
Local Treatment of Triple-Negative Breast Cancer: Is Mastectomy Superior to Breast-Conserving Surgery?

 , ,
, ,  , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
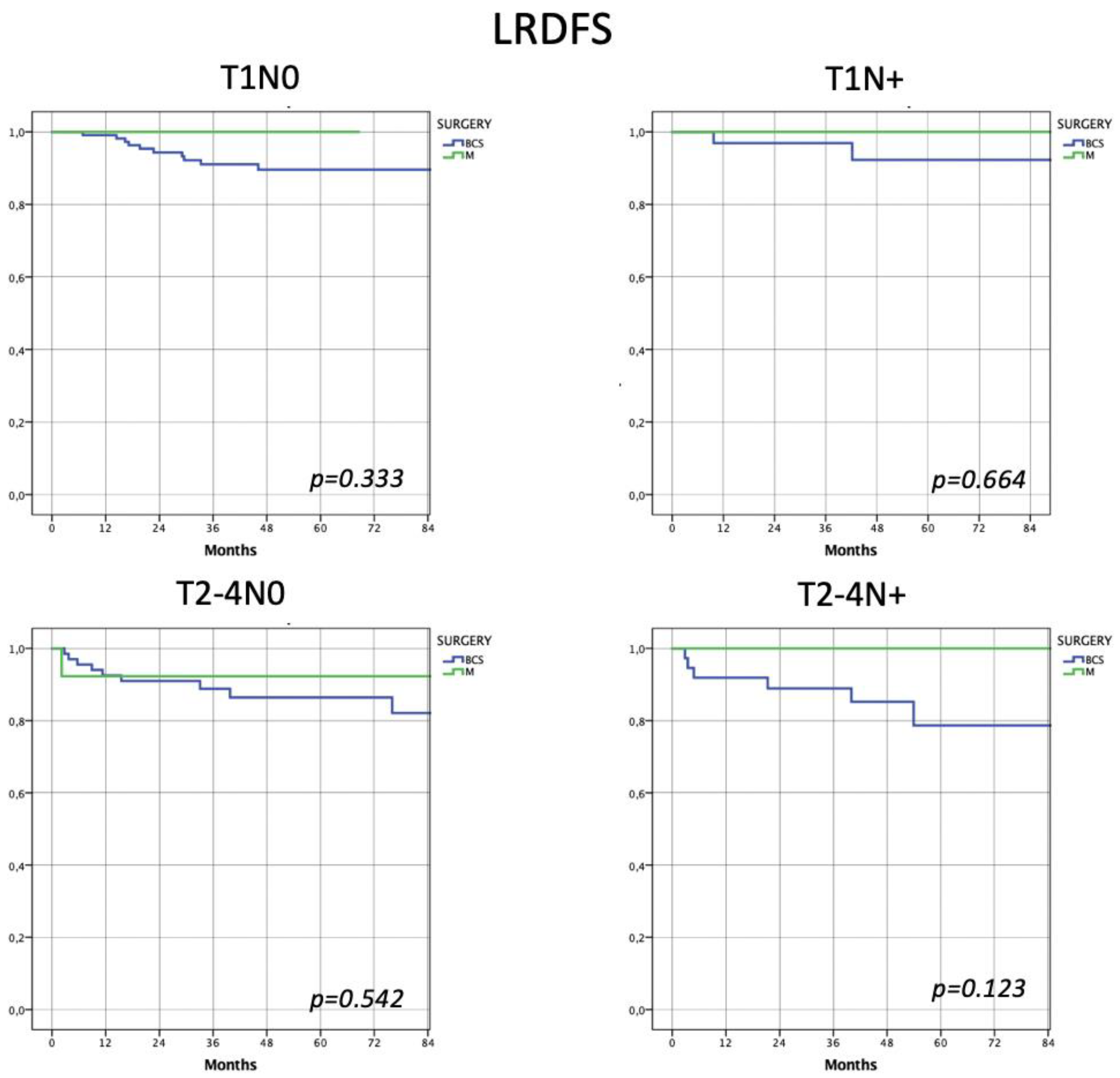
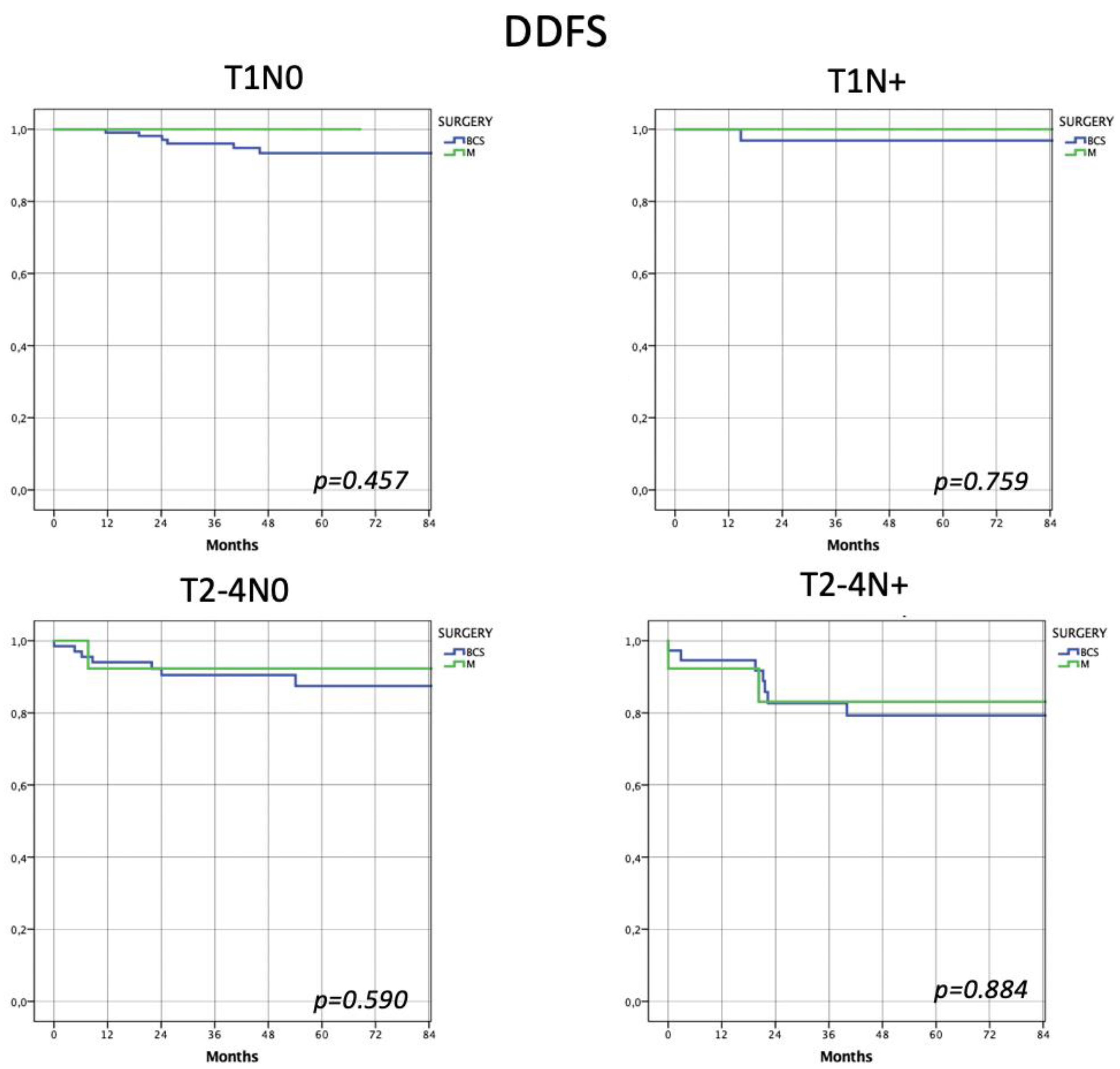
Oncological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Leone, A.; Fragomeni, S.M.; Scardina, L.; Ionta, L.; Mulè, A.; Magno, S.; Terribile, D.; Masetti, R.; Franceschini, G. Androgen receptor expression and outcome of neoadjuvant chemotherapy in triple-negative breast cancer. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1910–1915. [Google Scholar] [CrossRef]
- Pavese, F.; Capoluongo, E.D.; Muratore, M.; Minucci, A.; Santonocito, C.; Fuso, P.; Concolino, P.; Di Stasio, E.; Carbognin, L.; Tiberi, G.; et al. BRCA Mutation Status in Triple-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy: A Pivotal Role for Treatment Decision-Making. Cancers 2022, 14, 4571. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef]
- De Paolis, E.; Paris, I.; Tilocca, B.; Roncada, P.; Foca, L.; Tiberi, G.; D’angelo, T.; Pavese, F.; Muratore, M.; Carbognin, L.; et al. Assessing the pathogenicity of BRCA1/2 variants of unknown significance: Relevance and challenges for breast cancer precision medicine. Front. Oncol. 2023, 12, 1053035. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Pappas, L.; Neumayer, L.; Kokeny, K.; Agarwal, J. Effect of breast conservation therapy vs mastectomy on disease-specific survival for early-stage breast cancer. JAMA Surg. 2014, 149, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.S. Radiation therapy in the locoregional treatment of triple-negative breast cancer. Lancet Oncol. 2015, 16, e113–e122. [Google Scholar] [CrossRef]
