1. Introduction
Obesity is a complex medical condition that can lead to a wide range of health complications, many of which are linked to chronic low-grade systemic inflammation [
1]. Chronic inflammation occurs when the body’s immune response is constantly activated at a low level over an extended period. Some complications associated with obesity and the potential issues that can result from chronic low-grade systemic inflammation are type 2 diabetes, cardiovascular disease, metabolic syndrome, non-alcoholic fatty liver disease (NAFLD), respiratory issues, joint problems, cancer, neurological effects, hormonal dysregulation, psychological effects, immune dysfunction, and accelerated aging [
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13]. Obesity affects children from early childhood to late adolescence and is very likely to continue in their adult life. Over 340 million children and adolescents aged 5–19 years were overweight or dealing with obesity in 2016. The prevalence of overweight and obesity among children and adolescents aged 5–19 years has risen dramatically from just 4% in 1975 to over 18% in 2016. The rise occurred similarly among both boys and girls: in 2016, 18% of girls and 19% of boys were overweight [
14]. Obesity, amongst other definitions, could be described as abnormal or excessive fat accumulation that presents a major health hazard. It can be easily quantified via height and body weight percentiles in each age and gender group [
15,
16,
17]. All in all, obesity is one of the most prevalent non-communicable diseases and a major concern for public health worldwide, mainly due to its well-established pathophysiologic manifestations, such as insulin resistance, diabetes mellitus type 2, atherosclerosis, hypertension, or even some types of cancer. Obesity has a strong, persistent underlying inflammatory component, represented by a state of low-grade chronic systemic inflammation that is known to be harmful to the metabolism, endocrinology, and overall homeostasis of human systems. Earlier observations of elevated circulating levels of inflammatory cytokines and other mediators of inflammation in individuals living with obesity imply that inflammation is the consequence of tilting the stress axis. Obesity is directly linked to the adipose tissue metabolomic and transcriptomic microenvironment as a multimodal vector composed of a repertoire of genetic, cellular, and organ-level information streams due to the accumulation of excessive fat and the inevitable cytokine secretion [
18].
Lifestyle interventions play a crucial role in managing obesity and inflammation in children and adolescents. The most common changes in lifestyle consist in following a healthy diet and being active physically. Lifestyle interventions that promote a balanced, nutrient-rich diet can help reduce obesity and inflammation. Emphasizing the consumption of whole foods, fruits, vegetables, lean proteins, and healthy fats while reducing that of processed foods and sugary beverages can lead to weight loss and improved inflammatory markers [
19,
20]. Moreover, regular physical activity is associated with reduced obesity and improved inflammation in children and adolescents. Lifestyle interventions that encourage regular exercise can lead to weight management and the reduction of pro-inflammatory markers [
21,
22].
There have been numerous attempts in several studies to establish a correlation between obesity and stress indicators, inflammatory markers, or dysmetabolism markers in children and adults. Herein, an effort was made in the form of a meta-analysis to shed light on the elusive correlation of childhood and adolescent obesity with the above-mentioned physiological or molecular indicators and on how they can be modified by interventions focused on diet, exercise, supplements, or even drug therapy.
