
Development and Validation of Risk Prediction Models for Colorectal Cancer in Patients with Symptoms
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studies and Variables
2.2. Descriptive and Association Analysis
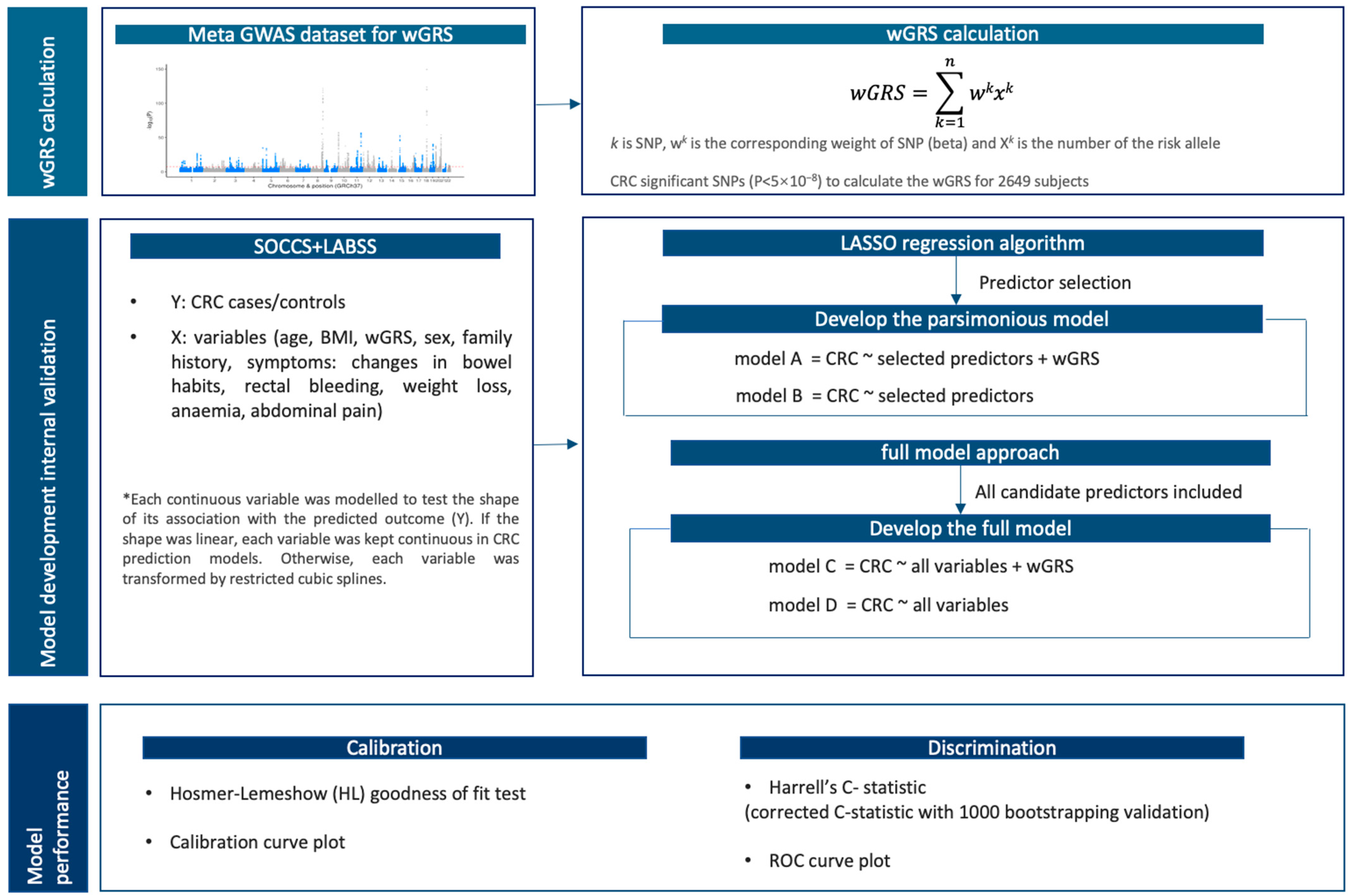
2.3. Weighted Genetic Risk Scores
2.4. Model Development and Internal Validation
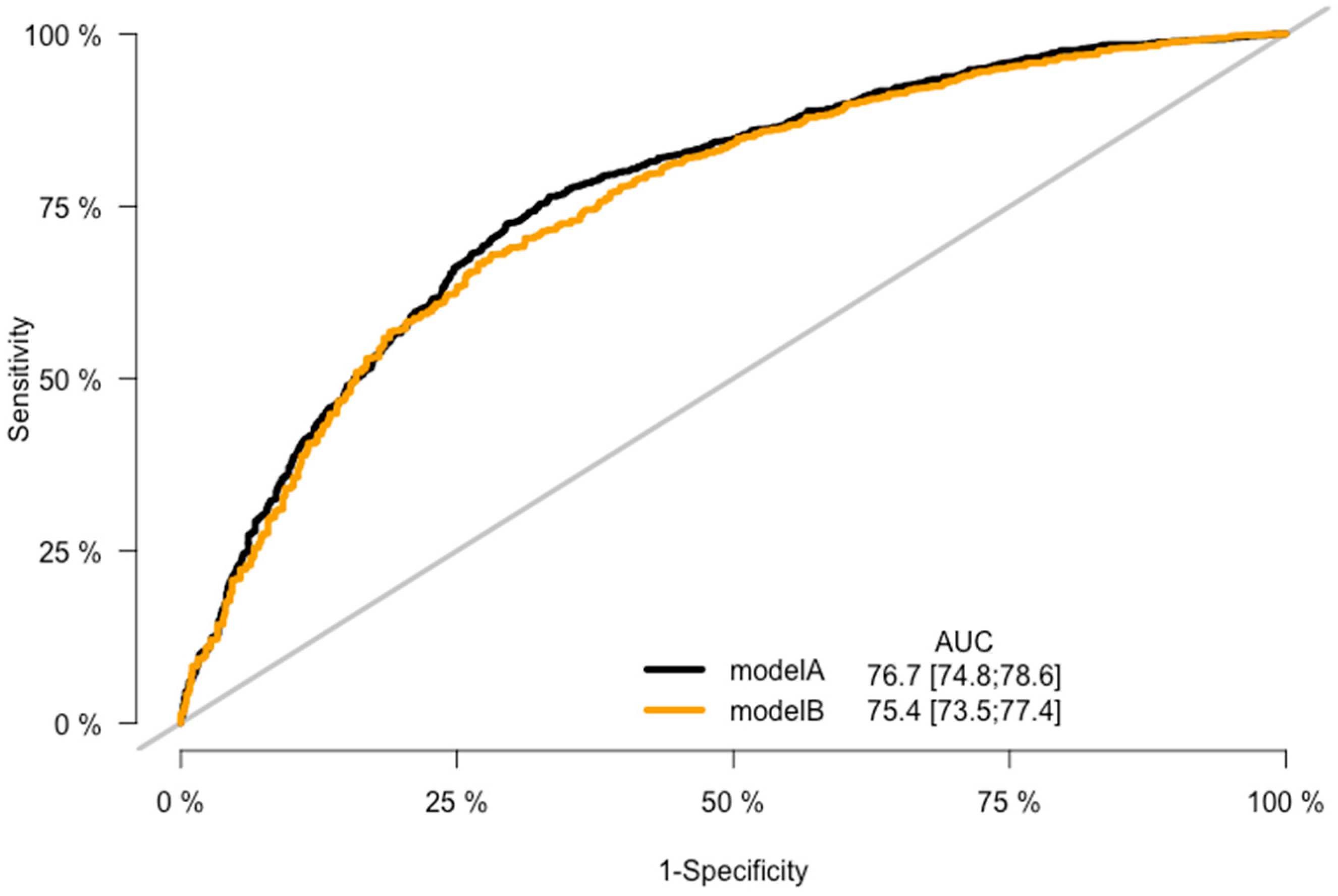
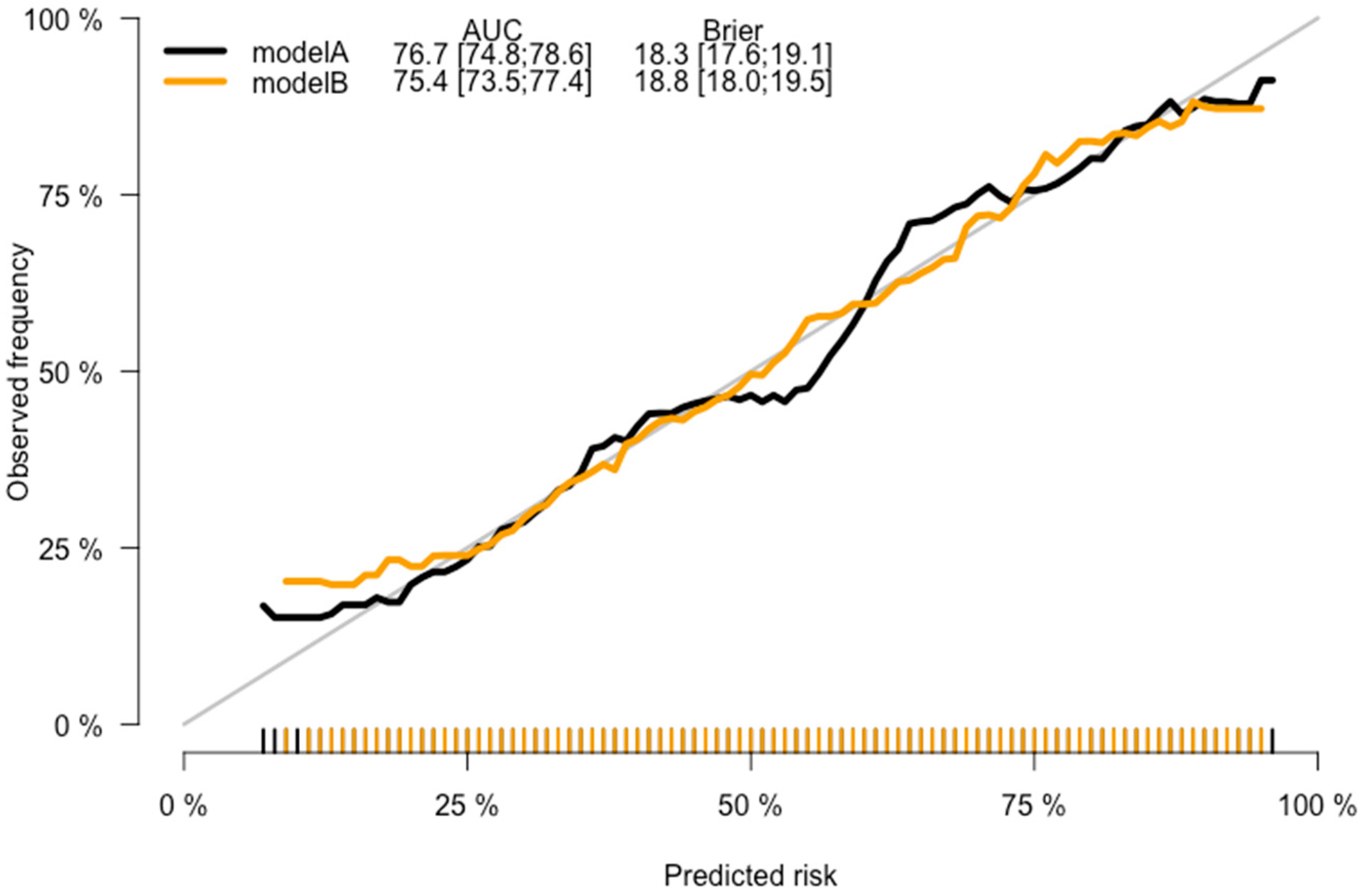
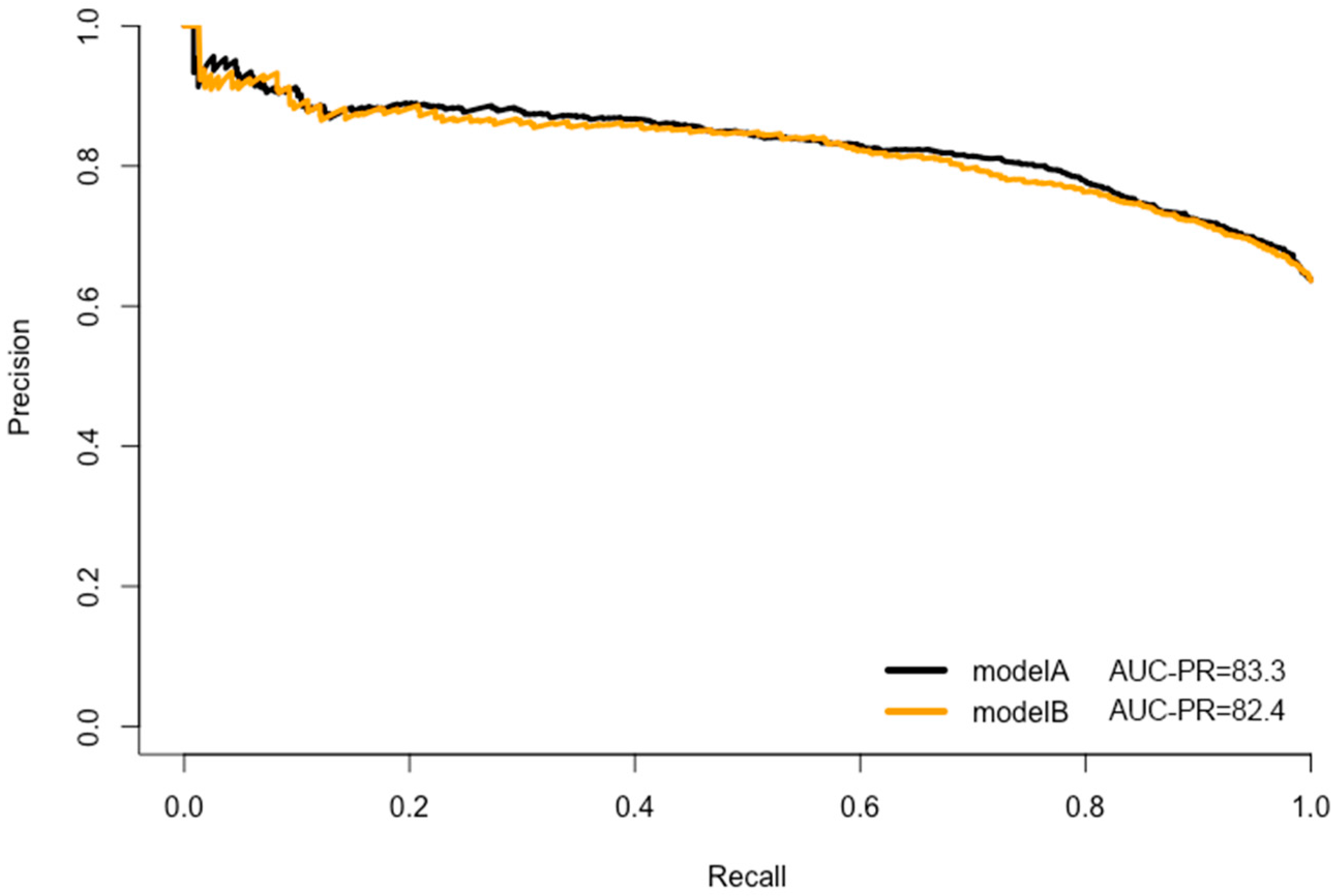
2.5. Model Prediction Performance
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Prediction Models of CRC Risk in Patients with Symptoms
3.2.1. Continuous Variables Adjustment
3.2.2. Models’ Development and Validation
4. Discussion
4.1. Interpretation of Main Findings
4.1.1. Model Predictors
4.1.2. Model Prediction Performance, Validation, and Clinical Impact
4.2. Strengths and Limitations
4.3. Clinical Implications and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cardoso, R.; Guo, F.; Heisser, T.; De Schutter, H.; Van Damme, N.; Nilbert, M.C.; Christensen, J.; Bouvier, A.-M.; Bouvier, V.; Launoy, G.; et al. Overall and stage-specific survival of patients with screen-detected colorectal cancer in European countries: A population-based study in 9 countries. Lancet Reg. Health—Eur. 2022, 21, 100458. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, D.; McMillan, D.C.; Crearie, C.; Morrison, D.S.; Crighton, E.M.; Horgan, P.G. Temporal trends in mode, site and stage of presentation with the introduction of colorectal cancer screening: A decade of experience from the West of Scotland. Br. J. Cancer 2015, 113, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Shipe, M.E.; Deppen, S.A.; Farjah, F.; Grogan, E.L. Developing prediction models for clinical use using logistic regression: An overview. J. Thorac. Dis. 2019, 11, S574–S584. [Google Scholar] [CrossRef]
- Adelstein, B.-A.; Irwig, L.; Macaskill, P.; Turner, R.M.; Chan, S.F.; Katelaris, P.H. Who needs colonoscopy to identify colorectal cancer? Bowel symptoms do not add substantially to age and other medical history. Aliment. Pharmacol. Ther. 2010, 32, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Adelstein, B.-A.; Macaskill, P.; Turner, R.M.; Katelaris, P.H.; Irwig, L. The value of age and medical history for predicting colorectal cancer and adenomas in people referred for colonoscopy. BMC Gastroenterol. 2011, 11, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alatise, O.I.; Ayandipo, O.O.; Adeyeye, A.; Seier, K.; Komolafe, A.O.; Bojuwoye, M.O.; Afuwape, O.O.; Zauber, A.; Omisore, A.; Olatoke, S.; et al. A symptom-based model to predict colorectal cancer in low-resource countries: Results from a prospective study of patients at high risk for colorectal cancer. Cancer 2018, 124, 2766–2773. [Google Scholar] [CrossRef]