- Wahba, H.A.; El-Hadaad, H.A. Current approaches in treatment of triple-negative breast cancer. Cancer Biol. Med. 2015, 12, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. NCCN Clinical Practice Guidelines in Oncology, Breast Cancer, Version 3. 2022. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Franceschini, G.; Terribile, D.; Fabbri, C.; Di Leone, A.; Masetti, R. Management of locally advanced breast cancer: Mini-review. Minerva Chir. 2007, 62, 249–255. [Google Scholar]
- Franceschini, G.; Di Leone, A.; Natale, M.; Sanchez, M.A.; Masett, R. Conservative surgery after neoadjuvant chemotherapy in patients with operable breast cancer. Ann. Ital. di Chir. 2018, 89, 290. [Google Scholar]
- Garufi, G.; Carbognin, L.; Schettini, F.; Seguí, E.; Di Leone, A.; Franco, A.; Paris, I.; Scambia, G.; Tortora, G.; Fabi, A. Updated Neoadjuvant Treatment Landscape for Early Triple Negative Breast Cancer: Immunotherapy, Potential Predictive Biomarkers, and Novel Agents. Cancers 2022, 14, 4064. [Google Scholar] [CrossRef]
- Yi, J.C.; Syrjala, K.L. Anxiety and depression in cancer survivors. Med. Clin. N. Am. 2017, 101, 1099–1113. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Scardina, L.; Visconti, G.; Hayashi, A.; Masetti, R. Editorial: Update of Current Evidences in Breast Cancer Surgery. Front. Oncol. 2022, 12, 928467. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, C.; Schmitz, K.; Lazovich, D.; Virnig, B.A.; Wallace, R.B.; Folsom, A.R. Functional limitations in elderly female cancer survivors. Gynecol. Oncol. 2006, 98, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Adkins, F.C.; Gonzalez-Angulo, A.M.; Lei, X.; Hernandez-Aya, L.F.; Mittendorf, E.A.; Litton, J.K.; Wagner, J.; Hunt, K.K.; Woodward, W.A.; Meric-Bernstam, F. Triple-negative breast cancer is not a contraindication for breast conservation. Ann. Surg. Oncol. 2011, 18, 3164–3173. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.X.; Wang, X.X.; Lin, P.Y.; Zhang, J.; Li, J.J.; Song, C.G.; Shao, Z.M. The different outcomes between breast-conserving surgery and mastectomy in triple-negative breast cancer: A population-based study from the SEER 18 database. Oncotarget 2017, 8, 4773–4780. [Google Scholar] [CrossRef]
