1. Introduction
In recent years, the global public health landscape has been profoundly affected by the formidable SARS-CoV-2 infection, leading to the widespread COVID-19 pandemic. Throughout this ongoing health crisis, various variants of SARS-CoV-2 have emerged, contributing to a spectrum of disease severity, from mild to severe [
1,
2]. A pivotal response to combat this pandemic has been the rapid development and deployment of diverse COVID-19 vaccines, primarily targeted at individuals with a high risk of infection and severe disease [
3,
4,
5].
The expedited vaccine development process predominantly centred on the viral spike protein [
6], with notable formulations including mRNA vaccines such as mRNA-1273 (Spikevax, Moderna—NIAID) and BNT162b2 (Comirnaty, Pfizer—BioNTech), as well as the ChAdOx1-S (Vaxzevria, AstraZeneca—University of Oxford) and Ad26.COV2.S (Jcovden, Janssen). The first to gain approval was the BNT162b2 vaccine on 31 December 2020 [
4].
The mRNA vaccine mechanism involves isolating the SARS-CoV-2 virus’s mRNA encoding the spike protein, encapsulating it in a lipid nanoparticle, and delivering it intramuscularly. Within host cells, the mRNA is translated by ribosomes to synthesize spike proteins, triggering an immune response. A modified chimpanzee DNA adenovirus serves as the vector for the AstraZeneca vaccine, generating an immune response against the viral protein encoded in the host DNA [
7,
8,
9].
It is crucial to emphasize that the effectiveness of COVID-19 vaccines can vary based on factors, such as viral variants, population demographics, and other considerations. After vaccination, immunity against SARS-CoV-2 in the respiratory mucosa primarily involves humoral immunity, with IgG prevailing over IgA titres against vaccine antigens. Individuals exhibited detectable levels of spike IgG in the airway mucosa, and their level was increased when accompanied by mucosal IgA in infected patients. [
10]
In the intricate interplay between metabolic diseases and the evolving landscape of COVID-19, the emergence of the Delta variant introduces a new layer of intricacy [
11].
The Delta variant (B.1.617.2), first identified in December 2020 in India, became the most transmissible variant, with 66% more prevalence over the Alpha variant in England and over 79% in some regions from France. In comparison with the previous variants, it has increased severity, higher viral loads, and implies a longer period of virus detection with the polymerase chain reaction (PCR) [
12,
13,
14,
15]. Individuals managing metabolic disorders may find themselves at an elevated risk of experiencing severe outcomes when confronted with the Delta variant [
16,
17]. This intersection emphasizes the urgent need for tailored strategies and nuanced medical interventions to address the unique challenges posed by COVID-19, particularly in individuals burdened by metabolic health issues. Exploring this intricate relationship not only deepens our understanding of the disease’s multifaceted nature but also underscores the imperative of widespread vaccination efforts to mitigate the impact on vulnerable populations.
This study aims to compare the patients characteristics, including demographic parameters, the smoking status, symptoms on hospital admission, comorbidities and CT lung involvement assessed by visual score, Padua score, oxygen saturation (O2 saturation), ventilation requirement, dynamic of arterial blood gas (ABG) parameters, ICU admission rate, and mortality rate in vaccinated and non-vaccinated hospitalized patients with the COVID-19 Delta variant, and to evaluate the impact of vaccination in preventing the severity of infection.
2. Materials and Methods
2.1. Study Population
This retrospective study, conducted between October 2021 and February 2022, investigated a cohort of 226 adult patients admitted to a COVID-19 department at a University Centre in Cluj-Napoca, Romania. The study adhered to the guidelines of the Declaration of Helsinki, and approval from the Human Research Ethics Committee (number: 60/2023) was obtained.
Inclusion criteria for patients were (1) patients with laboratory-confirmed SARS-CoV-2 infection through PCR test, (2) aged ≥ 18 years, (3) hospitalized in our unit, and (4) vaccinated and unvaccinated patients with Delta variant.
We excluded the patients with (1) insufficient laboratory or imaging records (n = 21 patients) and (2) patients transferred to other units (n = 8 patients).
Finally, 197 participants were eligible for taking part in the study. They were divided into two groups: 44 patients were fully vaccinated (group V) and 153 were unvaccinated (UV). Enrolment of the patients is described in
Figure 1.
The confirmation of COVID-19 was determined through PCR testing conducted on samples obtained from either nasopharyngeal swabs or sputum. Additionally, abnormal findings in computed tomography scans supported the diagnosis. Notably, the genetic analysis revealed that all individuals tested positive for the Delta variant, a significant concern at the time of the SARS-CoV-2 virus spreading. This determination was based on the distinctive genetic markers identified during the PCR testing process, enabling the specific identification of the Delta variant in each confirmed case. The vaccination status and the type of the vaccine was checked on the proof of vaccination. The term “fully vaccinated” refers to an individual who has received the complete dose regimen of COVID-19 vaccine as recommended by the relevant health authorities or vaccine manufacturers at the time (a two-dose regimen of mRNA-1273, BNT162b2, and ChAdOx1-S, and a single-dose regimen of Ad26.COV2.S).
