
Effect of Arabic Qahwa on Blood Pressure in Patients with Stage One Hypertension in the Eastern Region of Saudi Arabia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.3.1. Demographic Measures
2.3.2. Clinical Parameters
2.3.3. Biochemical Parameters
2.4. Intervention
2.5. Outcome Measures
2.6. Statistical Methods
3. Results
3.1. Demographic Charecteristics
3.2. Anthropometric Measures
3.3. Clinical Measures
3.4. Biochemical Measures
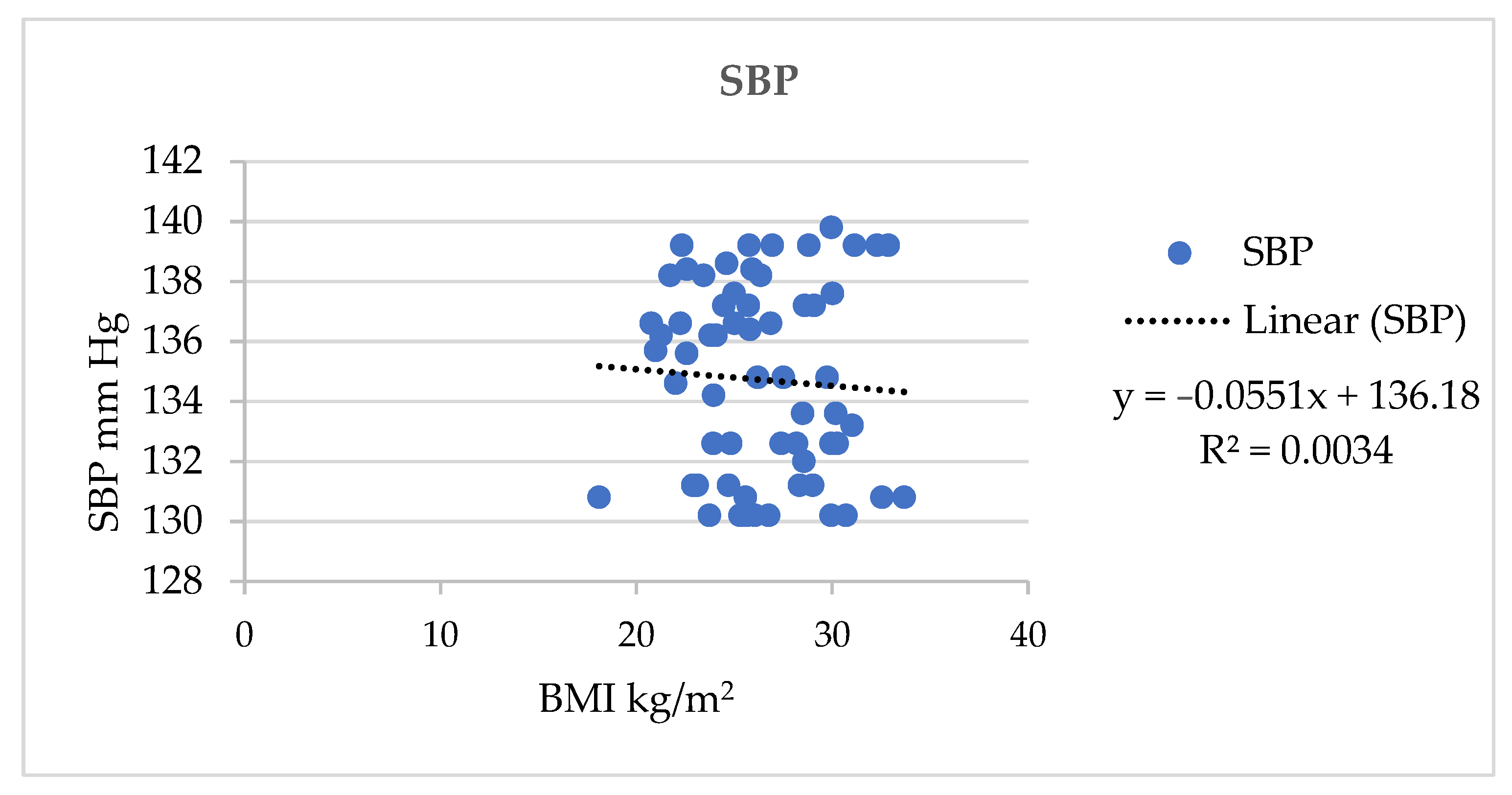
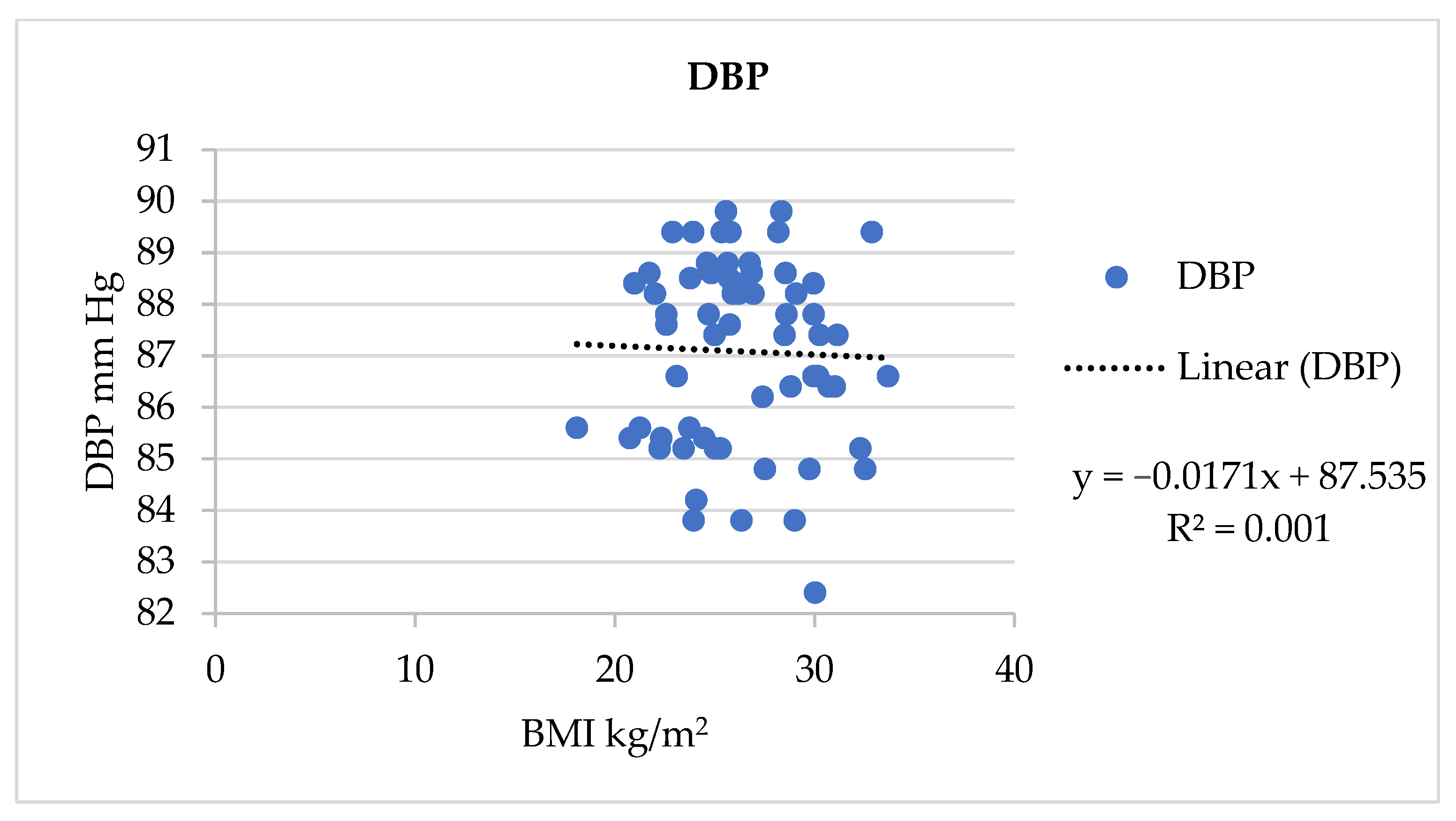
3.5. Association of BP and Demographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AQ | Arabic Qahwa |
| BMI | Body mass index |
| BP | Blood pressure |
| bpm | Beats per minute |
| DBP | Diastolic blood pressure |
| HDL | High density lipoprotein |
| HT | Hypertension |
| HR | Heart rate |
| IBM | International Business Machines Corporation |
| LDL | Low density lipoprotein |
| mm Hg | Millimetre mercury |
| MOH | Ministry of Health |
| NS | Non-significant |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
| SBP | Systolic blood pressure |
| USA | United States of America |
| WHO | World Health Organization |
References
- Aldiab, A.; Shubair, M.M.; Al-Zahrani, J.M.; Aldossari, K.K.; Al-Ghamdi, S.; Househ, M.; Razzak, H.A.; El-Metwally, A.; Jradi, H. Prevalence of hypertension and prehypertension and its associated cardioembolic risk factors; a population based cross-sectional study in Alkharj, Saudi Arabia. BMC Public Health 2018, 29, 1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation 2016, 9, 441–450. [Google Scholar] [CrossRef]
- Al-Ghamdi, S.; Alzubaidi, F.K.; Alharthai, S.A.; Alzahim, M.S.; Al Bahily, F.M.; Alsifaee, M.I.; Alshehri, H.A.; Anazi, M.S. Prevalence and correlates of diastolic dysfunction in patients with hypertension: A cross-sectional study from in the Kingdom of Saudi Arabia. Pan Afr. Med. J. 2021, 16, 159. [Google Scholar] [CrossRef]
- Bin Abdulrahman, K.A.; Khalaf, A.M.; Bin Abbas, F.B.; Alanezi, O.T. The lifestyle of Saudi medical students. Int. J. Environ. Res. Public Health 2021, 25, 7869. [Google Scholar] [CrossRef]