- Arvold, N.D.; Taghian, A.G.; Niemierko, A.; Raad, R.F.A.; Sreedhara, M.; Nguyen, P.L.; Bellon, J.R.; Wong, J.S.; Smith, B.L.; Harris, J.R. Age, breast cancer subtype approximation, and local recurrence after breast-conserving therapy. J. Clin. Oncol. 2011, 29, 3885–3891. [Google Scholar] [CrossRef]
- Zaky, S.S.; Lund, M.; May, K.A.; Godette, K.D.; Beitler, J.J.; Holmes, L.R.; O’regan, R.M.; Yu, E.S.; Yu, D.S.; Landry, J.C. The negative effect of triple-negative breast cancer on outcome after breast-conserving therapy. Ann. Surg. Oncol. 2011, 18, 2858–2865. [Google Scholar] [CrossRef]
- Fancellu, A.; Houssami, N.; Sanna, V.; Porcu, A.; Ninniri, C.; Marinovich, M.L. Outcomes after breast-conserving surgery or mastectomy in patients with triple-negative breast cancer: Meta-analysis. Br. J. Surg. 2021, 108, 760–768. [Google Scholar] [CrossRef]
- Wang, J.; Xie, X.; Wang, X.; Tang, J.; Pan, Q.; Zhang, Y.; Di, M. Locoregional and distant recurrences after breast conserving therapy in patients with triple-negative breast cancer: A meta-analysis. Surg. Oncol. 2013, 22, 247–255. [Google Scholar] [CrossRef]
- Gangi, A.; Chung, A.; Mirocha, J.; Liou, D.Z.; Leong, T.; Giuliano, A.E. Breast-conserving therapy for triple-negative breast cancer. JAMA Surg. 2014, 149, 252–258. [Google Scholar] [CrossRef]
- Saifi, O.; Chahrour, M.A.; Li, Z.; Hoballah, J.; Panoff, J.; Vallow, L.A.; Zeidan, Y.H. Is breast conservation superior to mastectomy in early stage triple negative breast cancer? Breast 2022, 62, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Masetti, R.; D’Ugo, D.; Belli, P.; Picciocchi, A. Synchronous bilateral Paget’s disease of the nipple associated with bilateral breast carcinoma. Breast J. 2005, 11, 355–356. [Google Scholar] [CrossRef]
