
Previous Lumbar Spine Surgery Decreases the Therapeutic Efficacy of Dorsal Root Ganglion Pulsed Radiofrequency in Patients with Chronic Lumbosacral Radicular Pain
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
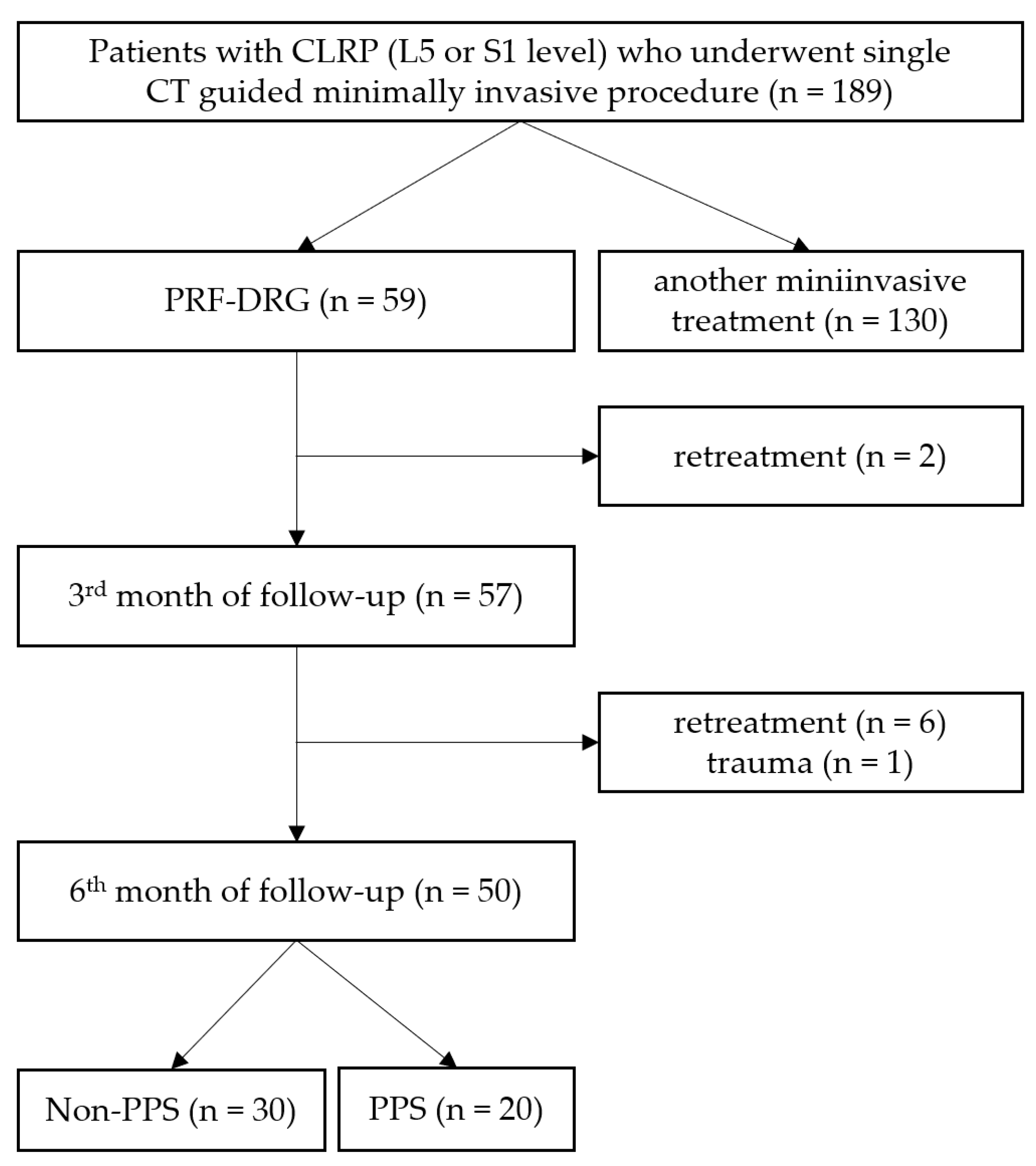
2.1. Study Design and Patient Selection
2.2. Settings and Equipment
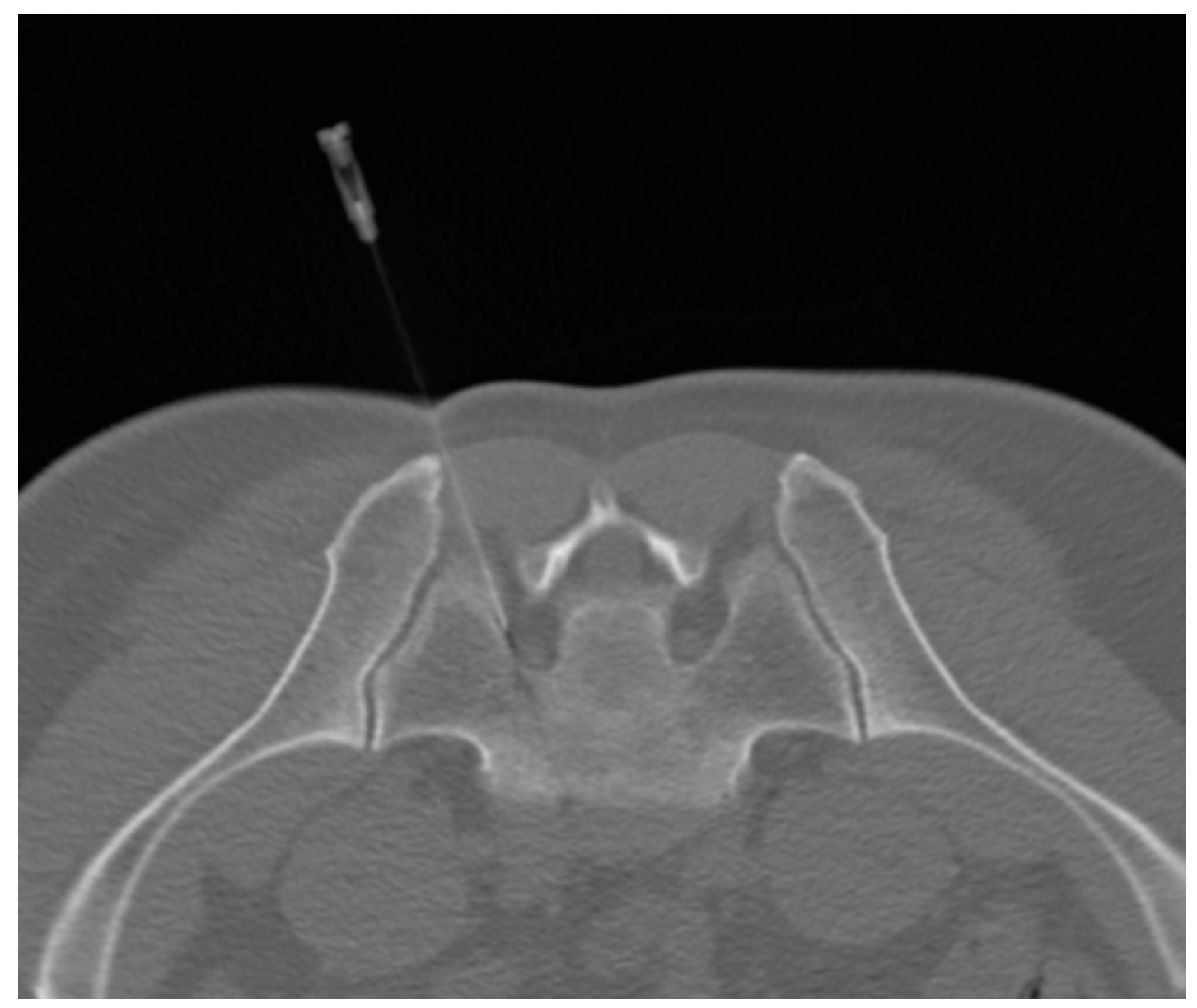
2.3. PRF–DRG Procedure
2.4. Outcome Evaluation
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Outcome Data
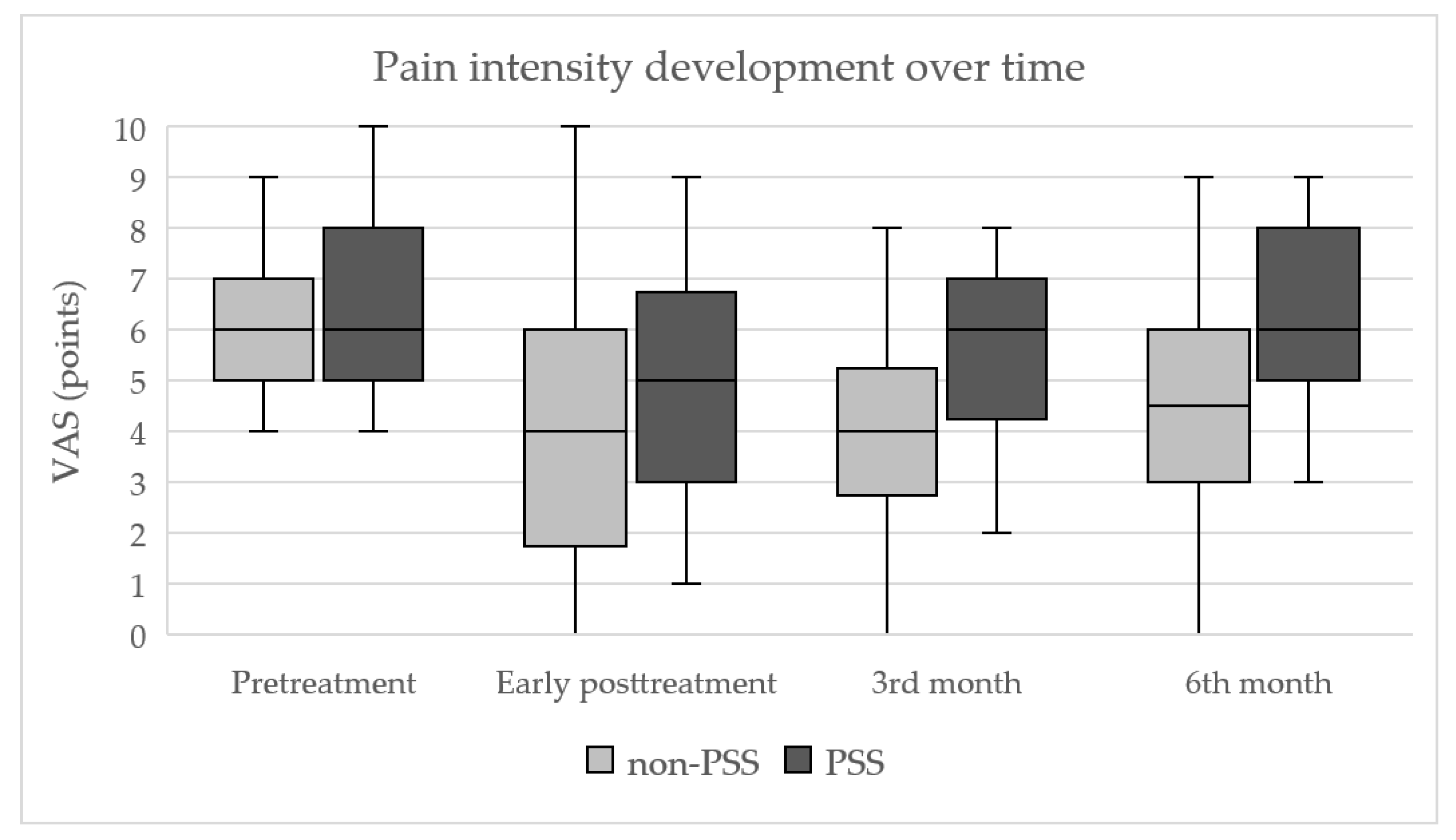
3.2.1. Development of Pain Intensity (VAS)
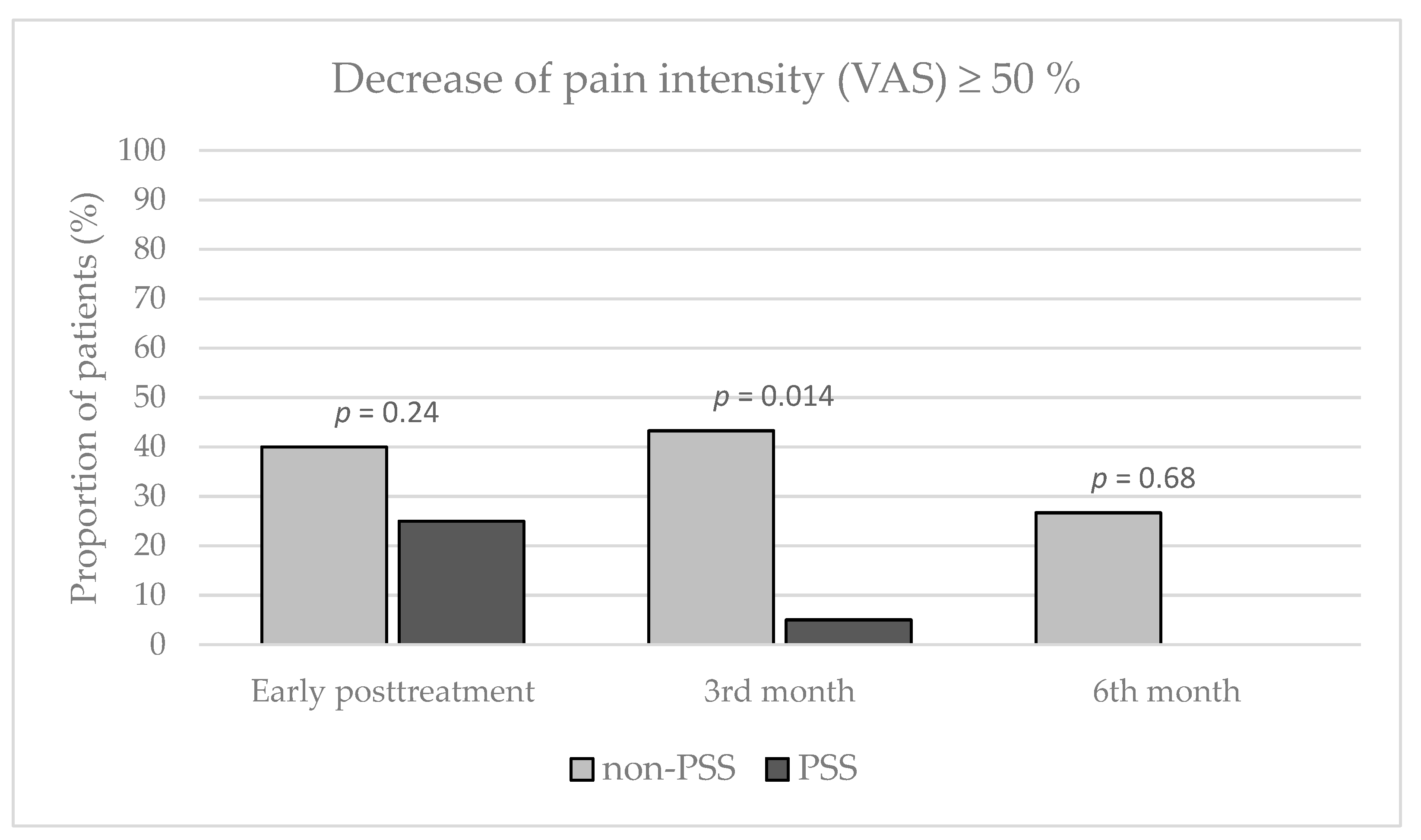
3.2.2. Relative Decrease of VAS ≥ 50%
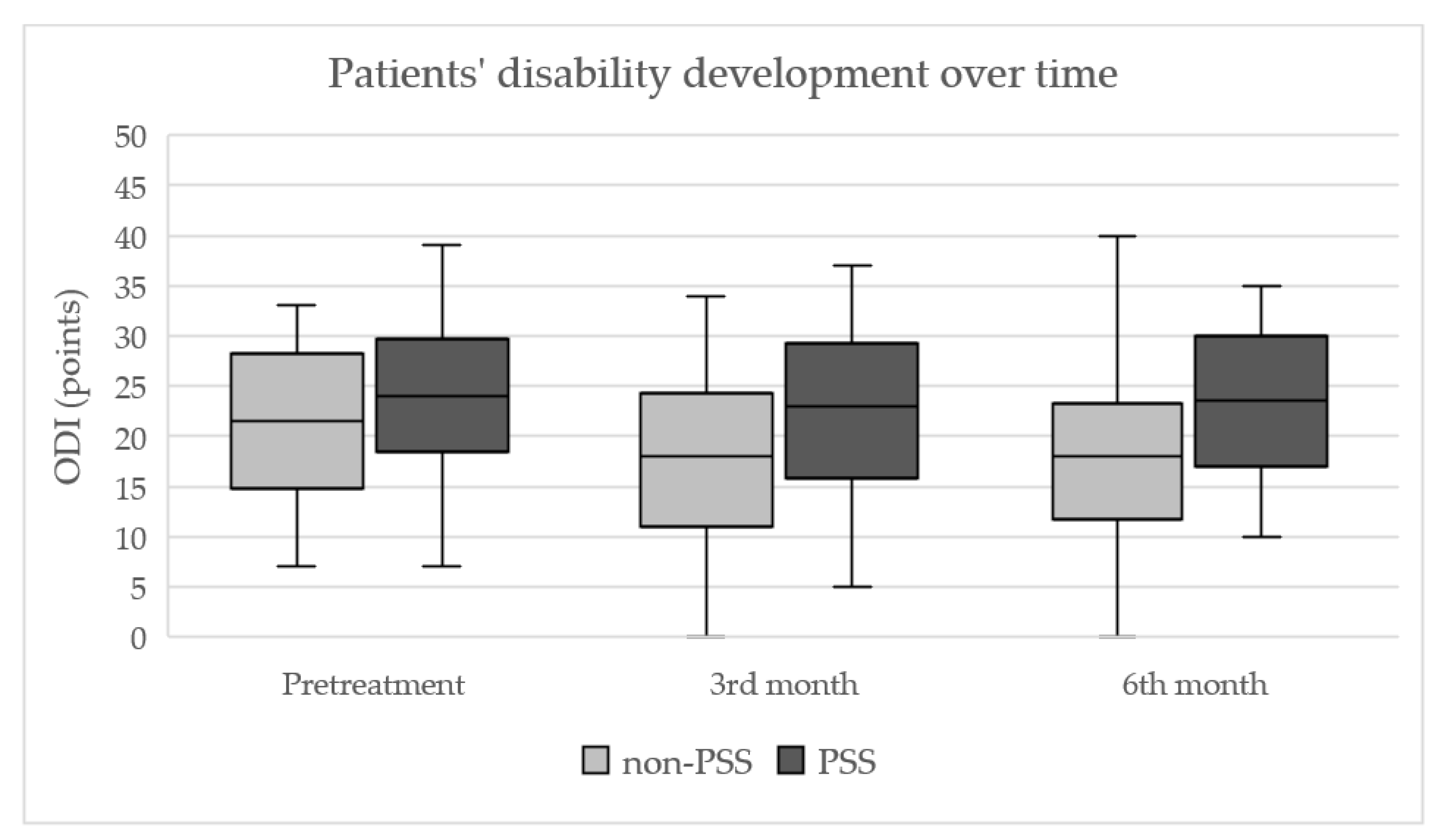
3.2.3. Development of Patients’ Disability (ODI)
3.2.4. Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vigneri, S.; Sindaco, G.; Gallo, G.; Zanella, M.; Paci, V.; La Grua, M.; Ravaioli, L.; Pari, G. Effectiveness of pulsed radiofrequency with multifunctional epidural electrode in chronic lumbosacral radicular pain with neuropathic features. Pain Physician 2014, 17, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, K.; Litchy, W.J.; O’Fallon, W.M.; Kurland, L.T. Epidemiology of cervical radiculopathy. A population-based study from Rochester, Minnesota, 