1. Introduction
There is increasing evidence that female patients have worse early and late outcomes in coronary, aortic and valve surgeries [
1,
2,
3,
4]. The reasons for this might be the following: women present with atypical symptoms (leading to under-diagnosis or misdiagnosis), are referred later for surgery (presenting older and with more comorbidities) and less often (despite a higher incidence of mitral prolapse) due to guidelines, which are derived from research mainly performed on male subjects [
1,
5,
6,
7]. Furthermore, women more often receive mitral valve replacement, and mitral repair does not restore their normal life expectancy [
8]. Therefore, the female gender has been identified as an independent risk factor for mortality after cardiac surgery and was included in the risk assessment scores (EuroSCORE II and STS Score) [
9,
10]. Minimally invasive video-assisted mitral valve surgery (MIV) is the standard of care at specialized centers worldwide, shows excellent short and long-term outcomes and is even superior to sternotomy, as shown in meta-analyses and propensity-matched studies [
11,
12,
13,
14]. However, little is known about gender-dependent outcomes in MIV. The EACTS guidelines suggest the “heart team” as a class 1C indication, which makes it a mandatory decision-making organ in the presence of an increasing number of transcatheter treatment options [
15]. However, there is still a lack of evidence regarding the influence of heart-team decision-making on gender-dependent outcomes. Therefore, the aim of our study was to analyze the outcomes of our single-center heart team’s decision-based and MIV-specialized cohort with regard to gender.
2. Materials and Methods
In 2013, we established a structural heart team center where every single valve case is discussed in an interdisciplinary approach to enable patient-tailored therapies (cardiac surgery, percutaneous, or conservative treatment) and, consequently, to reduce interventional risk. The concept and preliminary outcomes of our heart team approach comparing the outcomes of MIV and Mitra-clip patients have already been published elsewhere [
16]. Based on this decision-making by our institutionalized multidisciplinary heart team, we aimed to analyze our MIV cohort according to gender-related outcomes: preoperative characteristics, in-hospital outcomes (30 days) and follow-up information (survival, valve competence, freedom from reoperation) were collected and analyzed retrospectively from our institutional database, from follow-up records of our referring cardiologists, and prospectively by contacting all patients by phone. Ethics committee approval from our local institutional review board (amendment to the approval number 2017-01895) and signed informed consent were obtained from every patient in this study. Our heart team meets weekly and consists of cardiac surgeons, cardiologists (interventionalist and non-invasive cardiologists, including imaging specialists), cardiac anesthetists and intensivists. It is a financially independent organ, where every valve case is discussed and decision-making is performed according to guidelines and surgical risk assessments: patients younger than 80 years without excessive operative risk (i.e., EuroSCORE II < 4%) are primarily evaluated for MIV feasibility, “high risk” patients and those with a morphological lower probability for successful surgical MIV-repair are treated percutaneously with edge-to-edge technique (MitraClip, Abbott or Pascal Edwards). We are a specialized MIV center and our only contraindications for this approach are severe coronary disease requiring grafting with ischemic regurgitation, suspected adhesions in the right thorax (previous surgery or irradiation), severe annular calcification and grade III-IV arteriosclerosis of the ascending and/or descending aorta.
Our surgical technique has already been described previously [
17]; femoral cannulation is performed either percutaneously or surgically (Seldinger technique).