- Bjerregaard, N.C.; Tøttrup, A.; Sørensen, H.T.; Laurberg, S. Diagnostic value of self-reported symptoms in Danish outpatients referred with symptoms consistent with colorectal cancer. Color. Dis. 2007, 9, 443–451. [Google Scholar] [CrossRef]
- Chen, C.; Tsai, M.; Wen, C. A user-friendly objective prediction model in predicting colorectal cancer based on 234 044 Asian adults in a prospective cohort. ESMO Open 2021, 6, 100288. [Google Scholar] [CrossRef]
- Collins, G.S.; Altman, D.G. Identifying patients with undetected colorectal cancer: An independent validation of QCancer (Colorectal). Br. J. Cancer 2012, 107, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Cubiella, J.; on behalf of the COLONPREDICT study investigators; Vega, P.; Salve, M.; Díaz-Ondina, M.; Alves, M.T.; Quintero, E.; Álvarez-Sánchez, V.; Fernández-Bañares, F.; Boadas, J.; et al. Development and external validation of a faecal immunochemical test-based prediction model for colorectal cancer detection in symptomatic patients. BMC Med. 2016, 14, 128. [Google Scholar] [CrossRef] [Green Version]
- Fijten, G.H.; Starmans, R.; Muris, J.W.; Schouten, H.J.; Blijham, G.H.; Knottnerus, J.A. Predictive value of signs and symptoms for colorectal cancer in patients with rectal bleeding in general practice. Fam. Pr. 1995, 12, 279–286. [Google Scholar] [CrossRef]
- Hamilton, W.; Lancashire, R.; Sharp, D.; Peters, T.J.; Cheng, K.; Marshall, T. The risk of colorectal cancer with symptoms at different ages and between the sexes: A case-control study. BMC Med. 2009, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, W.; Round, A.; Sharp, D.; Peters, T. Clinical features of colorectal cancer before diagnosis: A population-based case–control study. Br. J. Cancer 2005, 93, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Hippisley-Cox, J.; Coupland, C. Identifying patients with suspected colorectal cancer in primary care: Derivation and validation of an algorithm. Br. J. Gen. Pr. 2012, 62, e29–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, N.G.; Stocken, D.D.; Wilson, S.; Keh, C.; Wakelam, M.J.O.; Ismail, T. Elevated serum matrix metalloproteinase 9 (MMP-9) concentration predicts the presence of colorectal neoplasia in symptomatic patients. Br. J. Cancer 2007, 97, 971–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, D.T.-Y.; Choy, C.L.-Y.; Lam, S.C.-W.; Kwok, S.P.-Y. Age and symptoms as a triage method for per-rectal bleeding. Ann. Coll. Surg. Hong Kong 2002, 6, 77–82. [Google Scholar] [CrossRef]
