
Arterial Blood Gas Analysis for Survival Prediction in Pediatric Patients with Out-of-Hospital Cardiac Arrest
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Variables
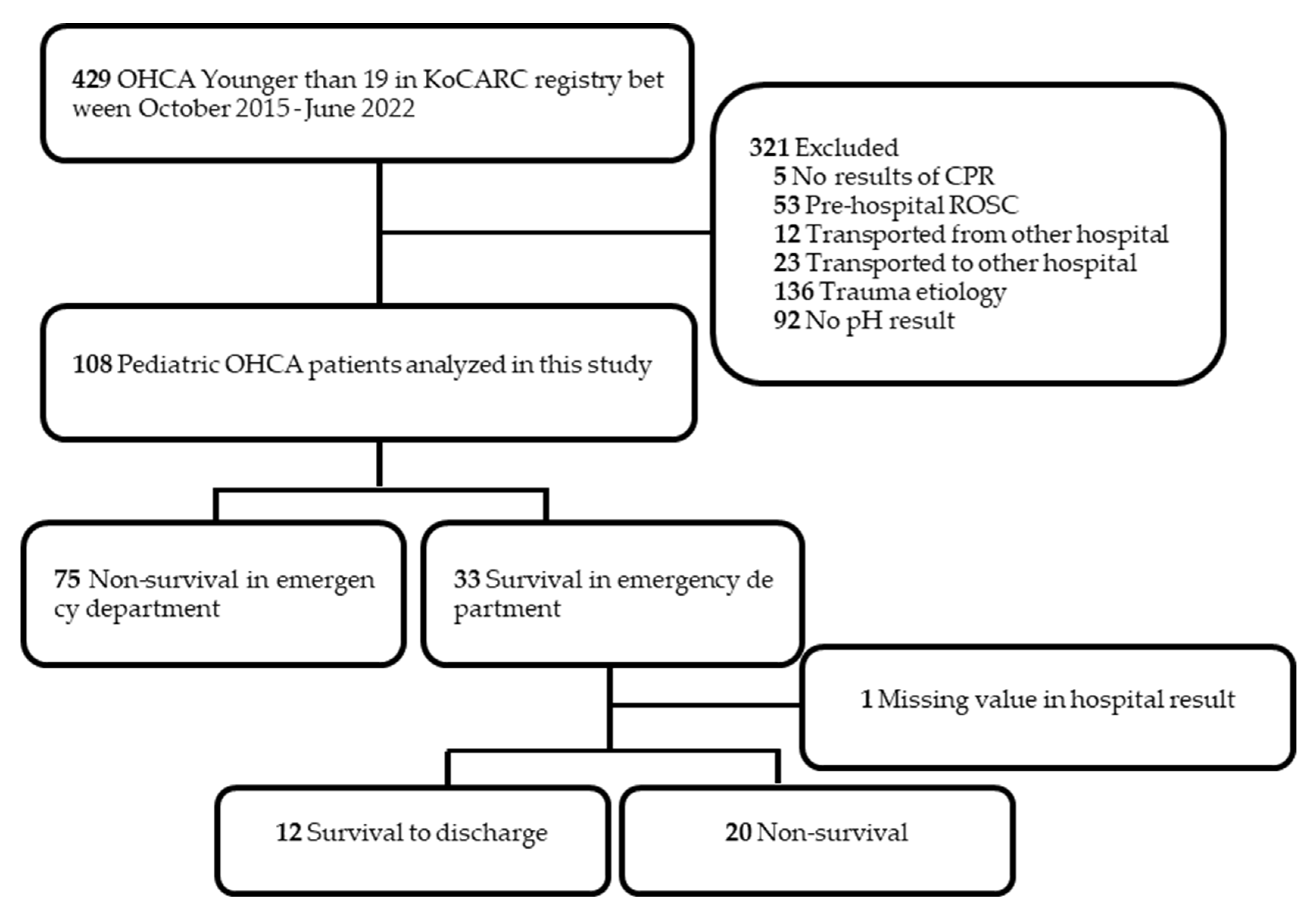
2.2. Participants
2.3. Outcome Variables
2.4. Statistical Analysis
3. Results
3.1. ABGA Result for Prediction of Survival to Hospital Admission
3.2. ABGA Result for Prediction of Survival to Discharge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.Y.; Lee, M.J.; Kim, H.; Yoon, H.D.; Jang, H.Y. Epidemiological and Survival Trends of Pediatric Cardiac Arrests in Emergency Departments in Korea: A Cross-sectional, Nationwide Report. J. Korean Med. Sci. 2015, 30, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, M.J.; Wiberg, S.; Ross, C.E.; Kleinman, M.; Hoeyer-Nielsen, A.K.; Donnino, M.W.; Andersen, L.W. For the American Heart Association’s Get with the Guidelines-Resuscitation Investigators Trends in Survival after Pediatric In-Hospital Cardiac Arrest in the United States. Circulation 2019, 140, 1398–1408. [Google Scholar] [CrossRef] [PubMed]
- Prause, G.; Ratzenhofer-Comenda, B.; Smolle-Jüttner, F.; Heydar-Fadai, J.; Wildner, G.; Spernbauer, P.; Smolle, J.; Hetz, H. Comparison of lactate or BE during out-of-hospital cardiac arrest to determine metabolic acidosis. Resuscitation 2001, 51, 297–300. [Google Scholar] [CrossRef]
- Takasu, A.; Sakamoto, T.; Okada, Y. Arterial base excess after CPR: The relationship to CPR duration and the characteristics related to outcome. Resuscitation 2007, 73, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Topjian, A.A.; Raymond, T.T.; Atkins, D.; Chan, M.; Duff, J.P.; Joyner, B.L., Jr.; Lasa, J.J.; Lavonas, E.J.; Levy, A.; Mahgoub, M.; et al. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S469–S523. [Google Scholar] [CrossRef]
- Topjian, A.A.; Clark, A.E.; Casper, T.C.; Berger, J.T.; Schleien, C.L.; Dean, J.M.; Moler, F.W. Early Lactate Elevations following Resuscitation from Pediatric Cardiac Arrest Are Associated with Increased Mortality. Pediatr. Crit. Care Med. 2013, 14, e380–e387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.H.; Kim, D.K.; Kang, E.K.; Kim, J.-T.; Na, J.Y.; Park, B.; Yeom, S.R.; Oh, J.S.; Lee, J.; Jhang, W.K.; et al. 2020 Korean Guidelines for Cardiopulmonary Resuscitation. Part 7. Pediatric advanced life support. Clin. Exp. Emerg. Med. 2021, 8, S81–S95. [Google Scholar] [CrossRef]
- Puri, S.; Paul, G.; Sood, P. Interpretation of arterial blood gas. Indian J. Crit. Care Med. 2010, 14, 57–64. [Google Scholar] [CrossRef]
