for Control of Chronic Hepatitis B
2. Materials and Methods
2.1. Patients
2.2. Pre-S1/Pre-S2/S HBV Vaccine
2.3. Vaccination Protocol and Monitoring
3. Results
3.1. Monitoring Unvaccinated Carriers
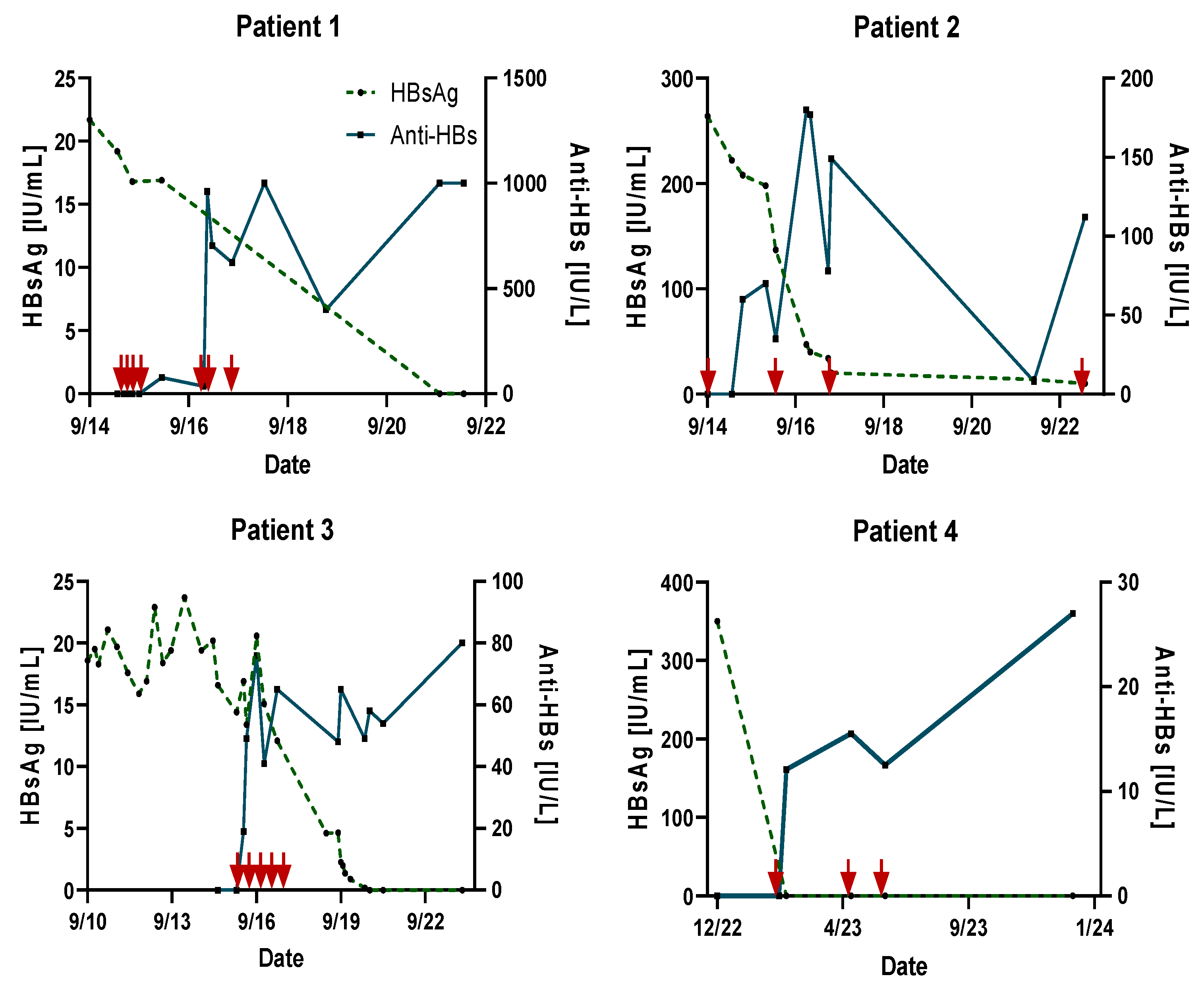
3.2. Follow-Up of Vaccinated Patients with or without Ongoing NUC Treatment
