
Clinical and Radiographic Outcomes and Treatment Algorithm for Septic Arthritis in Children
 , , , , , and
, , , , , and
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Most Common Microorganisms |
|---|---|
| <3 months | Staphylococcus aureus; Streptococcus agalactiae; Neisseria gonorrhoeae; Candida; |
| 3 months–5 years | Staphylococcus aureus; Streptococcus; Kingella kingae; Streptococcus pneumoniae; Haemophilus influenzae type b; |
| >5 years | Staphylococcus aureus; Streptococcus; Streptococcus pneumoniae; Salmonella; Neisseria meningitidis. |
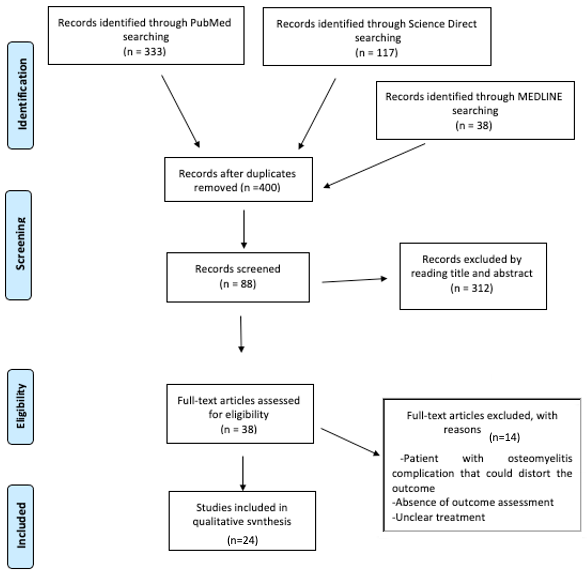
2. Materials and Methods
2.1. Search Selection
2.2. Study Selection
2.3. Data Extraction
2.4. Outcome Measures
3. Results
3.1. Demographics
3.2. Treatment of Septic Arthritis
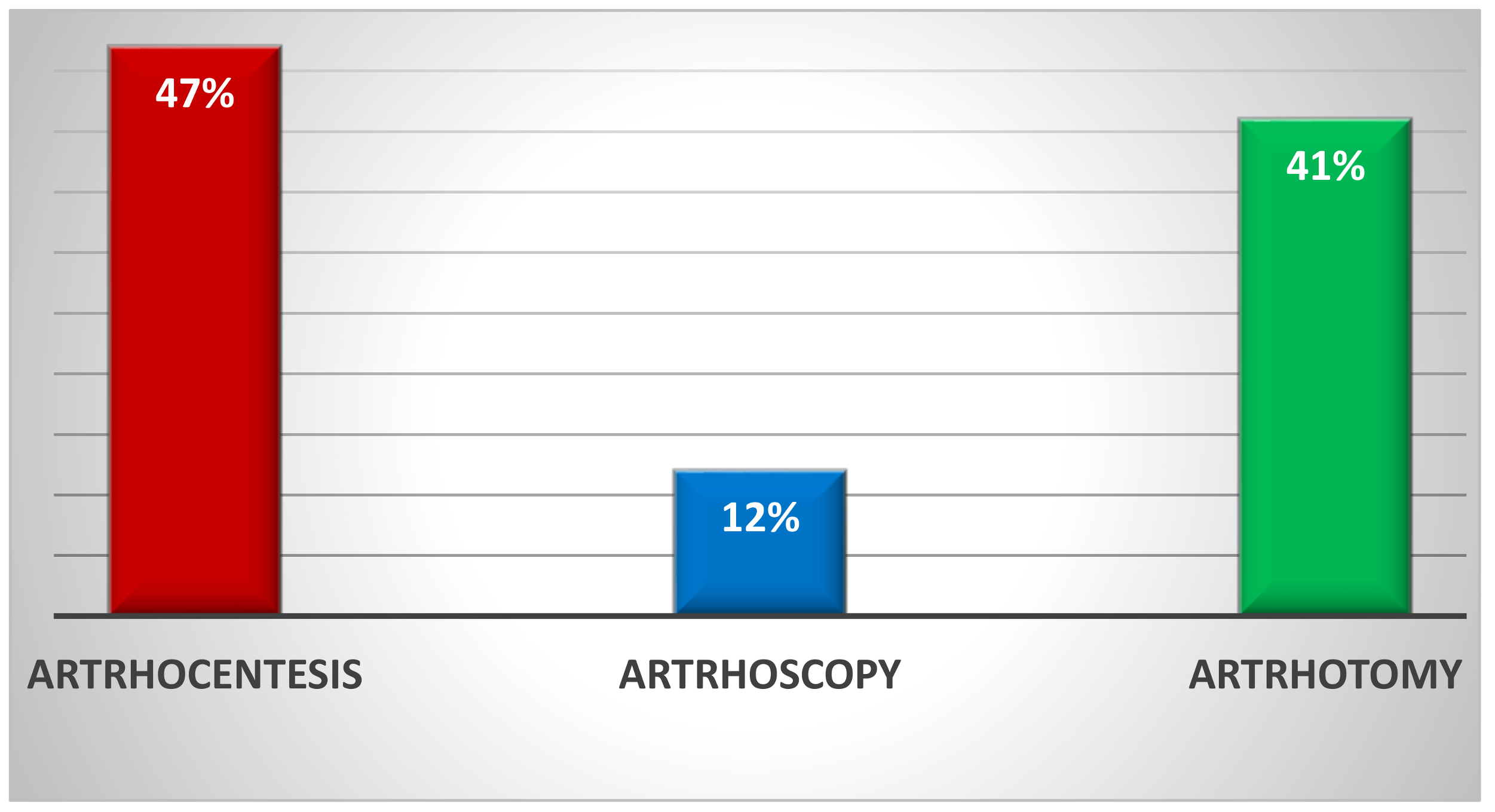
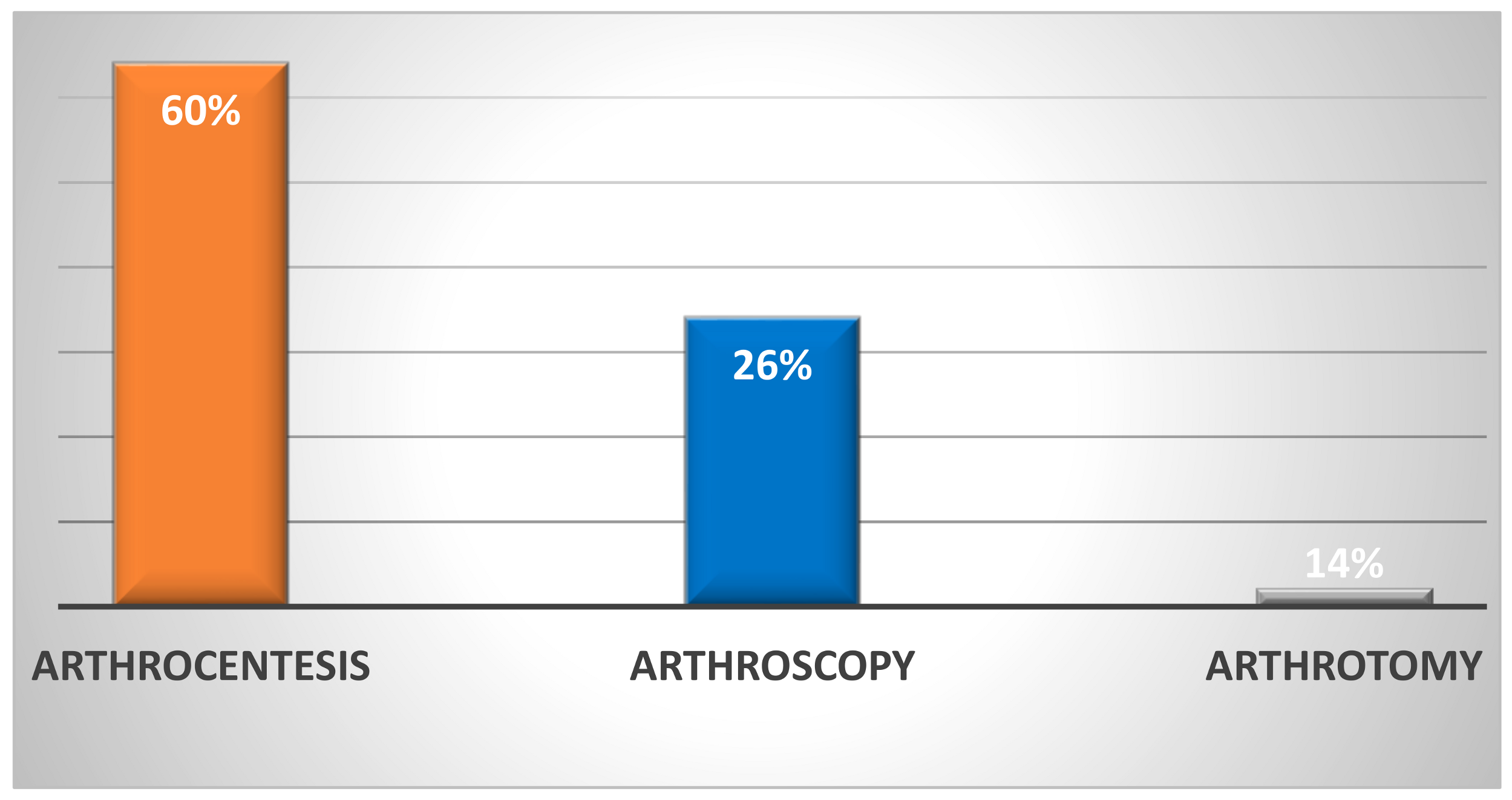
3.3. Type of Initial Treatment for Septic Hip Arthritis
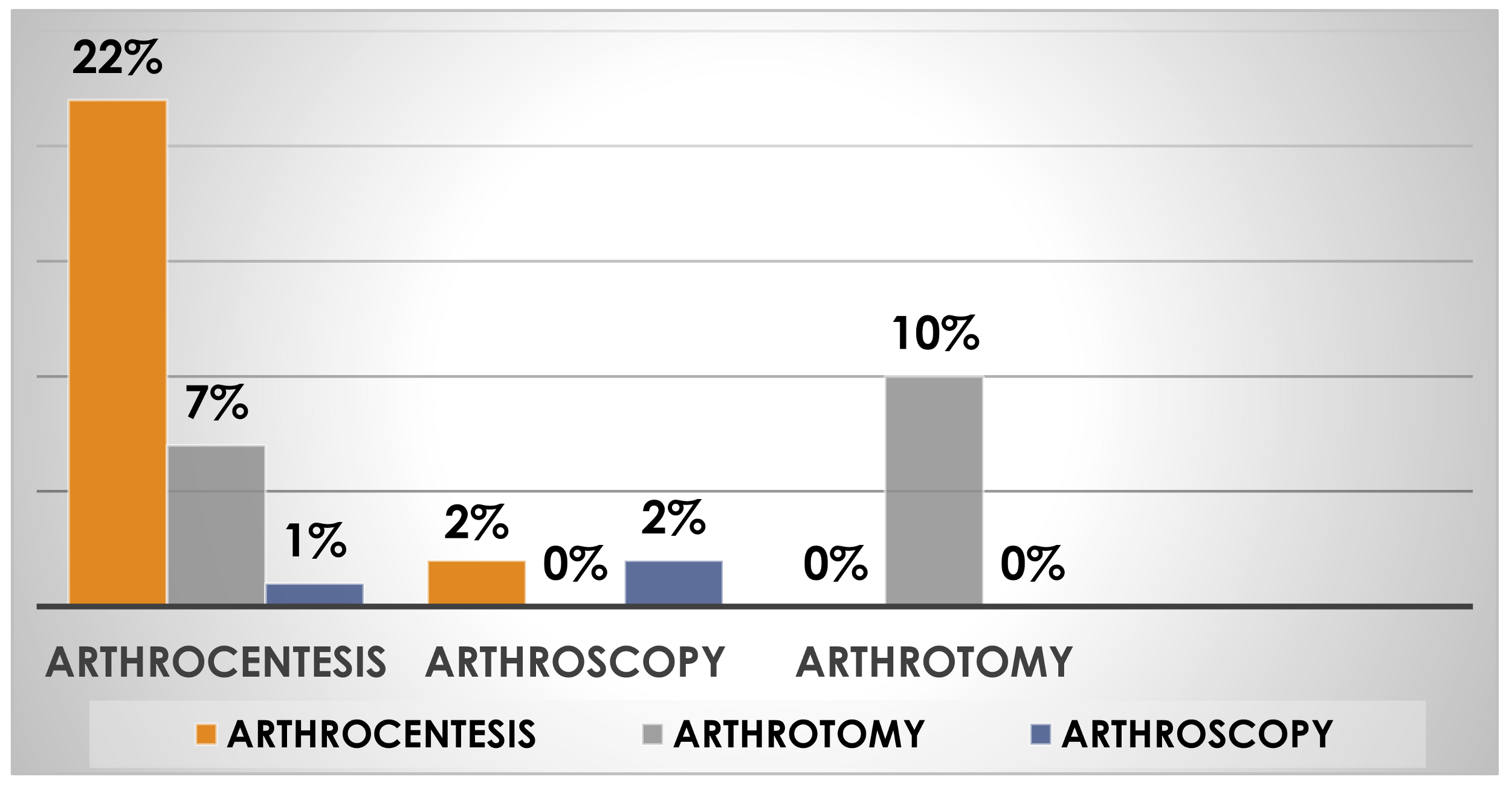
3.4. Percentage of Reoperation in Septic Hip Arthritis by Type of Initial Treatment
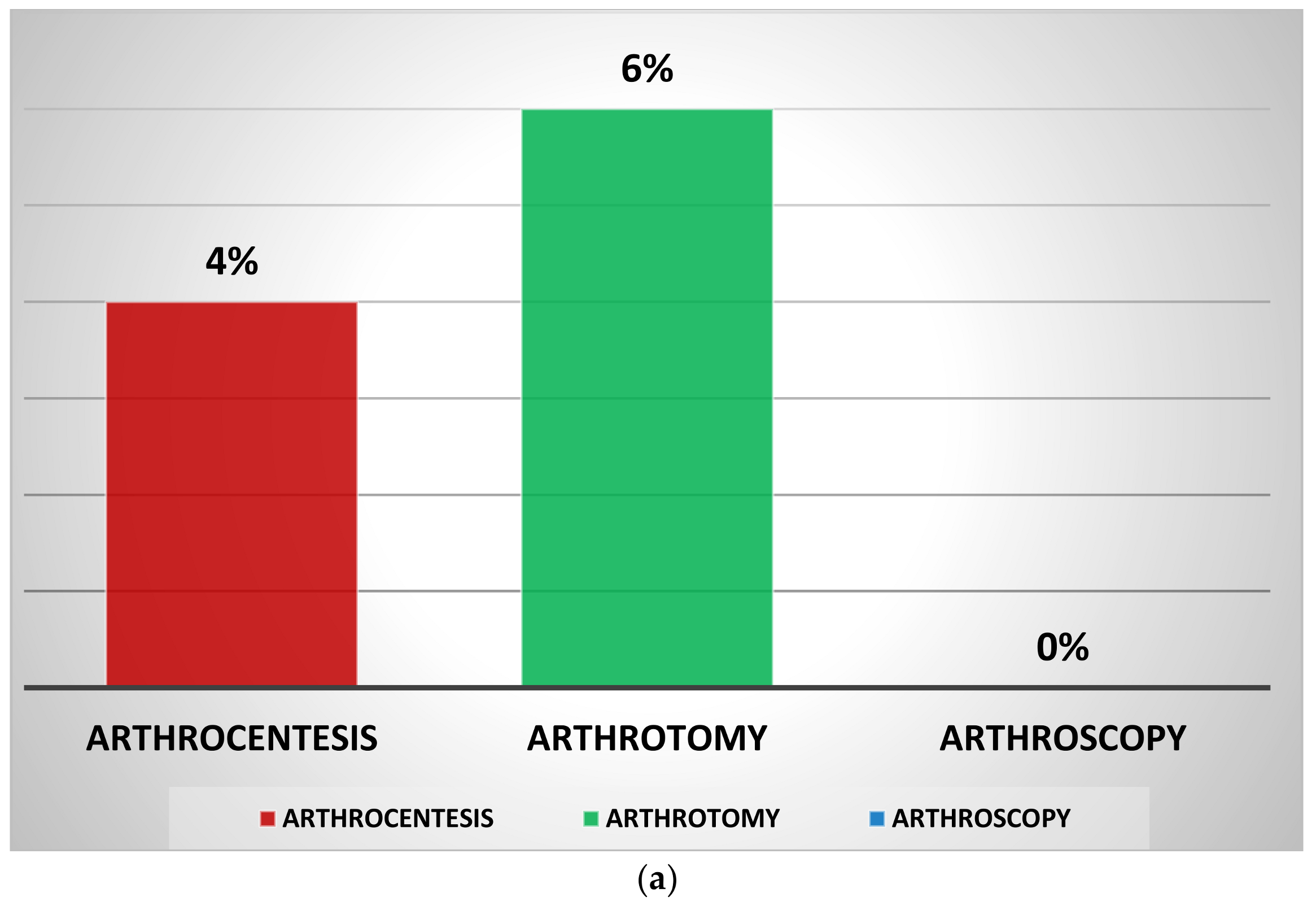
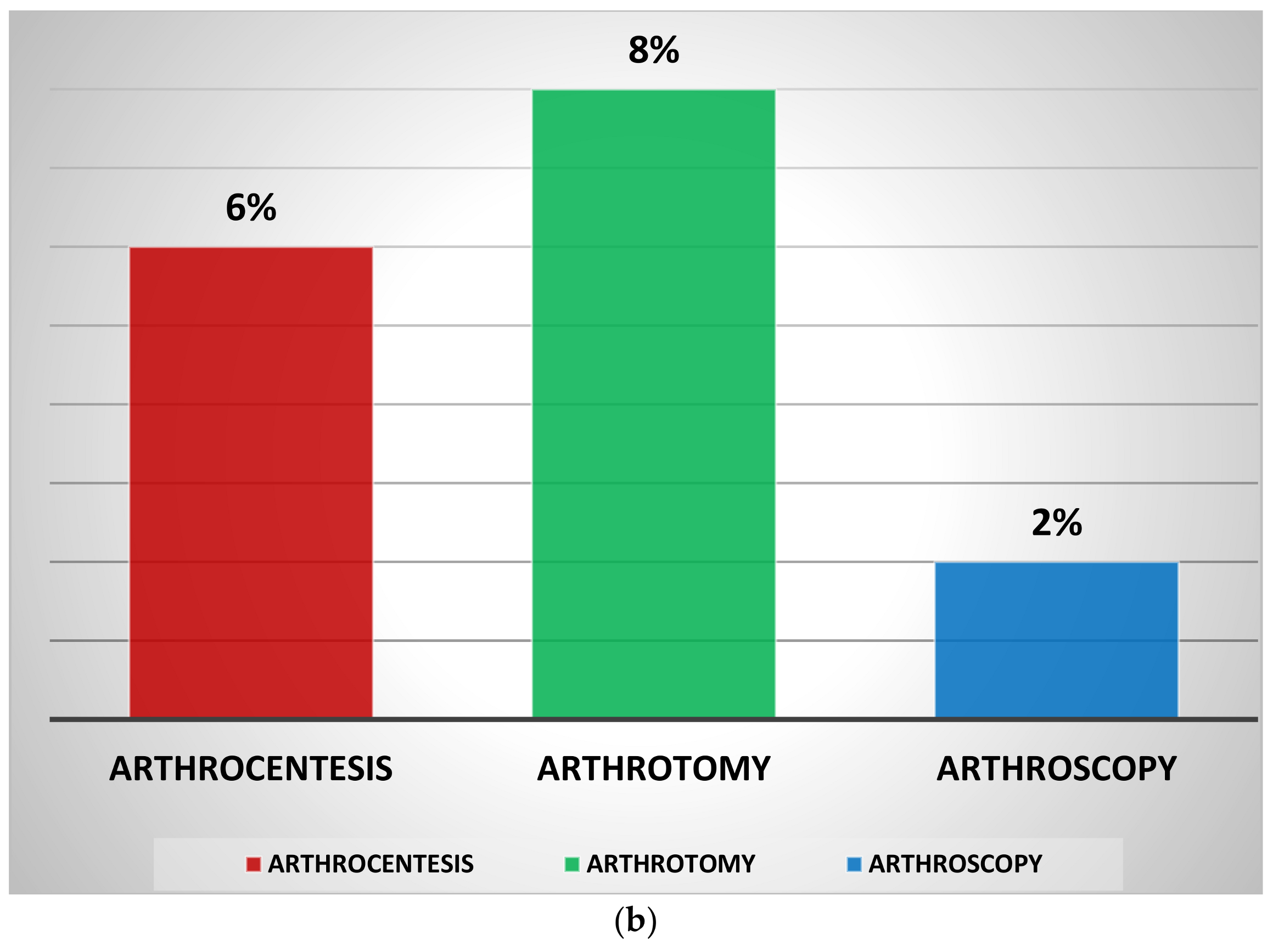
3.5. Percentage of Clinical Complications in Septic Hip Arthritis by Type of Initial Treatment
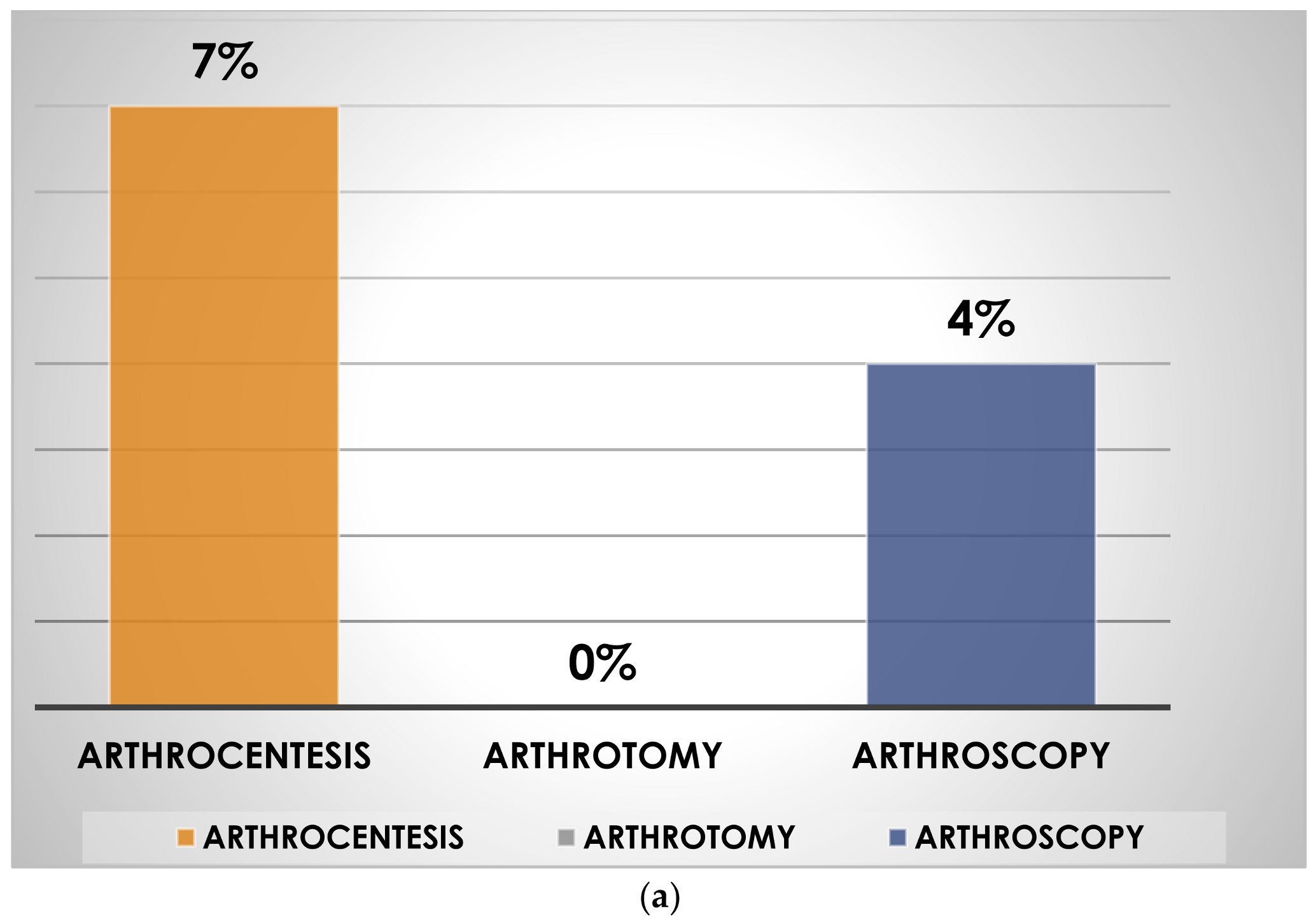
3.6. Percentage of Radiological Complications in Septic Hip Arthritis by Type of Initial Treatment
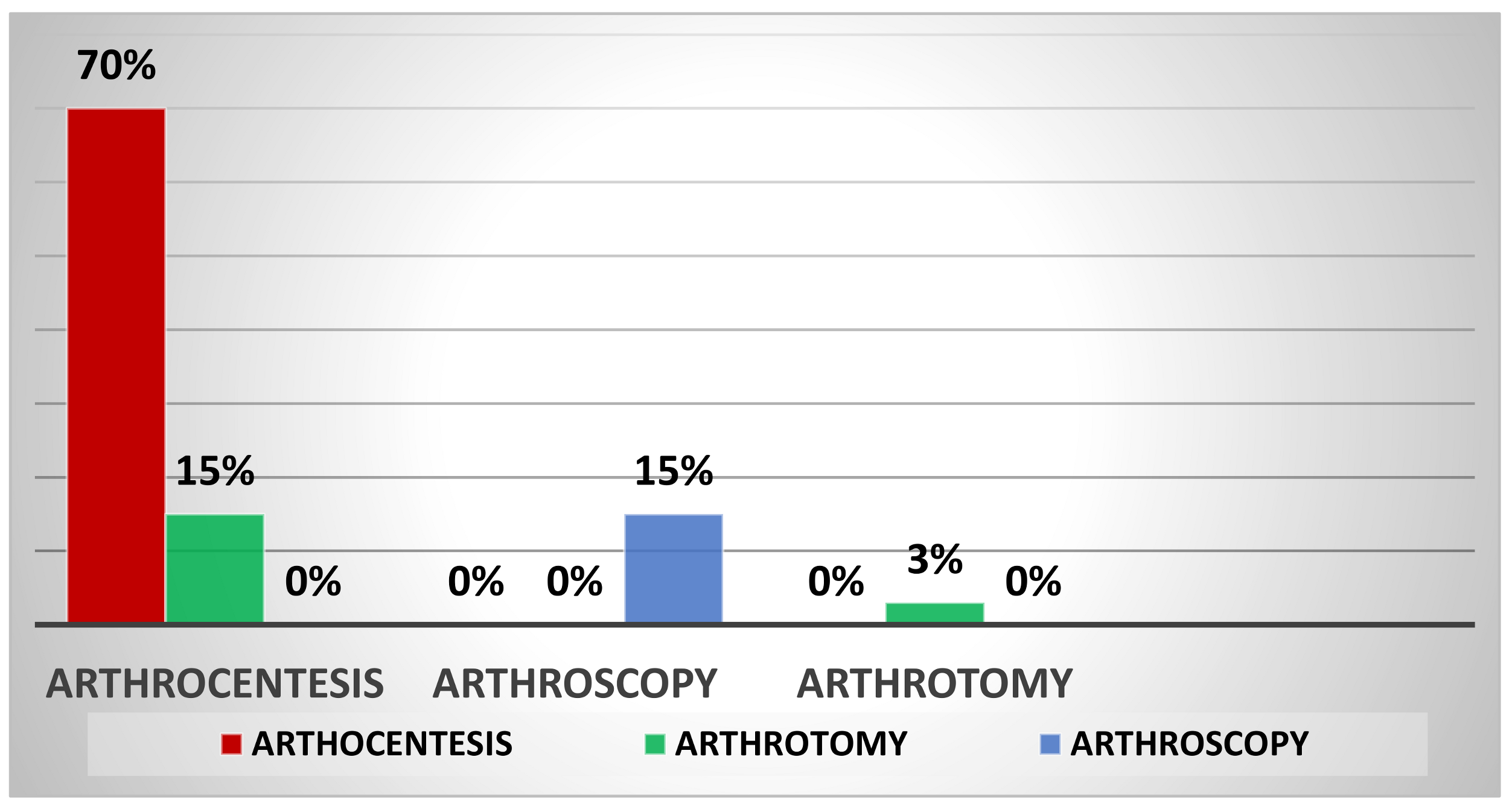
3.7. Type of Initial Treatment for Septic Knee Arthritis
3.8. Percentage of Reoperation in Septic Knee Arthritis by Type of Initial Treatment
3.9. Percentage of Clinical Complications in Septic Knee Arthritis by Type of Initial Treatment