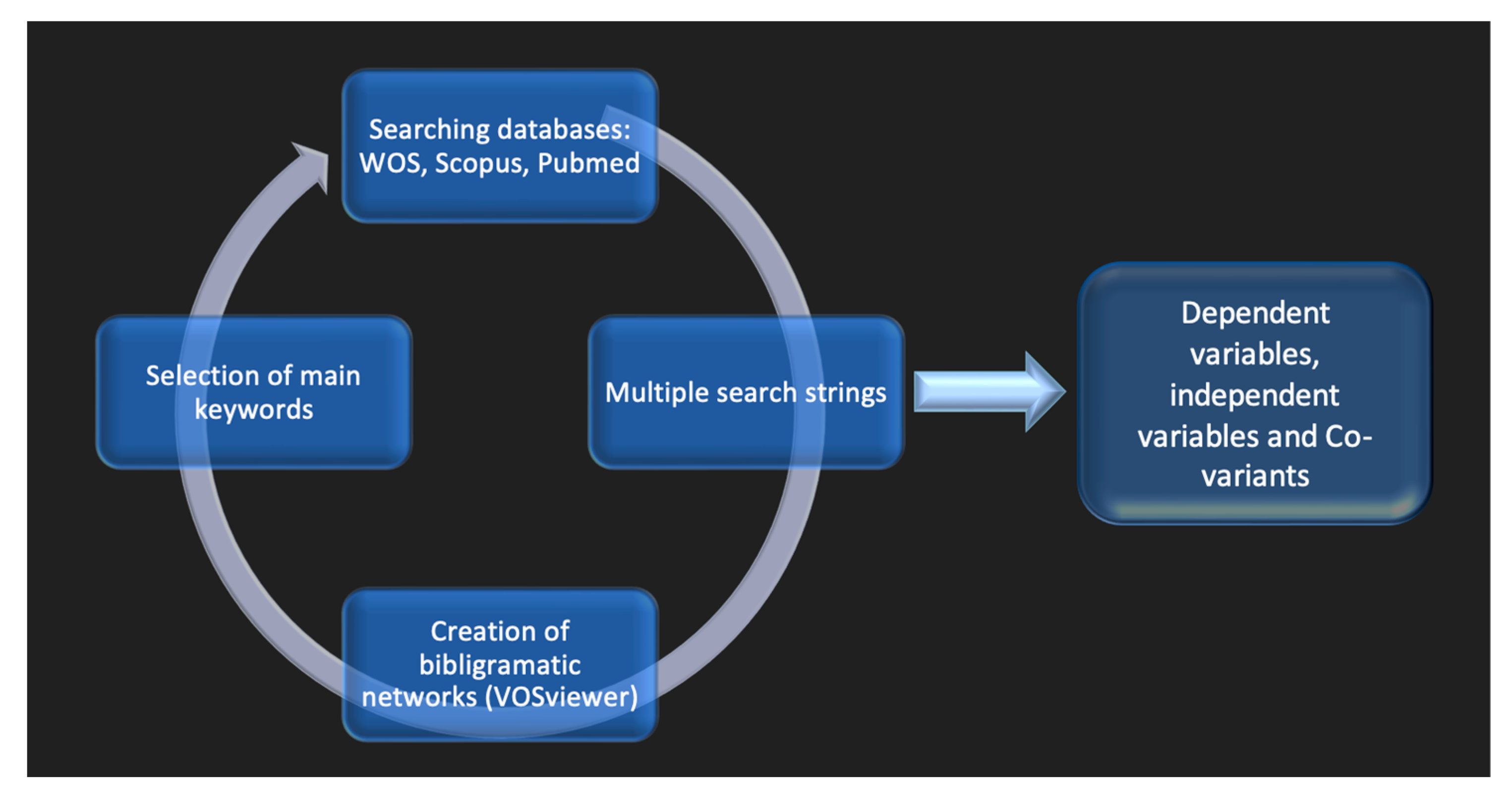
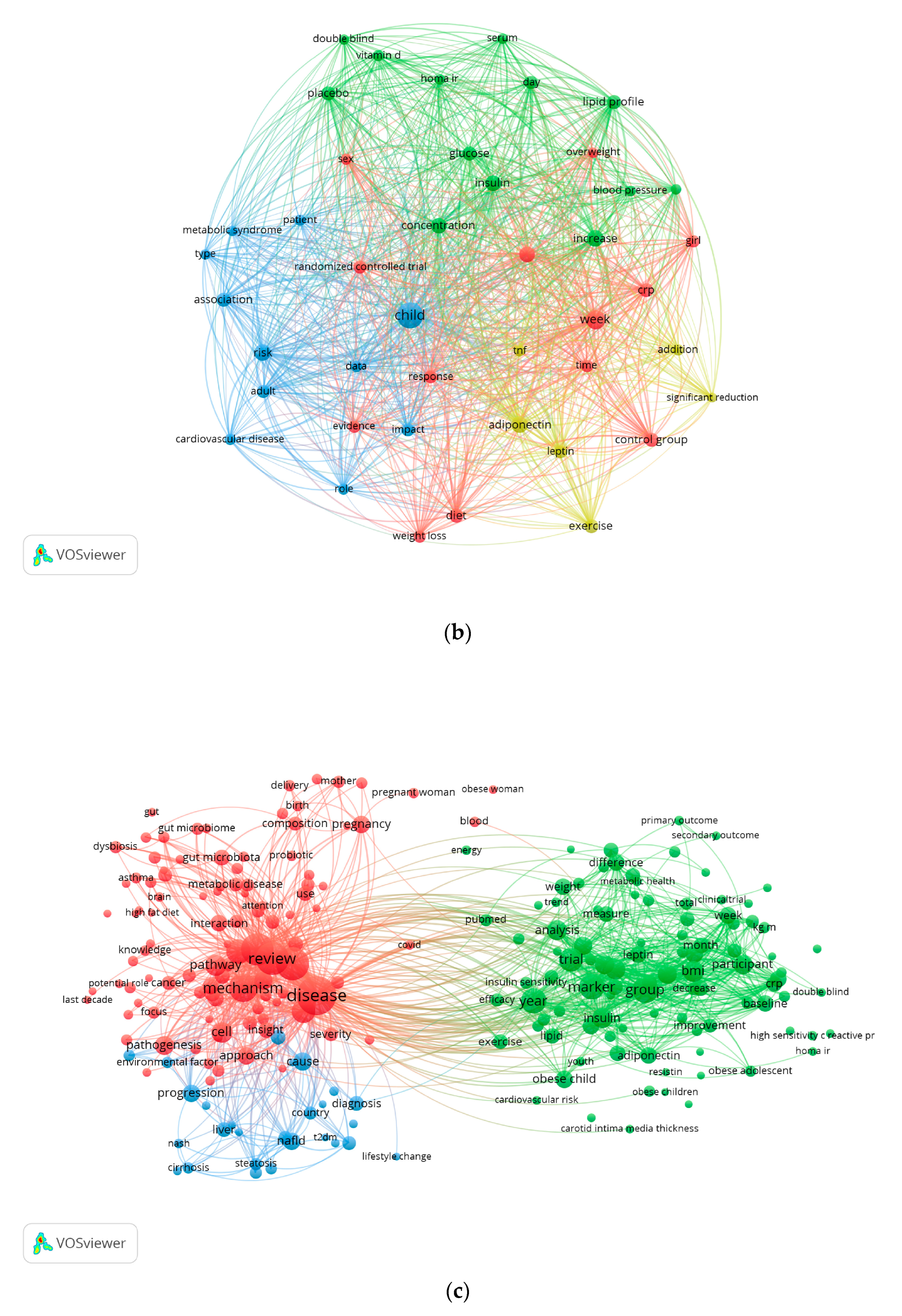
In this direction, a comprehensive review of the available scientific literature yielded over-abundant information, given that obesity-related literature is growing exponentially and numbers almost half a million articles to date. Special attention was therefore given to the filtering and careful selection of the available sources to allow for frequentist inference in childhood and adolescent obesity health effects. Although massively accumulated data might help search for statistical regularities in science, uncertainties, noise, and heterogenous (i.e., non-standardized) information might bias interpretation. Consequently, there is a need for an optimized mining pipeline to be deployed to search literature databases, as fragmented information is difficult to retrieve and combine towards a set hypothesis. In this study, we used a variety of in silico tools for creating bibliogram association networks [
23] to navigate as safely as possible the available literature, using a combination of keywords and buzzwords that are essential to optimally access these large databases. We opted for establishing a keyword-oriented network revolving mainly around mesh terms (the NLM gold standard for indexing scientific articles). Keywords can be extracted from either the title or the abstract of any indexed publication, or they can be taken from the author-supplied list of keywords accompanying and following a certain publication. Bibliogram networks are used exactly because the earlier literature search mode that tended to focus on individual keywords is currently developing to include lexical units (i.e., sentences indicating a specific object).