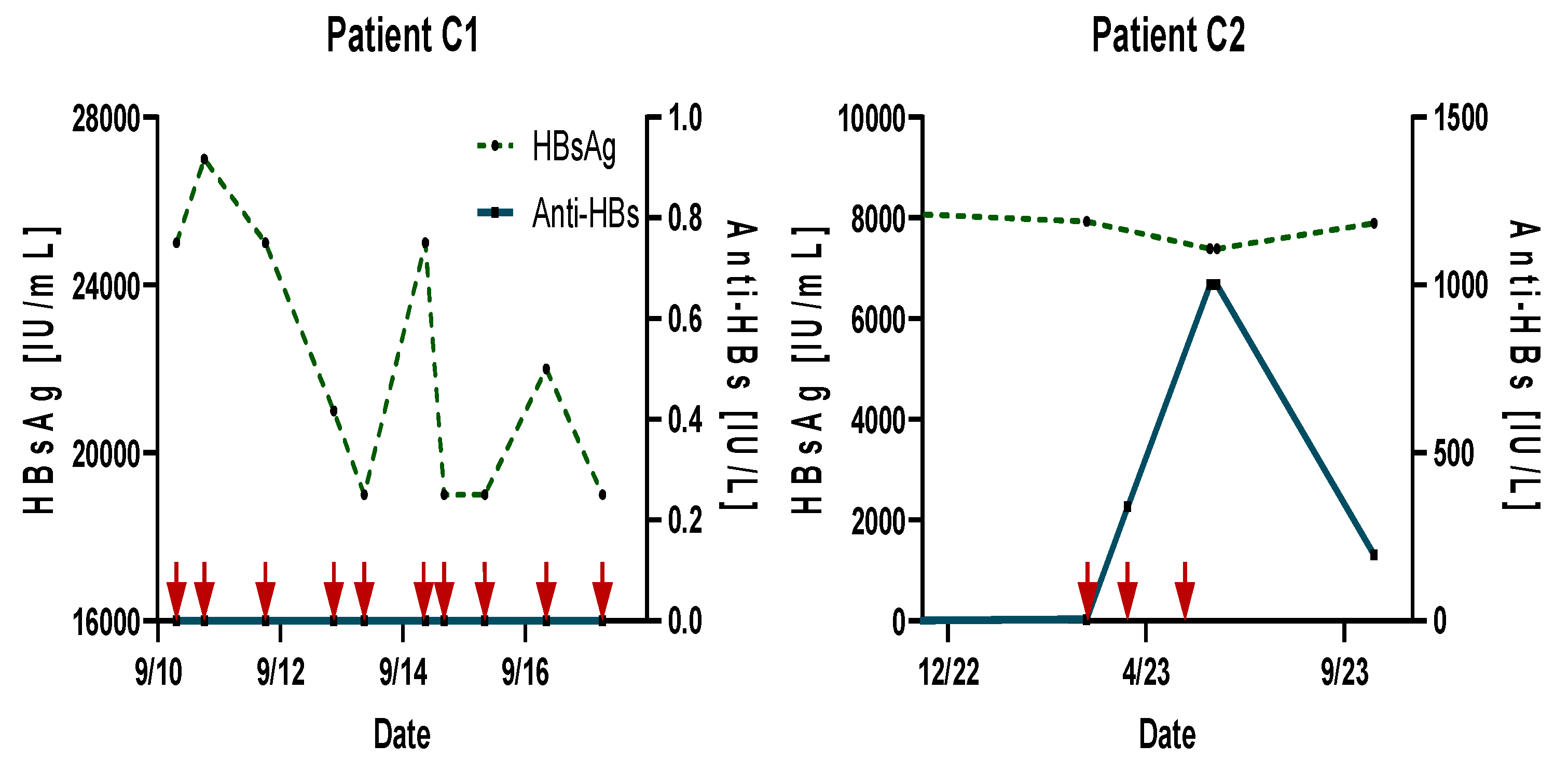
3.3. Vaccination of High-Level HBsAg Carrier Controls
4. Discussion
- -
- The results of the present observation revealed an excellent anti-HBs seroconversion response in three out of four HBsAg carriers immunized repeatedly with a PreS/S vaccine.