3.10. Percentage of Radiological Complications in Septic Knee Arthritis by Type of Initial Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rutz, E. Septic Arthritis of the Hip Joint in Children Is an Emergency. Afr. J. Paediatr. Surg. 2012, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Saavedra-Lozano, J.; Falup-Pecurariu, O.; Faust, S.N.; Girschick, H.; Hartwig, N.; Kaplan, S.; Lorrot, M.; Mantadakis, E.; Peltola, H.; Rojo, P.; et al. Bone and Joint Infections. Pediatr. Infect. Dis. J. 2017, 36, 788–799. [Google Scholar] [CrossRef]
- Wall, C.; Donnan, L. Septic Arthritis in Children. Aust. Fam. Physician 2015, 44, 213–215. [Google Scholar] [PubMed]
- Pääkkönen, M.; Peltola, H. Treatment of Acute Septic Arthritis. Pediatr. Infect. Dis. J. 2013, 32, 684–685. [Google Scholar] [CrossRef]
- Arnold, J.C.; Bradley, J.S. Osteoarticular Infections in Children. Infect. Dis. Clin. N. Am. 2015, 29, 557–574. [Google Scholar] [CrossRef] [PubMed]
- Castellazzi, L.; Mantero, M.; Esposito, S. Update on the Management of Pediatric Acute Osteomyelitis and Septic Arthritis. Int. J. Mol. Sci. 2016, 17, 855. [Google Scholar] [CrossRef] [Green Version]
- Swarup, I.; Meza, B.C.; Weltsch, D.; Jina, A.A.; Lawrence, J.T.; Baldwin, K.D. Septic Arthritis of the Knee in Children: A Critical Analysis Review. JBJS Rev. 2020, 8, e0069. [Google Scholar] [CrossRef]
- Ben-Zvi, L.; Sebag, D.; Izhaki, G.; Katz, E.; Bernfeld, B. Diagnosis and Management of Infectious Arthritis in Children. Curr. Infect. Dis. Rep. 2019, 21, 23. [Google Scholar] [CrossRef]
- Dodwell, E.R. Osteomyelitis and Septic Arthritis in Children: Current Concepts. Curr. Opin. Pediatr. 2013, 25, 58–63. [Google Scholar] [CrossRef]
- Ceroni, D.; Cherkaoui, A.; Ferey, S.; Kaelin, A.; Schrenzel, J. Kingella kingae Osteoarticular Infections in Young Children: Clinical Features and Contribution of a New Specific Real-Time PCR Assay to the Diagnosis. J. Pediatr. Orthop. 2010, 30, 301–304. [Google Scholar] [CrossRef]
