
Acute Foot Drop Caused by Intraneural Ganglion Cyst of the Peroneal Nerve: Literature Review and Case Report
 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Protocol
2.2. Search Strategy, Eligibility Criteria and Data Extraction
3. Results
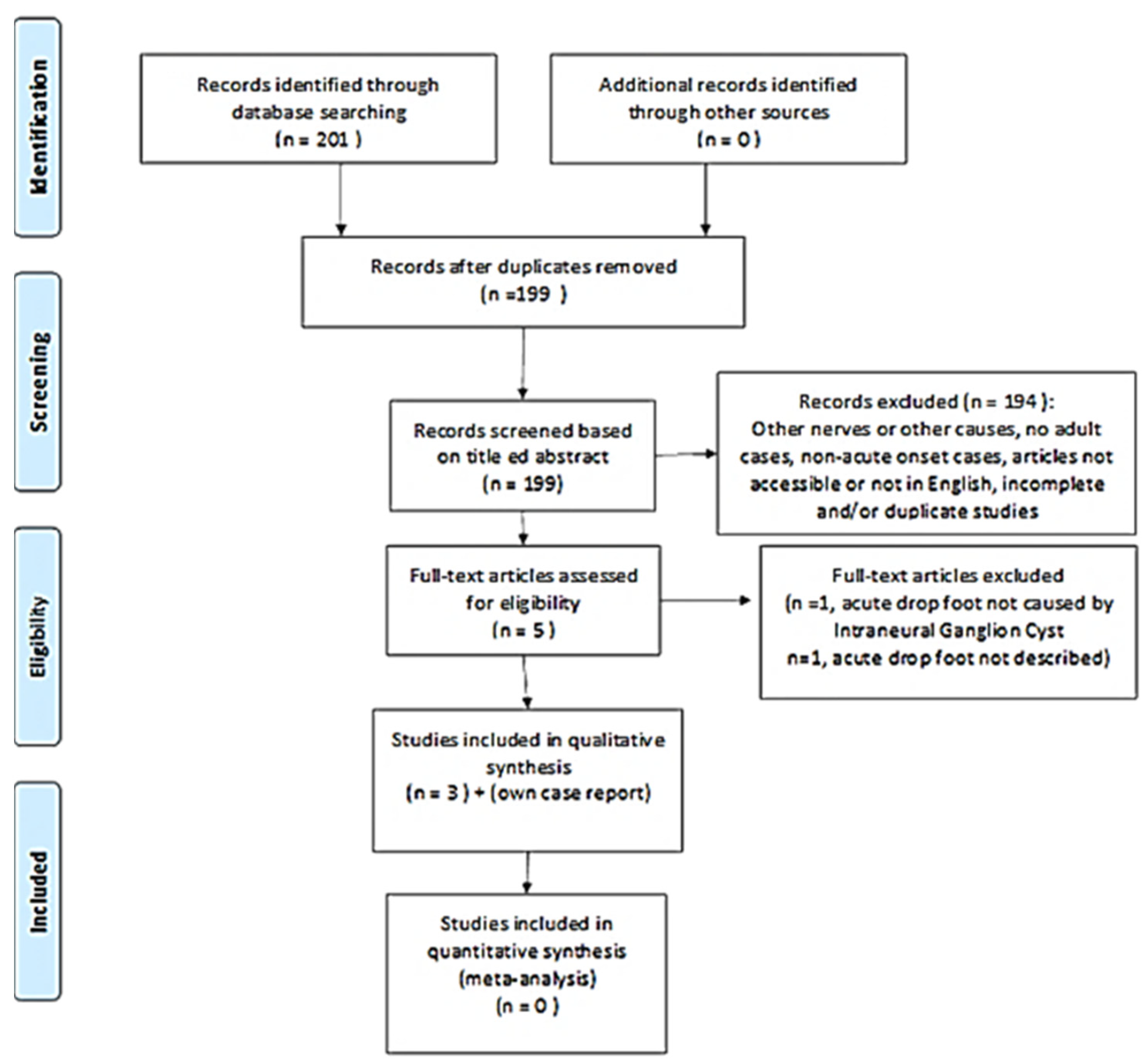
3.1. Study Selection
3.2. Case Report
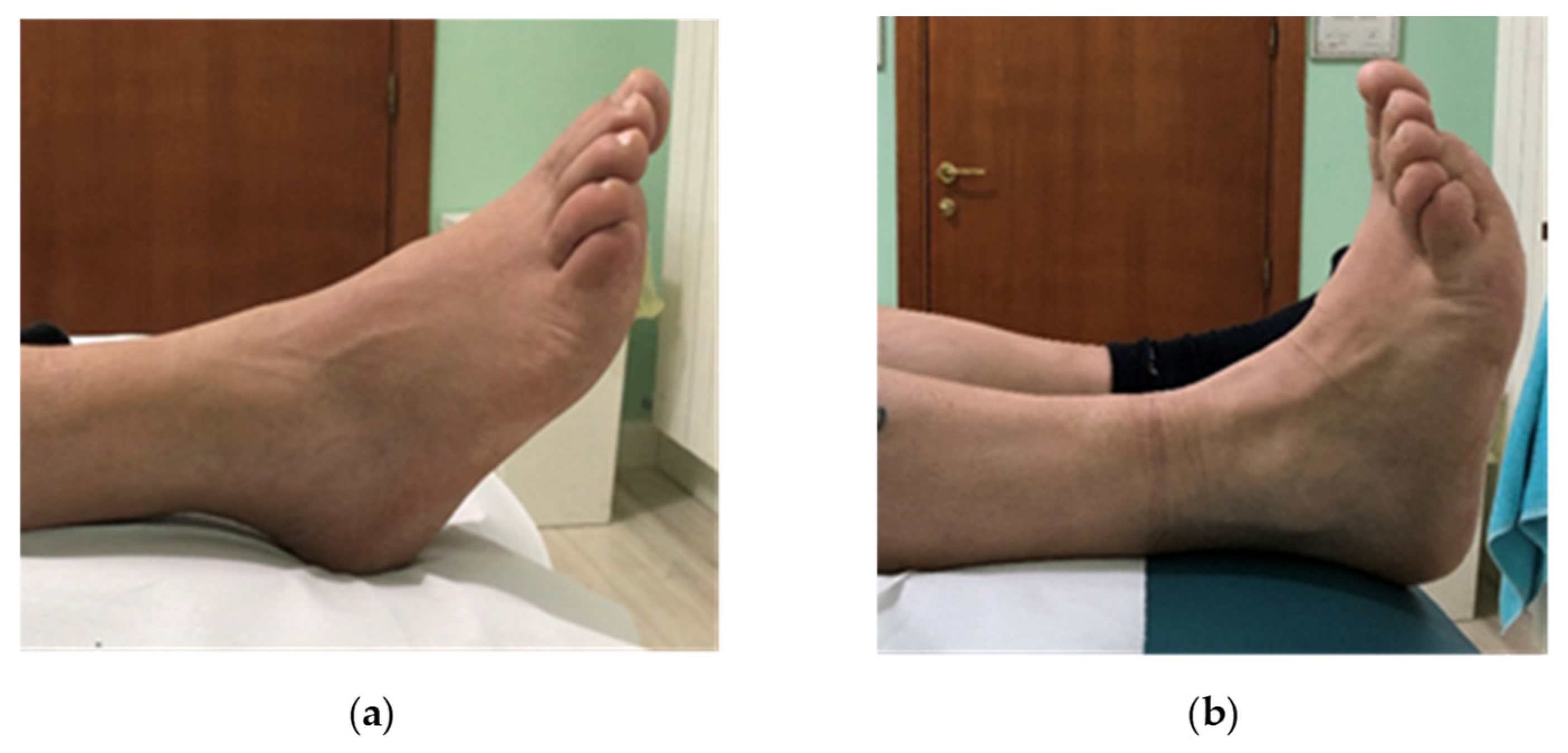
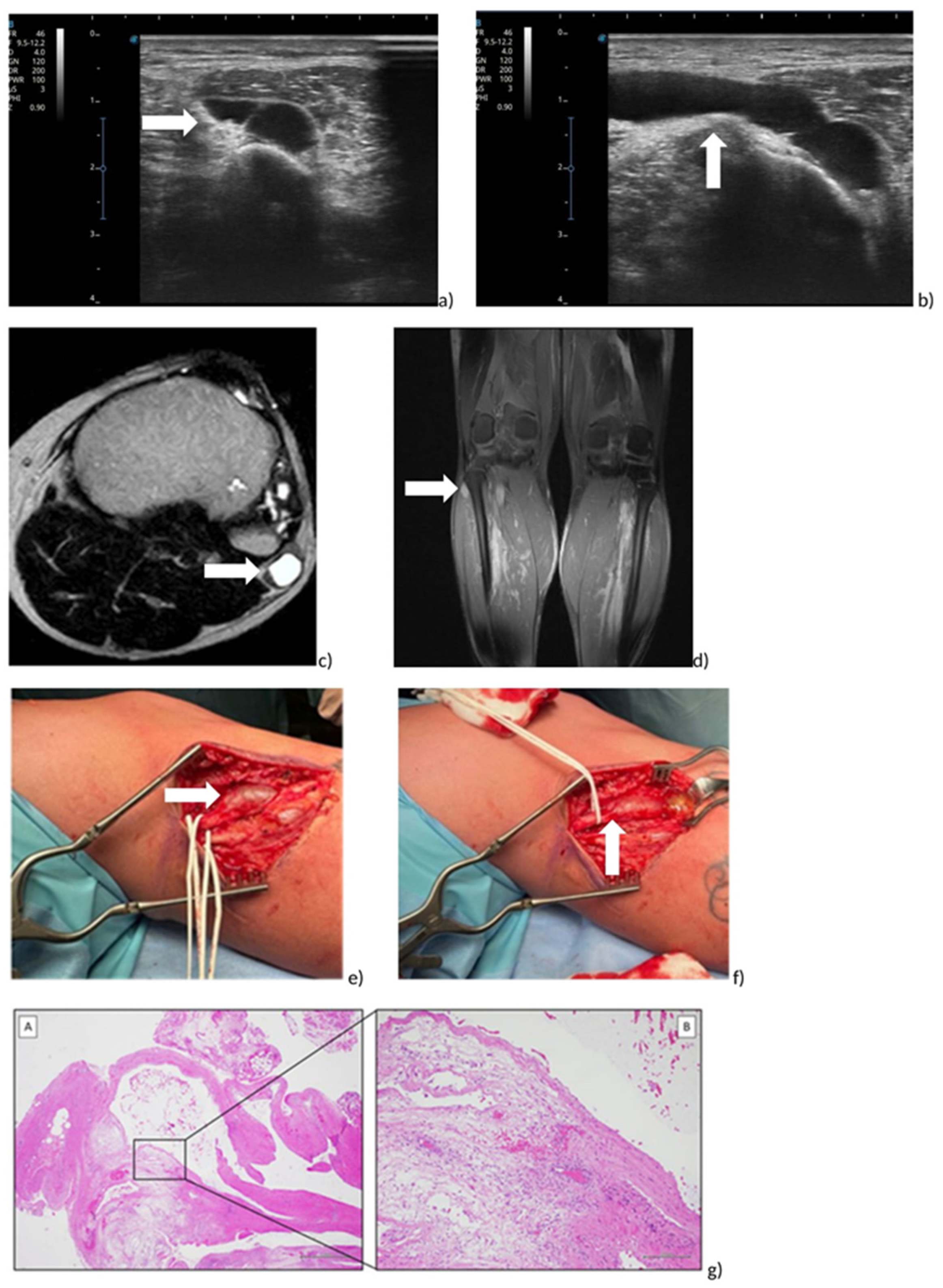
3.2.1. Evaluation
3.2.2. Treatment
3.2.3. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carolus, A.E.; Becker, M.; Cuny, J.; Smektala, R.; Schmieder, K.; Brenke, C. The Interdisciplinary Management of Foot Drop. Dtsch. Arztebl. Int. 2019, 116, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Vlahovic, T.; Ribeiro, C.; Lamm, B.; Denmark, J.; Walters, R.; Talbert, T.; Penugonda, S.; Furmato, J.; Brower, D.; McMahon, J.; et al. A case of peroneal neuropathy-induced footdrop. Correlated and compensatory lower-extremity function. J. Am. Podiatr. Med. Assoc. 2000, 90, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.D. Foot drop: Where, why and what to do? Pract Neurol. 2008, 8, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Alnajjar, F.; Zaier, R.; Khalid, S.; Gochoo, M. Trends and Technologies in Rehabilitation of Foot Drop: A Systematic Review. Expert. Rev. Med. Devices 2021, 18, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Kokkalis, Z.T.; Stavropoulos, N.A.; Mavrogenis, A.F.; Panagopoulos, A.; Soucacos, P.N. Benign peripheral nerve tumors. Injury 2019, 50 (Suppl. 5), S77–S83. [Google Scholar] [CrossRef]
- Kokkalis, Z.T.; Kalavrytinos, D.; Kokkineli, S.; Kouzelis, A.; Sioutis, S.; Mavrogenis, A.F.; Panagopoulos, A. Intraneural ganglion cysts of the peroneal nerve. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1639–1645. [Google Scholar] [CrossRef]
