
Preventive Proximal Splenic Artery Embolization for High-Grade AAST-OIS Adult Spleen Trauma without Vascular Anomaly on the Initial CT Scan: Technical Aspect, Safety, and Efficacy—An Ancillary Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Procedures
2.4. Technical Assessment
2.5. Safety and Efficacy Assessments
2.6. Statistics
3. Results
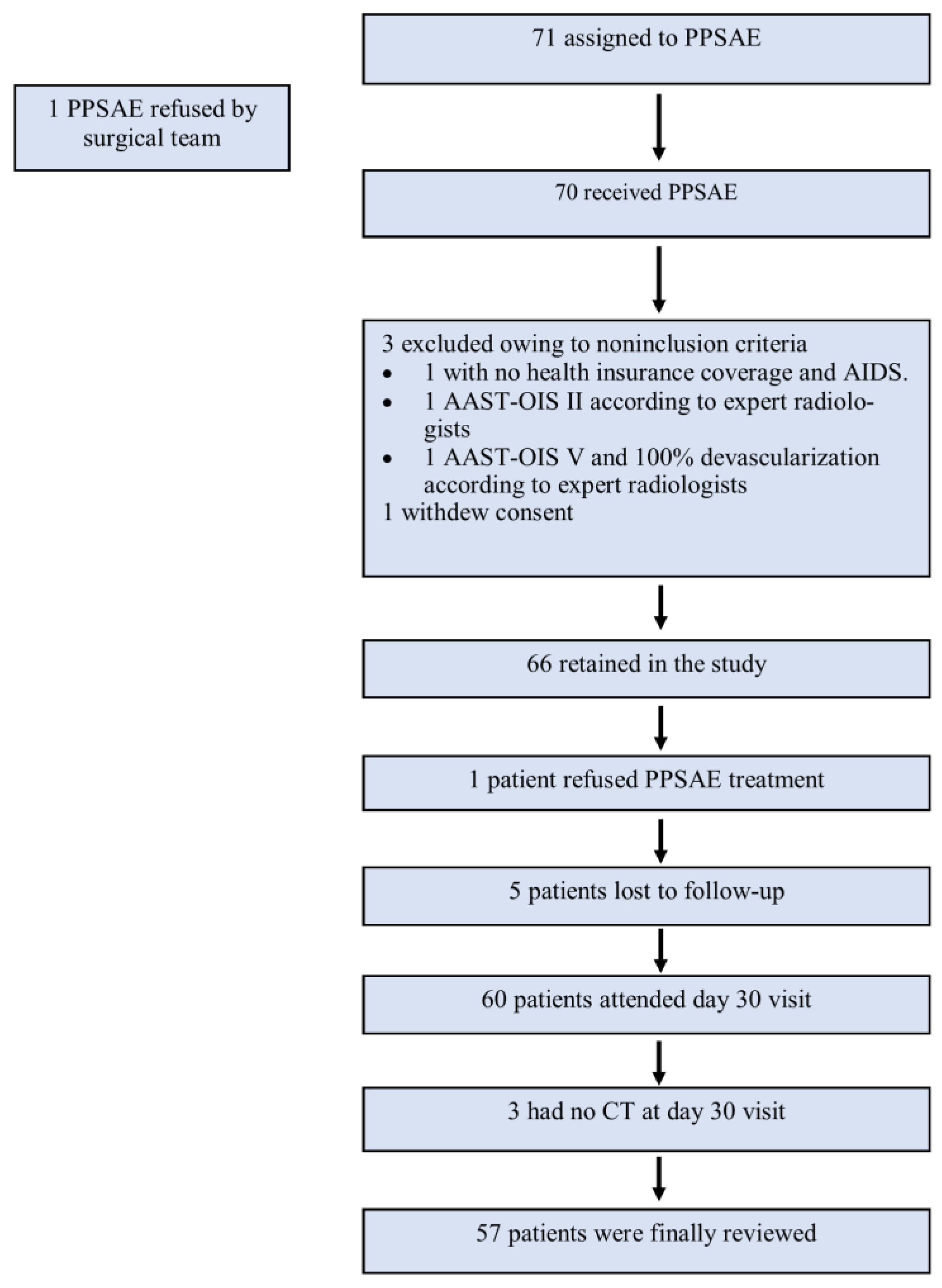
3.1. Patients
3.2. Technical Results
3.3. Safety, Efficacy, and One-Month Splenic Salvage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Requarth, J.A.; D’Agostino, R.B.; Miller, P.R. Nonoperative management of adult blunt splenic injury with and without splenic artery embolotherapy: A meta-analysis. J. Trauma 2011, 71, 898–903, discussion 903. [Google Scholar] [CrossRef] [PubMed]
- Zarzaur, B.L.; Croce, M.A.; Fabian, T.C. Variation in the Use of Urgent Splenectomy After Blunt Splenic Injury in Adults. J. Trauma Acute Care Surg. 2011, 71, 1333. [Google Scholar] [CrossRef] [PubMed]
- Quencer, K.B.; Smith, T.A. Review of proximal splenic artery embolization in blunt abdominal trauma. CVIR Endovasc. 2019, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Duane, T.M.; Wilson, S.P.; Haney, S.; O’Neill, P.J.; Evans, H.L.; Como, J.J.; Claridge, J.A. Trauma center variation in splenic artery embolization and spleen salvage: A multicenter analysis. J. Trauma Acute Care Surg. 2013, 75, 69–74, discussion 74–75. [Google Scholar] [CrossRef]
- Stassen, N.A.; Bhullar, I.; Cheng, J.D.; Crandall, M.L.; Friese, R.S.; Guillamondegui, O.D.; Jawa, R.S.; Maung, A.A.; Rohs, T.J., Jr.; Sangosanya, A.; et al. Selective nonoperative management of blunt splenic injury: An Eastern Association for the Surgery of Trauma practice management guideline. J. Trauma Acute Care Surg. 2012, 73 (Suppl. S4), S294–S300. [Google Scholar] [CrossRef]
- Patil, M.S.; Goodin, S.Z.; Findeiss, L.K. Update: Splenic Artery Embolization in Blunt Abdominal Trauma. Semin Intervent. Radiol. 2020, 37, 97–102. [Google Scholar] [CrossRef]
- Padia, S.A.; Ingraham, C.R.; Moriarty, J.M.; Wilkins, L.R.; Bream, P.R.; Tam, A.L.; Patel, S.; McIntyre, L.; Wolinsky, P.R.; Hanks, S.E. Society of Interventional Radiology Position Statement on Endovascular Intervention for Trauma. J. Vasc. Interv. Radiol. 2020, 31, 363–369.e2. [Google Scholar] [CrossRef]