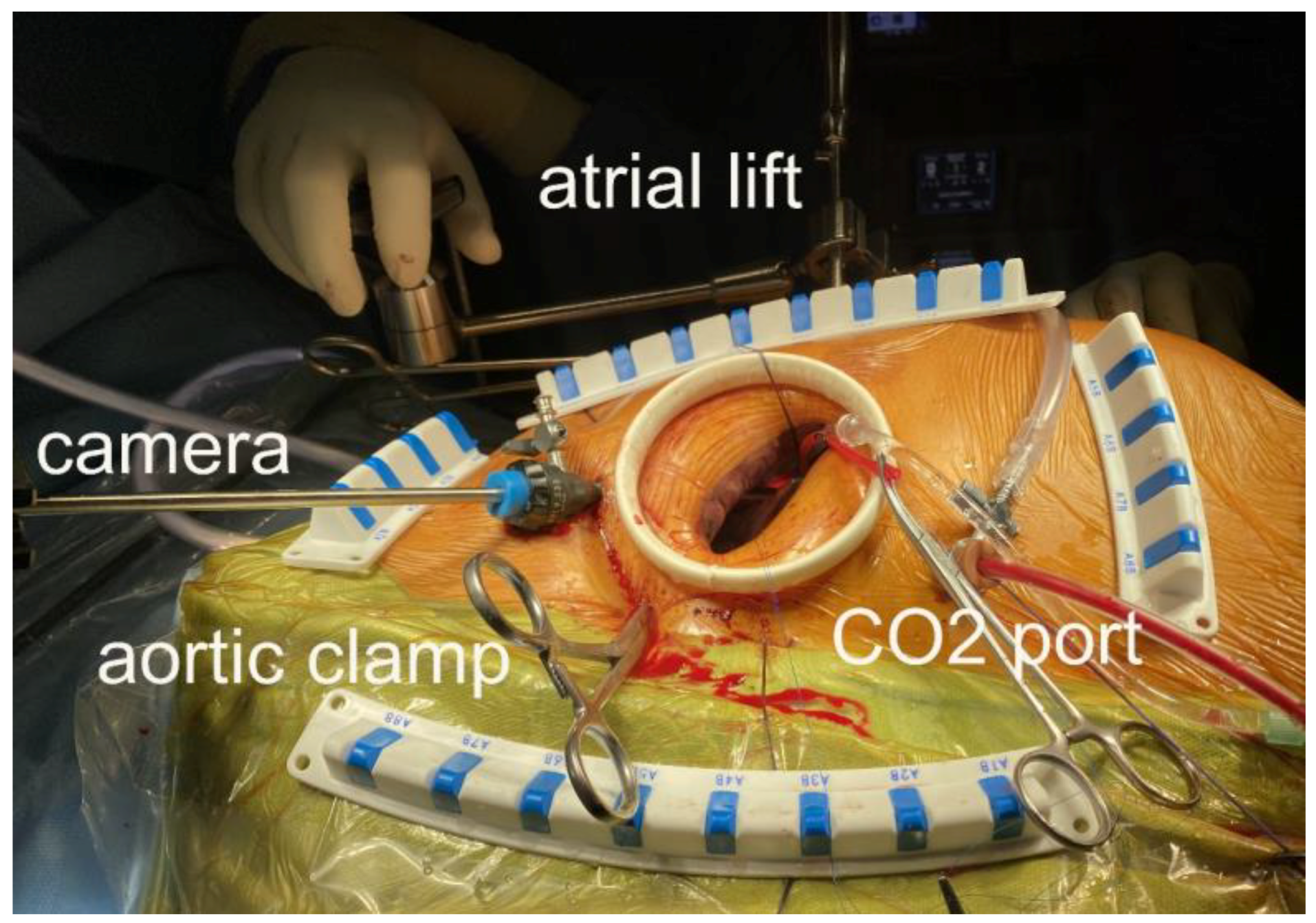
Figure 1 shows the intraoperative settings. CO
2 insufflation through a caudal port is mandatory. A long aortic root cannula is used for antegrade cardioplegia (Custodiol, Brettschneider), which is also used as a vent for de-airing. The atrial lift retractor is inserted through a right parasternal hole under camera guidance in order to avoid injuring the mammary artery. We implant an annuloplasty ring in all repair cases. When resection is required (excess tissue), we perform it triangularly (small area to avoid tension and immobility). When neo-chordae are required, we use single Goretex sutures (Gore, Newark, DE, USA). Further repair techniques include cleft closures, commissuroplasty and very rarely, sliding plasty or Alfieri-Stich. Concomitant procedures include left atrial appendage closure with sutures or clips, cryoablation, patent foramen ovale or ASD closure and tricuspid valve annuloplasty when indicated. During the mitral valve replacement, we resect the anterior leaflet only. Mitral repair and biological prosthesis patients receive warfarin for 3 months (mechanical valves are lifelong). All patients receive an echocardiogram by our specialized interventional imaging cardiologists in the theatre after de-clamping (transesophageal) and before discharge (transthoracic) to evaluate the results of the surgery. Regurgitation grade is defined from 1 to 4 with none and trace, mild, moderate, or severe. After the rehabilitation period, patients are evaluated clinically and echocardiographically by their referring cardiologists initially after 3 months, then after 1 year and annually thereafter.