- Brown, D.W.; Sheffer, B.W. Pediatric Septic Arthritis. Orthop. Clin. N. Am. 2019, 50, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Rutz, E.; Spoerri, M. Septic Arthritis of the Paediatric Hip—A Review of Current Diagnostic Approaches and Therapeutic Concepts. Acta Orthop. Belg. 2013, 79, 123–134. [Google Scholar]
- Donders, C.M.; Spaans, A.J.; Bessems, J.H.J.M.; van Bergen, C.J.A. A Systematic Review of the Optimal Drainage Technique for Septic Hip Arthritis in Children. HIP Int. 2022, 32, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Mignemi, M.E.; Menge, T.J.; Cole, H.A.; Mencio, G.A.; Martus, J.E.; Lovejoy, S.; Stutz, C.M.; Schoenecker, J.G. Epidemiology, Diagnosis, and Treatment of Pericapsular Pyomyositis of the Hip in Children. J. Pediatr. Orthop. 2014, 34, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Zurakowski, D.; Kasser, J.R. Differentiating between Septic Arthritis and Transient Synovitis of the Hip in Children: An Evidence-Based Clinical Prediction Algorithm. J. Bone Jt. Surg. 1999, 81, 1662–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saavedra-Lozano, J.; Calvo, C.; Huguet Carol, R.; Rodrigo, C.; Núñez, E.; Obando, I.; Rojo, P.; Merino, R.; Pérez, C.; Downey, F.J.; et al. SEIP–SERPE–SEOP Consensus Document on the Treatment of Uncomplicated Acute Osteomyelitis and Septic Arthritis. An. Pediatr. Engl. Ed. 2015, 82, 273.e1–273.e10. [Google Scholar] [CrossRef] [PubMed]
- Tantillo, T.J.; Katsigiorgis, G. Arthrocentesis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Puebla, D.L.; Farrow, R.A. Ultrasound Guided Arthrocentesis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Swarup, I.; LaValva, S.; Shah, R.; Sankar, W.N. Septic Arthritis of the Hip in Children: A Critical Analysis Review. JBJS Rev. 2020, 8, e0103. [Google Scholar] [CrossRef]
- Agout, C.; Lakhal, W.; Fournier, J.; de Bodman, C.; Bonnard, C. Arthroscopic Treatment of Septic Arthritis of the Knee in Children. Orthop. Traumatol. Surg. Res. 2015, 101, S333–S336. [Google Scholar] [CrossRef] [Green Version]