Mild or moderate cases were generally defined based on discomfort and illness that can be managed at home with mild clinical symptoms (low grade fever, cough, discomfort, shortness of breath, or fatigue) and recovery within a couple of weeks with rest, hydration, and over-the-counter medications to alleviate symptoms [
18,
19].
The severity of the SARS-CoV-2 infection was defined according to the national and international criteria: a lung’s involvement > 50% on CT scan, scored by visual assessment; hypoxia, defined by a drop in oxygen saturation SpO2 < 94%; PaO2/FiO2 < 300 mm Hg; or a respiratory rate (RR) > 30/min.
The Padua score, originally developed for estimating venous thromboembolism (VTE) risk in hospitalized patients, has been used to help identify COVID-19 patients who are at higher risk for VTE and who may benefit from prophylactic anticoagulation therapy. Studies have shown that COVID-19 patients have an increased risk of VTE due to the hypercoagulable state associated with the pro-inflammatory response to the pathogen [
20].
Patients were treated according to Romanian National Guidelines, receiving a standard care regimen inclusive of dexamethasone, anticoagulants, antibiotics, nutritional support, hepatic and gastric protective medications, and oxygen therapy. Severe cases received antivirals (remdesivir) and immunomodulators (tocilizumab or anakinra). [
21].
The administration of oxygen supplementation was initiated in the severe cases of COVID-19 (oxygen saturation ≤ 93% on room air) when patients experienced significant respiratory distress.
2.2. Data Collection: Clinical Characteristics and Blood Sample Collection
Medical records provided data on demographic parameters, smoking status, symptoms at hospital admission, comorbidities, CT lung involvement (visual score), Padua score, O2 saturation, ventilation requirement, ABG parameters, ICU admission rate, and mortality rate.
Arterial blood samples (ABG) were collected at admission and daily during the hospital stay. An anaerobic 2 to 3 mL of arterial specimen was obtained from a peripheral artery using a 3 or 5 mL airtight syringe. Analysis occurred within 10 min.
2.3. Statistical Analysis
Descriptive and inferential statistical methods were applied. Factor variables were described using frequency and percentages; continuous variables used mean, median, and interquartile range. Pearson’s Chi-square test and the Wilcoxon rank-sum test were used for nominal and continuous variables. Ordinal regression and univariate/multivariate linear regressions were performed. Significance was considered for p-value < 0.05. Analysis used R (version 2022.12.0+353) with RStudio (version 2022.12.0+353 for Mac).
3. Results
3.1. Patient’s Characteristics, Demographic Parameters, the Smoking Status, Symptoms on Hospital Admission, Comorbidities, Vaccine Type, and the Delay between Complete Vaccination–Infection (Table 1, Table 2, Table 3, Table 4 and Table 5)
We analysed a total of 197 patients, comprising 47 vaccinated and 153 unvaccinated individuals. The groups were homogeneous concerning age, body mass index (BMI), and smoking status. Notably, a statistically significant difference was observed in sex, with more women in the unvaccinated group (p = 0.008). Both groups exhibited comparable symptoms on hospital admission and comorbidities.
Table 1 reveals a statistically non-significant difference in age between vaccinated (mean = 59) and unvaccinated (mean = 64) groups (
p = 0.10). BMI mean values were 28.3 and 29.0 for vaccinated and unvaccinated groups, respectively (
p = 0.3). The smoking status distribution did not differ significantly between the groups (
p = 0.14).
Table 3 displays similar symptomatology on hospital admission between vaccinated and unvaccinated groups, with no significant differences observed.
Table 4 demonstrates no significant variations in comorbidities between the groups.
Table 5 shows a longer period of time between Pfizer vaccine and infection, translating to a longer period of immunization.
Table 1.
Patients’ characteristics.
Table 1.
Patients’ characteristics.
| Characteristic | Vaccinated,
n = 44 1 | Unvaccinated,
n = 153 1 | p-Value 2 |
|---|
| Sex | | | 0.008 |
| Females | 16 (36%) | 90 (59%) | |
| Males | 28 (64%) | 63 (41%) | |
| Age | | | 0.10 |
| Mean (SD) | 59 (16) | 64 (15) | |
| Median (IQR) | 62 (50, 72) | 66 (54, 74) | |
| Body Mass Index | | | 0.3 |
| Mean (SD) | 28.3 (4.8) | 29.0 (4.9) | |
| Median (IQR) | 27.7 (25.2, 31.2) | 28.0 (26.0, 32.6) | |
Table 2.