- Kiehl, E.L.; Amuthan, R.; Adams, M.P.; Love, T.E.; Enfield, K.B.; Gimple, L.W.; Cantillon, D.J.; Menon, V. Initial arterial pH as a predictor of neurologic outcome after out-of-hospital cardiac arrest: A propensity-adjusted analysis. Resuscitation 2019, 139, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.-I.; Kim, J.-S.; Kim, Y.-J.; Kim, W.Y. Dynamic changes in arterial blood gas during cardiopulmonary resuscitation in out-of-hospital cardiac arrest. Sci. Rep. 2021, 11, 23165. [Google Scholar] [CrossRef]
- Issa, M.S.; Grossestreuer, A.V.; Patel, H.; Ntshinga, L.; Coker, A.; Yankama, T.; Donnino, M.W.; Berg, K.M. Lactate and hypotension as predictors of mortality after in-hospital cardiac arrest. Resuscitation 2021, 158, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Lee, Y.J.; Ryoo, S.M.; Sohn, C.H.; Ahn, S.; Seo, D.-W.; Lim, K.S.; Kim, W.Y. Role of blood gas analysis during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients. Medicine 2016, 95, e3960. [Google Scholar] [CrossRef]
- Spindelboeck, W.; Schindler, O.; Moser, A.; Hausler, F.; Wallner, S.; Strasser, C.; Haas, J.; Gemes, G.; Prause, G. Increasing arterial oxygen partial pressure during cardiopulmonary resuscitation is associated with improved rates of hospital admission. Resuscitation 2013, 84, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Hwang, S.O.; Shin, S.D.; Yang, H.J.; Chung, S.P.; Lee, S.W.; Song, K.J.; Hwang, S.S.; Cho, G.C.; Moon, S.W.; et al. Korean Cardiac Arrest Research Consortium (KoCARC): Rationale, development, and implementation. Clin. Exp. Emerg. Med. 2018, 5, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; De Caen, A.R.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation 2015, 132, 1286–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef]
- Spindelboeck, W.; Gemes, G.; Strasser, C.; Toescher, K.; Kores, B.; Metnitz, P.; Haas, J.; Prause, G. Arterial blood gases during and their dynamic changes after cardiopulmonary resuscitation: A prospective clinical study. Resuscitation 2016, 106, 24–29. [Google Scholar] [CrossRef]
- Shin, J.; Lim, Y.S.; Kim, K.; Lee, H.J.; Lee, S.J.; Jung, E.; You, K.M.; Yang, H.J.; Kim, J.J.; Kim, J.; et al. Initial blood pH during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients: A multicenter observational registry-based study. Crit. Care 2017, 21, 322. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.; Cha, K.-C.; Lee, J.-H.; Park, S.; Kim, D.-H.; Lee, B.K.; Park, J.S.; Jung, W.J.; Lee, D.K.; Roh, Y.I.; et al. 2020 Korean Guidelines for Cardiopulmonary Resuscitation. Part 4. Adult advanced life support. Clin. Exp. Emerg. Med. 2021, 8, S26–S40. [Google Scholar] [CrossRef] [PubMed]