- Xu, S.S.; Eng, K.; Accorsi, F.; Cool, D.W.; Wiseman, D.; Mujoomdar, A.; Cardarelli-Leite, L. Proximal splenic artery embolization using a vascular plug in grade IV or V splenic trauma—A single centre 11-year experience. CVIR Endovasc. 2023, 6, 1. [Google Scholar] [CrossRef]
- Arvieux, C.; Frandon, J.; Tidadini, F.; Monnin-Bares, V.; Foote, A.; Dubuisson, V.; Lermite, E.; David, J.-S.; Douane, F.; Tresallet, C.; et al. Effect of Prophylactic Embolization on Patients With Blunt Trauma at High Risk of Splenectomy: A Randomized Clinical Trial. JAMA Surg. 2020, 155, 1102–1111. [Google Scholar] [CrossRef]
- Duranteau, J.; Asehnoune, K.; Pierre, S.; Ozier, Y.; Leone, M.; Lefrant, J.Y. Recommandations sur la réanimation du choc hémorragique. Anesth. Réanim. 2015, 1, 62–74. [Google Scholar] [CrossRef]
- Khalilzadeh, O.; Baerlocher, M.O.; Shyn, P.B.; Connolly, B.L.; Devane, A.M.; Morris, C.S.; Cohen, A.M.; Midia, M.; Thornton, R.H.; Gross, K.; et al. Proposal of a New Adverse Event Classification by the Society of Interventional Radiology Standards of Practice Committee. J. Vasc. Interv. Radiol. 2017, 28, 1432–1437.e3. [Google Scholar] [CrossRef]
- Zoppo, C.; Valero, D.A.; Murugan, V.A.; Pavidapha, A.; Flahive, J.; Newbury, A.; Fallon, E.; Harman, A. Splenic Artery Embolization for Unstable Patients with Splenic Injury: A Retrospective Cohort Study. J. Vasc. Interv. Radiol. 2023, 34, 86–93. [Google Scholar] [CrossRef]
- Demetriades, D.; Scalea, T.M.; Degiannis, E.; Barmparas, G.; Konstantinidis, A.; Massahis, J.; Inaba, K. Blunt splenic trauma: Splenectomy increases early infectious complications: A prospective multicenter study. J. Trauma Acute Care Surg. 2012, 72, 229. [Google Scholar] [CrossRef]
- Schnüriger, B.; Inaba, K.; Konstantinidis, A.; Lustenberger, T.; Chan, L.S.; Demetriades, D. Outcomes of proximal versus distal splenic artery embolization after trauma: A systematic review and meta-analysis. J. Trauma 2011, 70, 252–260. [Google Scholar] [CrossRef]
- Bhangu, A.; Nepogodiev, D.; Lal, N.; Bowley, D.M. Meta-analysis of predictive factors and outcomes for failure of non-operative management of blunt splenic trauma. Injury 2012, 43, 1337–1346. [Google Scholar] [CrossRef]