- Li, W.; Zhao, L.-Z.; Ma, D.-W.; Wang, D.-Z.; Shi, L.; Wang, H.-L.; Dong, M.; Zhang, S.-Y.; Cao, L.; Zhang, W.-H.; et al. Predicting the risk for colorectal cancer with personal characteristics and fecal immunochemical test. Medicine 2018, 97, e0529. [Google Scholar] [CrossRef] [PubMed]
- Mahadavan, L.; Loktionov, A.; Daniels, I.R.; Shore, A.; Cotter, D.; Llewelyn, A.H.; Hamilton, W. Exfoliated colonocyte DNA levels and clinical features in the diagnosis of colorectal cancer: A cohort study in patients referred for investigation. Color. Dis. 2011, 14, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Marshall, T.; Lancashire, R.; Sharp, D.; Peters, T.J.; Cheng, K.K.; Hamilton, W. The diagnostic performance of scoring systems to identify symptomatic colorectal cancer compared to current referral guidance. Gut 2011, 60, 1242–1248. [Google Scholar] [CrossRef] [Green Version]
- Thompson, M.R.; Perera, R.; Senapati, A.; Dodds, S. Predictive value of common symptom combinations in diagnosing colorectal cancer. Br. J. Surg. 2007, 94, 1260–1265. [Google Scholar] [CrossRef]
- Selvachandran, S.; Hodder, R.; Ballal; Jones, P.; Cade, D. Prediction of colorectal cancer by a patient consultation questionnaire and scoring system: A prospective study. Lancet 2002, 360, 278–283. [Google Scholar] [CrossRef]
- Anderson, C.A.; Pettersson, F.H.; Clarke, G.M.; Cardon, L.R.; Morris, A.P.; Zondervan, K.T. Data quality control in genetic case-control association studies. Nat. Protoc. 2010, 5, 1564–1573. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Forer, L.; Schönherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-generation genotype imputation service and methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Rozadilla, C.; Timofeeva, M.; Chen, Z.; Law, P.; Thomas, M.; Schmit, S.; Díez-Obrero, V.; Hsu, L.; Fernandez-Tajes, J.; Palles, C.; et al. Deciphering colorectal cancer genetics through multi-omic analysis of 100,204 cases and 154,587 controls of European and east Asian ancestries. Nat. Genet. 2022, 55, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. Br. J. Surg. 2015, 102, 148–158. [Google Scholar] [CrossRef] [Green Version]
- Assel, M.; Sjoberg, D.D.; Vickers, A.J. The Brier score does not evaluate the clinical utility of diagnostic tests or prediction models. Diagn. Progn. Res. 2017, 1, 19. [Google Scholar] [CrossRef] [Green Version]
