

Evaluation of the Safety of Percutaneous Sensory Nerve Stimulation in Patients with Head and Neck Cancer Receiving Chemoradiotherapy
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Objectives and Eligibility Criteria
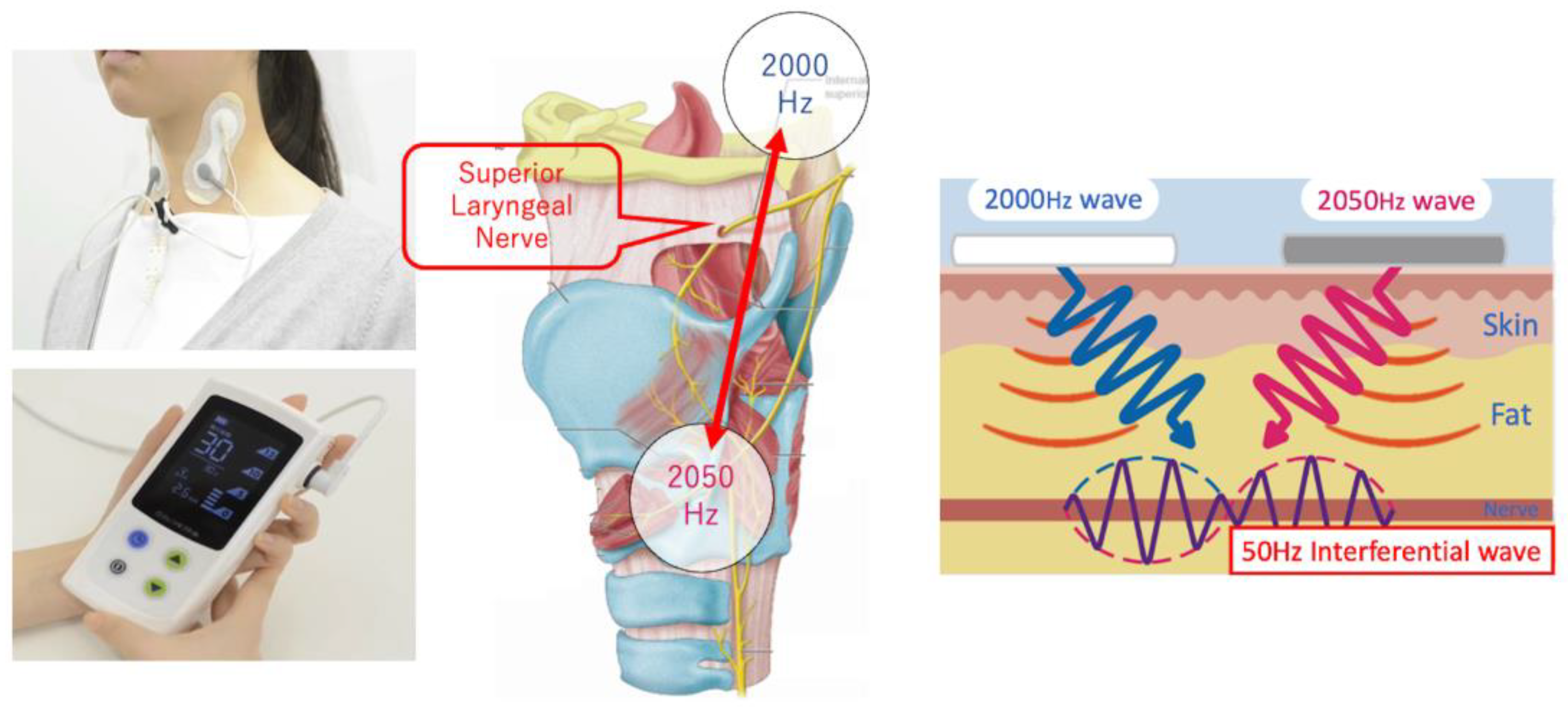
2.3. Medical Device Used
2.4. Interventions
2.5. Definition of “Feasible”
2.6. Outcome Measures
2.7. Primary Endpoint and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCCN Clinical Practice Guidelines in Oncology, Head and Neck Cancers. 2023. Available online: https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManagerGuid?FileManagerGuidId=c0d39f8d-46a2-4662-b373-467ca4cacd96 (accessed on 18 May 2023).