- Simpson, J.; Sadri, H.; Villar, R. Hip Arthroscopy Technique and Complications. Orthop. Traumatol. Surg. Res. 2010, 96, S68–S76. [Google Scholar] [CrossRef] [Green Version]
- Burman, M.S.; Peltier, L.F. Arthroscopy or the Direct Visualization of Joints: An Experimental Cadaver Study. Clin. Orthop. 2001, 390, 5–9. [Google Scholar] [CrossRef]
- Kotlarsky, P.; Shavit, I.; Kassis, I.; Eidelman, M. Treatment of Septic Hip in a Pediatric ED: A Retrospective Case Series Analysis. Am. J. Emerg. Med. 2016, 34, 602–605. [Google Scholar] [CrossRef]
- Thomas, M.; Bonacorsi, S.; Simon, A.-L.; Mallet, C.; Lorrot, M.; Faye, A.; Dingulu, G.; Caseris, M.; Boneca, I.G.; Aupiais, C.; et al. Acute Monoarthritis in Young Children: Comparing the Characteristics of Patients with Juvenile Idiopathic Arthritis versus Septic and Undifferentiated Arthritis. Sci. Rep. 2021, 11, 3422. [Google Scholar] [CrossRef] [PubMed]
- Biyani, A.; Sharma, J.C. Continuous Suction and Intermittent Irrigation for Septic Coxitis. Acta Orthop. Scand. 1988, 59, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Givon, U.; Liberman, B.; Schindler, A.; Blankstein, A.; Ganel, A. Treatment of Septic Arthritis of the Hip Joint by Repeated Ultrasound-Guided Aspirations. J. Pediatr. Orthop. 2004, 24, 266–270. [Google Scholar] [CrossRef]
- Pääkkönen, M.; Kallio, M.J.T.; Peltola, H.; Kallio, P.E. Pediatric Septic Hip with or without Arthrotomy: Retrospective Analysis of 62 Consecutive Nonneonatal Culture-Positive Cases. J. Pediatr. Orthop. B 2010, 19, 264–269. [Google Scholar] [CrossRef]
- Nusem, I.; McAlister, A. Arthroscopic lavage for the treatment of septic arthritis of the hip in children. Acta Orthop. Belg. 2012, 78, 730–734. [Google Scholar]
- Lyon, R.M.; Evanich, J.D. Culture-Negative Septic Arthritis in Children. J. Pediatr. Orthop. 1999, 19, 655–659. [Google Scholar] [CrossRef]