Smoking status.
| Characteristic | Vaccinated,
n = 44 1 | Unvaccinated,
n = 153 1 | p-Value 2 |
|---|
| Smoking status | | | 0.14 |
| Smoker | 10 (23%) | 41 (27%) | |
| Ex-smoker | 10 (23%) | 17 (11%) | |
| Non-smoker | 24 (55%) | 95 (62%) | |
Table 3.
Patients’ symptoms on hospital admission.
Table 3.
Patients’ symptoms on hospital admission.
| Symptoms on Hospital Admission | Vaccinated,
n = 44 1 | Unvaccinated,
n = 153 1 | p-Value 2 |
|---|
| Fever | | | 0.7 |
| YES | 31 (70%) | 112 (73%) | |
| NO | 13 (30%) | 41 (27%) | |
| Chills | | | 0.2 |
| YES | 32 (73%) | 95 (62%) | |
| NO | 12 (27%) | 58 (38%) | |
| Cough | | | 0.6 |
| YES | 34 (77%) | 113 (74%) | |
| NO | 10 (23%) | 40 (26%) | |
| Dyspnea | | | 0.3 |
| YES | 24 (55%) | 97 (63%) | |
| NO | 20 (45%) | 56 (37%) | |
| Arthralgia | | | 0.7 |
| YES | 6 (14%) | 28 (18%) | |
| NO | 38 (86%) | 124 (81%) | |
| Myalgias | | | 0.8 |
| YES | 13 (30%) | 49 (32%) | |
| NO | 31 (70%) | 104 (68%) | |
| Diarrhea | | | 0.13 |
| YES | 1 (2.3%) | 16 (10%) | |
| NO | 43 (98%) | 137 (90%) | |
Table 4.
Patients’ comorbidities.
Table 4.
Patients’ comorbidities.
| Comorbidities | Vaccinated,
n = 44 1 | Unvaccinated,
n = 153 1 | p-Value 2 |
|---|
| Obesity | | | 0.3 |
| YES | 16 (36%) | 68 (44%) | |
| NO | 28 (64%) | 85 (56%) | |
| Diabetes | | | 0.5 |
| YES | 15 (34%) | 43 (28%) | |
| NO | 29 (66%) | 109 (72%) | |
| Arterial Hypertension | | | 0.8 |
| YES | 26 (59%) | 94 (61%) | |
| NO | 18 (41%) | 59 (39%) | |
| Cardiovascular disease | | | 0.4 |
| YES | 21 (48%) | 63 (41%) | |
| NO | 23 (52%) | 90 (59%) | |
| Respiratory disease | | | 0.8 |
| YES | 8 (18%) | 31 (20%) | |
| NO | 36 (82%) | 122 (80%) | |
| Chronic kidney disease | | | 0.7 |
| YES | 2 (4.5%) | 12 (7.8%) | |
| NO | 42 (95%) | 141 (92%) | |
| CANCER | | | 0.5 |
| YES | 4 (9.1%) | 8 (5.2%) | |
| NO | 40 (91%) | 145 (95%) | |
Table 5.
Vaccine type and delay between complete vaccination and admission date.
Table 5.
Vaccine type and delay between complete vaccination and admission date.
| Vaccin Manufacturer | Average Difference between Vaccination and Admission Date (Months) |
|---|
| BNT162b2 | 6 |
| ChAdOx1-S | 5 |
| Ad26.COV2.S | 2 |
3.2. Disease Severity Assessed by CT Score and Padua Score
The severity of COVID-19, assessed by CT visual score and Padua score, revealed significant differences between vaccinated and unvaccinated groups. The unvaccinated group exhibited a higher frequency of severe forms of the disease (60% vs. 36%,
p < 0.001) (
Figure 2).
An ordinal regression model (
Table 6) indicated that unvaccinated individuals had 3.5 times higher odds of a severe disease form. CT scan determined pulmonary involvement was significantly higher in the unvaccinated group (median = 40%) compared to the vaccinated group (median = 22%,
p = 0.005) (
Figure 3).
Multivariate regression analysis (
Table 7) highlighted significant associations between lung involvement and vaccination status, with unvaccinated patients showing 11.5% higher lung involvement.
3.3. Padua Score
For the Padua score, median values did not differ significantly (Wilcoxon rank-sum test
p = 0.07). Distribution levels are displayed in
Figure 4.
We have compared two linear regression models using the Padua score, one with and one without vaccination status as a prediction variable. ANOVA analysis was not statistically significant (
p = 0.38), so we concluded that the Padua score was not influenced by vaccination status. Univariate and multivariate linear regression results of the Padua score, including the vaccination status, age, sex, and BMI, are displayed in
Table 8.
3.4. Oxygen Therapy, Ventilation Requirement and the Dynamic of ABG
Oxygen requirement comparisons revealed higher needs in the unvaccinated group at hospital admission and during hospitalization (
p = 0.003,
p = 0.047) (
Table 9). Non-invasive ventilation was more frequent in the unvaccinated group.