- Yang, W.; Nie, W.; Zhou, X.; Guo, W.; Mou, J.; Yong, J.; Wu, T.; Liu, X. Review of prophylactic swallowing interventions for head and neck cancer. Int. J. Nurs. Stud. 2021, 123, 104074. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Takemura, M.; Tsujita, J.; Oku, Y. Interferential electric stimulation applied to the neck increases swallowing fre-quency. Dysphagia 2012, 27, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Oku, Y.; Sugishita, S.; Imai, T.; Matsui, T.; Daimon, T.; Nozaki, S.; Yoshikawa, H. Effects of short term interferential current stimulation on swallowing reflex in dysphagic patients. Int. J. Speech Lang. Pathol. Audiol. 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Gallas, S.; Marie, J.P.; Leroi, A.M.; Verin, E. Sensory transcutaneous electrical stimulation improves post-stroke dysphagic pa-tients. Dysphagia 2010, 25, 291–297. [Google Scholar] [CrossRef]
- Hernigou, P.; Homma, Y.; Flouzat-Lachaniette, C.H.; Poignard, A.; Chevallier, N.; Rouard, H. Cancer risk is not increased in pa-tients treated for orthopaedic diseases with autologous bone marrow cell concentrate. J. Bone Jt. Surg. Am. 2013, 95, 2215–2221. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J.; MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer: An update on 93 randomised trials and 17346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Wall, L.R.; Ward, E.C.; Cartmill, B.; Hill, A.J. Physiological changes to the swallowing mechanism following (chemo)radiotherapy for head and neck cancer: A systematic review. Dysphagia 2013, 28, 481–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pointreau, Y.; Garaud, P.; Chapet, S.; Sire, C.; Tuchais, C.; Tortochaux, J.; Faivre, S.; Guerrif, S.; Alfonsi, M.; Calais, G. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J. Natl. Cancer Inst. 2009, 101, 498–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janoray, G.; Pointreau, Y.; Garaud, P.; Chapet, S.; Alfonsi, M.; Sire, C.; Jadaud, E.; Calais, G. Long-term results of a multicenter randomized phase 3 trial of induction chemotherapy with cisplatin, 5-fluorouracil ± docetaxel for larynx preservation. J. Natl. Cancer Inst. 2015, 108, djv368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ou, D.; Blanchard, P.; El Khoury, C.; De Felice, F.; Even, C.; Levy, A.; Nguyen, F.; Janot, F.; Gorphe, P.; Deutsch, E.; et al. Induction chemotherapy with docetaxel, cisplatin and fluorouracil followed by concurrent chemoradiotherapy or che-modaiotherapy alone in locally advanced non-endemic nasopharyngeal carcinoma. Oral Oncol. 2016, 62, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Posner, M.; Hitt, R.; Cohen, E.E.W.; Schulten, J.; Lefebvre, J.L.; Vermorken, J.B. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck: Role, controversy, and future directions. Ann. Oncol. 2018, 29, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.B.; Wu, X.P. A randomized controlled trail of combination therapy of neuromuscular electrical stimulation and bal-loon dilatation in the treatment of radiation-induced dysphagia in nasopharyngeal carcinoma patients. Disabil. Rehabil. 2013, 35, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.H.; Hsiao, T.Y.; Chang, Y.C.; Ting, L.L.; Chen, W.S.; Chen, S.C.; Wang, T.G. Effects of functional electrical stimulation on dysphagia caused by radiation therapy in patients with nasopharyngeal carcinoma. Support Care Cancer 2011, 19, 91–99. [Google Scholar] [CrossRef]