All statistical analyses were performed using R version 4.2.1 (The R Foundation for Statistical Computing, Vienna, Austria). Categorical variables are presented as frequencies with percentages and compared between groups using Fisher’s exact test. Continuous variables are presented as mean ± standard deviation (SD) and compared between groups using the Mann–Whitney test. Overall survival and freedom from re-intervention are presented as Kaplan–Meier curves and compared between groups using the log-rank test. Propensity score matching was used to overcome the inherent imbalance between female and male patients. Using logistic regression, the propensity score (PS) for the probability of being female was calculated for each operated patient. The used covariates in the model were EuroSCORE II (without female regression coefficient of 0.2196434), age, ejection fraction, atrial fibrillation, NYHA III/IV, COPD, coronary artery disease (CAD), previous stroke, previous percutaneous coronary intervention (PCI), Barlow’s disease, single-segment pathology, two-segment pathology anterior or posterior, posterior pathology only, anterior and posterior pathology without Barlow’s, commissural pathology, leaflet calcification and severe tricuspid regurgitation. We performed one-to-one nearest neighbour propensity score matching without replacement with a caliper of 0.2 of the SD of the logit-transformed PS. After matching, all standardized mean differences (SMD) for the covariates were below 0.1, indicating an adequate balance [
18].
Due to the small number of events, multivariable analysis, including possible variable transformations, interactions, cut-off values and model checking, would not be the correct method of analysis. Hence, we decided not to perform it in our study.
4. Discussion
Our data from a multidisciplinary structural heart team decision-based MIV cohort suggest, that despite women being older and sicker, with more complex valve pathology and subsequent replacement, more tricuspid repair, longer ICU and hospital stay and more atrial fibrillation, early and mid-term mortality, morbidity and re-intervention are still low and comparable to those of men. We believe that these favorable outcomes might be the combined result of our heart team approach, the MIV setting and the experienced surgeons, which seems to eliminate the female gender as an independent risk factor for cardiac surgery.
It could be argued that another reason for our good results might be the low-risk patient selection for MIV because the majority of degenerative mitral cases usually present with a single segment P2 prolapse, which can be easily repaired, resulting in excellent durability and a life expectancy comparable to the general population in both MIV and sternotomy studies [
19,
20,
21,
22]. However, our findings prove otherwise: despite a high incidence of mixed and complex valve pathologies in our MIV cohort (predominantly in women), we have a low mid-term morbidity/mortality and re-intervention rate, which is comparable to the outcomes in men. In our preliminary study of our heart team's decision-based approach, we showed that women older than 75 years and smaller than 170 cm have an increased risk if they are treated with MIV (16). With this finding in mind and the outcomes of our present analysis, it seems that our heart team approach was able to eliminate the female gender as an independent risk factor for MIV. Several studies of sternotomy cohorts showed that anterior and/or bi-leaflet pathologies, tissue thickening and calcifications are more common in women (comparable to our findings); therefore, they are more complex to repair with longer cross-clamping, which results in higher morbidity and mortality and an increased risk for recurrent mitral regurgitation in women [
19,
21,
23,
24]. A large study of Medicare beneficiaries (n = 183,792) also revealed a significantly increased early mortality after mitral surgery through sternotomy in women but comparable long-term outcomes [
8]. Furthermore, it was shown that women received mitral valve replacement more often due to more complex valve pathologies, and mitral repair only restored normal life expectancy in men but not in women [
8]. Similarly, Johnston et al. found that female patients had comparable early mortality and better survival after mitral valve replacement than men, whereas men had better survival after mitral repair [
3]. Propensity-matched studies comparing MIV versus sternotomy showed that women were older at admission and less likely to be considered for MIV, but with comparable results for both gender groups and surgical techniques [
25,
26]. When comparing the outcomes of surgical and percutaneous mitral valve treatments in the elderly, it was shown that there was lower morbidity and mortality up to 1 year compared with surgery, but a higher recurrence of regurgitation and mortality beyond [
27,
28].
