
Urgent Psychiatric Consultations for Suicidal Ideation and Behaviors in Italian Adolescents during Different COVID-19 Pandemic Phases
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Setting
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Child Psychiatry Consultations for Suicide Attempt and Suicidal Ideation from 2018 to 2022, Univariate Analysis
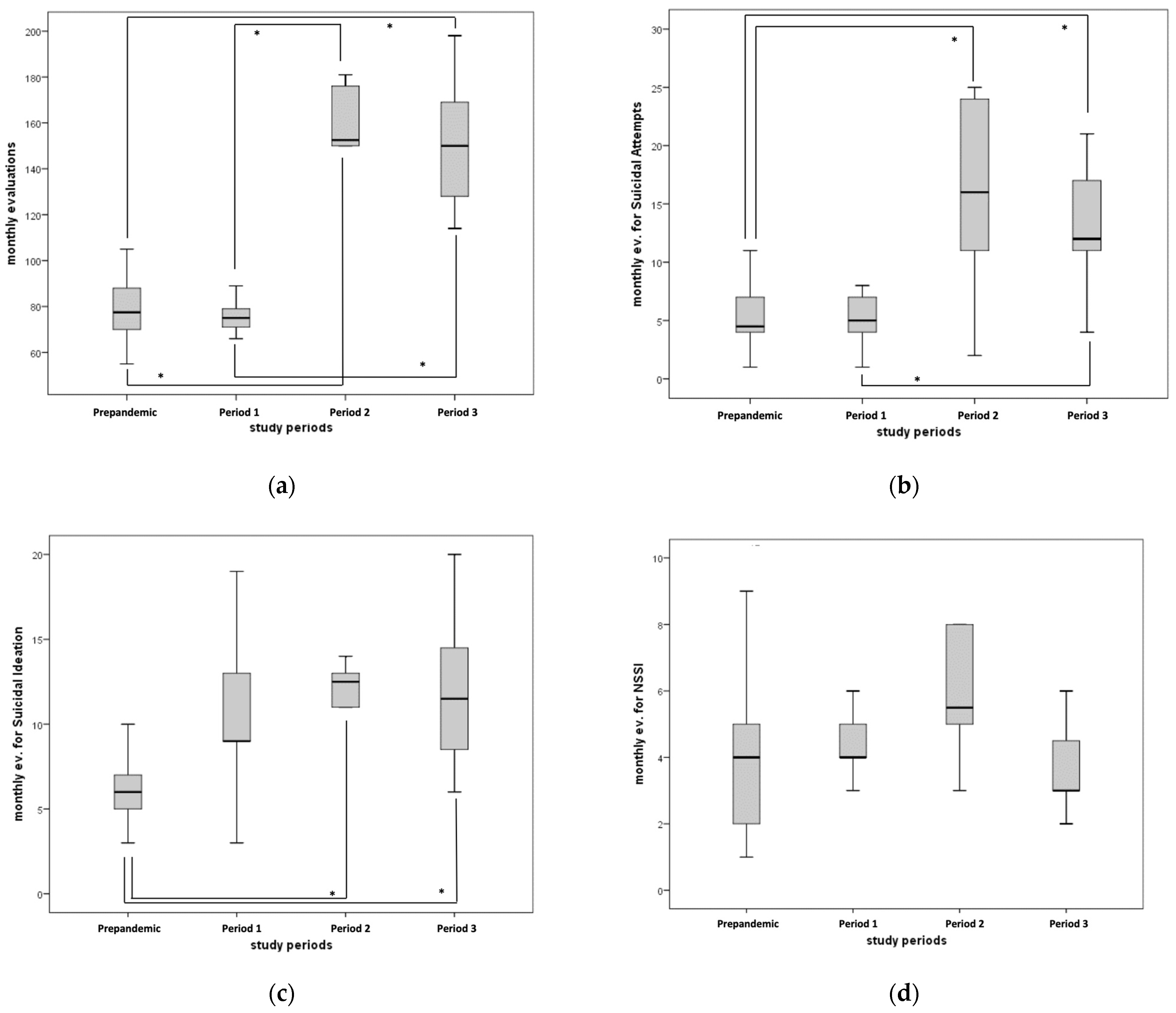
3.2. Child Psychiatry Consultations for Suicide Attempt and Suicidal Ideation during Different Pandemic Periods
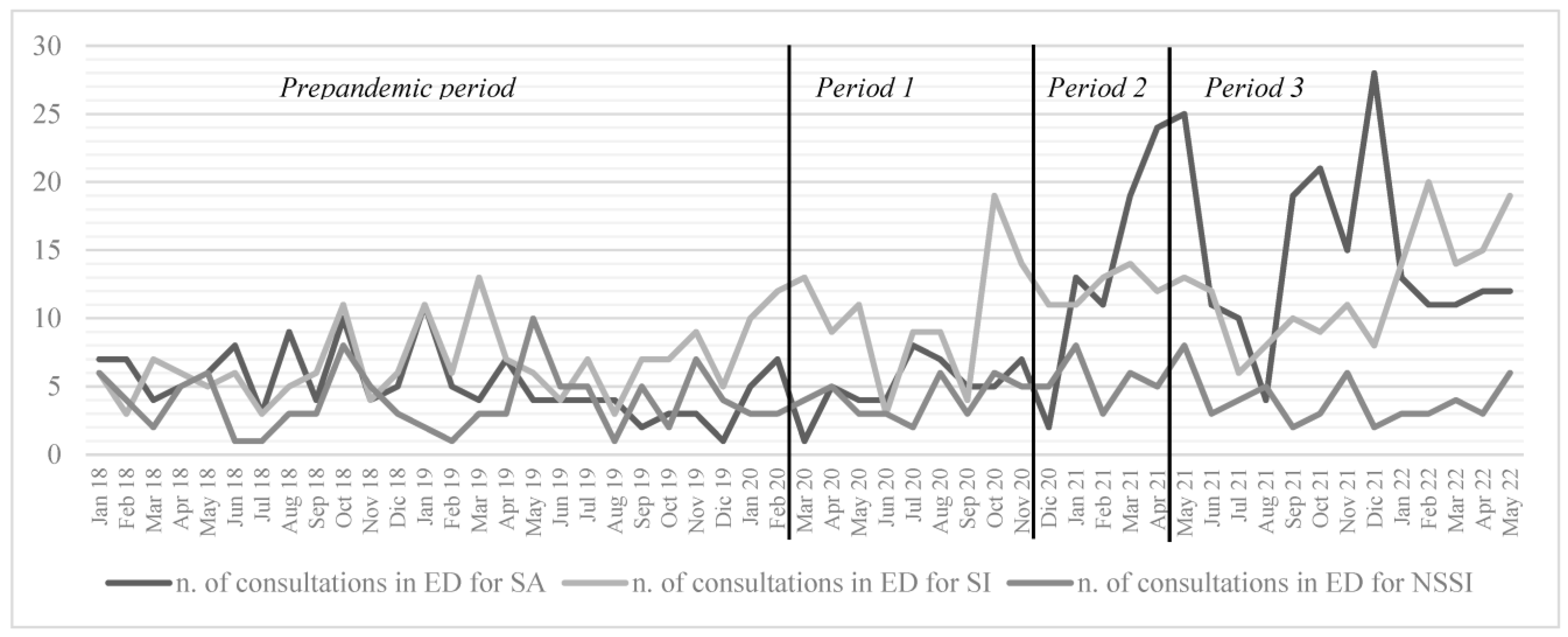
3.3. Access to the ED for Suicidal Attempts from 2018 to 2021
3.4. Suicide Attempts Pre- versus Post-COVID-19 Pandemic, Bivariate Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fazel, S.; Runeson, B. Suicide. N. Engl. J. Med. 2020, 382, 266–274. [Google Scholar] [CrossRef]
- Glenn, C.R.; Kleiman, E.M.; Kellerman, J.; Pollak, O.; Cha, C.B.; Esposito, E.C.; Porter, A.C.; Wyman, P.A.; Boatman, A.E. Annual Research Review: A meta-analytic review of worldwide suicide rates in adolescents. J. Child Psychol. Psychiatry 2019, 61, 294–308. [Google Scholar] [CrossRef]
- Istituto Nazionale di Statistica. Giornata Mondiale per la Prevenzione del Suicidio. In Le Statistiche Dell’Istat; ISTAT Istituto Nazionale di Statistica: Roma, Italy, 2017; Available online: https://www.istat.it/it/archivio/203353 (accessed on 15 December 2022).