- Kotz, T.; Federman, A.D.; Kao, J.; Milman, L.; Packer, S.; Lopez-Prieto, C.; Forsythe, K.; Genden, E.M. Prophylactic swallowing exercises in patients with head and neck cancer undergoing chemoradiation: A randomized trial. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Carnaby-Mann, G.; Crary, M.A.; Schmalfuss, I.; Amdur, R. “Pharyngocise”: Randomized controlled trial of preventative exer-cises to maintain muscle structure and swallowing function during head-and-neck chemoradiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Shen, Q.; Wang, Y.; Lu, K.; Wang, Y.; Peng, Y. A randomized prospective study of rehabilitation therapy in the treat-ment of radiation-induced dysphagia and trismus. Strahlenther Onkol. 2011, 187, 39–44. [Google Scholar] [CrossRef]
- Kulbersh, B.D.; Rosenthal, E.L.; McGrew, B.M.; Duncan, R.D.; McColloch, N.L.; Carroll, W.R.; Magnuson, J.S. Pretreatment, preoperative swallowing exercises may improve dysphagia quality of life. Laryngoscope 2006, 116, 883–886. [Google Scholar] [CrossRef]
- Iizumi, Y.; Ihara, Y.; Koike, J.; Takahashi, K. Effects of interferential current electrical stimulation (IFCS) on mastication and swal-lowing function in healthy young adults: A preliminary study. Clin. Exp. Dent. Res. 2023, 9, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Sakashita, T.; Homma, A.; Hatakeyama, H.; Furusawa, J.; Kano, S.; Mizumachi, T.; Iizuka, S.; Onimaru, R.; Tsuchiya, K.; Ya-suda, K.; et al. Comparison of acute toxicities associated with cetuximab-based bioradiotherapy and plati-num-based chemoradiotherapy for head and neck squamous cell carcinomas: A single-institution retrospective study in Ja-pan. Acta Otolaryngol. 2015, 135, 853–858. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| No. | Age/Sex | Primary Site | TNM/Stage | Treatment | Chemo Agent/Cycles |
|---|---|---|---|---|---|
| 1 | 70/Male | Hypopharynx | T1N2bM0/stage IVA | CRT after IC 2 cycles | Cisplatin/3 cycles |
| 2 | 59/Male | Nasopharynx | T1N1M0/stage II | CRT after IC 2 cycles | Cisplatin/2 cycles |
| 3 | 73/Male | Primary unknown | T0N3bM0/stage IVB | CRT | Cisplatin/3 cycles |
| 4 | 76/Male | Hypopharynx | T4aN2bM0/stage IVA | BRT | Cetuximab/7 cycles |
| 5 | 72/Male | Hypopharynx | T2N3bM0/stage IVB | CRT after IC 2 cycles | Cisplatin/3 cycles |
| 6 | 64/Male | Hypopharynx | T4aN2cM0/stage IVA | CRT after IC 2 cycles | Cisplatin/2 cycles |
| 7 | 45/Male | Hypopharynx | T4bN3bM0/stage IVB | CRT after IC 2 cycles | Cisplatin/2 cycles |
| 8 | 74/Male | Hypopharynx | T4aN3bM0/stage IVB | CRT after IC 2 cycles | Cisplatin/2 cycles |
| 9 | 51/Male | Larynx | T2N0M0/stage II | CRT | Cisplatin/3 cycles |