- Spinner, R.J.; Mikami, Y.; Desy, N.M.; Amrami, K.K.; Berger, R.A. Superfcial radial intraneural ganglion cysts at the wrist. Acta Neurochir. 2018, 160, 2479–2484. [Google Scholar] [CrossRef]
- Cush, G.; Irgit, K. Drop foot after knee dislocation: Evaluation and treatment. Sports Med. Arthrosc. Rev. 2011, 19, 139–146. [Google Scholar] [CrossRef]
- Brief, J.M.; Brief, R.; Ergas, E.; Brief, L.P.; A Brief, A. Peroneal nerve injury with foot drop complicating ankle sprain—A series of four cases with review of the literature. Bull. NYU Hosp. Jt. Dis. 2009, 67, 374–377. [Google Scholar]
- Stamiris, S.; Stamiris, D.; Sarridimitriou, A.; Anestiadou, E.; Karampalis, C.; Vrangalas, V. Acute Complete Foot Drop Caused by Intraneural Ganglion Cyst without a Prior Traumatic Event. Case Rep. Orthop. 2020, 2020, 1904595. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.K.; von Schoen-Angerer, T.; Tugwell, P.; Kiene, H.; Helfand, M.; Altman, D.G.; Sox, H.; et al. CARE guidelines for case reports: Explanation and elaboration document. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.I.; Nottmeier, E.; Blasser, K.E.; Peterson, J.J.; Kennelly, K. Acute onset of deep peroneal neuropathy during a golf game resulting from a ganglion cyst. J. Clin. Neuromuscul. Dis. 2004, 6, 49–53. [Google Scholar] [CrossRef]
- Williams, S.L.; Clancy, J.T.; Williamson, D.S. Acute-Onset Footdrop Caused by Intraneural Ganglion Cyst of the Common Peroneal Nerve: The Effects of Extraneural Pressure Gradients on Cyst Propagation. J. Am. Podiatr. Med. Assoc. 2022, 112, 20–252. [Google Scholar] [CrossRef]