- Jacobs, D.G.; Klein-Benheim, M. Current Status of Suicide-Focused Assessment and Treatment. An Online Resource for Clinicians. 2021. Available online: https://stopasuicide.org/wp-content/uploads/2023/05/Current-Status-of-Suicide-Focused-Assessment-and-Treatment-May-2023.pdf (accessed on 15 December 2022).
- Curtin, S.C. State Suicide Rates among Adolescents and Young Adults Aged 10–24: United States, 2000–2018; National Vital Statistics Reports Series; DHHS Publication: Hyattsville, MD, USA, 2020. [Google Scholar]
- Bould, H.; Mars, B.; Moran, P.; Biddle, L.; Gunnell, D. Rising suicide rates among adolescents in England and Wales. Lancet 2019, 394, 116–117. [Google Scholar] [CrossRef] [Green Version]
- Sheftall, A.H.; Asti, L.; Horowitz, L.M.; Felts, A.; Fontanella, C.A.; Campo, J.V.; Bridge, J.A. Suicide in Elementary School-Aged Children and Early Adolescents. Pediatrics 2016, 138, e20160436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plemmons, G.; Hall, M.; Doupnik, S.; Gay, J.; Brown, C.; Browning, W.; Casey, R.; Freundlich, K.; Johnson, D.P.; Lind, C.; et al. Hospitalization for Suicide Ideation or Attempt: 2008–2015. Pediatrics 2018, 141, e20172426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, E.; McMahon, E.; McNicholas, F.; Corcoran, P.; Perry, I.J.; Arensman, E. Increasing rates of self-harm among children, adolescents and young adults: A 10-year national registry study 2007–2016. Soc. Psychiatry 2018, 53, 663–671. [Google Scholar] [CrossRef]
- Collishaw, S. Annual Research Review: Secular trends in child and adolescent mental health. J. Child Psychol. Psychiatry 2014, 56, 370–393. [Google Scholar] [CrossRef]
- Castaldo, L.; Serra, G.; Piga, S.; Reale, A.; Vicari, S. Suicidal behaviour and non-suicidal self-injury in children and adolescents seen at an Italian paediatric emergency department. Ann. Dell’istituto Super. Sanità 2020, 56, 303–314. [Google Scholar] [CrossRef]
- Apicella, M.; Serra, G.; Trasolini, M.; Andracchio, E.; Chieppa, F.; Averna, R.; Iannoni, M.E.; Infranzi, A.; Moro, M.; Guidetti, C.; et al. Urgent psychiatric consultations for suicide attempt and suicidal ideation before and after the COVID-19 pandemic in an Italian pediatric emergency setting. Front. Psychiatry 2023, 14, 1135218. [Google Scholar] [CrossRef]
- Serra, G.; De Crescenzo, F.; Maisto, F.; Galante, J.R.; Iannoni, M.E.; Trasolini, M.; Maglio, G.; Tondo, L.; Baldessarini, R.J.; Vicari, S. Suicidal behavior in juvenile bipolar disorder and major depressive disorder patients: Systematic review and meta-analysis. J. Affect. Disord. 2022, 311, 572–581. [Google Scholar] [CrossRef]
- Baldessarini, R.; Tondo, L. Suicidal Risks in 12 DSM-5 Psychiatric Disorders. J. Affect. Disord. 2020, 271, 66–73. [Google Scholar] [CrossRef] [PubMed]
- GU, n.59, 08-03-2020. D.P.C.M. 8 Marzo 2020. Ulteriori Disposizioni Attuative del Decreto-legge 23 Febbraio 2020, n. 6, Recante Misure Urgenti in Materia di Contenimento e Gestione Dell’emergenza Epidemiologica da COVID-19. Gazzetta Ufficiale 8 Marzo 2020, n. 59, Edizione Straordinaria. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/08/20A01522/sg (accessed on 5 July 2023).
- GU, n.275, 04-11-2020. D.P.C.M. 3 Novembre 2020. Ulteriori Disposizioni Attuative del Decreto-Legge 25 Marzo 2020, n. 19, Convertito, con Modificazioni, dalla Legge 25 Maggio 2020, n. 35, Recante «Misure Urgenti per Fronteggiare L’emergenza Epidemiologica da COVID-19», e del Decreto-legge 16 Maggio 2020, n. 33, Convertito, con Modificazioni, dalla Legge 14 Luglio 2020, n. 74, Recante «Ulteriori Misure Rrgenti per Fronteggiare L’emergenza Epidemiologica da COVID-19». Supplemento Ordinario alla Gazzetta Ufficiale n. 275 del 4 Novembre 2020—Serie Generale. Available online: https://www.gazzettaufficiale.it/eli/id/2020/11/04/20A06109/sg (accessed on 5 July 2023).