- Samilson, R.L.; Bersani, F.A.; Watkins, M.B. Acute Suppurative Arthritis in Infants and Children; the Importance of Early Diagnosis and Surgical Drainage. Pediatrics 1958, 21, 798–804. [Google Scholar] [CrossRef]
- Bennett, O.M.; Namnyak, S.S. Acute Septic Arthritis of the Hip Joint in Infancy and Childhood. Clin. Orthop. Relat. Res. 1992, 281, 123–132. [Google Scholar] [CrossRef]
- Umer, M.; Hashmi, P.; Ahmad, T.; Ahmed, M.; Umar, M. Septic Arthritis of the Hip in Children—Aga Khan University Hospital Experience in Pakistan. J. Pak. Med. Assoc. 2003, 53, 472–478. [Google Scholar]
- Kim, H.K.; Alman, B.; Cole, W.G. A Shortened Course of Parenteral Antibiotic Therapy in the Management of Acute Septic Arthritis of the Hip. J. Pediatr. Orthop. 2000, 20, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Wiley, J.J.; Fraser, G.A. Septic Arthritis in Childhood. Can. J. Surg. 1979, 22, 326–330. [Google Scholar] [PubMed]
- Sanpera, I.; Raluy-Collado, D.; Sanpera-Iglesias, J. Arthroscopy for Hip Septic Arthritis in Children. Orthop. Traumatol. Surg. Res. 2016, 102, 87–89. [Google Scholar] [CrossRef]
- Chung, W.K.; Slater, G.L.; Bates, E.H. Treatment of Septic Arthritis of the Hip by Arthroscopic Lavage. J. Pediatr. Orthop. 1993, 13, 444–446. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, A.M.M. Treatment of Early Septic Arthritis of the Hip in Children: Comparison of Results of Open Arthrotomy versus Arthroscopic Drainage. J. Child. Orthop. 2008, 2, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, F.; Langendörfer, M.; Wirth, T.; Eberhardt, O. Arthroskopische Behandlung von septischen Hüftgelenksinfekten im Kindes- und Jugendalter. Z. Orthop. Unf. 2013, 151, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Griffet, J.; Oborocianu, I.; Rubio, A.; Leroux, J.; Lauron, J.; Hayek, T. Percutaneous