- Okada, A.; Okada, Y.; Kandori, K.; Nakajima, S.; Okada, N.; Matsuyama, T.; Kitamura, T.; Hiromichi, N.; Iiduka, R. Associations between initial serum pH value and outcomes of pediatric out-of-hospital cardiac arrest. Am. J. Emerg. Med. 2021, 40, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Ohashi-Fukuda, N.; Fukuda, T.; Doi, K.; Morimura, N. Effect of prehospital advanced airway management for pediatric out-of-hospital cardiac arrest. Resuscitation 2017, 114, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Kraut, J.A.; Madias, N.E. Lactic Acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Sarıaydın, T.; Çorbacıoğlu, K.; Çevik, Y.; Emektar, E. Effect of initial lactate level on short-term survival in patients with out-of-hospital cardiac arrest. Turk. J. Emerg. Med. 2017, 17, 123–127. [Google Scholar] [CrossRef]
- Nishioka, N.; Kobayashi, D.; Izawa, J.; Irisawa, T.; Yamada, T.; Yoshiya, K.; Park, C.; Nishimura, T.; Ishibe, T.; Yagi, Y.; et al. Association between serum lactate level during cardiopulmonary resuscitation and survival in adult out-of-hospital cardiac arrest: A multicenter cohort study. Sci. Rep. 2021, 11, 1639. [Google Scholar] [CrossRef]
- Moler, F.W.; Donaldson, A.E.; Meert, K.; Brilli, R.J.; Nadkarni, V.; Shaffner, D.H.; Schleien, C.L.; Clark, R.S.B.; Dalton, H.J.; Statler, K.; et al. Multicenter cohort study of out-of-hospital pediatric cardiac arrest. Crit. Care Med. 2011, 39, 141–149. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Survival to Hospital Admission | * p-Value | ||
|---|---|---|---|
| Survival (n = 33) | Non-Survival (n = 75) | ||
| Age (years) | 0.0 [0.0; 6.0] | 2.0 [0.0; 12.0] | 0.146 |
| Age category | 0.595 | ||
| <1 month | 3 (9.1%) | 3 (4.0%) | |
| 1 to 12 months | 13 (39.4%) | 24 (32.0%) | |
| 1 to 4 years | 7 (21.2%) | 14 (18.7%) | |
| 5 to 12 years | 5 (15.2%) | 17 (22.7%) | |
| 13 to 18 years | 5 (15.2%) | 17 (22.7%) | |
| Sex(male), n (%) | 21 (63.6%) | 44 (58.7%) | 0.785 |
| Comorbidities, n (%) | 9 (27.3%) | 40 (53.3%) | 0.022 * |
| Comorbidities | 0.126 | ||
| Lung or airway | 2 (22.2%) | 2 (5.0%) | |
| Neurologic | 2 (22.2%) | 18 (45.0%) | |
| Congenital heart disease | 4 (44.4%) | 6 (15.0%) | |
| Genetic or metabolic | 1 (11.1%) | 6 (15.0%) | |