- Di Leone, A.; Franco, A.; Terribile, D.A.; Magno, S.; Fabi, A.; Sanchez, A.M.; D’archi, S.; Scardina, L.; Natale, M.; Mason, E.J.; et al. Level II Oncoplastic Surgery as an Alternative Option to Mastectomy with Immediate Breast Reconstruction in the Neoadjuvant Setting: A Multidisciplinary Single Center Experience. Cancers 2022, 14, 1275. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Zheng, Y.; Yao, J.; Liu, Y.; Ruan, J.; Deng, Y.; Zhou, L.; Zhao, P.; Yang, S.; Hu, J.; et al. Evaluation of Adjuvant Treatments for T1 N0 M0 Triple-Negative Breast Cancer. JAMA Netw. Open 2020, 3, e2021881. [Google Scholar] [CrossRef] [PubMed]
- Bessa, J.D.F.; Marta, G.N. Triple-negative breast cancer and radiation therapy. Rep. Pr. Oncol. Radiother. 2022, 27, 545–551. [Google Scholar] [CrossRef]
- Zheng, Y.-Z.; Liu, Y.; Deng, Z.-H.; Liu, G.-W.; Xie, N. Determining prognostic factors and optimal surgical intervention for early-onset triple-negative breast cancer. Front. Oncol. 2022, 12, 910765. [Google Scholar] [CrossRef]
- Nardone, L.; Valentini, V.; Marino, L.; De Santis, M.C.; Terribile, D.; Franceschini, G.; Balducci, M.; Mantini, G.; Mattiucci, G.; Mulè, A.; et al. A Feasibility Study of Neo-Adjuvant Low-Dose Fractionated Radiotherapy with Two Different Concurrent Anthracycline-Docetaxel Schedules in Stage IIA/B-IIIA Breast Cancer. Tumori J. 2012, 98, 79–85. [Google Scholar] [CrossRef]
- Chen, H.; Wu, J.; Zhang, Z.; Tang, Y.; Li, X.; Liu, S.; Cao, S.; Li, X. Association Between BRCA Status and Triple-Negative Breast Cancer: A Meta-Analysis. Front. Pharmacol. 2018, 9, 909. [Google Scholar] [CrossRef]
- Solin, L.J.; Hwang, W.-T.; Vapiwala, N. Outcome after breast conservation treatment with radiation for women with triple-negative early-stage invasive breast carcinoma. Clin. Breast Cancer 2009, 9, 96–100. [Google Scholar] [CrossRef]
- Akbari, M.E.; Khayamzadeh, M.; Mirzaei, H.R.; Moradi, A.; Akbari, A.; Moradian, F.; Khalili, N. Saving the Breast Saves the Lives of Breast Cancer Patients. Int. J. Surg. Oncol. 2020, 2020, 8709231. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Conservative breast surgery | 247 (85.5%) |