- Brewer, M.J.; Butler, A.; Cooksley, S.L. The relative performance of AIC, AICc and BIC in the presence of unobserved heterogeneity. Methods Ecol. Evol. 2016, 7, 679–692. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Vergouwe, Y.; Royston, P. Prognosis and prognostic research: Application and impact of prognostic models in clinical practice. BMJ 2009, 338, b606. [Google Scholar] [CrossRef]
- Breiman, L.; Friedman, J.; Olshen, R.; Stone, C. Classification and regression trees. Wadsworth Int. Group 1984, 37, 237–251. [Google Scholar]
- Speiser, J.L.; Miller, M.E.; Tooze, J.; Ip, E. A comparison of random forest variable selection methods for classification prediction modeling. Expert Syst. Appl. 2019, 134, 93–101. [Google Scholar] [CrossRef]
- Valavi, R.; Elith, J.; Lahoz-Monfort, J.J.; Guillera-Arroita, G. Modelling species presence-only data with random forests. Ecography 2021, 44, 1731–1742. [Google Scholar] [CrossRef]
- Cook, J.; Ramadas, V. When to consult precision-recall curves. Stata Journal Promot. Commun. Stat. Stata 2020, 20, 131–148. [Google Scholar] [CrossRef]
- Collignon, O.; Han, J.; An, H.; Oh, S.; Lee, Y. Comparison of the modified unbounded penalty and the LASSO to select predictive genes of response to chemotherapy in breast cancer. PLoS ONE 2018, 13, e0204897. [Google Scholar] [CrossRef]
- Kerr, K.F.; McClelland, R.L.; Brown, E.R.; Lumley, T. Evaluating the Incremental Value of New Biomarkers with Integrated Discrimination Improvement. Am. J. Epidemiol. 2011, 174, 364–374. [Google Scholar] [CrossRef] [Green Version]
- Gauthier, J.; Wu, Q.V.; Gooley, T.A. Cubic splines to model relationships between continuous variables and outcomes: A guide for clinicians. Bone Marrow Transplant. 2019, 55, 675–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adelstein, B.-A.; Macaskill, P.; Chan, S.F.; Katelaris, P.H.; Irwig, L. Most bowel cancer symptoms do not indicate colorectal cancer and polyps: A systematic review. BMC Gastroenterol. 2011, 11, 65. [Google Scholar] [CrossRef] [Green Version]
- Hull, M.A.; Rees, C.J.; Sharp, L.; Koo, S. A risk-stratified approach to colorectal cancer prevention and diagnosis. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Sassano, M.; Mariani, M.; Quaranta, G.; Pastorino, R.; Boccia, S. Polygenic risk prediction models for colorectal cancer: A systematic review. BMC Cancer 2022, 22, 65. [Google Scholar] [CrossRef]
- Lewis, C.M.; Vassos, E. Polygenic risk scores: From research tools to clinical instruments. Genome Med. 2020, 12, 44. [Google Scholar] [CrossRef]
- Wang, Y. Challenges and opportunities for developing more generalizable polygenic risk scores. Eur. Neuropsychopharmacol. 2022, 63, e311. [Google Scholar] [CrossRef]