- GU, n.96 del 22-04-2021. Decreto-Legge 22 Aprile 2021, n. 52. Misure Urgenti per la Graduale Ripresa delle Attività Economiche e Sociali nel Rispetto delle Esigenze di Contenimento della Diffusione Dell’epidemia da COVID-19 Gazzetta Ufficiale n. 96 del 22 Aprile 2021—Serie Generale. Available online: https://www.gazzettaufficiale.it/eli/id/2021/04/22/21G00064/sg (accessed on 5 July 2023).
- Posner, K.; Brodsky, B.; Yershova, K.; Buchanan, J.; Mann, J. The classification of suicidal behavior. In The Oxford Handbook of Suicide and Self-Injury; Oxford Press: Oxford, UK, 2014; pp. 7–22. [Google Scholar]
- Wilkinson, P.; Kelvin, R.; Roberts, C.; Dubicka, B.; Goodyer, I. Clinical and Psychosocial Predictors of Suicide Attempts and Nonsuicidal Self-Injury in the Adolescent Depression Antidepressants and Psychotherapy Trial (ADAPT). Am. J. Psychiatry 2011, 168, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Faust, J.S.; Shah, S.B.; Du, C.; Li, S.-X.; Lin, Z.; Krumholz, H.M. Suicide Deaths During the COVID-19 Stay-at-Home Advisory in Massachusetts, March to May 2020. JAMA Netw. Open 2021, 4, e2034273. [Google Scholar] [CrossRef] [PubMed]
- Ridout, K.K.; Alavi, M.; Ridout, S.J.; Koshy, M.T.; Awsare, S.; Harris, B.; Vinson, D.R.; Weisner, C.M.; Sterling, S.; Iturralde, E. Emergency Department Encounters Among Youth with Suicidal Thoughts or Behaviors During the COVID-19 Pandemic. JAMA Psychiatry 2021, 78, 1319. [Google Scholar] [CrossRef]
- Orben, A.; Tomova, L.; Blakemore, S.-J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- Rajmil, L.; Hjern, A.; Boran, P.; Gunnlaugsson, G.; de Camargo, O.K.; Raman, S. Impact of lockdown and school closure on children’s health and well-being during the first wave of COVID-19: A narrative review. BMJ Paediatr. Open 2021, 5, e001043. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Yard, E.; Radhakrishnan, L.; Ballesteros, M.F.; Sheppard, M.; Gates, A.; Stein, Z.; Hartnett, K.; Kite-Powell, A.; Rodgers, L.; Adjemian, J.; et al. Emergency Department Visits for Suspected Suicide Attempts Among Persons Aged 12–25 Years Before and During the COVID-19 Pandemic—United States, January 2019–May 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 888–894. [Google Scholar] [CrossRef]
- Gracia, R.; Pamias, M.; Mortier, P.; Alonso, J.; Pérez, V.; Palao, D. Is the COVID-19 pandemic a risk factor for suicide attempts in adolescent girls? J. Affect. Disord. 2021, 292, 139–141. [Google Scholar] [CrossRef]
- Sokoloff, W.C.; Krief, W.I.; Giusto, K.A.; Mohaimin, T.; Murphy-Hockett, C.; Rocker, J.; Williamson, K.A. Pediatric emergency department utilization during the COVID-19 pandemic in New York City. Am. J. Emerg. Med. 2021, 45, 100–104. [Google Scholar] [CrossRef]
- Mucci, M.; Lenzi, F.; D’Acunto, G.M.; Gazzillo, M.; Accorinti, I.; Boldrini, S.; Distefano, G.; Falcone, F.; Fossati, B.; Annina, R.G.; et al. How COVID-19 Phases Have Impacted Psychiatric Risk: A Retrospective Study in an Emergency Care Unit for Adolescents. Children 2022, 9, 1921. [Google Scholar] [CrossRef]