- Khan, A.A.; Rodriguez-Collazo, E.R.; Lo, E.; Raja, A.; Yu, S.; Khan, H.A. Evaluation and Treatment of Foot Drop Using Nerve Transfer Techniques. Clin. Podiatr. Med. Surg. 2021, 38, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Schucany, W.G. A rare case of intraneural ganglion cyst involving the tibial nerve. Proc. Bayl. Univ. Med. Cent. 2012, 25, 132–135. [Google Scholar] [CrossRef]
- Gurdjian, E.S.; Larsen, R.D.; Lindner, D.W. Intraneural cyst of the peroneal and ulnar nerves. Report of two cases. J. Neurosurg. 1965, 23, 76–78. [Google Scholar] [CrossRef] [Green Version]
- Scherman, B.M.; Bilbao, J.M.; Hudson, A.R.; Briggs, S.J. Intraneural ganglion: A case report with electron microscopic observations. Neurosurgery 1981, 8, 487–490. [Google Scholar] [CrossRef]
- Spinner, R.J.; Atkinson, J.L.D.; Tiel, R.L.; Daniels, S.P.; Feinberg, J.H.; Carrino, J.A.; Behzadi, A.H.; Sneag, D.B.; Nwawka, O.K.; Lee, S.; et al. Peroneal intraneural ganglia: The importance of the articular branch. A unifying theory. J. Neurosurg. 2003, 99, 330–343. [Google Scholar] [CrossRef] [Green Version]
- Weyns, F.; Bringmans, T.; Vandevenne, J.; Daenekindt, T.; Van Goethem, A.; Wuyts, J.; Vanormelingen, L.; Vandersteen, M. Peripheral neuropathy caused by joint-related cysts: A review of 17 cases. Acta Neurochir. 2012, 154, 1741–1753. [Google Scholar] [CrossRef]
- Akcakaya, M.O.; Shapira, Y.; Rochkind, S. Peroneal and tibial intraneural ganglion cysts in children. Pediatr. Neurosurg. 2013, 49, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.A.; Lyne, D.E. Intraneural ganglion cyst of the peroneal nerve in a four-year-old girl: A case report. J. Pediatr. Orthop. 