| Hematology or oncology | 0 (0.0%) | 3 (7.5%) | |
| Others or unknown † | 0 (0.0%) | 5 (12.5%) | |
| Witnessed arrest, n (%) | 20 (60.6%) | 36 (48.0%) | 0.318 |
| Bystander CPR, n (%) | 23 (69.7%) | 47 (62.7%) | 0.627 |
| Prehospital advanced airway management, n (%) | 13 (39.4%) | 24 (32.0%) | 0.599 |
| First monitored ECG, shockable (%) | 3 (90.9%) | 4 (5.3%) | 0.759 |
| ABGA results | |||
| pH | 6.78 ± 0.18 | 6.70 ± 0.23 | 0.074 |
| PaCO2, mmHg †† | 84.34 ± 32.86 | 99.80 ± 43.78 | 0.079 |
| PaO2, mmHg | 49.0 [29.90; 88.40] | 34.70 [19.80; 58.60] | 0.063 |
| Lactate, mmol/L †† | 14.66 ± 4.83 | 15.18 ± 5.15 | 0.687 |
| Odds Ratio | 95% CI | * p-Value | |
|---|---|---|---|
| (A) Univariable analysis | |||
| Age | 0.95 | 0.89–1.02 | 0.154 |
| Age category | |||
| <1 month | Ref. | ||
| 1 to 12 months | 0.54 | 0.10–3.08 | 0.489 |
| 1 to 4 years | 0.50 | 0.08–3.14 | 0.460 |
| 5 to 12 years | 0.29 | 0.04–1.94 | 0.203 |
| 13 to 18 years | 0.29 | 0.04–1.94 | 0.203 |
| Sex (Female) | 0.81 | 0.35–1.89 | 0.627 |
| Comorbidities (No) | 3.05 | 1.25–7.42 | 0.014 * |
| Witnessed arrest (Yes) | 1.67 | 0.73–3.83 | 0.229 |
| Bystander CPR (Yes) | 1.37 | 0.57–3.30 | 0.482 |
| Prehospital advanced airway management (Yes) | 1.38 | 0.59–3.23 | 0.457 |
| First monitored ECG (Shockable) | 1.78 | 0.37–8.42 | 0.470 |
| pH > 6.795 | 2.13 | 0.93–4.90 | 0.074 |
| PaCO2 ≤ 95.750 (mmHg) † | 2.34 | 0.98–5.59 | 0.055 |
| PaO2 > 45.750 (mmHg) | 2.71 | 1.17–6.30 | 0.020 * |
| Lactate ≤ 16.600 (mmHg) † | 0.65 | 0.24–1.77 | 0.393 |
| Adjusted odds ratio | 95% CI | * p-Value | |
| (B) Multivariable analysis | |||
| Comorbidities (No) | 3.03 | 1.22–7.53 | 0.017 * |
| PaO2 > 45.750 (mmHg) | 2.69 | 1.13–6.42 | 0.026 * |
| Survival to Discharge | * p-Value | ||
|---|---|---|---|
| Survival (n = 12) | Non-Survival (n = 20) | ||
| Age (years) | 3.0 [0.0; 6.5] | 0.0 [0.0; 1.0] | 0.104 |
| Age category | 0.452 | ||
| <1 month | 1 (8.33%) | 2 (10.0%) | |
| 1 to 12 months | 3 (25.0%) | 10 (50.0%) | |
| 1 to 4 years | 3 (25.0%) | 4 (20.0%) | |
| 5 to 12 years | 3 (25.0%) | 1 (5.0%) | |
| 13 to 18 years | 2 (16.67%) | 3 (15.0%) | |
| Sex (male), n (%) | 9 (75.0%) | 11 (55.0%) | 0.451 |
| Comorbidities, n (%) | 5 (41.67%) | 4 (20.0%) | 0.361 |
| Comorbidities | 0.268 | ||
| Lung or airway | 2 (40.0%) | 0 (0.0%) | |
| Neurologic | 1 (20.0%) | 1 (25.0%) | |
| Congenital heart disease | 1 (20.0%) | 3 (75.0%) | |
| Genetic or metabolic | 1 (20.0%) | 0 (0.0%) | |
| Witnessed arrest | 8 (66.7%) | 11 (55.0%) | 0.780 |