- El Bcheraoui, C.; Memish, Z.A.; Tuffaha, M.; Daoud, F.; Robinson, M.; Jaber, S.; Mikhitarian, S.; Al Saeedi, M.; AlMazroa, M.A.; Mokdad, A.H.; et al. Hypertension, and its associated risk factors in the Kingdom of Saudi Arabia, 2013: A national survey. Int. J. Hypertens. 2014, 2014, 564679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B.; Jose, P.O.; Pu, J.; Chung, S.; Ancheta, I.B.; Fortmann, S.P.; Palaniappan, L.P. Racial/ethnic differences in hypertension prevalence, treatment, and control for outpatients in northern California 2010–2012. Am. J. Hypertens. 2015, 28, 631–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S. Executive summary: Heart disease and stroke statistics-2012 update: A report from the American Heart Association. Circulation 2012, 125, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Jaber, S.; Mokdad, A.H.; AlMazroa, M.A.; Murray, C.J.; Al Rabeeah, A.A. Saudi burden of disease collaborators, burden of disease, injuries, and risk factors in the Kingdom of Saudi Arabia, 1990–2010. Prev. Chronic. Dis. 2014, 2, E169. [Google Scholar] [CrossRef] [Green Version]
- Sorato, M.M.; Davari, M.; Kebriaeezadeh, A.; Sarrafzadegan, N.; Shibru, T. Societal economic burden of hypertension at selected hospitals in southern Ethiopia: A patient-level analysis. BMJ Open 2022, 12, e056627. [Google Scholar] [CrossRef] [PubMed]
- Di Palo, K.E.; Barone, N.J. Hypertension and Heart Failure: Prevention, Targets, and Treatment. Heart Fail. Clin. 2020, 16, 99–106. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W., Jr.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. Joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. national heart, lung, and blood institute; national high blood pressure education program coordinating committee. seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [Green Version]
- Missriya, M.A.S.; John, J. Assess the prevalence of hypertension and knowledge regarding the prevention of stroke. Asian J. Pharm. Clin. Res. 2017, 10, 177–180. [Google Scholar] [CrossRef]
- Borghi, C.; Fogacci, F.; Agnoletti, D.; Cicero, A.F.G. Hypertension and Dyslipidemia Combined Therapeutic Approaches. High Blood Press. Cardiovasc. Prev. 2022, 29, 221–230. [Google Scholar] [CrossRef]
- Alzoman, H.; Alzahrani, A.; Alwehaiby, K.; Alanazi, W.; AlSarhan, M. Efficacy of arabic coffee and black tea in reducing halitosis: A randomized, double-blind, controlled, crossover clinical trial. Healthcare 2021, 9, 250. [Google Scholar] [CrossRef] [PubMed]