- Martin, A.R.; Kanai, M.; Kamatani, Y.; Okada, Y.; Neale, B.M.; Daly, M.J. Current clinical use of polygenic scores will risk exacerbating health disparities. Nat. Genet. 2019, 51, 584. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.; Welter, D.; Bowler, E.H.; Cerezo, M.; Harris, L.W.; McMahon, A.C.; Hall, P.; Junkins, H.A.; Milano, A.; Hastings, E.; et al. A standardized framework for representation of ancestry data in genomics studies, with application to the NHGRI-EBI GWAS Catalog. Genome Biol. 2018, 19, 21. [Google Scholar] [CrossRef]
- Vassos, E.; Di Forti, M.; Coleman, J.; Iyegbe, C.; Prata, D.; Euesden, J.; O’reilly, P.; Curtis, C.; Kolliakou, A.; Patel, H.; et al. An Examination of Polygenic Score Risk Prediction in Individuals with First-Episode Psychosis. Biol. Psychiatry 2016, 81, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Torkamani, A.; Wineinger, N.E.; Topol, E.J. The personal and clinical utility of polygenic risk scores. Nat. Rev. Genet. 2018, 19, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Pavlou, M.; Ambler, G.; Seaman, S.; De Iorio, M.; Omar, R.Z. Review and evaluation of penalised regression methods for risk prediction in low-dimensional data with few events. Stat. Med. 2015, 35, 1159–1177. [Google Scholar] [CrossRef] [Green Version]
- Vandekerckhove, J.; Matzke, D.; Wagenmakers, E.-J. Model Comparison and the Principle of Parsimony; Oxford Handbooks Online; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Boughanem, H.; Canudas, S.; Hernandez-Alonso, P.; Becerra-Tomás, N.; Babio, N.; Salas-Salvadó, J.; Macias-Gonzalez, M. Vitamin D Intake and the Risk of Colorectal Cancer: An Updated Meta-Analysis and Systematic Review of Case-Control and Prospective Cohort Studies. Cancers 2021, 13, 2814. [Google Scholar] [CrossRef]
- Monahan, K.J.; Davies, M.M.; Abulafi, M.; Banerjea, A.; Nicholson, B.D.; Arasaradnam, R.; Barker, N.; Benton, S.; Booth, R.; Burling, D.; et al. Faecal immunochemical testing (FIT) in patients with signs or symptoms of suspected colorectal cancer (CRC): A joint guideline from the Association of Coloproctology of Great Britain and Ireland (ACPGBI) and the British Society of Gastroenterology (BSG). Gut 2022, 71, 1939–1962. [Google Scholar] [CrossRef]
- Gurdasani, D.; Barroso, I.; Zeggini, E.; Sandhu, M.S. Genomics of disease risk in globally diverse populations. Nat. Rev. Genet. 2019, 20, 520–535. [Google Scholar] [CrossRef]