| 227 (78.5%) |
| 20 (6.9%) |
| Mastectomy | 42 (14.5%) |
| 25 (8.7%) |
| 17 (5.9%) |
| Characteristics | All 289 Patients | BCS 247 (85.5%) | M 42 (14.5%) | Significance |
|---|---|---|---|---|
| Mean age (years) | 59.6 ± 14.2 (57.9–61.2) | 59.6 ± 13.9 (57.9–61.4) | 58.8 ± 15.8 (53.9–63.8) | p = 0.738 |
| Menopausal status | 207 (71.6%) | 176 (71.3%) | 31 (73.8%) | p = 0.854 |
| BRCA 1/2 pathological mutations | 31 (10.7%) | 22 (8.9%) | 9 (21.4%) | p = 0.027 |
| Multifocality/multicentricity | 38 (13.1%) | 29 (11.7%) | 9 (21.4%) | p = 0.134 |
| Tumor size (mm) | 20.8 ± 13.8 (19.1–22.4) | 18.9 ± 10.3 (17.6–20.3) | 32.4 ± 23.8 (24.4–40.3) | p < 0.0001 |
Istotype
| 200 (69.2%) 2 (0.7%) 44 (15.2%) 43 (14.9%) | 165 (66.8%) 2 (0.8%) 37 (15.0%) 43 (17.4%) | 35 (83.3%) 0 (0%) 7 (16.7%) 0 (0%) | p = 0.006 |
Grading
| 10 (3.5%) 51 (17.6%) 182 (63.0%) 46 (15.9%) | 9 (3.6%) 45 (18.2%) 148 (59.9%) 45 (18.2%) | 1 (2.4%) 6 (14.2%) 34 (81.0%) 1 (2.4%) | p = 0.019 |
DCIS
| 53 (18.3%) 236 (81.7%) | 46 (18.6%) 201 (81.4%) | 7 (16.7%) 35 (83.3%) | p = 0.833 |
pT
| 158 (54.7%) 14 (39.4%) 8 (2.8%) 9 (3.1%) | 143 (57.9%) 96 (38.9%) 3 (1.2%) 5 (2.0%) | 15 (35.7%) 18 (42.9%) 5 (11.9%) 4 (9.5%) | p < 0.0001 |
pN
| 221 (78.6%) 45 (16.0%) 11 (3.9%) 4 (1.4%) | 185 (77.4%) 41 (17.2%) 9 (3.8%) 4 (1.6%) | 36 (85.7%) 4 (9.5%) 2 (4.8%) 0 (0%) | p = 0.568 |
| All 289 Patients | BCS 247 (85.5%) | M 42 (14.5%) | p-Value | |
|---|---|---|---|---|
Subclasses
| 123 (42.6%) 36 (12.5%) 80 (27.7%) 50 (17.3%) | 111 (44.9%) 32 (13.0%) 67 (27.1%) 37 (15.0%) | 12 (28.5%) 4 (9.5%) 13 (31.0%) 13 (31.0%) | p = 0.052 |
| Characteristics | Univariate Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| OR | p Value | 95% CI | OR | p Value | 95% CI | |
| Menopausal status | 1.316 | 0.561 | 0.522–3.317 | |||
| BRCA pathological mutations | 0.352 | 0.306 | 0.048–2.603 | |||
| Istotype | 1.061 | 0.719 | 0.768–1.466 | |||
| Grading | 1.367 | 0.300 | 0.757–2.468 | |||
| cT | ||||||