- Saudi Coffee Industry to Join Top Table of Global Producers. Arab News [Internet]. Available online: https://www.arabnews.com/node/2277846/business-economy (accessed on 31 March 2023).
- Alfawaz, H.A.; Khan, N.; Yakout, S.M.; Khattak, M.N.K.; Alsaikhan, A.A.; Almousa, A.A.; Alsuwailem, T.A.; Almjlad, T.M.; Alamri, N.A.; Alshammari, S.G.; et al. Prevalence, predictors, and awareness of coffee consumption and its trend among saudi female students. Int. J. Environ. Res. Public Health 2020, 17, 7020. [Google Scholar] [CrossRef] [PubMed]
- Capek, P.; Paulovičová, E.; Matulová, M.; Mislovičová, D.; Navarini, L.; Suggi-Liverani, F. Coffea arabica instant coffee--chemical view and immunomodulating properties. Carbohydr. Polym. 2014, 15, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Das, I.; Singh, S.; Saha, T. Chemopreventive properties of indole-3-carbinol, diindolylmethane and other constituents of cardamom against carcinogenesis. Recent Pat. Food Nutr. Agric. 2010, 2, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Tasew, T.; Mekonnen, Y.; Gelana, T.; Redi-Abshiro, M.; Chandravanshi, B.S.; Ele, E.; Mohammed, A.M.; Mamo, H. In vitro antibacterial and antioxidant activities of roasted and green coffee beans originating from different regions of Ethiopia. Int. J. Food Sci. 2020, 25, 8490492. [Google Scholar] [CrossRef]
- Habib, S.S.; Ahmed, S.M.; Al Hadlaq, A.; Marzouk, A. Effect of drinking Arabian qahwa on fractional exhaled nitric oxide levels in healthy nonsmoking Saudi adults. Ann. Thorac. Med. 2012, 7, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Jain, V.; Katewa, S.S. Blood pressure lowering, fibrinolysis enhancing and antioxidant activities of cardamom (Elettaria cardamomum). Indian J. Biochem. Biophys. 2009, 46, 503–506. [Google Scholar]
- Hermanussen, M.; Stec, K.; ABmann, C.; Meigen, C.; Van Buuren, S. Synthetic growth reference charts. Am. J. Hum. Biol. 2016, 28, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Awaad, A.S.; Soliman, G.A.; Al-Outhman, M.R.; Al-Shdoukhi, I.F.; Al-Nafisah, R.S.; Al-Shamery, J.; Al-Samkhan, R.; Baqer, M.; Al-Jaber, N.A. The effect of four coffee types on normotensive rats and normal/hypertensive human volunteers. Phytother. Res. 2011, 25, 803–808. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Orozco-Arbeláez, E.; Leon-Muñoz, L.M.; Guallar-Castillon, P.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Habitual coffee consumption and 24-h blood pressure control in older adults with hypertension. Clin. Nutr. 2016, 35, 1457–1463. [Google Scholar] [CrossRef]
- Surma, S.; Oparil, S. Coffee and arterial hypertension. Curr. Hypertens. Rep. 2021, 23, 38. [Google Scholar] [CrossRef] [PubMed]
- Rezq, A.A.; Qadhi, A.H.; Almasmoum, A.; Ghafouri, K.J. Effect of Arabian coffee (saudi coffee) consumption on body mass index, blood glucose level and blood pressure in some people of Makkah Region, KSA. Kasmera J. 2020, 48, 62–70. [Google Scholar] [CrossRef]
- Badkook, M.M.; Shrourou, R.M. Arabic coffee with two doses of cardamom: Effects on health biomarkers in healthy women. Int. J. Nutr. Food Sci. 2013, 2, 280–286. [Google Scholar] [CrossRef]
- Gebeyehu, G.M.; Feleke, D.G.; Molla, M.D.; Admasu, T.D. Effect of habitual consumption of Ethiopian Arabica coffee on the risk of cardiovascular diseases among non-diabetic healthy adults. Heliyon 2020, 6, e04886. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-Ochoa, G.M.; Pulgarín-Zapata, I.C.; Velásquez-Rodriguez, C.M.; Duque-Ramírez, M.; Naranjo-Cano, M.; Quintero-Ortiz, M.M.; Lara-Guzmán, O.J.; Muñoz-Durango, K. Coffee consumption increases the antioxidant capacity of plasma and has no effect on the lipid profile or vascular function in healthy adults in a randomized controlled trial. J. Nutr. 2016, 146, 524–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, L.; Ma, D.; Zhang, Y.; Liu, Z.; Wang, P. The effect of coffee consumption on serum lipids: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2012, 66, 872–877. [Google Scholar] [CrossRef]
- Hino, A.; Adachi, H.; Enomoto, M.; Furuki, K.; Shigetoh, Y.; Ohtsuka, M.; Kumagae, S.; Hirai, Y.; Jalaldin, A.; Satoh, A.; et al. Habitual coffee but not green tea consumption is inversely associated with metabolic syndrome: An epidemiological study in a general Japanese population. Diabetes Res. Clin. Pract. 2007, 76, 383–389. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Hu, G.; Bidel, S.; Lindström, J.; Jousilahti, P. Coffee consumption and risk of type 2 diabetes mellitus among middle-aged Finnish men and women. J. Am. Med. Assoc. 