- Mo, S.; Zhou, Z.; Dai, W.; Xiang, W.; Han, L.; Zhang, L.; Wang, R.; Cai, S.; Li, Q.; Cai, G. Development and external validation of a predictive scoring system associated with metastasis of T1-2 colorectal tumors to lymph nodes. Clin. Transl. Med. 2020, 10, 275–287. [Google Scholar] [CrossRef]
- McKeigue, P. Quantifying performance of a diagnostic test as the expected information for discrimination: Relation to the C-statistic. Stat. Methods Med. Res. 2018, 28, 1841–1851. [Google Scholar] [CrossRef] [Green Version]
- Nattino, G.; Pennell, M.L.; Lemeshow, S. Assessing the goodness of fit of logistic regression models in large samples: A modification of the Hosmer-Lemeshow test. Biometrics 2020, 76, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.J.; Poppe, K.K. Validation of clinical prediction models: What does the “Calibration Slope” really measure? J. Clin. Epidemiol. 2020, 118, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Verma, M. Personalized Medicine and Cancer. J. Pers. Med. 2012, 2, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, P.P.-C.; Glance, D.; Walker, J.; Walter, F.M.; Emery, J.D. Implementing a QCancer risk tool into general practice consultations: An exploratory study using simulated consultations with Australian general practitioners. Br. J. Cancer 2015, 112, S77–S83. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.G.; Crecrc; Bickerstaffe, A.; Hewabandu, N.; Maddumarachchi, S.; Dowty, J.G.; Jenkins, M.; Pirotta, M.; Walter, F.M.; Emery, J.D. The CRISP colorectal cancer risk prediction tool: An exploratory study using simulated consultations in Australian primary care. BMC Med. Inform. Decis. Mak. 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SOCCS + LABSS (N = 2649) | Univariable Analysis | Multivariable Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cases (n = 1686) | Controls (n = 963) | Total (N = 2649) | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| wGRS202 † | 0.11 (−0.19–0.42) | −0.03 (−0.34–0.26) | 0.06 (−0.24–0.37) | 3.36 × 10−16 | 2.14 | 1.77–2.58 | 1.88 × 10−15 | 2.14 | 1.74–2.64 | 5.52 × 10−13 |
| Age † | 68.01 (59.32–75.36) | 60.00 (51.00–70.00) | 65.42 (56.00–73.50) | <2.2 × 10−16 | 1.05 | 1.04–1.05 | 3.61 × 10−42 | 1.04 | 1.03–1.05 | 1.43 × 10−28 |
| Sex | ||||||||||
| Female | 730 (43.30%) | 537 (55.76%) | 1267 (47.83%) | 8.38 × 10−10 | 1 * | 1 * | ||||
| Male | 956 (56.70%) | 426 (44.24%) | 1382 (52.17%) | 1.65 | 1.41–1.94 | 7.35 × 10−10 | 1.44 | 1.20–1.72 | 7.11 × 10−5 | |
| BMI † | 26.11 (23.39–29.91) | 26.64 (23.50–30.47) | 26.35 (23.44–30.11) | 0.017 | 0.98 | 0.97–1.00 | 0.016 | 0.98 | 0.97–1.00 | 0.019 |
| Family history | ||||||||||
| No | 1418 (84.10%) | 801 (83.18%) | 2219 (83.77%) | 0.570 | 1 * | |||||