In this study, a state-of-the-art combination of bibliometric software and tools and meta-analysis techniques was adopted, adapted, and used to collate published evidence and examine any potential correlation between children and/or adolescent obesity and specific markers/indicators before and upon intervention. The methodological hierarchy was positioned within the two views of medical science, with emphasis on the evaluation of existing data, especially from randomized trials, to “see whether there is “something” in it” [
24] (p. 0339). After decades of meta-analyzing meta-analyses as a statistical technique in medical research, its pros and cons are well understood [
25,
26,
27]. Several limitations have been already uncovered (e.g., replicability, sample size, statistical power effects, Type I and II errors, prior probabilities, and so on) and, potentially, are technically rectifiable [
28,
29,
30]. We then explored the potential of coupling networks of medical objects–concepts with error-free meta-analysis techniques to construct a landscape of empirical knowledge regarding the childhood obesity epidemy.
A systematic meta-analysis investigating the relationship between stress, inflammation, and childhood obesity/overweight holds substantial scientific significance for various reasons. Firstly, it can provide a comprehensive overview of the existing research, clarifying the extent and consistency of the relationship between stress, inflammation, and childhood obesity/overweight. By pooling data from numerous studies, a meta-analysis offers a more precise estimation of the overall effect size and the strength of the relationships between stress, inflammation, and childhood obesity with respect to other types of analysis. Individual studies may produce conflicting results due to variations in methodology, populations, and other factors. A meta-analysis can help reconcile these discrepancies and offer a more balanced assessment of the relationship. Also, a meta-analysis can identify potential moderators that influence the stress–inflammation–obesity relationship, such as age, gender, socioeconomic status, and geographic location. This can lead to a more nuanced understanding of the phenomenon. A well-designed meta-analysis might provide insights into the temporal relationship between stress, inflammation, and obesity/overweight, aiding in the discussion about potential causal pathways. If a strong relationship is found, it can inform the clinical practice by highlighting the importance of addressing stress and inflammation in childhood obesity prevention and management strategies. It can identify gaps in the literature, areas of inconsistency, and areas with limited research. This information can guide future research efforts by highlighting the areas needing additional studies. If the relationship between stress, inflammation, and childhood obesity/overweight is robust, the findings can have implications for public health policies and interventions targeting childhood obesity and its underlying mechanisms. Finally, this information can advance the scientific knowledge by offering a synthesized perspective on a complex and evolving field, potentially leading to new hypotheses and research directions [
31,
32,
33,
34,
35].
In summary, a systematic meta-analysis on the relationship between stress, inflammation, and childhood/adolescence obesity/overweight has the potential to provide comprehensive insights, refine our understanding, and guide future research. It offers a valuable synthesis of evidence that can inform clinical practice, interventions, and policy decisions related to childhood obesity and its underlying factors.
4. Discussion
Herein, an effort was made to shed light on the impact that diet/exercise interventions can achieve on markers related to inflammation and dysmetabolism in children living with obesity or overweight. Our findings indicate that any intervention aiming to reduce excess body fat (diet, exercise, supplements/drugs) in children and adolescents living with obesity or overweight can lead to significant changes in a variety of markers, mainly by re-establishing homeostasis even if the change is subtle.
In a similar meta-analysis, Sirico F. et al., 2018 [
54], studied the effects of physical exercise on adiponectin, leptin, and inflammatory markers (IL-6, CRP, TNF-alpha) in children with obesity. The authors of the study reported significant changes in both adiponectin and leptin levels in favor of the intervention group. Also the IL-6 levels were significantly reduced. A trend towards a reduction was also observed in the CRP levels, although no effect on the TNF-alpha levels was reported, due to contradictory results. However, there are major differences between our study and this prior meta-analysis, mainly in the selection of the studies to be analyzed. Notably, our study had an open plan and did not focus only on randomized controlled trials; in addition, there is a difference in the nature of the scientific question, which, in our study, included every available intervention. Finally, herein we investigated not only inflammatory but also dysmetabolism markers.