| 6.092 | 0.078 | 0.818–45.352 | |||
| 0.238 | 0.238 | 0.032–1.759 | |||
| 0838 | 0.672 | 0.370–1.897 | |||
| 1.859 | 0.122 | 0.848–4.075 | |||
| cN | 1.280 | 0.591 | 0.520–3.150 | |||
Kind of surgery
| 1.172 0.853 | 0.796 0.796 | 0.351–3.918 0.255–2.851 | |||
pT
| 0.303 2.359 4.087 1.427 | 0.007 0.036 0.057 0.728 | 0.127–0.726 1.060–5.251 0.959–17.411 0.193–10.575 | 0.228 0.728 | 0.034 0.622 | 0.058–0.898 0.205–2.578 |
pN
| 0.868 0.704 1.002 6.633 | 0.762 0.569 0.999 0.010 | 0.346–2.174 0.211–2.354 0.135–7.422 1.560–28.210 | 6.599 | 0.012 | 1.511–28.818 |
| Outcomes | BCS (247–85.5%) | M (42–14.5%) | Significance |
|---|---|---|---|
| LR-DFS | 27 (9.3%) | 1 (0.3%) | p = 0.095 |
| 86.3% | 97.6% | LR = 0.103 | |
| DDFS | 22 (7.6%) | 4 (1.4%) | p = 0.778 |
| 88.3% | 92.1% | LR = 0.796 | |
| OS | 17 (5.9%) | 2 (0.7%) | p = 0.748 |
| 69.2% | 93.3% | LR = 0.652 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Leone, A.; Franco, A.; Zotta, F.; Scardina, L.; Sicignano, M.; Di Guglielmo, E.; Castagnetta, V.; Magno, S.; Terribile, D.; Sanchez, A.M.; et al. Local Treatment of Triple-Negative Breast Cancer: Is Mastectomy Superior to Breast-Conserving Surgery? J. Pers. Med. 2023, 13, 865. https://doi.org/10.3390/jpm13050865
Di Leone A, Franco A, Zotta F, Scardina L, Sicignano M, Di Guglielmo E, Castagnetta V, Magno S, Terribile D, Sanchez AM, et al. Local Treatment of Triple-Negative Breast Cancer: Is Mastectomy Superior to Breast-Conserving Surgery? Journal of Personalized Medicine. 2023; 13(5):865. https://doi.org/10.3390/jpm13050865
Chicago/Turabian StyleDi Leone, Alba, Antonio Franco, Francesca Zotta, Lorenzo Scardina, Margherita Sicignano, Enrico Di Guglielmo, Virginia Castagnetta, Stefano Magno, Daniela Terribile, Alejandro Martin Sanchez, and et al. 2023. "Local Treatment of Triple-Negative Breast Cancer: Is Mastectomy Superior to Breast-Conserving Surgery?" Journal of Personalized Medicine 13, no. 5: 865. https://doi.org/10.3390/jpm13050865