- Sclafani, S.J.; Shaftan, G.W.; Scalea, T.M.; Patterson, L.A.; Kohl, L.; Kantor, A.; Herskowitz, M.M.; Michael, M.; Hoffer, E.K.; Henry, S.; et al. Nonoperative salvage of computed tomography-diagnosed splenic injuries: Utilization of angiography for triage and embolization for hemostasis. J. Trauma 1995, 39, 818–825, discussion 826–827. [Google Scholar] [CrossRef]
- Haan, J.M.; Bochicchio, G.V.; Kramer, N.; Scalea, T.M. Nonoperative management of blunt splenic injury: A 5-year experience. J. Trauma 2005, 58, 492–498. [Google Scholar] [CrossRef]
- Haan, J.M.; Biffl, W.; Knudson, M.M.; Davis, K.A.; Oka, T.; Majercik, S.; Dicker, R.; Marder, S.; Scalea, T.M. Splenic embolization revisited: A multicenter review. J. Trauma 2004, 56, 542–547. [Google Scholar] [CrossRef]
- Rong, J.J.; Liu, D.; Liang, M.; Wang, Q.H.; Sun, J.Y.; Zhang, Q.Y.; Peng, C.-F.; Xuan, F.-Q.; Zhao, L.-J.; Tian, X.-X.; et al. The impacts of different embolization techniques on splenic artery embolization for blunt splenic injury: A systematic review and meta-analysis. Mil. Med. Res. 2017, 4, 17. [Google Scholar] [CrossRef]
- Dent, D.; Alsabrook, G.; Erickson, B.A.; Myers, J.; Wholey, M.; Stewart, R.; Root, H.; Ferral, H.; Postoak, D.; Napier, D.; et al. Blunt splenic injuries: High nonoperative management rate can be achieved with selective embolization. J. Trauma 2004, 56, 1063–1067. [Google Scholar] [CrossRef]
- Bessoud, B.; Denys, A.; Calmes, J.M.; Madoff, D.; Qanadli, S.; Schnyder, P.; Doenz, F. Nonoperative management of traumatic splenic injuries: Is there a role for proximal splenic artery embolization? AJR Am. J. Roentgenol. 2006, 186, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Rajani, R.R.; Claridge, J.A.; Yowler, C.J.; Patrick, P.; Wiant, A.; Summers, J.I.; McDonald, A.A.; Como, J.J.; Malangoni, M.A. Improved outcome of adult blunt splenic injury: A cohort analysis. Surgery 2006, 140, 625–631, discussion 631–632. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.R.; Chang, M.C.; Hoth, J.J.; Mowery, N.T.; Hildreth, A.N.; Martin, R.S.; Holmes, J.H.; Meredith, W.J.; Requarth, J.A. Prospective trial of angiography and embolization for all grade III to V blunt splenic injuries: Nonoperative management success rate is significantly improved. J. Am. Coll. Surg. 2014, 218, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, R.M.; Schermer, C.R.; Morris, A. Nonoperative management of blunt splenic injuries: Factors influencing success in age >55 years. Am. Surg. 2002, 68, 227–230, discussion 230–231. [Google Scholar] [CrossRef]