Differences in arterial blood gas (ABG) parameters were observed (
Figure 5,
Figure 6,
Figure 7,
Figure 8 and
Figure 9), with unvaccinated individuals showing higher pCO
2 values at discharge (
p < 0.001).
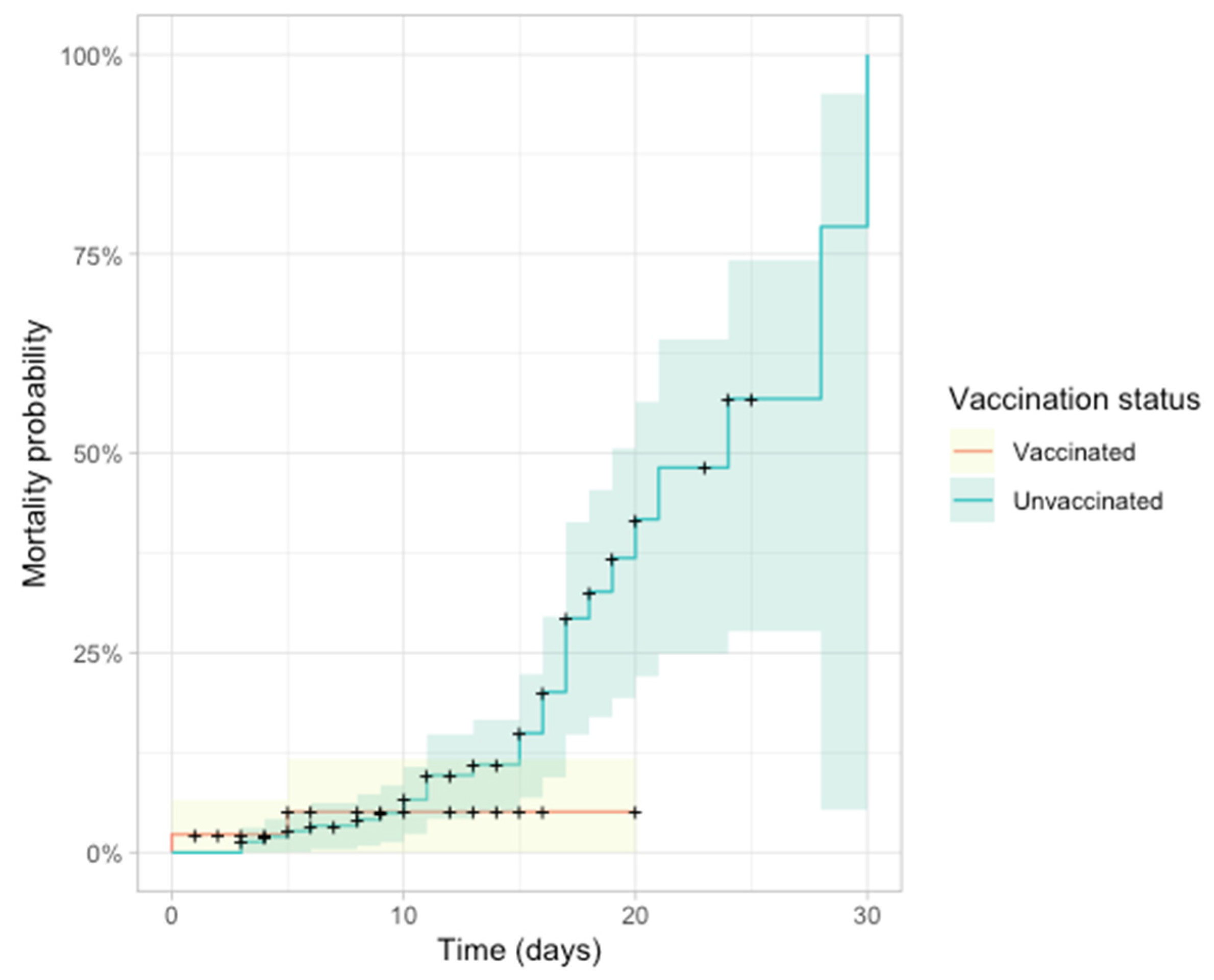
3.5. ICU Admission and Mortality
ICU admission and mortality rates were significantly higher in the unvaccinated group (
p = 0.07,
p = 0.03) (
Table 10). Stratification by disease severity demonstrated a significant association between disease severity and ICU admission/mortality (
Table 11).
Figure 10 illustrates the Kaplan–Meier plot, indicating higher mortality probability in the unvaccinated group after day 20.
