
High Frequency of Osteophytes Detected by High-Resolution Ultrasound at the Finger Joints of Asymptomatic Factory Workers
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. General Investigations
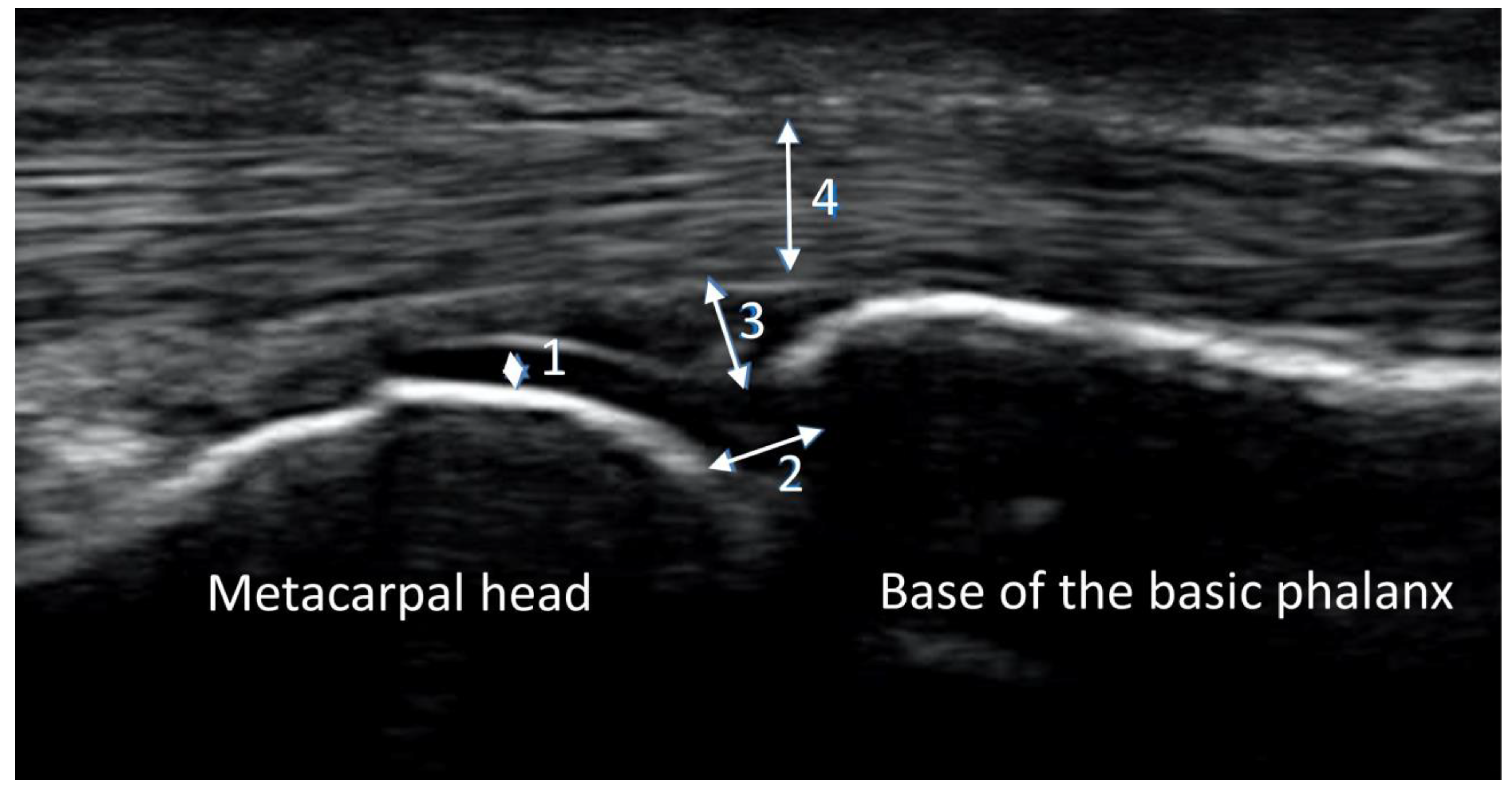
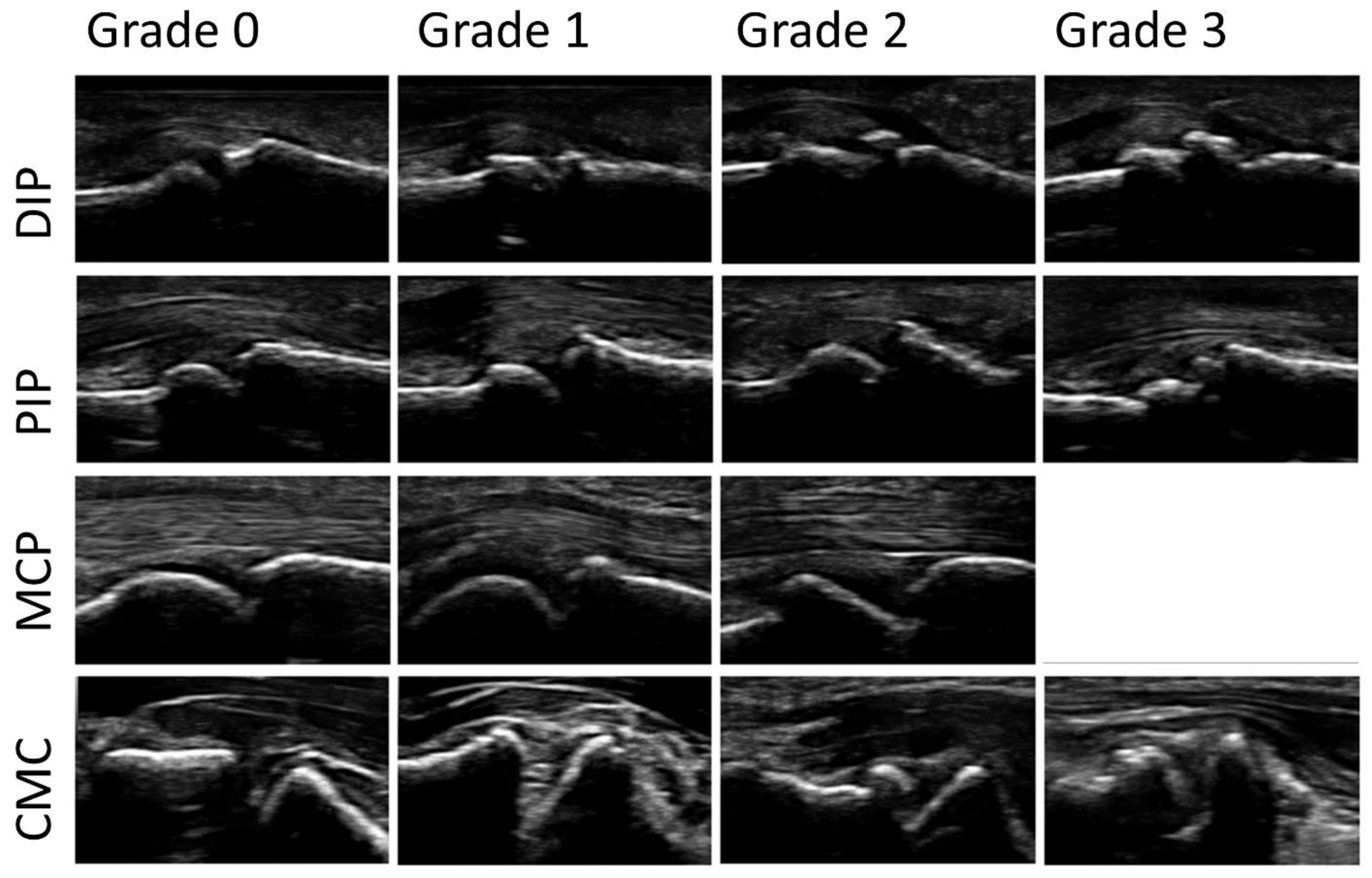
2.3. Ultrasound Imaging
2.4. Reading Procedures
2.5. Statistical Analysis
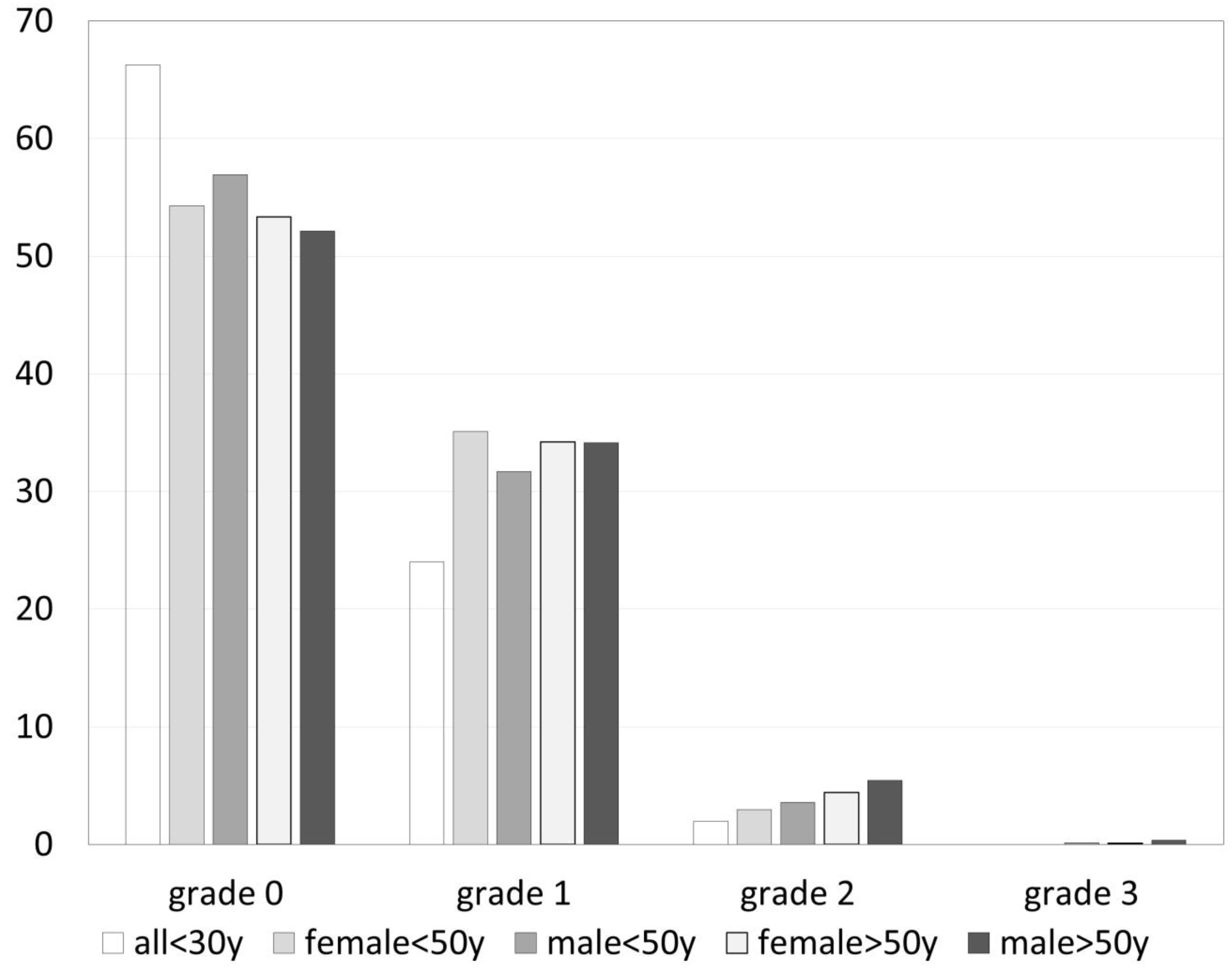
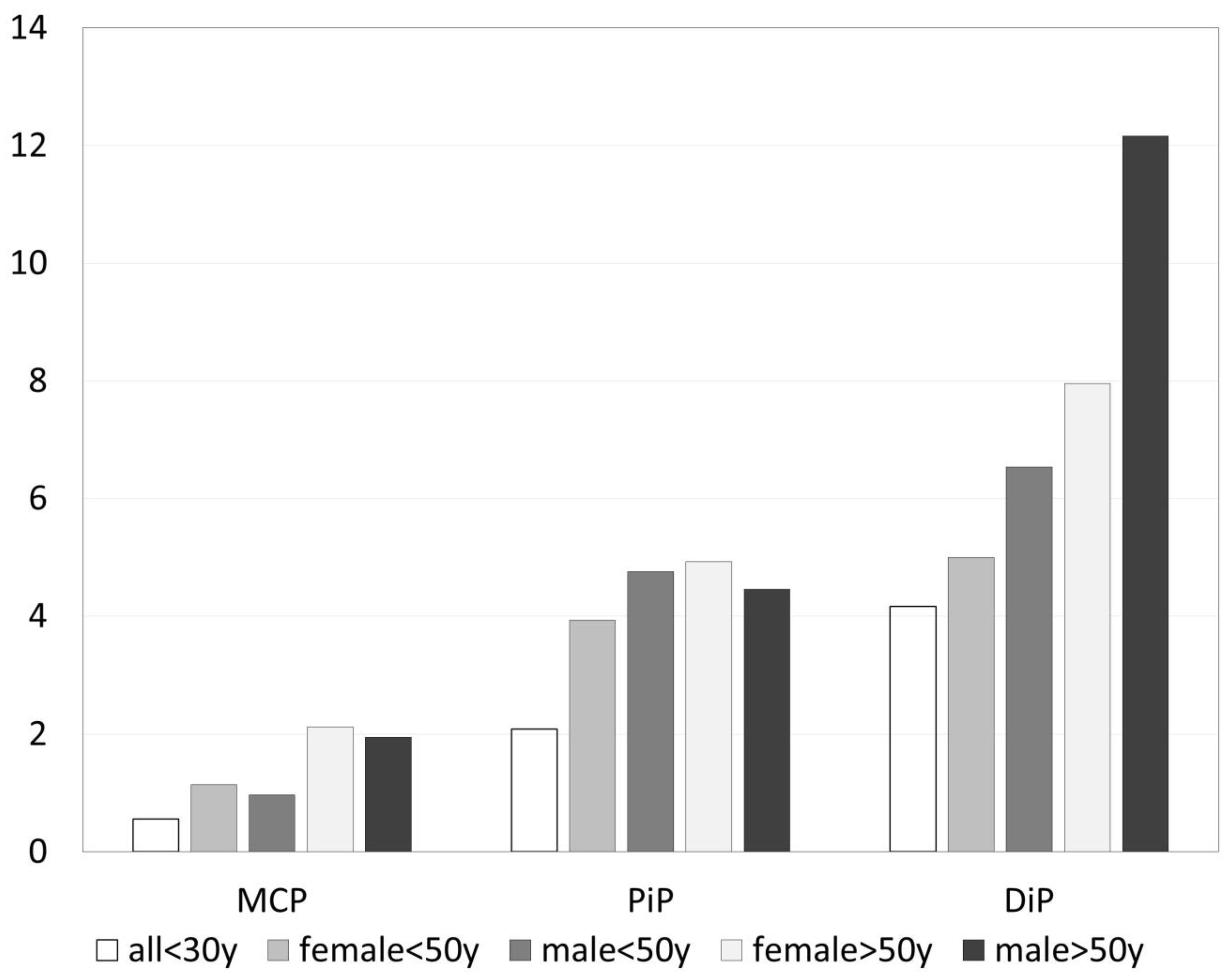
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haugen, I. Hand osteoarthritis: Current knowledge and new ideas. Scand. J. Rheumatol. 2016, 45, 58–63. [Google Scholar] [CrossRef]
- Kloppenburg, M.; Bøyesen, P.; Smeets, W.; Haugen, I.; Liu, R.; Visser, W.; van der Heijde, D.M. Report from the OMERACT Hand Osteoarthritis Special Interest Group: Advances and Future Research Priorities. J. Rheumatol. 2014, 41, 810–818. [Google Scholar] [CrossRef]