Another meta-analysis by Schwingshackl L. et al., 2015 [
55], focused on the effect of a low glycemic load diet on several risk factors in children and adolescents living with obesity or overweight. The parameters considered were body weight, body mass index, z-score of the body mass index, fat mass, fat-free mass, height, waist circumference, hip circumference, waist-to-hip ratio, total cholesterol, LDL-cholesterol, HDL- cholesterol, triglycerides, diastolic and systolic blood pressure, fasting serum glucose, fasting serum insulin, HOMA-IR index, glycosylated hemoglobin, and C-reactive protein. Significant changes were observed in the triglyceride levels and HOMA-IR index in the low-glycemic diet group. This meta-analysis was also focused on randomized controlled trials. Unlike our own, the intervention included only diet changes and did not consider some of the markers we monitored in our study.
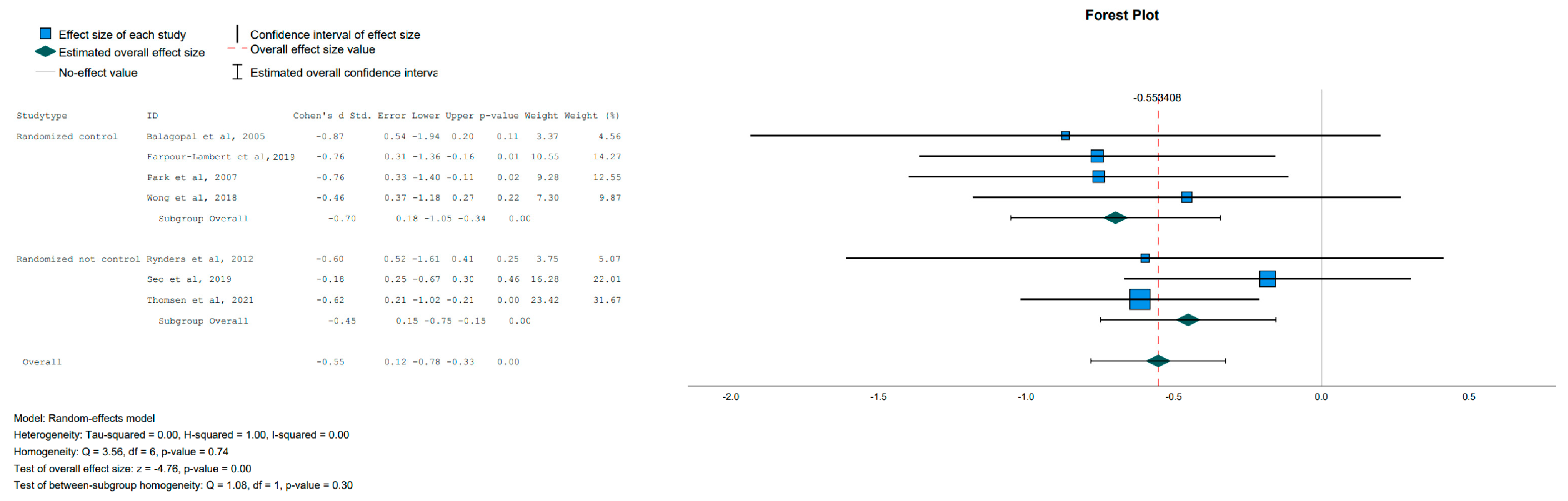
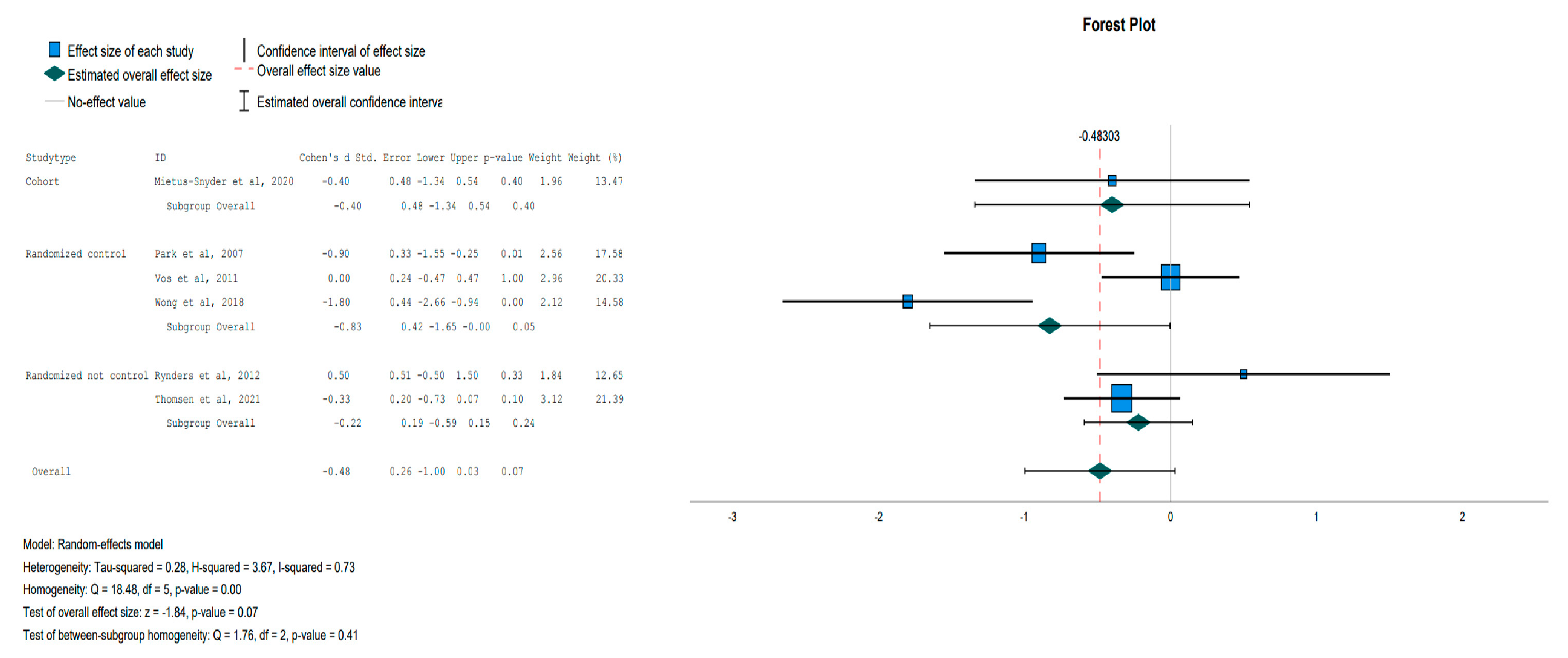
At this point, it is crucial to focus the attention on adiponectin’s and leptin’s roles as adipokines involved in several biochemical pathways and thus inevitably modulating metabolic processes and inflammatory responses. Adiponectin’s metabolic effects include a reduction in glucose production and an increase in insulin sensitivity and energy expenditure, while leptin signals energy sufficiency and also increases energy expenditure. Regarding inflammation, adiponectin has anti-inflammatory properties, as it promotes the reduction of TNF-alpha production in macrophages, and leptin has proinflammatory properties, as high levels of leptin activate monocytes and macrophages to produce IL-6 and TNF-alpha. [
56,
57]. In children with obesity or overweight, the adiponectin levels are significantly lower compared to those in normal-weight children, while the leptin levels are increased [
58]. The importance of our findings regarding adiponectin and leptin (a trend towards a reduction, driven by the randomized controlled trials subgroup), lies in the fact that their levels changed preferentially in the intervention group after any type of intervention, even if the BMI was not significantly altered (however, there was a significant change in body fat).