- -
- Furthermore, these data suggest that low-level HBV carriership seems to be a pre-requisite for successful therapeutic vaccination resulting in functional cure.
- -
- No patient in this long-term observation (1 to 6 years) had a relapse or deterioration of the clinical status.
- -
- These findings provide strong support for the development of a larger prospective study focused on low-level HBV carriers, utilizing a pre-S/S HBV vaccine in combination with NUC therapy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Available online: https://who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 15 March 2024).
- Liu, Z.; Li, M.; Hutton, D.W.; Wagner, A.L.; Yao, Y.; Zhu, W.; Cao, L.; Tang, S.; Pan, J.; Wang, Y.; et al. Impact of the national hepatitis B immunization program in China: A modeling study. Infect. Dis. Poverty 2022, 11, 106. [Google Scholar] [CrossRef] [PubMed]
- Chien, R.N.; Liaw, Y.F. Current Trend in Antiviral Therapy for Chronic Hepatitis B. Viruses 2022, 14, 434. [Google Scholar] [CrossRef]
- Brechot, C.; Pourcel, C.; Louise, A.; Rain, B.; Tiollais, P. Presence of integrated hepatitis B virus DNA sequences in cellular DNA of human hepatocellular carcinoma. Nature 1980, 286, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Grudda, T.; Hwang, H.S.; Taddese, M.; Quinn, J.; Sulkowski, M.S.; Sterling, R.K.; Balagopal, A.; Thio, C.L. Integrated hepatitis B virus DNA maintains surface antigen production during antiviral treatment. Clin. Investig. 2022, 132, e161818. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Ninomiya, M.; Kakazu, E.; Kimura, O.; Shimosegawa, T. Hepatitis B surface antigen could contribute to the immunopathogenesis of hepatitis B virus infection. ISRN Gastroenterol. 2013, 2013, 935295. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.N.; Kuo, C.F.; Ou, J.J. Mechanisms of Hepatitis B Virus Persistence. Trends Microbiol. 2018, 26, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Menne, S.; Roneker, C.A.; Roggendorf, M.; Gerin, J.L.; Cote, P.J.; Tennant, B.C. Deficiencies in the acute-phase cell-mediated immune response to viral antigens are associated with development of chronic woodchuck hepatitis virus infection following neonatal inoculation. J. Virol. 2002, 76, 1769–1780. [Google Scholar] [CrossRef]
- Thomson, A.W.; Knolle, P.A. Antigen-presenting cell function in the tolerogenic liver environment. Nat. Rev. Immunol. 2010, 10, 753–766. [Google Scholar] [CrossRef]
- Alawad, A.; Auh, S.; Suarez, D.; Ghany, M. Durability of Spontaneous and Treatment-Related Loss of Hepatitis B s Antigen. Clin. Gastroenterol. Hepatol. 2020, 18, 700–709.e3. [Google Scholar] [CrossRef]
- Berg, T.; Simon, K.G.; Mauss, S.; Schott, E.; Heyne, R.; Klass, D.M.; Eisenbach, C.; Welzel, T.M.; Zachoval, R.; Felten, G.; et al. FINITE CHB study investigators [First investigation in stopping TDF Long-term response after stopping tenofovir disoproxil fumarate in non-cirrhotic HBeAg-negative patients treatment after long-term virological suppression in HBeAg-negative chronic hepatitis B]. J. Hepatol. 2017, 67, 918–924. [Google Scholar] [CrossRef]