- Slatkowsky-Christensen, B.; Mowinckel, P.; Loge, J.H.; Kvien, T.K. Health-related quality of life in women with symptomatic hand osteoarthritis: A comparison with rheumatoid arthritis patients, healthy controls, and normative data. Arthritis Rheum. 2007, 57, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Alarcon, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Gray, R.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum. 1990, 33, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Hochberg, M.; Vignon, E.; Maheu, E. Session 2: Clinical aspects. Clinical assessment of hand OA. Osteoarthr. Cartil. 2000, 8, S38–S40. [Google Scholar] [CrossRef]
- Neogi, T.; Zhang, Y. Epidemiology of Osteoarthritis. Rheum. Dis. Clin. N. Am. 2013, 39, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.P.; Simon, D.; Englbrecht, M.; Haschka, J.; Kleyer, A.; Bayat, S.; Hueber, A.; Pereira, R.M.R.; Rech, J.; Schett, G. Quantification and Impact of Secondary Osteoarthritis in Patients with Anti-Citrullinated Protein Antibody-Positive Rheumatoid Arthritis. Arthritis Rheumatol. 2016, 68, 2114–2121. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.O.; Günther, K.-P.; Goronzy, J.; Albrecht, K.; Chenot, J.-F.; Callhoff, J.; Richter, A.; Kasch, R.; Ahrens, W.; Becher, H.; et al. Häufigkeiten muskuloskelettaler Symptome und Erkrankungen in der bevölkerungsbezogenen NAKO Gesundheitsstudie. Bundesgesundheitsblatt 2020, 63, 415–425. [Google Scholar] [CrossRef]
- Bellach, B.M. Bundesgesundheitssurvey 1998; Das Gesundheitswesen; Thieme: Stuttgart, Germany, 1999. [Google Scholar]
- Steinberg, S.U.; Behrendt, G.; Caffier, K.; Schultz, M. Jakob Leitmerkmalmethode Manuelle Arbeitsprozesse. Bundesanstalt für Arbeitsschutz und Arbeitsmedizin; Springer: Berlin/Heidelberg, Germany, 2007; ISBN 978-3-88261-073-4. [Google Scholar]
- Lautwein, A.; Ostendorf, B.; Vordenbäumen, S.; Liedmann, A.; Brinks, R.; Giulini, M.; Ohrndorf, S.; Backhaus, M.; Acar, H.; Sander, O.; et al. Musculoskeletal ultrasound as a screening-tool for rheumatoid arthritis: Results of the “Rheuma-Truck” screening and awareness initiative. Adv. Rheumatol. 2022, 62, 1. [Google Scholar] [CrossRef]
- Federal Institute for Occupational Safety and Health. Formblatt Leitmerkmalmethode Manuelle Arbeitsprozesse. Berlin, Group 3.4, Version 2007. Available online: http://www.baua.de/de/Publikationen/Fachbeitraege/F1994.html (accessed on 20 January 2012).