1976 through 1990. Brain 1994, 117, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, K.; Dunn, K.M. Sciatica: Review of epidemiological studies and prevalence estimates. Spine 2008, 15, 2464–2472. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; O’Connor, A.B.; Backonja, M.; Farrar, J.T.; Finnerup, N.B.; Jensen, T.S.; Kalso, E.A.; Loeser, J.D.; Miaskowski, C.; Nurmikko, T.J.; et al. Pharmacologic management of neuropathic pain: Evidence-based recommendations. Pain 2007, 132, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.J.; Wedderburn, L.; Whaley, A.; Grahame, R.; Newman, S. Outcome assessment after epidural corticosteroid injection for low back pain and sciatica. Spine 1993, 18, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Suri, P.; Rainville, J.; Hunter, D.J.; Li, L.; Katz, J.N. Recurrence of radicular pain or back pain after nonsurgical treatment of symptomatic lumbar disk herniation. Arch. Phys. Med. Rehabil. 2012, 93, 690–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grøvle, L.; Haugen, A.J.; Keller, A.; Ntvig, B.; Brox, J.I.; Grotle, M. Prognostic factors for return to work in patients with sciatica. Spine J. 2013, 13, 1849–1857. [Google Scholar] [CrossRef]
- Van Boxem, K.; de Meij, N.; Kessels, A.; Van Kleef, M.; Van Zundert, J. Pulsed radiofrequency for chronic intractable lumbosacral radicular pain: A six-month cohort study. Pain Med. 2015, 16, 1155–1162. [Google Scholar] [CrossRef] [Green Version]
- Mehta, V.; Snidvongs, S.; Ghai, B.; Langford, R.; Wodehouse, T. Characterization of peripheral and central sensitization after dorsal root ganglion intervention in patients with unilateral lumbosacral radicular pain: A prospective pilot study. Br. J. Anaesth. 2017, 118, 924–931. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.G.; Cho, Y.W.; Ahn, S.H.; Chang, M.C. The Effect of Bipolar Pulsed Radiofrequency Treatment on Chronic Lumbosacral Radicular Pain Refractory to Monopolar Pulsed Radiofrequency Treatment. Pain Physician 2018, 21, E97–E103. [Google Scholar]
- Byrd, D.; Mackey, S. Pulsed radiofrequency for chronic pain. Curr. Pain Headache Rep. 2008, 12, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Sluijter, M.; Racz, G. Technical aspects of radiofrequency. Pain Pract. 2002, 2, 195–200. [Google Scholar] [CrossRef]
- Park, D.; Chang, M.C. The mechanism of action of pulsed radiofrequency in reducing pain: A narrative review. J. Yeungnam Med. Sci. 2022, 39, 200–205. [Google Scholar] [CrossRef]