- Wong, G.L.H.; Gane, E.; Lok, A.S.F. How to achieve functional cure of HBV: Stopping NUCs, adding interferon or new drug development? J. Hepatol. 2022, 76, 1249–1262. [Google Scholar] [CrossRef] [PubMed]
- Hadziyannis, S.J.; Sevastianos, V.; Rapti, I.; Vassilopoulos, D.; Hadziyannis, E. Sustained responses and loss of HBsAg in HBeAg-negative patients with chronic hepatitis B who stop long-term treatment with adefovir. Gastroenterology 2012, 143, 629–636. [Google Scholar] [CrossRef]
- Jeng, W.J.; Chen, Y.C.; Chien, R.N.; Sheen, I.S.; Liaw, Y.F. Incidence and predictors of hepatitis B surface antigen seroclearance after cessation of nucleos(t)ide analogue therapy in hepatitis B e antigen-negative chronic hepatitis B. Hepatology 2018, 68, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Pol, S.; Nalpas, B.; Driss, F.; Michel, M.L.; Tiollais, P.; Denis, J.; Brécho, C. Multicenter study group. Efficacy and limitations of a specific immunotherapy in chronic hepatitis B. J. Hepatol. 2001, 34, 917–921. [Google Scholar] [CrossRef]
- Michler, T.; Kosinska, A.; Festag, J.; Bunse, T.; Su, J.; Ringelhan, M.; Imhof, H.; Grimm, D.; Steiger, K.; Mogler, C.; et al. Knockdown of Virus Antigen Expression Increases Therapeutic Vaccine Efficacy in High-Titer Hepatitis B Virus Carrier Mice. Gastroenterology 2020, 158, 1762–1775.e9. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Finn, A.; van Damme, P.; Leroux-Roels, I.; Leroux-Roels, G.; Segall, N.; Toma, A.; Vallieres, G.; Aronson, R.; Reich, D.; et al. CONSTANT Study Group Immunogenicity and Safety of a 3-Antigen Hepatitis B Vaccine vs a Single-Antigen Hepatitis B Vaccine: A Phase 3 Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2128652. [Google Scholar] [CrossRef] [PubMed]
- Shouval, D. Hepatitis B vaccines. J. Hepatol. 2003, 39 (Suppl. S1), S70–S76. [Google Scholar] [CrossRef] [PubMed]
- Shouval, D.; Roggendorf, H.; Roggendorf, M. Enhanced immune response to hepatitis B vaccination through immunization with a Pre-S1/Pre-S2/S Vaccine. Med. Microbiol. Immun. 2015, 204, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, A.; Ludwig, C.; Jochum, C.; Fiedler, M.; Heinemann, F.M.; Shouval, D.; Roggendorf, M.; Roggendorf, H.; Lindemann, M. Induction of a robust T- and B-cell immune response in non- and low-responders to conventional vaccination against hepatitis B by using a third generation PreS/S vaccine. Vaccine 2014, 32, 5077–5082. [Google Scholar] [CrossRef]
- Rendi-Wagner, P.; Shouval, D.; Genton, B.; Lurie, Y.; Rümke, H.; Boland, G.; Cerny, A.; Heim, M.; Bach, D.; Schroeder, M.; et al. Comparative immunogenicity of a PreS/S hepatitis B vaccine in non- and low responders to conventional vaccine. Vaccine 2006, 24, 2781–2789. [Google Scholar] [CrossRef]
- Roggendorf, H.; Krawczyk, A.; Lindemann, M.; Shouval, D.; Michler, T.; Roggendorf, M.; Gerken, G. Induction of Functional Control in Chronic Hepatitis B Patients with Low Level HBsAg Using a Combination of a PreS1/S2/S HBV Vaccine (Sci-B- VacTM) and a Nucleoside Analogue. J. Infect. Dis. Ther. 2019, 7, 390. [Google Scholar] [CrossRef]
- Lok, A.S.; Zoulim, F.; Dusheiko, G.; Ghany, M.G. Hepatitis B cure: From discovery to regulatory approval. J. Hepatol. 2017, 67, 847–861. [Google Scholar] [CrossRef] [PubMed]