- Zhang, W.; Doherty, M.; Leeb, B.F.; Alekseeva, L.; Arden, N.K.; Bijlsma, J.W.; Dincer, F.; Dziedzic, K.; Hauselmann, H.J.; Kaklamanis, P.; et al. EULAR evidence-based recommendations for the diagnosis of hand osteoarthritis: Report of a task force of ESCISIT. Ann. Rheum. Dis. 2009, 68, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Keen, H.I.; Lavie, F.; Wakefield, R.J.; D’Agostino, M.-A.; Hammer, H.B.; Hensor, E.; Pendleton, A.; Kane, D.; Guerini, H.; Schueller-Weidekamm, C.; et al. The development of a preliminary ultrasonographic scoring system for features of hand osteoarthritis. Ann. Rheum. Dis. 2008, 67, 651–655. [Google Scholar] [CrossRef]
- Kortekaas, M.C.; Kwok, W.-Y.; Reijnierse, M.; Huizinga, T.W.J.; Kloppenburg, M. Osteophytes and joint space narrowing are independently associated with pain in finger joints in hand osteoarthritis. Ann. Rheum. Dis. 2011, 70, 1835–1837. [Google Scholar] [CrossRef] [PubMed]
- Mathiessen, A.; Haugen, I.K.; Slatkowsky-Christensen, B.; Bøyesen, P.; Kvien, T.K.; Hammer, H.B. Ultrasonographic assessment of osteophytes in 127 patients with hand osteoarthritis: Exploring reliability and associations with MRI, radiographs and clinical joint findings. Ann. Rheum. Dis. 2013, 72, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Hammer, H.B.; Iagnocco, A.; Mathiessen, A.; Filippucci, E.; Gandjbakhch, F.; Kortekaas, M.C.; Möller, I.; Naredo, E.; Wakefield, R.J.; Aegerter, P.; et al. Global ultrasound assessment of structural lesions in osteoarthritis: A reliability study by the OMERACT ultrasonography group on scoring cartilage and osteophytes in finger joints. Ann. Rheum. Dis. 2016, 75, 402–407. [Google Scholar] [CrossRef]
- Gale, C.R.; Martyn, C.N.; Cooper, C.; Sayer, A.A. Grip strength, body composition, and mortality. Leuk. Res. 2007, 36, 228–235. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Arvandi, M.; Strasser, B.; Meisinger, C.; Volaklis, K.; Gothe, R.M.; Siebert, U.; Ladwig, K.-H.; Grill, E.; Horsch, A.; Laxy, M.; et al. Gender differences in the association between grip strength and mortality in older adults: Results from the KORA-age study. BMC Geriatr. 2016, 16, 201. [Google Scholar] [CrossRef]
- Kim, Y.; Wijndaele, K.; Lee, D.-C.; Sharp, S.J.; Wareham, N.; Brage, S. Independent and joint associations of grip strength and adiposity with all-cause and cardiovascular disease mortality in 403,199 adults: The UK Biobank study. Am. J. Clin. Nutr. 2017, 106, 773–782. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Welsh, P.; Lyall, D.M.; Steell, L.; Petermann, F.; Anderson, J.; Iliodromiti, S.; Sillars, A.; Graham, N.; Mackay, D.F.; et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: Prospective cohort study of half a million UK Biobank participants. BMJ 2018, 361, k1651. [Google Scholar] [CrossRef]
- Xie, K.H.; Han, X.; Zheng, W.J.; Zhuang, S.F. Low Grip Strength and Increased Mortality Hazard among Middle-Aged and Older Chinese Adults with Chronic Diseases. Biomed. Environ. Sci. 2023, 36, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Liu, L.; Wang, J.; Gao, Y.; Guo, Z.; Ping, Z. Linear association between grip strength and all-cause mortality among the elderly: Results from the SHARE study. Aging Clin. Exp. Res. 2021, 33, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, L.; Nevitt, M.C.; Niu, J.; Goggins, J.P.; Aliabadi, P.; Yu, W.; Lui, L.-Y.; Felson, D.T. Lower prevalence of hand osteoarthritis among Chinese subjects in Beijing compared with white subjects in the United States: The Beijing Osteoarthritis Study. Arthritis Rheum. 