| 10 | 64/Male | Hypopharynx | T1N2bM0/stage IVA | CRT | Cisplatin/3 cycles |
| No. | Days of SR | Days of IFCD | Output Power | Procedure Time | IP/TID |
|---|---|---|---|---|---|
| 1 | 5-5-5-4-5-5-4 | 4-5-5-5-5-5-4 | 13-13-12-12-12-12-13 | 29-30-30-30-30-30-30 | 68 Gy/70 Gy |
| 2 | 5-5-5-5-5-5-2 | 4-5-5-5-5-5-2 | 9-5-6-6-11-6-7 | 30-30-30-30-30-30-30 | 64 Gy/70 Gy |
| 3 | 5-5-5-5-5-5-5 | 5-5-5-5-5-5-5 | 8-7-5-7-7-10-13 | 30-30-30-30-30-30-30 | 66 Gy/66 Gy |
| 4 | 4-5-5-5-5-5-5 | 4-5-5-5-5-5-1 | 3-7-7-3-4-1-1 | 30-30-30-30-30-30-30 | 62 Gy/70 Gy |
| 5 | 4-5-5-5-5-5-5 | 4-5-5-5-5-5-5 | 9-6-9-8-8-9-8 | 30-30-30-30-30-30-30 | 70 Gy/70 Gy |
| 6 | 5-5-4-5-4-5-3 | 5-5-4-5-4-5-3 | 13-13-15-12-10-10-10 | 30-30-30-30-30-30-30 | 66 Gy/70 Gy |
| 7 | 4-5-5-5-4-5-5 | 4-5-5-5-5-5-5 | 5-4-4-7-3-2-3 | 30-30-30-30-30-30-30 | 70 Gy/70 Gy |
| 8 | 4-5-5-5-5-5-5 | 4-5-5-5-5-5-5 | 5-3-2-2-2-1-1 | 30-30-30-30-30-30-30 | 70 Gy/70 Gy |
| 9 | 4-5-3-5-5-5-5 | 4-5-3-5-5-5-5 | 5-7-8-8-10-11-11 | 30-30-30-30-30-30-30 | 66 Gy/70 Gy |
| 10 | 4-5-3-4-5-5-5 | 4-5-3-4-5-5-5 | 6-7-8-6-8-8-7 | 30-30-30-30-30-30-30 | 68 Gy/70 Gy |
| p = 0.8493 | p = 0.8767 | p = 0.7926 | p = 0.1347 |
| Adverse Event | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 |
|---|---|---|---|---|---|
| Dermatitis | 3 | 4 | 3 | 0 | 0 |
| Mucositis | 4 | 4 | 2 | 0 | 0 |
| Dry mouth | 4 | 5 | 1 | 0 | 0 |
| Dysgeusia | 3 | 5 | 0 | 0 | 0 |
| Aspiration | 1 | 0 | 0 | 0 | 0 |
| Alopecia | 1 | 0 | 0 | 0 | 0 |
| No. | 10 Gy | 20 Gy | 30 Gy | 40 Gy | 50 Gy | 60 Gy | 70 Gy |
|---|---|---|---|---|---|---|---|
| 1 | F | F | F | F | F | F | F |
| 2 | F | F | F | F | F | F | NF |
| 3 | F | F | F | F | F | F | - * |
| 4 | F | F | F | F | F | F | NF |
| 5 | F | F | F | F | F | F | F |
| 6 | F | F | F | F | F | F | F |
| 7 | F | F | F | F | F | F | F |
| 8 | F | F | F | F | F | F | F |
| 9 | F | F | F | F | F | F | F |
| 10 | F | F | F | F | F | F | F |
| RF ** | 100% | 100% | 100% | 100% | 100% | 100% | 78% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamamoto, T.; Sato, Y.; Yumii, K.; Chikuie, N.; Taruya, T.; Horibe, Y.; Ishino, T.; Ueda, T.; Takeno, S.; Yoshimura, K. Evaluation of the Safety of Percutaneous Sensory Nerve Stimulation in Patients with Head and Neck Cancer Receiving Chemoradiotherapy. J. Pers. Med. 2023, 13, 1129. https://doi.org/10.3390/jpm13071129
Hamamoto T, Sato Y, Yumii K, Chikuie N, Taruya T, Horibe Y, Ishino T, Ueda T, Takeno S, Yoshimura K. Evaluation of the Safety of Percutaneous Sensory Nerve Stimulation in Patients with Head and Neck Cancer Receiving Chemoradiotherapy. Journal of Personalized Medicine. 2023; 13(7):1129. https://doi.org/10.3390/jpm13071129
Chicago/Turabian StyleHamamoto, Takao, Yuki Sato, Kohei Yumii, Nobuyuki Chikuie, Takayuki Taruya, Yuichiro Horibe, Takashi Ishino, Tsutomu Ueda, Sachio Takeno, and Kenichi Yoshimura. 2023. "Evaluation of the Safety of Percutaneous Sensory Nerve Stimulation in Patients with Head and Neck Cancer Receiving Chemoradiotherapy" Journal of Personalized Medicine 13, no. 7: 1129. https://doi.org/10.3390/jpm13071129