- McIntyre, L.K.; Schiff, M.; Jurkovich, G.J. Failure of nonoperative management of splenic injuries: Causes and consequences. Arch Surg. 2005, 140, 563–568, discussion 568–569. [Google Scholar] [CrossRef]
- Splenic Artery Embolization: Proximal or Distal? Endovascular Today. Bryn Mawr Communications. Available online: https://evtoday.com/articles/2018-apr/splenic-artery-embolization-proximal-or-distal (accessed on 11 April 2023).
- Vaidya, S.; Tozer, K.R.; Chen, J. An Overview of Embolic Agents. Semin Intervent. Radiol. 2008, 25, 204–215. [Google Scholar] [CrossRef]
- Crooker, K.G.; Howard, J.M.; Alvarado, A.R.; McDonald, T.J.; Berry, S.D.; Green, J.L.; Winfield, R.D. Splenic Embolization After Trauma: An Opportunity to Improve Best Immunization Practices. J. Surg. Res. 2018, 232, 293–297. [Google Scholar] [CrossRef]
- Frandon, J.; Rodiere, M.; Arvieux, C.; Vendrell, A.; Boussat, B.; Sengel, C.; Broux, C.; Bricault, I.; Ferretti, G.; Thony, F. Blunt splenic injury: Are early adverse events related to trauma, nonoperative management, or surgery? Diagn. Interv. Radiol. 2015, 21, 327–333. [Google Scholar] [CrossRef]
- Gunn, A.J.; Raborn, J.R.; Griffin, R.; Stephens, S.W.; Richman, J.; Jansen, J.O. A pilot randomized controlled trial of endovascular coils and vascular plugs for proximal splenic artery embolization in high-grade splenic trauma. Abdom. Radiol. 2021, 46, 2823–2832. [Google Scholar] [CrossRef]
- Jambon, E.; Hocquelet, A.; Petitpierre, F.; Le Bras, Y.; Marcelin, C.; Dubuisson, V.; Grenier, N.; Cornelis, F. Proximal embolization of splenic artery in acute trauma: Comparison between Penumbra occlusion device versus coils or Amplatzer vascular plug. Diagn. Interv. Imaging 2018, 99, 801–808. [Google Scholar] [CrossRef]
- Johnson, P.; Wong, K.; Chen, Z.; Bercu, Z.L.; Newsome, J.; West, D.L.; Dariushnia, S.; Findeiss, L.K.; Kokabi, N. Meta-analysis of Intraprocedural Comparative Effectiveness of Vascular Plugs vs. Coils in Proximal Splenic Artery Embolization and Associated Patient Radiation Exposure. Curr. Probl. Diagn. Radiol. 2021, 50, 623–628. [Google Scholar] [CrossRef]
- FDA. OMNIPAQUE-Iohexol Injection, Solution. FDA Report. Available online: https://fda.report/DailyMed/ba2fb00e-ba4c-48d4-81ad-93371a63a902 (accessed on 21 December 2022).