4. Discussion
The emergence of the Delta variant has introduced unprecedented challenges to our understanding and management of COVID-19 [
22,
23]. This highly transmissible variant has not only complicated the existing narrative of the pandemic but has also underscored the dynamic nature of the virus, requiring swift adaptations in our approach to diagnosis, treatment, and prevention. The ongoing evolution of the virus necessitates a continuous pursuit of knowledge and the development of flexible strategies to effectively navigate the complexities introduced by emerging variants [
24,
25]. In this study, we have classified the patients infected with the Delta variant by their vaccination status to further explore the vaccination’s impact on disease severity and outcomes.
Our meticulous focus on patients infected with the Delta variant reveals compelling evidence regarding the efficacy of vaccination against severe disease associated with this highly transmissible strain. While breakthrough infections occurred among both fully vaccinated and unvaccinated individuals, our findings underscore the vaccine’s protective advantage, particularly in preventing severe forms of the illness.
In the context of the Delta variant, our study aligns with and extends existing research on the efficacy of COVID-19 vaccines. Notably, our results contribute to the growing body of evidence supporting the vaccines’ resilience against the Delta variant [
26,
27].
A preprint study analysing data from Scotland, found that the Pfizer-BioNTech vaccine was 79% effective at preventing symptomatic infection from the Delta variant. The study also found that the vaccine was 90% effective for preventing hospitalization [
28].
A study conducted by Bernal et al. from UK on 19109 patients with the Alpha or Delta variant showed that after one dose of the vaccine (BNT162b2 or ChAdOx1 nCoV-19), the effectiveness was lower in the Delta variant group versus Alpha variant group (30.7% versus 48.7%), and these results were almost the same for both types of vaccines. Regarding the two doses of vaccines, the effectiveness was 93.7% for the Alpha variant and 88% for Delta among those vaccinated with Pfizer. In the ChAdOx1 nCoV-19 vaccine group, the effectiveness was 74.5% for those with the Alpha variant and 67.0% for those with the Delta variant [
6].
We showed that the vaccination effectiveness drops after a period of 3–6 months depending on the type of vaccine used, with a shorter period in those vaccinated with Ad26.COV2.S. Our results are aligned with those of Nordström et al. whose study concerned patients previously vaccinated with heterologous immunisation that underwent Delta infection [
29]. Feikin et al. in a meta-analysis showed that after 6 months following complete vaccination, there was a decline in vaccine effectiveness against severe disease, averaging between 9.5 and 10.0 percentage points [
30]. In a cohort from USA, composed of individuals infected with Delta variant, lower effectiveness was noted in those aged 65 years or older and in those who were administered the Ad26.COV2.S vaccine [
31].
While COVID-19 vaccines offer numerous benefits, it is essential to consider the associated risks. Serious adverse events (SAEs) accounted for a significant proportion of reported adverse events (AEs), comprising 25.23% of cases in the VigiBase database. Fatalities occurred in 0.40% of total SAEs attributed to the Pfizer-BioNTech vaccine, with data from clinical trials indicating deaths in two recipients (0.01%), both aged over 55. Non-fatal SAEs were reported in 0.6% of cases, with appendicitis (0.04%), acute myocardial infarction (0.02%), and cerebrovascular accident (0.02%) being the most common. Similarly, fatalities were observed in 1.23% of total SAEs linked to the Moderna vaccine, with myocardial infarction (0.03%), cholecystitis (0.02%), and nephrolithiasis (0.02%) among the frequently reported SAEs. Adverse events associated with the AstraZeneca COVID-19 vaccine, as reported by the Medicines & Healthcare products Regulatory Agency (MHRA), were primarily classified as general disorders and administration site conditions, including injection site reactions/pain, fatigue, headache, and nausea [
32].
4.1. Top of Form
The recommendations for COVID-19 vaccination have evolved over time, reflecting the dynamic nature of the pandemic and the emergence of new variants. However, with the emergence of subsequent variants like Omicron, which exhibit even more attenuated disease progression, there has been a discernible shift in vaccination strategies. At the time of our investigation, Romania exhibited one of the lowest vaccination rates in Europe. [
33,
34].
4.2. Bottom of Form
CT Scan and Lung Involvement. Our analysis of CT scan findings sheds light on the extent of lung involvement, a critical marker of disease severity. These findings resonate with studies investigating the impact of the Delta variant on pulmonary manifestations. For instance, Kumari et al. demonstrated that complete vaccination led to significantly lower mean CT scores (14.18 ± 7.223) compared to unvaccinated individuals (11.1 ± 6.016) [
35]. Another study by Jong Eun Lee et al. found a higher number of negative CT scans in fully vaccinated individuals compared to the unvaccinated group (
p < 0.001) [
36].
Padua Score and VTE Risk. Incorporating the Padua score to assess the risk of venous thromboembolism (VTE) adds a valuable dimension to our study. While our results show no significant influence of vaccination status on the Padua score, it remains a crucial tool for assessing VTE risk. This finding resonates with Marietta et al.’s study, which found that a Padua score of four or higher was associated with a significantly higher risk of VTE in COVID-19 patients [
37].