2004, 291, 1213–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Marventano, S.; Galvano, F.; Pajak, A.; Mistretta, A. Factors associated with metabolic syndrome in a mediterranean population: Role of caffeinated beverages. J. Epidemiol. 2014, 24, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linderman, G.C.; Lu, J.; Lu, Y.; Sun, X.; Xu, W.; Nasir, K.; Schulz, W.; Jiang, L.; Krumholz, H.M. Association of body mass index with blood pressure among 1.7 million Chinese adults. JAMA Netw. Open 2018, 1, e181271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranasinghe, P.; Cooray, D.N.; Jayawardena, R.; Katulanda, P. The influence of family history of hypertension on disease prevalence and associated metabolic risk factors among Sri Lankan adults. BMC Public Health 2015, 15, 576. [Google Scholar] [CrossRef] [Green Version]
- Jalloun, R.A.; Alhathlool, M.H. Arabic coffee consumption and the risk of obesity among Saudi’s female population. J. Saud. Soc. Food Nutr. 2020, 13, 59–67. [Google Scholar]
- Alawadh, R.A.; Abid, N.; Alsaad, A.S.; Aljohar, H.I.; Alharbi, M.M.; Alhussain, F.K. Arabic Coffee consumption, and its correlation to obesity among the general population in the eastern province, Kingdom of Saudi Arabia. Cureus 2022, 14, e30848. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.Y.; Kim, J. Coffee consumption, and the risk of obesity in Korean Women. Nutrients 2017, 9, 1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naser, L.R.; Sameh, A.; Muzaffar, I.; Omar, A.R.; Ahmed, M.A. Comparative evaluation of caffeine content in Arabian coffee with other caffeine beverages. Afr. J. Pharm. Pharmacol. 2018, 12, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Alkaabi, J.; Al-Dabbagh, B.; Saadi, H.; Gariballa, S.; Yasin, J. Effect of traditional Arabic coffee consumption on the glycemic index of Khalas dates tested in healthy and diabetic subjects. Asia Pac. J. Clin. Nutr. 2013, 22, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Al-Mssallem, M.Q.; Brown, J.E. Arabic coffee increases the glycemic index but not insulinemic index of dates. Saudi Med. J. 2013, 34, 923–928. [Google Scholar] [PubMed]