| Yes | 268 (15.90%) | 162 (16.82%) | 430 (16.23%) | 0.93 | 0.75–1.16 | 0.534 | ||||
| Symptoms | ||||||||||
| Changes in bowel habits | ||||||||||
| No | 971 (57.59%) | 242 (25.13%) | 1213 (45.79%) | <2.2 × 10−16 | 1 * | 1 * | ||||
| Yes | 715 (42.41%) | 721 (74.87%) | 1436 (54.21%) | 0.25 | 0.21–0.29 | 2.12 × 10−55 | 0.28 | 0.23–0.34 | 7.92 × 10−37 | |
| Rectal bleeding | ||||||||||
| No | 1130 (67.02%) | 622 (64.59%) | 1752 (66.14%) | 0.219 | 1 * | |||||
| Yes | 556 (32.98%) | 341 (35.41%) | 897 (33.86%) | 0.90 | 0.76–1.06 | 0.203 | ||||
| Weight loss | ||||||||||
| No | 1437 (85.23%) | 784 (81.41%) | 2221 (83.84%) | 0.012 | 1 * | 1 * | ||||
| Yes | 249 (14.77%) | 179 (18.59%) | 428 (16.16%) | 0.76 | 0.61–0.94 | 0.010 | 0.99 | 0.78–1.26 | 0.910 | |
| Anaemia | ||||||||||
| No | 1293 (76.69%) | 821 (85.25%) | 2114 (79.80%) | 1.69 × 10−07 | 1 * | 1 * | ||||
| Yes | 393 (23.31%) | 142 (14.75%) | 535 (20.20%) | 1.76 | 1.42–2.17 | 1.61 × 10−07 | 0.94 | 0.73–1.20 | 0.619 | |
| Abdominal pain | ||||||||||
| No | 1354 (80.31%) | 540 (56.07%) | 1894 (71.50%) | <2.2 × 10−16 | 1 * | 1 * | ||||
| Yes | 332 (19.69%) | 423 (43.93%) | 755 (28.50%) | 0.31 | 0.26–0.37 | 1.03 × 10−38 | 0.51 | 0.42–0.61 | 8.48 × 10−12 | |
| Model | Method | Case | Control | λ | Intercept | Predictors | Coefficient | OR (95% CI) | p-Value | R2 | Brier | AIC | BIC | C-Statistic | Corrected C-Statistic | AUC-PR | HL p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model A | LASSO | 1686 | 963 | 0.0257 | −1.3030 | wGRS202 | 0.7612 | 2.14 (1.74–2.64) | 5.31 × 10−13 | 0.266 | 0.183 | 2911.234 | 2946.526 | 0.767 (0.748–0.786) | 0.765 (1000 bootstrap) | 0.8325 | 0.024 |
| Age | 0.0410 | 1.04 (1.03–1.05) | 3.53 × 10−29 | ||||||||||||||
| Sex | 0.3611 | 1.43 (1.20–1.72) | 7.19 × 10−5 | ||||||||||||||
| Changes in bowel habits | −1.2411 | 0.29 (0.24–0.35) | 8.06 × 10−29 | ||||||||||||||
| Abdominal pain | −0.6784 | 0.51 (0.42–0.62) | 7.65 × 10−12 | ||||||||||||||
| Model B | LASSO | 1686 | 963 | 0.0310 | −1.2124 | Age | 0.0401 | 1.04 (1.03–1.05) | 1.06 × 10−28 | 0.244 | 0.188 | 2962.840 | 2992.25 | 0.754 (0.735–0.774) | 0.753 (1000 bootstrap) | 0.8243 | 0.711 |
| Sex | 0.3690 | 1.45 (1.21–1.73) | 4.09 × 10−5 | ||||||||||||||
| Changes in bowel habits | −1.2411 | 0.29 (0.24–0.35) | 1.34 × 10−39 | ||||||||||||||
| Abdominal pain | −0.7020 | 0.50 (0.41–0.60) | 7.77 × 10−13 | ||||||||||||||
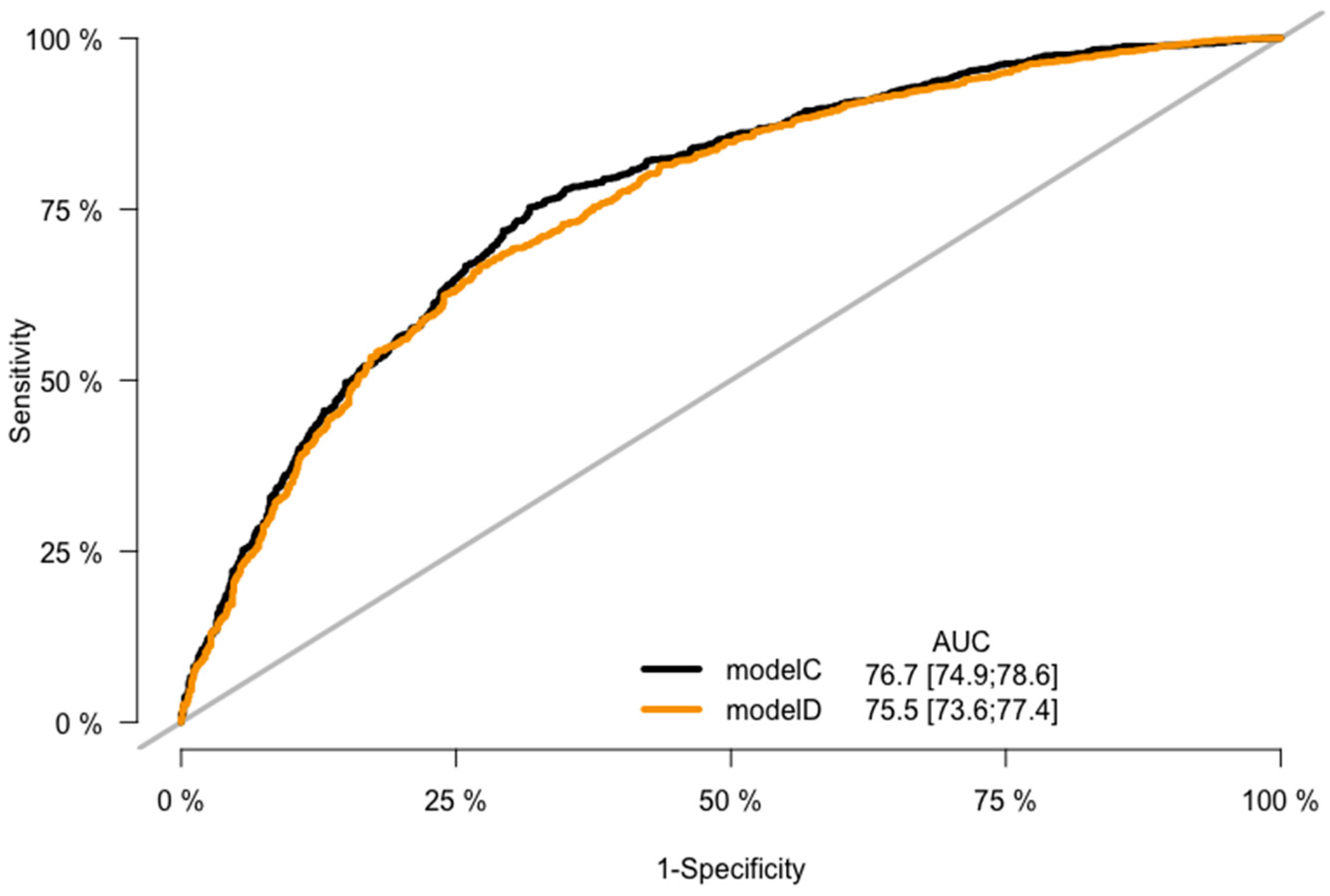
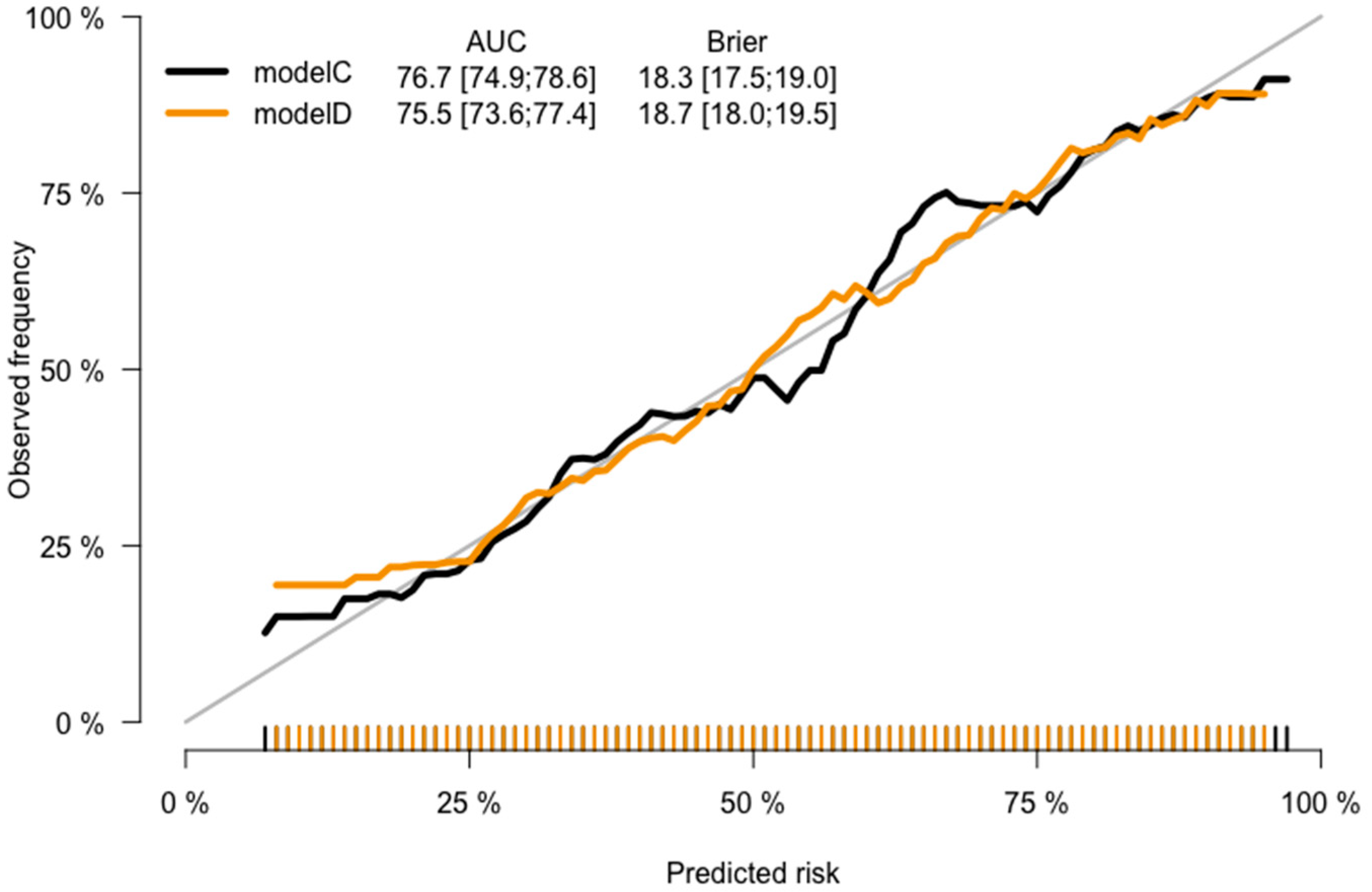
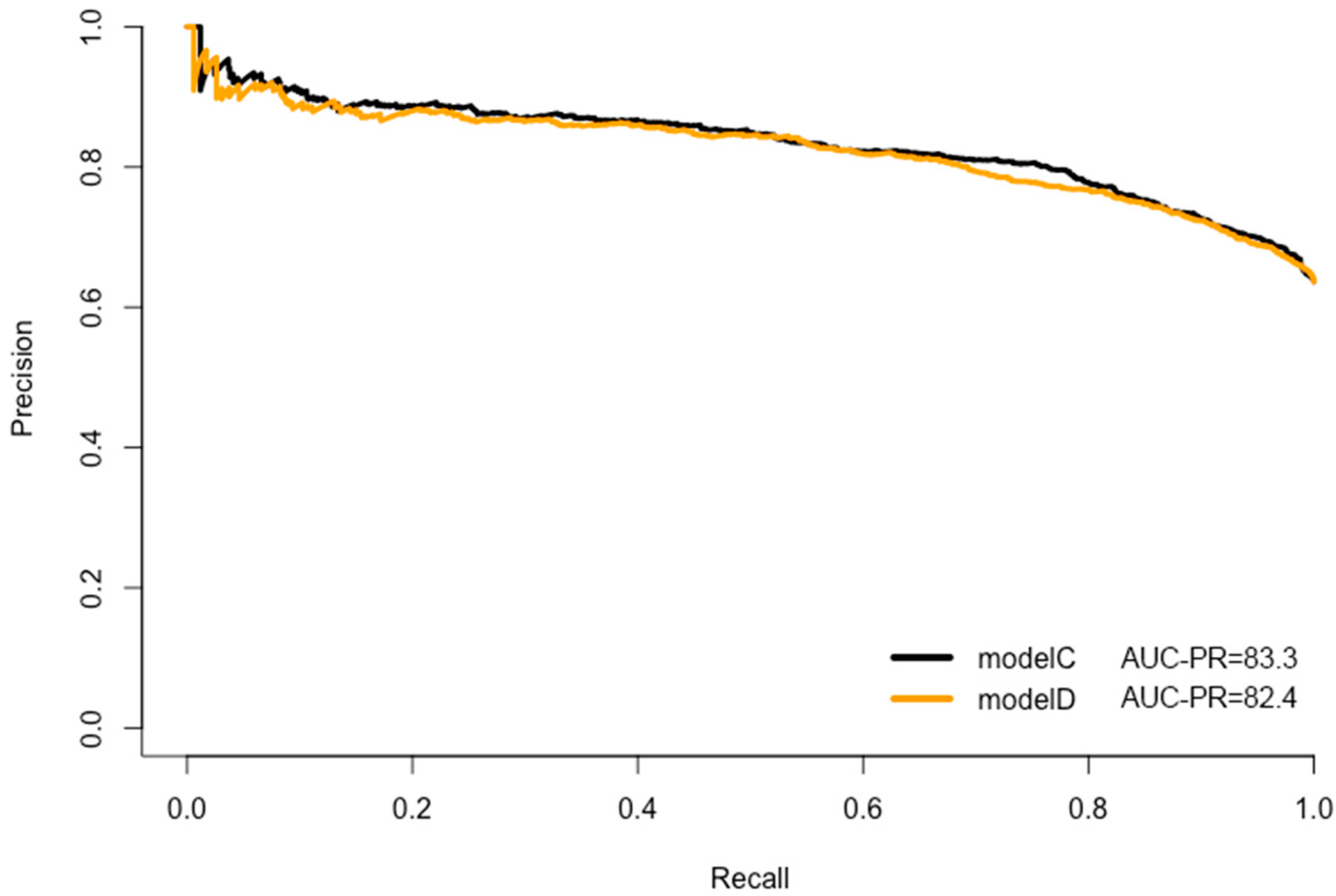