Oxygen Requirement and Respiratory Failure. Our observations regarding oxygen requirements underscore the severity of respiratory failure, particularly in unvaccinated individuals. These findings align with studies suggesting that vaccination significantly reduces the risk of severe disease, hospitalization, and mortality. For example, Balachandran et al. found that vaccines reduced the risk of non-invasive ventilation need by 48% compared to unvaccinated individuals (OR = 0.52, 95% CI = 0.3–0.91) [
27].
Arterial Blood Parameters. The significance of oxygen saturation levels in assessing disease severity cannot be overstated. Our study contributes to this understanding, highlighting the potential impact of vaccination on maintaining higher oxygen saturation levels. Korishettar et al.’s study, involving 820 patients, showed that unvaccinated patients had significantly lower mean oxygen saturation levels compared to vaccinated patients [
38].
ICU Admission and Mortality. Our results reveal a significantly higher rate of ICU admission and mortality among the unvaccinated, affirming the pivotal role of vaccination in preventing severe outcomes. This is consistent with global studies, including one conducted by Public Health England, which found that fully vaccinated individuals had an 84% lower risk of hospitalization and an 89% lower risk of death compared to unvaccinated individuals [
39].
Length of Hospitalization. The relationship between hospitalization length and mortality rates underscores the broader implications of vaccination on patient outcomes. While statistically non-significant, our findings echo studies showing a shorter hospital stay for vaccinated individuals and a potential link between extended hospitalization and increased mortality in unvaccinated patients. Dagan et al.’s study, analysing 1107 COVID-19 patients in Israel, found that the length of hospitalization was significantly shorter for fully vaccinated patients compared to unvaccinated patients [
40].
5. Limitations
Our study, comparing vaccinated and unvaccinated COVID-19 patients, have some potential limitations. The relatively small number of patients, particularly within the vaccinated group, may introduce a potential source of bias. It is essential to acknowledge that, at the time of our study, the vaccination rate in our country was notably low, reflecting the early stages of vaccine rollout. Another limitation is the selection bias. The inherent risk of selection bias must be acknowledged, as vaccinated individuals might exhibit different health-conscious behaviours or possess distinct risk profiles unrelated to vaccination status. These variations could contribute to differences in outcomes, necessitating cautious interpretation of our findings. Also, the diversity in vaccine types administered to our study population introduces a layer of complexity. Different vaccines may exhibit varying efficacy rates, potential side effects, and levels of protection against the Delta variant. Recognizing this variability is crucial for a comprehensive understanding of our results. Furthermore, timing of vaccination is another bias, because the study included individuals who received vaccines at different times, affecting the level of immunity and susceptibility to the virus. Also, the study’s follow-up period may not be long enough to capture long-term effects of vaccination among the studied population.
6. Conclusions
In summary, our study presents compelling insights into the notable efficacy of COVID-19 vaccination against severe SARS-CoV-2 infection, contributing valuable perspectives to the discourse on pandemic management. The observed protective effects of the vaccine are instrumental, demonstrating a significant reduction in the incidence of severe disease, alongside notable decreases in the rates of ICU admission and mortality among hospitalized patients grappling with severe SARS-CoV-2 infection.
Unique to our investigation is the comprehensive examination of oxygen/ventilation requirements and the nuanced analysis of oxygen interface types at various time points. This reveals a distinct pattern of heightened oxygen needs in unvaccinated groups upon hospital admission and during hospitalization. These nuanced findings underscore the pivotal role of vaccination in not only preventing severe disease outcomes but also in shaping the trajectory of oxygen supplementation needs.
As we navigate the complexities of the COVID-19 landscape, our study positions vaccination as a paramount strategy in mitigating hospitalization, ICU admissions, and mortality. The evidence presented herein reinforces the centrality of vaccination as a frontline medical intervention, establishing its indisputable efficacy in combatting the challenges posed by the COVID-19 pandemic. Moving forward, our findings contribute to the evolving understanding of vaccination outcomes, emphasizing its pivotal role in public health strategies aimed at reducing the burden of severe SARS-CoV-2 infections.