2007, 27, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Leijten, F.S.S.; Arts, W.-F.; Puylaert, J.B.C.M. Ultrasound diagnosis of an intraneural ganglion cyst of the peroneal nerve. J. Neurosurg. 1992, 76, 538–540. [Google Scholar] [CrossRef] [PubMed]
- Panwar, J.; Mathew, A.; Thomas, B.P. Cystic lesions of peripheral nerves: Are we missing the diagnosis of the intraneural ganglion cyst? World J. Radiol. 2017, 9, 230–244. [Google Scholar] [CrossRef] [PubMed]
- Spinner, R.J.; Desy, N.M.; Amrami, K.K. The Cystic Transverse Limb of the Articular Branch: A Pathognomonic Sign for Peroneal Intraneural Ganglia at the Superior Tibiofibular Joint. Neurosurgery 2006, 59, 157–166. [Google Scholar] [CrossRef]
- Consales, A.; Pacetti, M.; Imperato, A.; Valle, M.; Cama, A. Intraneural Ganglia of the Common Peroneal Nerve in Children: Case Report and Review of the Literature. World Neurosurg. 2016, 86, e11–e17. [Google Scholar] [CrossRef]
- Waldschmidt, U.; Slongo, T. An unusual cause of paralysis of the peroneal nerve-a case report. J. Pediatr. Surg. 2010, 45, 259–261. [Google Scholar] [CrossRef]
- Broekx, S.; Van Der Straeten, R.; D’haen, B.; Vandevenne, J.; Ernon, L.; Weyns, F. Intraneural ganglion cyst of the common peroneal nerve causing foot drop in a 12-year old child. Clin. Neurol. Neurosurg. 2021, 209, 106915. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Study Design, Participant | Pathological Anatomy | Diagnostic Exams | Outcome Measures | Treatment | Follow Up Results |
|---|---|---|---|---|---|---|
| Devon I. Rubin (2004) [13] | Short report, III, 1 participant, age 67, man. | ganglion cyst | MRI, EMG, blood test | complete paralysis of dorsiflexor ankle muscles | surgery | Three months. Ankle dorsiflexion MRC = 3/5, Toe extension MRC = 2/5. |