- Panda, P.K.; Gupta, J.; Chowdhury, S.R.; Kumar, R.; Meena, A.K.; Madaan, P.; Sharawat, I.K.; Gulati, S. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J. Trop. Pediatr. 2020, 67, fmaa122. [Google Scholar] [CrossRef] [PubMed]
- Fındık, O.T.P.; Erdoğdu, A.B.; Fadıloğlu, E.; Arman, A.R. Emergency Department Visits for Non-suicidal Self-harm, Suicidal Ideation, and Suicide Attempts in Children and Adolescents. Child Psychiatry Hum. Dev. 2021, 53, 289–299. [Google Scholar] [CrossRef]
- Coppersmith, D.D.; Nada-Raja, S.; Beautrais, A.L. Non-suicidal self-injury and suicide attempts in a New Zealand birth cohort. J. Affect. Disord. 2017, 221, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Bang, Y.S.; Min, S.; Ahn, J.-S.; Kim, H.; Cha, Y.-S.; Park, I.-S.; Kim, M.-H. Characteristics of adolescents who visit the emergency department following suicide attempts: Comparison study between adolescents and adults. BMC Psychiatry 2019, 19, 231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lilley, R.; Owens, D.; Horrocks, J.; House, A.; Noble, R.; Bergen, H.; Hawton, K.; Casey, D.; Simkin, S.; Murphy, E.; et al. Hospital care and repetition following self-harm: Multicentre comparison of self-poisoning and self-injury. Br. J. Psychiatry 2008, 192, 440–445. [Google Scholar] [CrossRef]
- Chartrand, H.; Kim, H.; Sareen, J.; Mahmoudi, M.; Bolton, J.M. A comparison of methods of self-harm without intent to die: Cutting versus self-poisoning. J. Affect. Disord. 2016, 205, 200–206. [Google Scholar] [CrossRef]
- Fox, K.R.; Millner, A.J.; Franklin, J.C. Classifying nonsuicidal overdoses: Nonsuicidal self-injury, suicide attempts, or neither? Psychiatry Res. 2016, 244, 235–242. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 2018 | 2019 | 2020 | 2021 | 2022 | Total | p-Value (F) | |
|---|---|---|---|---|---|---|---|
| Total psychiatric evaluations | 70.9 (11.4) | 88.3 (17.6) | 77.3 (11.8) | 152 (21.1) * | 157 (32.6) * | 103 (39.6) | <0.001 (51.2) |
| Evaluations for suicidal ideation, attempts and self harm | 15.8 (5.36) | 15.6 (4.70) | 19.5 (5.23) | 31.8 (8.49) * | 32.0 (3.39) * | 21.7 (9.18) | <0.001 (19.0) |
| Suicide attempts | 6.00 (2.22) | 4.33 (2.57) | 5.00 (2.09) | 16.7 (7.18) $ | 11.8 (0.84) * | 8.36 (6.25) | <0.001 (20.7) |
| Suicidal ideation | 5.67 (2.10) | 7.08 (2.81) | 10.3 (4.25) ** | 10.6 (2.43) ** | 16.4 (2.88) $ | 9.17 (4.24) | <0.001 (13.9) |
| Non-suicidal self-injury | 4.17 (2.29) | 4.17 (2.52) | 4.17 (1.27) | 4.58 (2.11) | 3.80 (1.30) | 4.23 (1.98) | 0.96 (0.15) |
| Age | 14.2 (3.54) | 14.0 (3.49) | 14.5 (3.10) ** | 14.6 (2.81) ** | 14.7 (2.63) ** | 14.4 (3.12) | <0.001 (8.19) |
| Pre-Pandemic | Period 1 | Period 2 | Period 3 | Total | Kruskal–Wallis; p-Value | |
|---|---|---|---|---|---|---|
| Total | 77.5 (69.8–88.0) | 75.0 (68.5–84.0) | 153 (132–177) | 150 (124–174) | 86.0 (73.5–138) | 31.4; p < 0.001 |
| Suicide attempts | 4.50 (4.00–7.00) | 5.00 (4.00–7.00) | 16.0 (8.75–24.3) | 12.0 (11.0–18.0) | 7.00 (4.00–11.0) | 23.4; p < 0.001 |
| Suicidal ideation | 6.00 (5.00–7.50) | 9.00 (6.50–13.5) | 12.5 (11.0–13.3) | 11.50 (8.25–14.8) | 9.00 (6.00–12.0) | 19.7; p < 0.001 |
| Non-suicidal self-injury | 4.00 (2.00–5.00) | 4.00 (3.50–5.50) | 5.50 (4.50–8.00) | 3.00 (3.004.75) | 4.00 (3.00–5.00) | 5.32; p = 0.150 |