Author Contributions
Conceptualization, D.-M.V., L.-Ș.M. and D.-A.T.; methodology, D.-M.V., O.-E.M., A.C.T. and M.A.N.; software, A.-O.M.; validation, D.-M.V., M.A.N., A.C.T. and D.-A.T.; formal analysis, I.M.C., L.-Ș.M. and T.-G.A.; investigation, D.-M.V., D.G., I.F. and I.M.C.; resources, D.-M.V., L.-Ș.M. and D.-A.T.; data curation, I.M.C., I.F., O.-E.M., A.C.T. and A.-O.M.; writing—original draft preparation, D.-M.V. and L.-Ș.M.; writing—review and editing, M.A.N., C.D.G. and T.-G.A.; visualization, T.-G.A.; supervision, D.-A.T.; project administration, D.-M.V. and D.-A.T.; funding acquisition, D.-M.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the ethical approval committee of “Iuliu Hațieganu” Cluj-Napoca, Approval No. (number: 60/2023).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data presented in this study are available on request from the first author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; de Silva, T.I.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; et al. SARS-CoV-2 Variant Biology: Immune Escape, Transmission and Fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef]
- Nesseler, N.; Fadel, G.; Mansour, A.; Para, M.; Falcoz, P.E.; Mongardon, N.; Porto, A.; Bertier, A.; Levy, B.; Cadoz, C.; et al. Extracorporeal Membrane Oxygenation for Respiratory Failure Related to COVID-19: A Nationwide Cohort Study. Anesthesiology 2022, 136, 732–748. [Google Scholar] [CrossRef] [PubMed]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; et al. Effectiveness of MRNA-1273 against Delta, Mu, and Other Emerging Variants of SARS-CoV-2: Test Negative Case-Control Study. BMJ 2021, 375, e068848. [Google Scholar] [CrossRef] [PubMed]
- Hitchings, M.D.T.; Ranzani, O.T.; Torres, M.S.S.; de Oliveira, S.B.; Almiron, M.; Said, R.; Borg, R.; Schulz, W.L.; de Oliveira, R.D.; da Silva, P.V.; et al. Effectiveness of CoronaVac among Healthcare Workers in the Setting of High SARS-CoV-2 Gamma Variant Transmission in Manaus, Brazil: A Test-Negative Case-Control Study. Lancet Reg. Health Am. 2021, 1, 100025. [Google Scholar] [CrossRef] [PubMed]
- Al Fayez, N.; Nassar, M.S.; Alshehri, A.A.; Alnefaie, M.K.; Almughem, F.A.; Alshehri, B.Y.; Alawad, A.O.; Tawfik, E.A. Recent Advancement in MRNA Vaccine Development and Applications. Pharmaceutics 2023, 15, 1972. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccines: MODERNA|PFIZER/BIONTECH|ASTRAZENECA-YouTube. Available online: https://www.youtube.com/watch?v=35Idb_lCU4o (accessed on 11 March 2023).
- How Does Vaxzevria, the Oxford-AstraZeneca COVID-19 Vaccine Work?|COVID-19 Info Vaccines. Available online: https://www.covid19infovaccines.com/en-posts/how-does-vaxzevria-the-oxford-astrazeneca-covid-19-vaccine-work (accessed on 11 March 2023).
- Mitsi, E.; Diniz, M.O.; Reiné, J.; Collins, A.M.; Robinson, R.E.; Hyder-Wright, A.; Farrar, M.; Liatsikos, K.; Hamilton, J.; Onyema, O.; et al. Respiratory Mucosal Immune Memory to SARS-CoV-2 after Infection and Vaccination. Nat. Commun. 2023, 14, 6815. [Google Scholar] [CrossRef] [PubMed]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, V.A.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and Metabolic Disease: Mechanisms and Clinical Management. Lancet. Diabetes Endocrinol. 2021, 9, 786. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Delta Variant: What Is Happening with Transmission, Hospital Admissions, and Restrictions? BMJ 2021, 373, n1513. [Google Scholar] [CrossRef]
- Alizon, S.; Haim-Boukobza, S.; Foulongne, V.; Verdurme, L.; Trombert-Paolantoni, S.; Lecorche, E.; Roquebert, B.; Sofonea, M.T. Rapid Spread of the SARS-CoV-2 Delta Variant in Some French Regions, June 2021. Eurosurveillance 2021, 26, 2100573. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.M.; Cui, L.; Toh, M.P.H.S.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and Virological Features of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants of Concern: A Retrospective Cohort Study Comparing B.1.1.7 (Alpha), B.1.351 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2022, 75, E1128–E1136. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, H. COVID-19 and Metabolic Syndrome. Best Pract. Res. Clin. Endocrinol. Metab. 2023, 37, 101753. [Google Scholar] [CrossRef] [PubMed]
- Rico-Martín, S.; Calderón-García, J.F.; Basilio-Fernández, B.; Clavijo-Chamorro, M.Z.; Muñoz-Torrero, J.F.S. Metabolic Syndrome and Its Components in Patients with COVID-19: Severe Acute Respiratory Syndrome (SARS) and Mortality. A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 162. [Google Scholar] [CrossRef]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.H.; Dong, J.H.; An, W.M.; Lv, X.Y.; Yin, X.P.; Zhang, J.Z.; Dong, L.; Ma, X.; Zhang, H.J.; Gao, B.L. Clinical and Computed Tomographic Imaging Features of Novel Coronavirus Pneumonia Caused by SARS-CoV-2. J. Infect. 2020, 80, 394–400. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Der Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- ORDIN 2103 12/10/2021 Portal Legislativ. Available online: https://legislatie.just.ro/Public/DetaliiDocument/247389 (accessed on 25 March 2023).