Another significant finding was that reduced insulin levels were observed after intervention, and the trend towards a reduction in both HOMA-IR and glucose levels was driven by randomized controlled trials. It is common among individuals living with obesity or overweight for insulin levels to be elevated, and this is also associated with insulin resistance. Insulin resistance (IR) is a pathological condition supporting several dysmetabolic conditions including obesity and type 2 diabetes (T2D), dyslipidemia, atherosclerosis, polycystic ovarian syndrome (PCOS), and non-alcoholic fatty liver disease (NAFLD). In children and adolescents with obesity, of any age, a strong association between IR and a higher prevalence of the components of the metabolic syndrome (MS) was observed; therefore a higher cardiovascular risk is predicted in these subjects [
59].
Finally, the significant reduction in systolic blood pressure that we observed needs to be mentioned, as an elevated blood pressure is firmly reported in children and adolescents living with obesity or overweight and contributes to the occurrence and severity of hypertension along with an increase in cardiovascular risk. The duration of hypertension affects the risk of end-organ damage; so, it is of uttermost importance to restrain and control the blood pressure at a young age. Considering that the global prevalence of childhood hypertension is rising along with the prevalence of overweight and obesity [
60], every measure taken against blood pressure elevation is important.
The results of the current meta-analysis should be considered with caution, as some limitations can be identified. Firstly, only a few studies focused on the several outcome parameters chosen for the data synthesis were available. This fact could potentially explain the lack of statistical significance for the differences observed in various outcome parameters between the intervention and the control group and the occurrence of tendencies towards an improvement in the groups. Secondly, all the included studies had a small sample size (about 100 or less). Another limitation concerns the duration and intensity of the interventions, as the several protocols used followed neither the same time frame for the completion of the study nor the same exercise duration. For example, more significant differences could have been observed between the control and the intervention groups with a longer study duration or exercise time. Nevertheless, it was important to include studies with different durations to increase the sample size and improve the statistical viability and the credibility of our scientific arguments. Generally, the duration of the interventions in childhood/adolescence obesity/overweight studies is crucial for understanding their short- and long-term impacts on various physiological, behavioral, and developmental aspects. It influences the ability to detect sustained effects, assess developmental interactions, study metabolic changes, observe behavioral adaptations, and determine the overall efficacy and feasibility of the interventions. Even though these limitations are common in interventional studies including exercise protocols, they affect the validity of the results.
Another concern arising from the study of leptin and adiponectin in overweight/obesity in children/adolescents regards the different expression of these adipokines according to sex and age; in fact, hormonal differences between boys and girls and between prepubertal and postpubertal individuals of both sexes are major determinants of the levels of plasma adipokines [
58]. The studies included in our meta-analysis were not specifically designed nor performed any special calculation of the results considering the mentioned issues.
5. Conclusions
All in all, the current meta-analysis provides evidence of the beneficial effect of a lifestyle intervention (diet, exercise, supplements/drugs) in children and adolescents with obesity or overweight. With a significant reduction in Body Fat (although not in BMI or Waist Circumference), an increase in the adiponectin levels, a reduction in the circulating insulin levels and in diastolic blood pressure, and a trend towards a reduction of circulating leptin and glucose levels and HOMA-IR, our findings corroborate the hypothesis that lifestyle interventions could reduce overweight-/obesity-associated systemic inflammation and dysmetabolism. Considering the discussed limitations of this analysis, further studies are necessary to confirm our findings.
As overweight and obesity among children and adolescents have become a major pandemic, it is very important to sensitize not only individuals but also public health stakeholders. As obesity and overweight at a young age most commonly persist in adults, causing several health complications, it is extremely important to address this problem as early as possible.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