| Pre-Pandemic N = 136 | During Pandemic N = 248 | Total N = 384 | Statistic | p-Value | |
|---|---|---|---|---|---|
| Age | 16 (1.58) | 15.7 (1.42) | 15.8 (1.48) | 1.796 | 0.073 |
| Female sex | 85.3% (116) | 83.5% (207) | 84.1% (323) | 0.219 | 0.640 |
| Anamnesis of at least one previous psychiatric evaluation in ED for any reason | 50.0% (68) | 46.8% (116) | 47.9% (184) | 0.366 | 0.545 |
| Number of previous psychiatric evaluation in ED for any reason | 1.81 (4.65) | 1.19 (3.23) | 1.41 (3.81) | 1.379 | 0.169 |
| Methods of SA | |||||
| Cutting, ICD-10 X78 | 6.62% (9) | 6.85% (17) | 6.77% (26) | 0.008 | 0.929 |
| Precipitation, ICD-10 X80 | 22.8% (31) | 12.9% (32) | 16.4% (63) | 6.265 | 0.012 |
| Self-poisoning, ICD-10 X60-69 | 57.4% (78) | 68.9% (171) | 64.8% (249) | 5.183 | 0.023 |
| Suffocation, ICD-10 X70-71 | 10.3% (14) | 8.47% (21) | 9.11% (35) | 0.354 | 0.552 |
| Vehicle accident, ICD-10 X81 | 2.94% (4) | 1.61% (4) | 2.08% (8) | 0.760 | 0.383 |
| Psychiatric diagnosis at admission | |||||
| Any mood disorder diagnosis | 65.4% (89) | 83.1% (206) | 76.8% (295) | 15.321 | <0.001 |
| Bipolar and related disorders | 3.68% (5) | 4.03% (10) | 3.91% (15) | 0.030 | 0.863 |
| Major depressive episode | 41.2% (56) | 63.7% (158) | 55.7% (214) | 18.076 | <0.001 |
| Mood disorder not otherwise specified | 20.6% (28) | 15.3% (38) | 17.2% (66) | 1.711 | 0.191 |
| Psychosis not otherwise specified | 6.62% (9) | 2.82% (7) | 4.17% (16) | 3.168 | 0.075 |
| Post-traumatic stress disorder | 10.3% (14) | 4.84% (12) | 6.77% (26) | 4.141 | 0.055 |
| Anxiety disorder | 0.735% (1) | 2.02% (5) | 1.56% (6) | 0.937 | 0.333 |
| Oppositional defiant disorder/conduct disorder | 10.3% (14) | 3.63% (9) | 5.99% (23) | 6.929 | 0.008 |
| Eating disorder | 3.68% (5) | 1.61% (4) | 2.34% (9) | 1.634 | 0.289 |
| Presence of at least one comorbid neurodevelopmental disorder | 14.7% (20) | 4.44% (11) | 8.07% (31) | 12.484 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serra, G.; Apicella, M.; Iannoni, M.E.; Trasolini, M.; Andracchio, E.; Chieppa, F.; Averna, R.; Guidetti, C.; Maglio, G.; Reale, A.; et al. Urgent Psychiatric Consultations for Suicidal Ideation and Behaviors in Italian Adolescents during Different COVID-19 Pandemic Phases. J. Pers. Med. 2023, 13, 1112. https://doi.org/10.3390/jpm13071112
Serra G, Apicella M, Iannoni ME, Trasolini M, Andracchio E, Chieppa F, Averna R, Guidetti C, Maglio G, Reale A, et al. Urgent Psychiatric Consultations for Suicidal Ideation and Behaviors in Italian Adolescents during Different COVID-19 Pandemic Phases. Journal of Personalized Medicine. 2023; 13(7):1112. https://doi.org/10.3390/jpm13071112
Chicago/Turabian StyleSerra, Giulia, Massimo Apicella, Maria Elena Iannoni, Monia Trasolini, Elisa Andracchio, Fabrizia Chieppa, Roberto Averna, Clotilde Guidetti, Gino Maglio, Antonino Reale, and et al. 2023. "Urgent Psychiatric Consultations for Suicidal Ideation and Behaviors in Italian Adolescents during Different COVID-19 Pandemic Phases" Journal of Personalized Medicine 13, no. 7: 1112. https://doi.org/10.3390/jpm13071112