- Bouchard, D.R.; Ross, R.; Janssen, I. Coffee, tea, and their additives: Association with BMI and waist circumference. Obes. Facts 2010, 3, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.O. Dates fruits effects on blood glucose among patients with diabetes mellitus: A review and meta-analysis. Pak. J. Med. Sci. 2021, 37, 1230–1236. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | AQ (n = 62) | Control (n = 64) | p Value | |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Age | 20–30 years | 3 (5) | 4 (6) | 0.869 |
| 31–40 years | 12 (19) | 15 (24) | ||
| 41–50 years | 28 (45) | 29 (45) | ||
| 51–59 years | 19 (31) | 16 (25) | ||
| Gender | Male | 34 (55) | 32 (50) | 0.587 |
| Female | 28 (45) | 32 (50) | ||
| Educational level | Primary | 4 (6) | 5 (8) | 0.547 |
| High school | 14 (23) | 20 (31) | ||
| Higher secondary | 34 (55) | 27(42) | ||
| Graduate | 10 (16) | 12 (19) | ||
| Employment status | Employed | 39 (63) | 34 (53) | 0.266 |
| Unemployed | 23 (37) | 30 (47) | ||
| Marital status | Unmarried | 2 (3) | 5 (8) | 0.261 |
| Married | 60 (97) | 59 (92) | ||
| Diet pattern | Vegetarian | 13 (21) | 19 (30) | 0.261 |
| Non-vegetarian | 49 (79) | 45 (70) | ||
| Family history of HT | Yes | 27 (43) | 26 (41) | |
| No | 35 (57) | 38 (59) | 0.74 | |
| Measurements | AQ Group (n = 62) | Control (n = 64) | ||||
|---|---|---|---|---|---|---|
| Pre-Test Mean (SD) | Post-Test Mean (SD) | Paired ‘t’ Test | Pre-Test Mean (SD) | Post-Test Mean (SD) | Paired ‘t’ Test | |
| SBP (mm Hg) | 134.72 ± 3.23 | 133.14 ± 3.69 | t = 8.397; p = 0.009 * | 136.49 ± 2.97 | 136.72 ± 2.79 | t = 0.984; p = 0.329 NS |
| DBP (mm Hg) | 87.08 ± 1.8 | 85.98 ± 1.95 | t = 9.069; p = 0.0001 * | 87.08 ± 1.79 | 87.19 ± 1.92 | t = 0.684; p = 0.497 NS |
| HR (bpm) | 78.13 ± 5.02 | 77.21 ± 4.82 | t = 1.8376; p = 0.7099 NS | 78.41 ± 5.16 | 78.55 ± 5.25 | t = 0.4695; p = 0.643 NS |
| Measurements | AQ Group (n = 62) | Control (n = 64) | ||||
|---|---|---|---|---|---|---|
| Pre-Test Mean (SD) | Post-Test Mean (SD) | Paired ‘t’ Test | Pre-Test Mean (SD) | Post-Test Mean (SD) | Paired ‘t’ Test | |
| Triglyceride (mg/dL) | 115.28 ± 9.72 | 113.25 ± 10.2 | t = 7.2117; p = 0.0001 * | 115.87 ± 10.03 | 115.84 ± 9.94 | t = 0.0361; p = 0.9713 NS |