- Samieefar, N.; Rashedi, R.; Akhlaghdoust, M.; Mashhadi, M.; Darzi, P.; Rezaei, N. Delta Variant: The New Challenge of COVID-19 Pandemic, an Overview of Epidemiological, Clinical, and Immune Characteristics. Acta Bio Medica Atenei Parm. 2022, 93, e2022179. [Google Scholar] [CrossRef]
- Wei, L.; Zhaoyin, L.; Yuxuan, Z.; Yumin, Z.; Elita, L.Y.; Masrur, A.; Yu, M. Spatiotemporal Patterns and Progression of the Delta Variant of COVID-19 and Their Health Intervention Linkages in Southeast Asia. medRxiv 2021. [Google Scholar] [CrossRef]
- Zhang, M.; He, Y.; Jie, Z. Delta Variant: Partially Sensitive to Vaccination, but Still Worth Global Attention. J. Transl. Intern. Med. 2022, 10, 227. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Delta Variant Is Now UK’s Most Dominant Strain and Spreading through Schools. BMJ 2021, 373, n1445. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: Unvaccinated Face 11 Times Risk of Death from Delta Variant, CDC Data Show. BMJ 2021, 374, n2282. [Google Scholar] [CrossRef]
- Balachandran, S.; Moni, M.; Sathyapalan, D.T.; Varghese, P.; Jose, M.P.; Murugan, M.R.; Rajan, C.; Saboo, D.; Nair, S.S.; Varkey, R.A.; et al. A Comparison of Clinical Outcomes between Vaccinated and Vaccine-Naive Patients of COVID-19, in Four Tertiary Care Hospitals of Kerala, South India. Clin. Epidemiol. Glob. Health 2022, 13, 100971. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of Heterologous ChAdOx1 NCoV-19 and MRNA Prime-Boost Vaccination against Symptomatic COVID-19 Infection in Sweden: A Nationwide Cohort Study. Lancet Reg. Health Eur. 2021, 11, 100249. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of Effectiveness of Vaccines against SARS-CoV-2 Infection and COVID-19 Disease: Results of a Systematic Review and Meta-Regression. Lancet 2022, 399, 924. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Dutta, S.; Kaur, R.J.; Bhardwaj, P.; Sharma, P.; Ambwani, S.; Islam, S.; Tandon, A.; Abhayanand, J.P.; Sukhija, S.; Venkatesh, S.S.; et al. Adverse Events Reported from the COVID-19 Vaccines: A Descriptive Study Based on the WHO Database (VigiBase®). J. Appl. Pharm. Sci. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Enciu, B.G.; Pițigoi, D.; Zaharia, A.; Popescu, R.; Niculcea, A.; Crăciun, M.D.; Pistol, A. COVID-19 Vaccination in Romania and the Benefits of the National Electronic Registry of Vaccinations. Vaccines 2023, 11, 370. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Covaciu, O.; Chereches, R.M.; Diaconu, G.; Dumitra, G.G.; Gheorghita, V.; Popovici, E.D. Prospects of COVID-19 Vaccination in Romania: Challenges and Potential Solutions. Front. Public Health 2021, 9, 644538. [Google Scholar] [CrossRef]
- Kumari, N.; Ahmad, M.S.; Gupta, A.; Prakash, G. Comparison of HRCT Chest Findings among Vaccinated and Non-Vaccinated COVID-19 Patients. Int. J. Res. Med. Sci. 2022, 10, 2911–2915. [Google Scholar] [CrossRef]
- Lee, J.E.; Hwang, M.; Kim, Y.H.; Chung, M.J.; Sim, B.H.; Chae, K.J.; Yoo, J.Y.; Jeong, Y.J. Imaging and Clinical Features of COVID-19 Breakthrough Infections: A Study. Radiology 2022, 303, 682. [Google Scholar] [CrossRef] [PubMed]
- Marietta, M.; Ageno, W.; Artoni, A.; De Candia, E.; Gresele, P.; Marchetti, M.; Marcucci, R.; Tripodi, A. COVID-19 and Haemostasis: A Position Paper from Italian Society on Thrombosis and Haemostasis (SISET). Blood Transfus. 2020, 18, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Korishettar, G.; Chikkahonnaiah, P.; Tulimilli, S.R.V.; Dallavalasa, S.; Byrappa, S.H.; Madhunapantula, S.R.V.; Veeranna, R.P. Assessment of Clinical Profile and Treatment Outcome in Vaccinated and Unvaccinated SARS-CoV-2 Infected Patients. Vaccines 2022, 10, 1125. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.L.; Lutrick, K.; et al. Prevention and Attenuation of COVID-19 with the BNT162b2 and MRNA-1273 Vaccines. N. Engl. J. Med. 2021, 385, 320–329. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 MRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