- Facchini, G.; Spinnato, P.; Guglielmi, G.; Albisinni, U.; Bazzocchi, A. A comprehensive review of pulsed radiofrequency in the treatment of pain associated with different spinal conditions. Brit. J. Radiol. 2017, 90, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.W.; Peng, P. Failed back surgery syndrome. Pain Med. 2011, 12, 577–606. [Google Scholar] [CrossRef] [Green Version]
- Daniell, J.R.; Osti, O.L. Failed Back Surgery Syndrome: A Review Article. Asian Spine J. 2018, 12, 372–379. [Google Scholar] [CrossRef]
- Ortiz, A.O.; de Moura, A.; Johnson, B.A. Postsurgical Spine: Techniques, Expected Imaging Findings, and Complications. Semin. Ultrasound CT MR 2018, 39, 630–650. [Google Scholar] [CrossRef]
- Hussain, A.; Erdek, M. Interventional pain management for failed back surgery syndrome. Pain Pract. 2014, 14, 64–78. [Google Scholar] [CrossRef]
- Ryska, P.; Jandura, J.; Hoffmann, P.; Dvorak, P.; Klimova, B.; Valis, M.; Vajda, M. Comparison of Pulsed Radiofrequency, Oxygen-Ozone Therapy and Epidural Steroid Injections for the Treatment of Chronic Unilateral Radicular Syndrome. Medicina 2021, 57, 136. [Google Scholar] [CrossRef]