In the past decades, selective studies have made us aware of the fact that, despite women having a higher incidence of mitral prolapse, fewer are referred for surgery, and they are older, sicker, have lower repair rates and worse outcomes than men after cardiac surgery through sternotomy [
1,
2,
4,
5,
7,
29,
30,
31]. The reasons for this might be misdiagnosis (mild and/or atypical cardiovascular symptoms) and underdiagnosis (women less often reach diameter-based surgical guideline criteria because they were originally established for men) [
1,
5,
6,
7,
29,
31,
32]. A propensity-matched report of 270 gender pairs showed comparable gender outcomes through sternotomy due to their dedicated use of speckle-tracking echo analysis, which can reveal ventricular dysfunction and prevent delayed surgery in women [
33]. We did not use speckle-tracking, and in our cohort, women were also older and sicker (which could be a sign of delayed referral). However, short- and mid-term mortality and the need for re-intervention were low and comparable to those in men.
We believe that our favorable outcomes are the result of our multidisciplinary heart team decision-making concept, which allows patient-tailored medicine combined with the dedicated work of our experienced surgeons and the MIV approach itself, which has proven to be advantageous mainly in high-risk and elderly patients [
34]. However, the Leipzig group also showed in their large all-comer MIV cohort that the female gender is an independent predictor of cardiac mortality with significantly worse long-term survival in women. They had less posterior leaflet pathology and received more valve replacements and tricuspid surgery than men, which is comparable to our findings [
19,
22]. We still have to wait for our long-term data in order to confirm our excellent and comparable mid-term outcomes, but we are confident that the re-intervention rate will remain low because the incidence mainly occurs at a mean of 15 months [
35].
Our propensity-matched analysis showed a 5-year survival of women with 94.2% (95% CI 87.1–100%) and men with 88.4.5% (95% CI 79.7–98%) (
p = 0.03), which is better than that reported in other studies (65–85%), where anterior and bi-leaflet pathologies showed the worst outcomes [
19,
23,
36,
37]. Our freedom from re-intervention at 5 years is 92.7% (95% CI 84.3–100%) in women and 98.2% (95% CI 94.8–100%) in men (
p = 0.03) and is comparable or better than in other studies (90–96%) where anterior leaflet pathology is described as the only independent predictor of reoperation [
19,
22,
23,
36]. At the closing of the follow-up on 31 December 2022 (up to 9.5 years), only two patients (0.7%, both women) had New York Heart Association function class III/IV symptoms and 96.3% of the valves were competent (<grade 2 regurgitation), which was constant over time (comparable between the groups). These findings are similar or superior to those described in other studies with up to 11% NYHA III/IV in long-term follow-up [
20,
23].
The limitations of our study are the following: it is a low-volume, single-center, retrospective observational study, which allows for potential biases. There was no control group available because we did not perform median sternotomy for isolated mitral valve surgery at our institution. Furthermore, we decided not to include our Mitra-Clip cohort again, since we already published a comparison of the two cohorts previously. The strength of this study is the use of propensity score matching. There is a variation in the follow-up duration (a few weeks up to 9 years), which reduces the validity of the long-term results. We are a specialized heart team decision-based MIV center and our outcomes might not be reproducible elsewhere. Our MIV patient cohort was low-risk, and some were lost to follow-up or were waiting for outpatient visits. Except for in-hospital echocardiography, we did not use a core lab for follow-up imaging, which might have resulted in interpretational bias.







{kind=link}
{kind=link}
{kind=link}
{kind=link}