| Bystander CPR | 8 (66.7%) | 15 (75.0%) | 0.919 |
| Prehospital advanced airway management, n (%) | 4 (33.33%) | 8 (40.00%) | 1.000 |
| First monitored ECG, shockable (%) | 3 (25.0%) | 0 (0.0%) | 0.085 |
| ABGA results | |||
| pH | 6.87 ± 0.15 | 6.73 ± 0.18 | 0.030 * |
| PaCO2, mmHg † | 75.07 ± 37.97 | 87.66 ± 29.57 | 0.314 |
| PaO2, mmHg | 48.6 [29.10; 87.20] | 48.35 [26.10; 106.25] | 0.938 |
| Lactate, mmol/L † | 15.56 ± 4.50 | 13.46 ± 5.03 | 0.320 |
| Odds Ratio | 95% CI | * p-Value | |
|---|---|---|---|
| (A) Univariable analysis | |||
| Age | 1.06 | 0.94–1.19 | 0.367 |
| Age category | |||
| <1 month | Ref | ||
| 1 to 12 months | 0.6 | 0.04–9.16 | 0.713 |
| 1 to 4 years | 1.5 | 0.09–25.39 | 0.779 |
| 5 to 12 years | 6.00 | 0.22–162.53 | 0.287 |
| 13 to 18 years | 1.33 | 0.07–26.62 | 0.851 |
| Sex (female) | 0.40 | 0.08–1.97 | 0.264 |
| Comorbidities (No) | 0.35 | 0.07–1.71 | 0.195 |
| Witnessed arrest (yes) | 1.64 | 0.37–7.25 | 0.517 |
| Bystander CPR (Yes) | 0.67 | 0.14–3.20 | 0.613 |
| Prehospital advanced airway management (Yes) | 0.75 | 0.17–3.35 | 0.706 |
| pH > 6.775 | 7.5 | 1.29–43.69 | 0.025 * |
| PaCO2 ≤ 66.500 (mmHg) † | 6.8 | 1.23–37.50 | 0.028 * |
| PaO2 > 47.850 (mmHg) | 1.40 | 0.33–5.93 | 0.648 |
| Lactate ≤ 14.865 (mmol/L) † | 0.31 | 0.05–1.80 | 0.191 |
| Adjusted odds ratio | 95% CI | p-Value | |
| (B) Multivariable analysis | |||
| pH > 6.775 | 4.15 | 0.62–27.97 | 0.144 |
| PaCO2 ≤ 66.500 (mmHg) | 3.99 | 0.63–25.23 | 0.141 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Shin, H.; Cho, Y.; Oh, J.; Choi, H.-J.; The Korean Cardiac Arrest Research Consortium (KoCARC) Investigators. Arterial Blood Gas Analysis for Survival Prediction in Pediatric Patients with Out-of-Hospital Cardiac Arrest. J. Pers. Med. 2023, 13, 1061. https://doi.org/10.3390/jpm13071061
Lee S-H, Shin H, Cho Y, Oh J, Choi H-J, The Korean Cardiac Arrest Research Consortium (KoCARC) Investigators. Arterial Blood Gas Analysis for Survival Prediction in Pediatric Patients with Out-of-Hospital Cardiac Arrest. Journal of Personalized Medicine. 2023; 13(7):1061. https://doi.org/10.3390/jpm13071061
Chicago/Turabian StyleLee, Sang-Hwan, Hyungoo Shin, Yongil Cho, Jaehoon Oh, Hyuk-Joong Choi, and The Korean Cardiac Arrest Research Consortium (KoCARC) Investigators. 2023. "Arterial Blood Gas Analysis for Survival Prediction in Pediatric Patients with Out-of-Hospital Cardiac Arrest" Journal of Personalized Medicine 13, no. 7: 1061. https://doi.org/10.3390/jpm13071061