- Abejón, D.; Garcia-del-Valle, S.; Fuentes, M.L.; Gómez-Arnau, J.I.; Reig, E.; van Zundert, J. Pulsed radiofrequency in lumbar radicular pain: Clinical effects in various etiological groups. Pain Pract. 2007, 7, 21–26. [Google Scholar] [CrossRef]
- Yang, L.; Huang, Y.; Ma, J.; Li, Z.; Han, R.; Guo, G.; Ni, Y.; Hu, R.; Yan, X.; Zhou, H.; et al. Clinical Outcome of Pulsed-Radiofrequency Combined with Transforaminal Epidural Steroid Injection for Lumbosacral Radicular Pain Caused by Distinct Etiology. Front. Neurosci. 2021, 15, 683298. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, S.J.; Yoon, D.M.; Yoon, K.B.; Kim, S.H. Predictors of the analgesic efficacy of pulsed radiofrequency treatment in patients with chronic lumbosacral radicular pain: A retrospective observational study. J. Pain Res. 2018, 11, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Shanthanna, H.; Chan, P.; McChesney, J.; Thabane, L.; Paul, J. Pulsed radiofrequency treatment of the lumbar dorsal root ganglion in patients with chronic lumbar radicular pain: A randomized, placebo-controlled pilot study. J. Pain Res. 2014, 7, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Shiri, R.; Lallukka, T.; Karppinen, J.; Viikari-Juntura, E. Obesity as a risk factor for sciatica: A meta-analysis. Am. J. Epidemiol. 2014, 179, 929–937. [Google Scholar] [CrossRef] [Green Version]