- Knolle, P.A.; Thimme, R. Hepatic immune regulation and its involvement in viral hepatitis infection. Gastroenterology 2014, 146, 1193–1207. [Google Scholar] [CrossRef]
- Dembek, C.; Protzer, U.; Roggendorf, M. Overcoming immunetolerance in chronic hepatitis B by therapeutic vaccination. Curr. Opin. Virol. 2018, 30, 58–67. [Google Scholar] [CrossRef]
- Gish, R.G.; Yuen, M.-F.; Chan, H.L.Y.; Given, B.D.; Lai, C.-L.; Locarnini, S.A.; Lau, J.Y.; Wooddell, C.I.; Schluep, T.; Lewis, D.L. Synthetic RNAi triggers and their use in chronic hepatitis B therapies with curative intent. Antivir. Res. 2015, 121, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Yuen, M.F.; Lim, S.G.; Plesniak, R.; Tsuji, K.; Janssen, H.L.A.; Pojoga, C.; Gadano, A.; Popescu, C.P.; Stepanova, T.; Asselah, T.; et al. Efficacy and Safety of Bepirovirsen in Chronic Hepatitis B Infection. N. Engl. J. Med. 2022, 387, 1957–1968. [Google Scholar] [CrossRef] [PubMed]
- Kasianchuk, N.; Dobrowolska, K.; Harkava, S.; Bretcan, A.; Zarębska-Michaluk, D.; Jaroszewicz, J.; Flisiak, R.; Rzymski, P. Gene-Editing and RNA Interference in Treating Hepatitis B: A Review. Viruses 2023, 15, 2395. [Google Scholar] [CrossRef] [PubMed]
- Van Gulck, E.; Conceição-Neto, N.; Aerts, L.; Pierson, W.; Verschueren, L.; Vleeschouwer, M.; Krishna, V.; Nájera, I.; Pauwels, F. Retreatment with HBV siRNA Results in Additional Reduction in HBV Antigenemia and Immune Stimulation in the AAV-HBV Mouse Model. Viruses 2024, 16, 347. [Google Scholar] [CrossRef]
- Al-Mahtab, M.; Bazinet, M.; Vaillant, A. Safety and Efficacy of Nucleic Acid Polymers in Monotherapy and Combined with Immunotherapy in Treatment-Naive Bangladeshi Patients with HBeAg+ Chronic Hepatitis B Infection. PLoS ONE 2016, 11, e0156667. [Google Scholar] [CrossRef]
- Bazinet, M.; Pantea, V.; Cebotarescu, V.; Cojuhari, L.; Jimbei, P.; Albrecht, J.; Schmid, P.; Le Gal, F.; Gordien, E.; Krawczyk, A.; et al. Safety and efficacy of REP 2139 and pegylated interferon alfa-2a for treatment-naive patients with chronic hepatitis B virus and hepatitis D virus co-infection (REP 301 and REP 301-LTF): A non-randomised, openlabel, phase 2 trial. Lancet Gastroenterol. Hepatol. 2017, 2, 877–889. [Google Scholar] [CrossRef]
- Liang, P.; Zu, J.; Zhuang, G. A Literature Review of Mathematical Models of Hepatitis B Virus Transmission Applied to Immunization Strategies From 1994 to 2015. J. Epidemiol. 2018, 28, 221–229. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient | HBV-DNA Quant. IU/L (CobasX800) | HBs-Ag IU/mL (CMIA) | Anti-HBs IU/L (ECLIA) |
|---|---|---|---|
| Patient 1 Male, 46 y | |||
| Prior to Vaccination | Negative | 22 | Negative |
| Number of Vaccinations: 4 with PreHevbrioR (10 μg) | |||
| Number of Vaccinations: 3 with PreHevbrioR (20 μg) | |||
| Post-Vaccination (48 months) | Negative | Negative | 1000 |
| Termination of NUC Treatment (24 Months after Vaccination): 2021 | |||
| Patient 2 Male, 68 y | |||
| Prior to Vaccination | Negative | 264 | Negative |
| Number of Vaccinations: 4 with PreHevbrioR (20 μg) | |||
| Post-Vaccination (60 months) | Negative | 10 | 112 |
| Termination of NUC Treatment (30 Months after Vaccination): 2014 | |||