2003, 48, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Dahaghin, S.; Bierma-Zeinstra, S.M.A.; Ginai, A.Z.; Pols, H.A.P.; Hazes, J.M.W.; Koes, B.W. Prevalence and pattern of radiographic hand osteoarthritis and association with pain and disability (the Rotterdam study). Ann. Rheum. Dis. 2005, 64, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Wilder, F.; Barrett, J.; Farina, E. Joint-specific prevalence of osteoarthritis of the hand. Osteoarthr. Cartil. 2006, 14, 953–957. [Google Scholar] [CrossRef]
- Szoeke, C.; Cicuttini, F.; Guthrie, J.; Clark, M.; Dennerstein, L. Factors affecting the prevalence of osteoarthritis in healthy middle-aged women: Data from the longitudinal Melbourne Women’s Midlife Health Project. Bone 2006, 39, 1149–1155. [Google Scholar] [CrossRef]
- Kwok, W.; Bijsterbosch, J.; Malm, S.; Biermasz, N.; Huetink, K.; Nelissen, R.; Meulenbelt, I.; Huizinga, T.; Klooster, R.v.; Stoel, B.; et al. Validity of joint space width measurements in hand osteoarthritis. Osteoarthr. Cartil. 2011, 19, 1349–1355. [Google Scholar] [CrossRef]
- Haugen, I.K.; Englund, M.; Aliabadi, P.; Niu, J.; Clancy, M.; Kvien, T.K.; Felson, D.T. Prevalence, incidence and progression of hand osteoarthritis in the general population: The Framingham Osteoarthritis Study. Rheumatology 2011, 70, 1581–1586. [Google Scholar] [CrossRef]
- Caspi, D.; Flusser, G.; Farber, I.; Ribak, J.; Leibovitz, A.; Habot, B.; Yaron, M.; Segal, R. Clinical, radiologic, demographic, and occupational aspects of hand osteoarthritis in the elderly. Semin. Arthritis Rheum. 2001, 30, 321–331. [Google Scholar] [CrossRef]
- Kalichman, L.; Li, L.; Batsevich, V.; Malkin, I.; Kobyliansky, E. Prevalence, pattern and determinants of radiographic hand osteoarthritis in five Russian community-based samples. Osteoarthr. Cartil. 2010, 18, 803–809. [Google Scholar] [CrossRef]
- Kodama, R.; Muraki, S.; Oka, H.; Iidaka, T.; Teraguchi, M.; Kagotani, R.; Asai, Y.; Yoshida, M.; Morizaki, Y.; Tanaka, S.; et al. Prevalence of hand osteoarthritis and its relationship to hand pain and grip strength in Japan: The third survey of the ROAD study. Mod. Rheumatol. 2016, 26, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Sowers, M.; Lachance, L.; Hochberg, M.; Jamadar, D. Radiographically defined osteoarthritis of the hand and knee in young and middle-aged African American and Caucasian women. Osteoarthr. Cartil. 2000, 8, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Niu, J.; Kelly-Hayes, M.; Chaisson, C.E.; Aliabadi, P.; Felson, D.T. Prevalence of Symptomatic Hand Osteoarthritis and Its Impact on Functional Status among the Elderly: The Framingham Study. Am. J. Epidemiol. 2002, 156, 1021–1027. [Google Scholar] [CrossRef]
- Carmona, L. The burden of musculoskeletal diseases in the general population of Spain: Results from a national survey. Ann. Rheum. Dis. 2001, 60, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Andrianakos, A.A.; Kontelis, L.K.; Karamitsos, D.G.; Aslanidis, S.I.; Georgountzos, A.; Kaziolas, G.O.; Pantelidou, K.V.; Vafiadou, E.V.; Dantis, P.C. Prevalence of symptomatic knee, hand, and hip osteoarthritis in Greece. The ESORDIG study. J. Rheumatol. 2006, 33, 2507–2513. [Google Scholar]
- Keen, H.I.; Wakefield, R.J.; Grainger, A.J.; Hensor, E.M.A.; Emery, P.; Conaghan, P.G. Can ultrasonography improve on radiographic assessment in osteoarthritis of the hands? A comparison between radiographic and ultrasonographic detected pathology. Ann. Rheum. Dis. 2008, 67, 1116–1120. [Google Scholar] [CrossRef]