Aspiration Irrigation Drainage Technique in the Management of Septic Arthritis in Children. J. Trauma Inj. Infect. Crit. Care 2011, 70, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Halder, D.; Seng, Q.B.; Malik, A.S.; Choo, K.E. Neonatal Septic Arthritis. Southeast Asian J. Trop. Med. Public Health 1996, 27, 600–605. [Google Scholar]
- Strong, M.; Lejman, T.; Michno, P.; Hayman, M. Sequelae from Septic Arthritis of the Knee during the First Two Years of Life. J. Pediatr. Orthop. 1994, 14, 745–751. [Google Scholar] [CrossRef]
- Herndon, W.A.; Knauer, S.; Sullivan, J.A.; Gross, R.H. Management of Septic Arthritis in Children. J. Pediatr. Orthop. 1986, 6, 576–578. [Google Scholar] [CrossRef]
- Katz, K.; Goldberg, I.; Yosipovitch, Z. Early Mobilization in Septic Arthritis. 14 Children Followed for 2 Years. Acta Orthop. Scand. 1990, 61, 161–162. [Google Scholar] [CrossRef] [PubMed]
- Johns, B.; Loewenthal, M.; Ho, E.; Dewar, D. Arthroscopic Versus Open Treatment for Acute Septic Arthritis of the Knee in Children. Pediatr. Infect. Dis. J. 2018, 37, 413–418. [Google Scholar] [CrossRef]
- Stanitski, C.L.; Harvell, J.C.; Fu, F.H. Arthroscopy in Acute Septic Knees. Management in Pediatric Patients. Clin. Orthop. Relat. Res. 1989, 241, 209–212. [Google Scholar] [CrossRef]
- Smith, M.J. Arthroscopic Treatment of the Septic Knee. Arthroscopy 1986, 2, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.R.; Larson, C.M.; Bedi, A. Indications for Hip Arthroscopy. Sports Health Multidiscip. Approach 2017, 9, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Hoswell, R.L.; Johns, B.P.; Loewenthal, M.R.; Dewar, D.C. Outcomes of Paediatric Septic Arthritis of the Hip and Knee at 1-20 Years in an Australian Urban Centre. ANZ J. Surg. 2019, 89, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-N.; Sanghera, T.; Mangwani, J.; Paterson, J.M.H.; Ramachandran, M. The Management of Septic Arthritis in Children: Systematic review of the english language literature. J. Bone Jt. Surg. Br. 2009, 91-B, 1127–1133. [Google Scholar] [CrossRef] [Green Version]