| Patient 3 Female, 43 y | |||
| Prior to Vaccination | Negative | 21 | Negative |
| Number of Vaccinations: 5 with PreHevbrioR (20 μg) | |||
| Post-vaccination (48 months) | Negative | Negative | 58 |
| Termination of NUC Treatment (24 Months after Vaccination): 2020 | |||
| Patient 4 Female, 61 y | |||
| Prior to Vaccination | Negative | 350 | Negative |
| Number of Vaccinations: 3 with PreHevbrioR (20 μg) | |||
| Post-Vaccination (7 months) | Negative | Negative | 27 |
| NUC Treatment: Ongoing | |||
| Patient | HBV-DNA Quant. IU/L (CobasX800) | HBs-Ag IU/mL (CMIA) | Anti-HBs IU/L (ECLIA) |
|---|---|---|---|
| Patient C1 Male, 68 y | |||
| Prior to Vaccination | Negative | 24.000 | Negative |
| Number of Vaccinations: 10 with PreHevbrioR (20 μg) | |||
| Post-Vaccination (40 months) | negative | 24.000 | Negative |
| Termination of NUC Treatment (32 Months after Vaccination): 2019 | |||
| Patient C2 Female, 65 y | |||
| Prior to Vaccination | Negative | 8442 | Negative |
| Number of Vaccinations: 3 with PreHevbrioR (20 μg) | |||
| Post-Vaccination (6 months) | Negative | 7687 | >1.000 |
| NUC Treatment: Ongoing | |||
| Patient | GOT/GPT IU/L 10–50 | GGT IU/L < 66 |
|---|---|---|
| Patient 1 Male, 46 y | ||
| Prior to Vaccination | 41/60 | 45 |
| Post-Vaccination (48 months) | 39/47 | 43 |
| Termination of NUC Treatment (24 Months after Vaccination): 2021 | ||
| Patient 2 Male, 68 y | ||
| Prior to Vaccination | 27/38 | 24 |
| Post-Vaccination (60 months) | 23/28 | 13 |
| Termination of NUC Treatment (30 Months after Vaccination): 2014 | ||
| Patient 3 Female, 43 y | ||
| Prior to Vaccination | 24/16 | 12 |
| Post-Vaccination (48 months) | 21/14 | 10 |
| Termination of NUC Treatment (24 Months after Vaccination): 2020 | ||
| Patient 4 Female, 61 y | ||
| Prior to Vaccination | 18/20 | 18 |
| Post-Vaccination (7 months) | 25/27 | 22 |
| NUC Treatment: Ongoing | ||
| Patient | GOT/GPT IU/L 10–50 | GGT IU/L < 66 |
|---|---|---|
| Patient C1 Male, 68 y | ||
| Prior to Vaccination | 24/18 | 34 |
| Post-Vaccination (2 months) | 28/22 | 56 |
| Termination of NUC Treatment (32 Months after Vaccination): 2019 | ||
| Patient C2 Female, 65 y | ||
| Prior to Vaccination | 23/17 | 19 |
| Post-Vaccination (1.5 months) | 24/12 | 12 |
| NUC Treatment: Ongoing | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roggendorf, H.; Shouval, D.; Roggendorf, M.; Gerken, G. Longterm Outcome of Therapeutic Vaccination with a Third Generation Pre-S/S HBV Vaccine (PreHevbrioR) of Chronically HBV Infected Patients. J. Pers. Med. 2024, 14, 364. https://doi.org/10.3390/jpm14040364
Roggendorf H, Shouval D, Roggendorf M, Gerken G. Longterm Outcome of Therapeutic Vaccination with a Third Generation Pre-S/S HBV Vaccine (PreHevbrioR) of Chronically HBV Infected Patients. Journal of Personalized Medicine. 2024; 14(4):364. https://doi.org/10.3390/jpm14040364
Chicago/Turabian StyleRoggendorf, Hedwig, Daniel Shouval, Michael Roggendorf, and Guido Gerken. 2024. "Longterm Outcome of Therapeutic Vaccination with a Third Generation Pre-S/S HBV Vaccine (PreHevbrioR) of Chronically HBV Infected Patients" Journal of Personalized Medicine 14, no. 4: 364. https://doi.org/10.3390/jpm14040364