- Boscà-Ramon, A.; Ratnam, L.; Cavenagh, T.; Chun, J.Y.; Morgan, R.; Gonsalves, M.; Das, R.; Ameli-Renani, S.; Pavlidis, V.; Hawthorn, B.; et al. Impact of site of occlusion in proximal splenic artery embolisation for blunt splenic trauma. CVIR Endovasc. 2022, 5, 43. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Imaging Findings |
|---|---|
| I | Subcapsular hematoma < 10% surface area Parenchymal laceration < 1 cm depth capsular tear |
| II | Subcapsular hematoma 10–50% surface area; intraparenchymal hematoma < 5 cm Parenchymal laceration 1–3 cm |
| III | Subcapsular hematoma > 50% surface area; ruptured subcapsular or intraparenchymal hematoma ≥ 5 cm Parenchymal laceration > 3 cm depth |
| IV | Any injury in the presence of a splenic vascular injury or active bleeding confined within the splenic capsule Parenchymal laceration involving segmental or hilar vessels producing > 25% devascularization |
| V | Any injury in the presence of a splenic vascular injury with active bleeding extended beyond the spleen into the peritoneum Shattered spleen |
| Characteristics | Patients |
|---|---|
| Sex | |
| Male | 47/57 (82.4%) |
| Female | 10/57 (17.6%) |
| Age | 31 (SD = +/−7.5 years) |
| Circumstances of injury | |
| Traffic | 35/57 (61.5%) |
| Domestic | 2/57 (3.5%) |
| Sport | 14/57 (24.6%) |
| Work | 3/57 (5.2%) |
| Other | 3/57 (5.2%) |
| AAST-OIS grade | |
| 3 | 33/57 (57.9%) |
| 4 | 23/57 (40.3%) |
| 5 | 1/57 (1.8%) |
| NISS | 19.6 (SD = +/−8.1) |
| AVP (n = 29) | POD (n = 18) | Microcoils (n = 10) | p | |
|---|---|---|---|---|
| OIS-AAST grade | ||||
| Grade 3 | 18 | 11 | 4 | 0.48 |
| Grade 4 | 10 | 7 | 6 | 0.40 |
| Grade 5 | 1 | 0 | 0 | 1 |
| Technical success (%) | 100 | 100 | 60 | <0.01 |
| Clinical efficacy (%) | 96.6 | 94.4 | 100 | 1 |
| Procedure time (min, mean +/− SD) | 52.3 (41.4) | 61.4 (39.3) | 67 (68.7) | 0.2 |
| Contrast (mL, mean +/−SD) | 57 (25.8) | 83.2 (56.4) | 88.3 (57.8) | <0.01 |
| Spleen parenchyma J30 (%, mean+/−SD) | 90.5 (11.1) | 82.8 (17.9) | 82.9 (10.3) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sammoud, S.; Ghelfi, J.; Barbois, S.; Beregi, J.-P.; Arvieux, C.; Frandon, J. Preventive Proximal Splenic Artery Embolization for High-Grade AAST-OIS Adult Spleen Trauma without Vascular Anomaly on the Initial CT Scan: Technical Aspect, Safety, and Efficacy—An Ancillary Study. J. Pers. Med. 2023, 13, 889. https://doi.org/10.3390/jpm13060889
Sammoud S, Ghelfi J, Barbois S, Beregi J-P, Arvieux C, Frandon J. Preventive Proximal Splenic Artery Embolization for High-Grade AAST-OIS Adult Spleen Trauma without Vascular Anomaly on the Initial CT Scan: Technical Aspect, Safety, and Efficacy—An Ancillary Study. Journal of Personalized Medicine. 2023; 13(6):889. https://doi.org/10.3390/jpm13060889
Chicago/Turabian StyleSammoud, Skander, Julien Ghelfi, Sandrine Barbois, Jean-Paul Beregi, Catherine Arvieux, and Julien Frandon. 2023. "Preventive Proximal Splenic Artery Embolization for High-Grade AAST-OIS Adult Spleen Trauma without Vascular Anomaly on the Initial CT Scan: Technical Aspect, Safety, and Efficacy—An Ancillary Study" Journal of Personalized Medicine 13, no. 6: 889. https://doi.org/10.3390/jpm13060889