| Ref | Author | Joint | No. of Joints | Treatment | Mean Follow-Up | Radiological Outcome | Clinical Outcome |
|---|---|---|---|---|---|---|---|
| [23] | Kotlarsky P. et al. (2016) | Hip | 14 | AS | 6–8 Y | None | None |
| [24] | Thomas M. et al. (2021) | Hip | 103 | AS + AT (82) AC (21) | Nk | Nk | Nk |
| [25] | Byani A. et al. (1988) | Hip | 42 | AS | 1–3 Y | Coxa Magna, Joint destruction | Limitation of ROM |
| [26] | Givon U. et al. (2004) | Hip | 28 | AS | 2–9 Y | None | None |
| [27] | Pääkkönen (2010) | Hip | 45 | AS | >1 Y | None | None |
| [28] | Griffet J. et al. (2011) | Hip | 19 | AS | 1–3 Y | Smaller ossification nucleus, Coxa Magna | None |
| [29] | Lyon R.M. et al. (1999) | Hip | 25 | AT | 4 M–7 Y | Heterotop ossification, Coxa-Magna | None |
| [30] | Samilson S.R. et al. (1958) | Hip | 7 | AS | 10 Y | None | None |
| [31] | Bennett O.M. et al. (1992) | Hip | 45 | AT | 2–5 Y | Coxa Magna, Ischemic necrosis of epiphysis, dysplasia of the acetabolum | Reduction of ROM, residual pain, limb length discrepancy |
| [32] | Umer et al. (2003) | Hip | 40 | AT | 1–2 Y | Partial growth plate, partial avascular necrosis of the femoral epiphysis | Reduction of ROM |
| [33] | Kim H.M. et al. (2000) | Hip | 20 | AT | 1–5 Y | Smaller ossification nucleus, Coxa Magna | Residual pain |
| [34] | Wiley J.J. et al. (1999) | Hip Knee | 16 15 + 7 | AT AC + AT | Nk Nk | Avascularal necrosis None | Reduction of ROM None |
| [35] | Sanpera I. et al. (2016) | Hip | 11 | AS | 3–8 Y | Metaphyseal modification | None |
| [36] | Chung W.K. et al. (1993) | Hip | 9 | AS | Nk | Metaphyseal modification | None |