- Vanneste, T.; Van Lantschoot, A.; Van Boxem, K.; Van Zundert, J. Pulsed radiofrequency in chronic pain. Curr. Opin. Anaesthesiol. 2017, 30, 577–582. [Google Scholar] [CrossRef]
- Gabrhelik, T.; Michalek, P.; Berta, E.; Adamus, M.; Pieran, M.; Dolecek, L. Pulzni radiofrekvencni terapie radikularni bolesti. Cesk Slov. Neurol. Neurosurg. 2007, 70/103, 533–537. [Google Scholar]
- Chang, M.C. Efficacy of Pulsed Radiofrequency Stimulation in Patients with Peripheral Neuropathic Pain: A Narrative Review. Pain Physician 2018, 21, E225–E234. [Google Scholar] [CrossRef]
- Farì, G.; de Sire, A.; Fallea, C.; Albano, M.; Grossi, G.; Bettoni, E.; Di Paolo, S.; Agostini, F.; Bernetti, A.; Puntillo, F.; et al. Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 600. [Google Scholar] [CrossRef]
- Sluijter, M.E. The role of radiofrequency in failed back surgery patients. Curr. Rev. Pain. 2000, 4, 49–53. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Varonen, H.; Kalso, E.; Ukkola, O.; Viikari-Juntura, E. Cardiovascular and lifestyle risk factors in lumbar radicular pain or clinically defined sciatica: A systematic review. Cardiovascular and lifestyle risk factors in lumbar radicular pain or clinically defined sciatica: A systematic review. Eur. Spine J. 2007, 16, 2043–2054. [Google Scholar] [CrossRef] [Green Version]