| Samantha L. Williams (2022) [14] | Case report, III, 1 participant, age 52, man | not available | MRI, EMG, blood test | Unspecified rating scale. Complete dorsiflexors paralysis of the foot and toes reported | surgery, physiotherapy (with physical therapy and electrostimulation) | One year. Reported complete recovery of strength of the dorsiflexors muscles |
| Stavros Stamiris (2020) [10] | Case report, III, 1 participant, age 42, man | ganglion cyst | X-ray, EMG, MRI, blood test | TA MRC = 1/5, EHL MRC = 0/5, EDC MRC = 0/5, PM MRC = 2/5. | surgery, physiotherapy | three months. TA MRC = 4/5, EHL MRC = 2/5, EDC MRC = 3/5, PM MRC = 4/5. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
della Vecchia, G.; Baldi, A.; Passavanti, M.B.; Lucariello, A.; De Luca, A.; De Blasiis, P. Acute Foot Drop Caused by Intraneural Ganglion Cyst of the Peroneal Nerve: Literature Review and Case Report. J. Pers. Med. 2023, 13, 1137. https://doi.org/10.3390/jpm13071137
della Vecchia G, Baldi A, Passavanti MB, Lucariello A, De Luca A, De Blasiis P. Acute Foot Drop Caused by Intraneural Ganglion Cyst of the Peroneal Nerve: Literature Review and Case Report. Journal of Personalized Medicine. 2023; 13(7):1137. https://doi.org/10.3390/jpm13071137
Chicago/Turabian Styledella Vecchia, Giuseppe, Alfonso Baldi, Maria Beatrice Passavanti, Angela Lucariello, Antonio De Luca, and Paolo De Blasiis. 2023. "Acute Foot Drop Caused by Intraneural Ganglion Cyst of the Peroneal Nerve: Literature Review and Case Report" Journal of Personalized Medicine 13, no. 7: 1137. https://doi.org/10.3390/jpm13071137