| [37] | El- Sayed et al. (2008) | Hip | 10 | AS | 1–3 Y | None | None |
| [38] | Fernandez F. et al. 2013) | Hip | 18 | AS | 6 M–4 Y | Avascular necrosis | Limitation of the ROM |
| [23] | Kotlarsky P. et al. (2016) | Knee | 17 | AC | 4 Y | None | None |
| [39] | Halder D. et al. (1996) | Knee | 9 | AC | 3–16 M | None | Limitation of the ROM |
| [40] | Strong M. et al. (1954) | Knee | 50 | AC | 1–21 Y | None | Pain, limb length discrepancy, reduction of ROM |
| [41] | Herdon W.A. et al. (1986) | Knee | 15 | AC | 1–5 Y | None | None |
| [42] | Katz K. et al. (1990) | Knee | 5 | AT | 1–3 Y | Partial necrosis of the tibial plate | None |
| [43] | Johns B. et al. (2018) | Knee | 13 11 | AT AS | 1–20 Y | None | None |
| [44] | Smith M.J. et al. (1956) | Knee | 20 | AS | 6–60 M | None | None |
| [45] | Stanitski C.L. et al. (1989) | Knee | 15 | AS | 30–48 M | None | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldaci, A.; Testa, G.; Vaccalluzzo, M.S.; Vescio, A.; Prestianni, I.; Lucenti, L.; de Cristo, C.; Sapienza, M.; Pavone, V. Clinical and Radiographic Outcomes and Treatment Algorithm for Septic Arthritis in Children. J. Pers. Med. 2023, 13, 1097. https://doi.org/10.3390/jpm13071097
Caldaci A, Testa G, Vaccalluzzo MS, Vescio A, Prestianni I, Lucenti L, de Cristo C, Sapienza M, Pavone V. Clinical and Radiographic Outcomes and Treatment Algorithm for Septic Arthritis in Children. Journal of Personalized Medicine. 2023; 13(7):1097. https://doi.org/10.3390/jpm13071097
Chicago/Turabian StyleCaldaci, Alessia, Gianluca Testa, Marco Simone Vaccalluzzo, Andrea Vescio, Ignazio Prestianni, Ludovico Lucenti, Claudia de Cristo, Marco Sapienza, and Vito Pavone. 2023. "Clinical and Radiographic Outcomes and Treatment Algorithm for Septic Arthritis in Children" Journal of Personalized Medicine 13, no. 7: 1097. https://doi.org/10.3390/jpm13071097