| LDL (mg/dL) | 99.95 ± 3.41 | 98.76 ± 3.27 | t = 6.636; p = 0.0001 * | 99.74 ± 3.43 | 100.12 ± 3.997 | t = 0.7717; p = 0.4434 NS |
| HDL (mg/dL) | 42.35 ± 5.003 | 53.45 ± 3.4 | t = 6.4034 p = 0.0001 * | 42.01 ± 5.096 | 42.53 ± 5.24 | t = 1.9404; p = 0.05711 NS |
| Demographic Characteristics | AQ (n = 62) N (%) | SBP Mean Score | p Value | DBP Mean Score | p Value | |
|---|---|---|---|---|---|---|
| Age | 20–30 years | 3 (5) | 132.13 | 0.1621 | 87.3 | 0.1194 |
| 31–40 years | 12 (19) | 131.13 | NS | 86.89 | NS | |
| 41–50 years | 28 (45) | 133.5 | 85.84 | |||
| 51–59 years | 19 (31) | 134.03 | 85.41 | |||
| Gender | Male | 34 (55) | 132.59 | 0.2992 | 85.61 | 0.1027 |
| Female | 28 (45) | 133.58 | NS | 86.43 | NS | |
| Educational Level | Primary | 4 (6) | 133.95 | 0.3637 | 87.55 | 0.1295 |
| High school | 14 (23) | 131.59 | NS | 86.44 | NS | |
| Higher secondary | 34 (55) | 133.55 | 85.87 | |||
| Graduate | 10 (16) | 133.58 | 85.08 | |||
| Employment Status | Employed | 39 (63) | 133.43 | 0.4193 | 86.25 | 0.1539 |
| Unemployed | 23 (37) | 132.64 | NS | 85.52 | NS | |
| Marital Status | Unmarried | 2 (3) | 130.7 | 0.3469 | 86.00 | 0.6207 |
| Married | 60 (97) | 133.22 | NS | 85.3 | NS | |
| Diet Pattern | Vegetarian | 13 (21) | 133.5 | 0.6936 | 85.49 | 0.3153 |
| Non-vegetarian | 49 (79) | 133.04 | NS | 86.11 | NS | |
| Family history of HT | Yes | 27 (43) | 133.5 | 0.0412 * | 85.46 | 0.0428 * |
| No | 35 (57) | 133.86 | 86.38 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jalal, S.M.; Alsebeiy, S.H.; Aleid, H.A.; Alhamad, S.A. Effect of Arabic Qahwa on Blood Pressure in Patients with Stage One Hypertension in the Eastern Region of Saudi Arabia. J. Pers. Med. 2023, 13, 1011. https://doi.org/10.3390/jpm13061011
Jalal SM, Alsebeiy SH, Aleid HA, Alhamad SA. Effect of Arabic Qahwa on Blood Pressure in Patients with Stage One Hypertension in the Eastern Region of Saudi Arabia. Journal of Personalized Medicine. 2023; 13(6):1011. https://doi.org/10.3390/jpm13061011
Chicago/Turabian StyleJalal, Sahbanathul Missiriya, Saad Hamoud Alsebeiy, Hamida Ali Aleid, and Sukinah Ali Alhamad. 2023. "Effect of Arabic Qahwa on Blood Pressure in Patients with Stage One Hypertension in the Eastern Region of Saudi Arabia" Journal of Personalized Medicine 13, no. 6: 1011. https://doi.org/10.3390/jpm13061011