- Abraham, A.M.; Pearce, M.S.; Mann, K.D.; Francis, R.M.; Birrell, F. Population prevalence of ultrasound features of osteoarthritis in the hand, knee and hip at age 63 years: The Newcastle thousand families birth cohort. BMC Musculoskelet. Disord. 2014, 15, 162. [Google Scholar] [CrossRef]
- Hart, D.; Spector, T. Kellgren & Lawrence grade 1 osteophytes in the knee—Doubtful or definite? Osteoarthr. Cartil. 2003, 11, 149–150. [Google Scholar] [CrossRef]
- Mathiessen, A.; Slatkowsky-Christensen, B.; Kvien, T.K.; Haugen, I.K.; Hammer, H.B. Ultrasound-detected osteophytes predict the development of radiographic and clinical features of hand osteoarthritis in the same finger joints 5 years later. RMD Open 2017, 3, e000505. [Google Scholar] [CrossRef]
- Rossignol, M.; Leclerc, A.; Hilliquin, P.; Allaert, F.A.; Rozenberg, S.; Valat, J.-P.; Avouac, B.; Coste, P.; Savarieau, B.; Fautrel, B. Primary osteoarthritis and occupations: A national cross sectional survey of 10 412 symptomatic patients. Occup. Environ. Med. 2003, 60, 882–886. [Google Scholar] [CrossRef]
- Haara, M.M.; Manninen, P.; Kröger, H.; Arokoski, J.P.A.; Kärkkäinen, A.; Knekt, P.; Aromaa, A.; Heliövaara, M. Osteoarthritis of finger joints in Finns aged 30 or over: Prevalence, determinants, and association with mortality. Ann. Rheum. Dis. 2003, 62, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Zhang, Y.; Nevitt, M.C.; Xu, L.; Niu, J.; Lui, L.-Y.; Yu, W.; Aliabadi, P.; Felson, D.T. Chopstick arthropathy: The Beijing Osteoarthritis Study. Arthritis Rheum. 2004, 50, 1495–1500. [Google Scholar] [CrossRef] [PubMed]
- Kallman, D.A.; Wigley, F.M.; Scott, W.W.; Hochberg, M.C.; Tobin, J.D. The longitudinal course of hand osteoarthritis in a male population. Arthritis Rheum. 1990, 33, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Egger, P.; Coggon, D.; Hart, D.J.; Masud, T.; Cicuttini, F.; Doyle, D.V.; Spector, T.D. Generalized osteoarthritis in women: Pattern of joint involvement and approaches to definition for epidemiological studies. J. Rheumatol. 1996, 23, 1938–1942. [Google Scholar] [PubMed]
- Kalichman, L.; Cohen, Z.; Kobyliansky, E.; Livshits, G. Patterns of joint distribution in hand osteoarthritis: Contribution of age, sex, and handedness. Am. J. Hum. Biol. 2004, 16, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Cooley, H.M.; Stankovich, J.M. A cross sectional study of the association between sex, smoking, and other lifestyle factors and osteoarthritis of the hand. J. Rheumatol. 2002, 29, 1719–1724. [Google Scholar] [PubMed]
- Vlychou, M.; Koutroumpas, A.; Malizos, K.; Sakkas, L. Ultrasonographic evidence of inflammation is frequent in hands of patients with erosive osteoarthritis. Osteoarthr. Cartil. 2009, 17, 1283–1287. [Google Scholar] [CrossRef]
- Wittoek, R.; Carron, P.; Verbruggen, G. Structural and inflammatory sonographic findings in erosive and non-erosive osteoarthritis of the interphalangeal finger joints. Ann. Rheum. Dis. 2010, 69, 2173–2176. [Google Scholar] [CrossRef]
- Backhaus, M.; Kamradt, T.; Sandrock, D.; Loreck, D.; Fritz, J.; Wolf, K.J.; Raber, H.; Hamm, B.; Burmester, G.-R.; Bollow, M. Arthritis of the finger joints: A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum. 1999, 42, 1232–1245. [Google Scholar] [CrossRef]