- Nordstoga, A.L.; Nilsen, T.I.L.; Vasseljen, O.; Unsgaard-Tøndel, M.; Mork, P.J. The influence of multisite pain and psychological comorbidity on prognosis of chronic low back pain: Longitudinal data from the Norwegian HUNT Study. BMJ Open 2017, 7, e015312. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.C.; Chen, C.J.; Chou, C.C.; Wang, H.Y.; Chung, W.Y.; Peng, G.S.; Lin, C.P. Lumbar Dorsal Root Ganglion Block as a Prognostic Tool Before Pulsed Radiofrequency: A Randomized, Prospective, and Comparative Study on Cost-Effectiveness. World Neurosurg. 2018, 112, e157–e164. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-PSS | PSS | p-Value | |
|---|---|---|---|
| n | 30 | 20 | |
| age (median/q3-q1) | 57.5/51.8–66.2 | 53.5/46.5–61 | 0.25 |
| sex (male/female) | 12/18 | 9/11 | 0.78 |
| BMI (median/q3-q1) | 29.2/26.6–33.4 | 26.5/24.4–29 | 0.043 |
| treated DRG (L5/S1) | 15/15 | 14/6 | 0.11 |
| smokers n (%) | 3 (10%) | 2 (10%) |
| Interventions | Total | Non-Fusion | Fusion | Disc Replacement |
|---|---|---|---|---|
| n | 20 | 16 | 3 | 1 |
| Etiology | ||||
| trauma | 1 | 0 | 1 | 0 |
| disc hernia | 14 | 14 | 0 | 0 |
| foraminostenosis | 8 | 5 | 2 | 1 |