| Model C | Full model | 1686 | 963 | NA | −0.7679 | wGRS202 | 0.7603 | 2.14 (1.74–2.64) | 6.91 × 10−13 | 0.269 | 0.183 | 2915.181 | 2979.883 | 0.767 (0.749–0.786) | 0.764 (1000 bootstrap) | 0.8334 | 0.018 |
| Age | 0.0410 | 1.04 (1.03–1.05) | 2.65 × 10−28 | ||||||||||||||
| Sex | 0.3631 | 1.44 (1.20–1.72) | 7.05 × 10−5 | ||||||||||||||
| BMI | −0.0195 | 0.98 (0.96–1.00) | 0.0187 | ||||||||||||||
| Family history | −0.0024 | 1.00 (0.78–1.27) | 0.9846 | ||||||||||||||
| Changes in bowel habits | −1.2616 | 0.28 (0.23–0.34) | 7.68 × 10−37 | ||||||||||||||
| Rectal bleeding | 0.0402 | 1.04 (0.86–1.27) | 0.6858 | ||||||||||||||
| Weight loss | −0.0112 | 0.99 (0.78–1.26) | 0.9278 | ||||||||||||||
| Anaemia | −0.0531 | 0.95 (0.74–1.22) | 0.6785 | ||||||||||||||
| Abdominal pain | −0.6786 | 0.51 (0.42–0.63) | 1.55 × 10−11 | ||||||||||||||
| Model D | Full model | 1686 | 963 | NA | −0.7170 | Age | 0.0404 | 1.04 (1.03–1.05) | 4.12 × 10−28 | 0.247 | 0.187 | 2966.240 | 3025.059 | 0.755 (0.736–0.775) | 0.752 (1000 bootstrap) | 0.8240 | 0.428 |
| Sex | 0.3714 | 1.45 (1.21–1.73) | 3.94 × 10−5 | ||||||||||||||
| BMI | −0.0191 | 0.98 (0.97–1.00) | 0.0200 | ||||||||||||||
| Family history | −0.0349 | 1.04 (0.82–1.32) | 0.7738 | ||||||||||||||
| Changes in bowel habits | −1.2667 | 0.28 (0.23–0.34) | 7.07 × 10−38 | ||||||||||||||
| Rectal bleeding | 0.0734 | 1.08 (0.89–1.31) | 0.4553 | ||||||||||||||
| Weight loss | −0.0661 | 0.99 (0.78–1.27) | 0.9655 | ||||||||||||||
| Anaemia | −0.6999 | 0.94 (0.73–1.20) | 0.6021 | ||||||||||||||
| Abdominal pain | −0.6786 | 0.50 (0.41–0.60) | 2.03 × 10−12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, W.; Mesa-Eguiagaray, I.; Kirkpatrick, T.; Devlin, J.; Brogan, S.; Turner, P.; Macdonald, C.; Thornton, M.; Zhang, X.; He, Y.; et al. Development and Validation of Risk Prediction Models for Colorectal Cancer in Patients with Symptoms. J. Pers. Med. 2023, 13, 1065. https://doi.org/10.3390/jpm13071065
Xu W, Mesa-Eguiagaray I, Kirkpatrick T, Devlin J, Brogan S, Turner P, Macdonald C, Thornton M, Zhang X, He Y, et al. Development and Validation of Risk Prediction Models for Colorectal Cancer in Patients with Symptoms. Journal of Personalized Medicine. 2023; 13(7):1065. https://doi.org/10.3390/jpm13071065
Chicago/Turabian StyleXu, Wei, Ines Mesa-Eguiagaray, Theresa Kirkpatrick, Jennifer Devlin, Stephanie Brogan, Patricia Turner, Chloe Macdonald, Michelle Thornton, Xiaomeng Zhang, Yazhou He, and et al. 2023. "Development and Validation of Risk Prediction Models for Colorectal Cancer in Patients with Symptoms" Journal of Personalized Medicine 13, no. 7: 1065. https://doi.org/10.3390/jpm13071065