- Szkudlarek, M.; Court-Payen, M.; Jacobsen, S.; Klarlund, M.; Thomsen, H.S.; Østergaard, M. Interobserver agreement in ultrasonography of the finger and toe joints in rheumatoid arthritis. Arthritis Rheum. 2003, 48, 955–962. [Google Scholar] [CrossRef]
- Szkudlarek, M.; Klarlund, M.; Narvestad, E.; Court-Payen, M.; Strandberg, C.; Jensen, K.; Thomsen, H.; Østergaard, M. Ultrasonography of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis: A comparison with magnetic resonance imaging, conventional radiography and clinical examination. Thromb. Haemost. 2006, 8, R52. [Google Scholar] [CrossRef]
- Bajaj, S.; Lopez-Ben, R.; Oster, R.; Alarcón, G.S. Ultrasound detects rapid progression of erosive disease in early rheumatoid arthritis: A prospective longitudinal study. Skelet. Radiol. 2007, 36, 123–128. [Google Scholar] [CrossRef]
- Hayashi, D.; Roemer, F.; Guermazi, A. Imaging for osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, P.; Bowen, C.; Ellis, R.; Rome, K.; Frecklington, M.; Carroll, M. Evaluation of osteoarthritic features in peripheral joints by ultrasound imaging: A systematic review. Osteoarthr. Cartil. Open 2021, 3, 100194. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, B.A.; Schousboe, M.; Terslev, L.; Iversen, N.; Lindegaard, H.; Savarimuthu, T.R.; Just, S.A. Ultrasound joint examination by an automated system versus by a rheumatologist: From a patient perspective. Hortic. Bras. 2022, 62, 30. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.B.H.; Just, S.A.; Andersen, J.K.H.; Savarimuthu, T.R. Applying cascaded convolutional neural network design further enhances automatic scoring of arthritis disease activity on ultrasound images from rheumatoid arthritis patients. Ann. Rheum. Dis. 2020, 79, 1189–1193. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Left Hand | Right Hand | |||
|---|---|---|---|---|
| Joint | Any | >Grade 1 | Any | >Grade 1 |
| DIP 2 | 59.6% | 9.2% | 66.7% | 12.2% |
| DIP 3 | 67.3% | 12.2% | 67.4% | 12.8% |
| DIP 4 | 56.2% | 7.3% | 65.6% | 11.1% |
| DIP 5 | 47.5% | 4.0% | 56.8% | 7.1% |
| PIP 2 | 45.8% | 6.1% | 48.5% | 4.5% |
| PIP 3 | 53.2% | 5.6% | 58.7% | 6.8% |
| PIP 4 | 51.5% | 4.2% | 51.4% | 4.5% |
| PIP 5 | 34% | 3.5% | 38.2% | 2.6% |
| MCP 2 | 14.6% | 0.2% | 19.8% | 1.2% |
| MCP 3 | 19.7% | 1.2% | 28.3% | 2.6% |
| MCP 4 | 12.3% | 0.2% | 18.1% | 0.7% |
| MCP 5 | 7.3% | 0.0% | 8.5% | 0.2% |
| CMC 1 | 40.1% | 6.4% | 37.5% | 4.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giulini, M.; Brinks, R.; Vordenbäumen, S.; Acar, H.; Richter, J.G.; Baraliakos, X.; Ostendorf, B.; Schneider, M.; Sander, O.; Sewerin, P. High Frequency of Osteophytes Detected by High-Resolution Ultrasound at the Finger Joints of Asymptomatic Factory Workers. J. Pers. Med. 2023, 13, 1343. https://doi.org/10.3390/jpm13091343
Giulini M, Brinks R, Vordenbäumen S, Acar H, Richter JG, Baraliakos X, Ostendorf B, Schneider M, Sander O, Sewerin P. High Frequency of Osteophytes Detected by High-Resolution Ultrasound at the Finger Joints of Asymptomatic Factory Workers. Journal of Personalized Medicine. 2023; 13(9):1343. https://doi.org/10.3390/jpm13091343
Chicago/Turabian StyleGiulini, Mario, Ralph Brinks, Stefan Vordenbäumen, Hasan Acar, Jutta G. Richter, Xenofon Baraliakos, Benedikt Ostendorf, Matthias Schneider, Oliver Sander, and Philipp Sewerin. 2023. "High Frequency of Osteophytes Detected by High-Resolution Ultrasound at the Finger Joints of Asymptomatic Factory Workers" Journal of Personalized Medicine 13, no. 9: 1343. https://doi.org/10.3390/jpm13091343