| instability | 3 | 0 | 3 | 0 |
| Spinal segments | ||||
| L4-5/L5-S1 | 18 | 9/7 | 1/0 | 0/1 |
| >1 spinal segment | 2 | 0 | 1 | 1 |
| Repeat surgery | 1 | 1 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jandura, J.; Vajda, M.; Kostysyn, R.; Vanasek, J.; Cermakova, E.; Zizka, J.; Ryska, P. Previous Lumbar Spine Surgery Decreases the Therapeutic Efficacy of Dorsal Root Ganglion Pulsed Radiofrequency in Patients with Chronic Lumbosacral Radicular Pain. J. Pers. Med. 2023, 13, 1054. https://doi.org/10.3390/jpm13071054
Jandura J, Vajda M, Kostysyn R, Vanasek J, Cermakova E, Zizka J, Ryska P. Previous Lumbar Spine Surgery Decreases the Therapeutic Efficacy of Dorsal Root Ganglion Pulsed Radiofrequency in Patients with Chronic Lumbosacral Radicular Pain. Journal of Personalized Medicine. 2023; 13(7):1054. https://doi.org/10.3390/jpm13071054
Chicago/Turabian StyleJandura, Jiri, Milan Vajda, Roman Kostysyn, Jiri Vanasek, Eva Cermakova, Jan Zizka, and Pavel Ryska. 2023. "Previous Lumbar Spine Surgery Decreases the Therapeutic Efficacy of Dorsal Root Ganglion Pulsed Radiofrequency in Patients with Chronic Lumbosacral Radicular Pain" Journal of Personalized Medicine 13, no. 7: 1054. https://doi.org/10.3390/jpm13071054