
Five-to-Fifteen—Parental Perception of Developmental Profile from Age 5 to 8 Years in Children Born Very Preterm
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
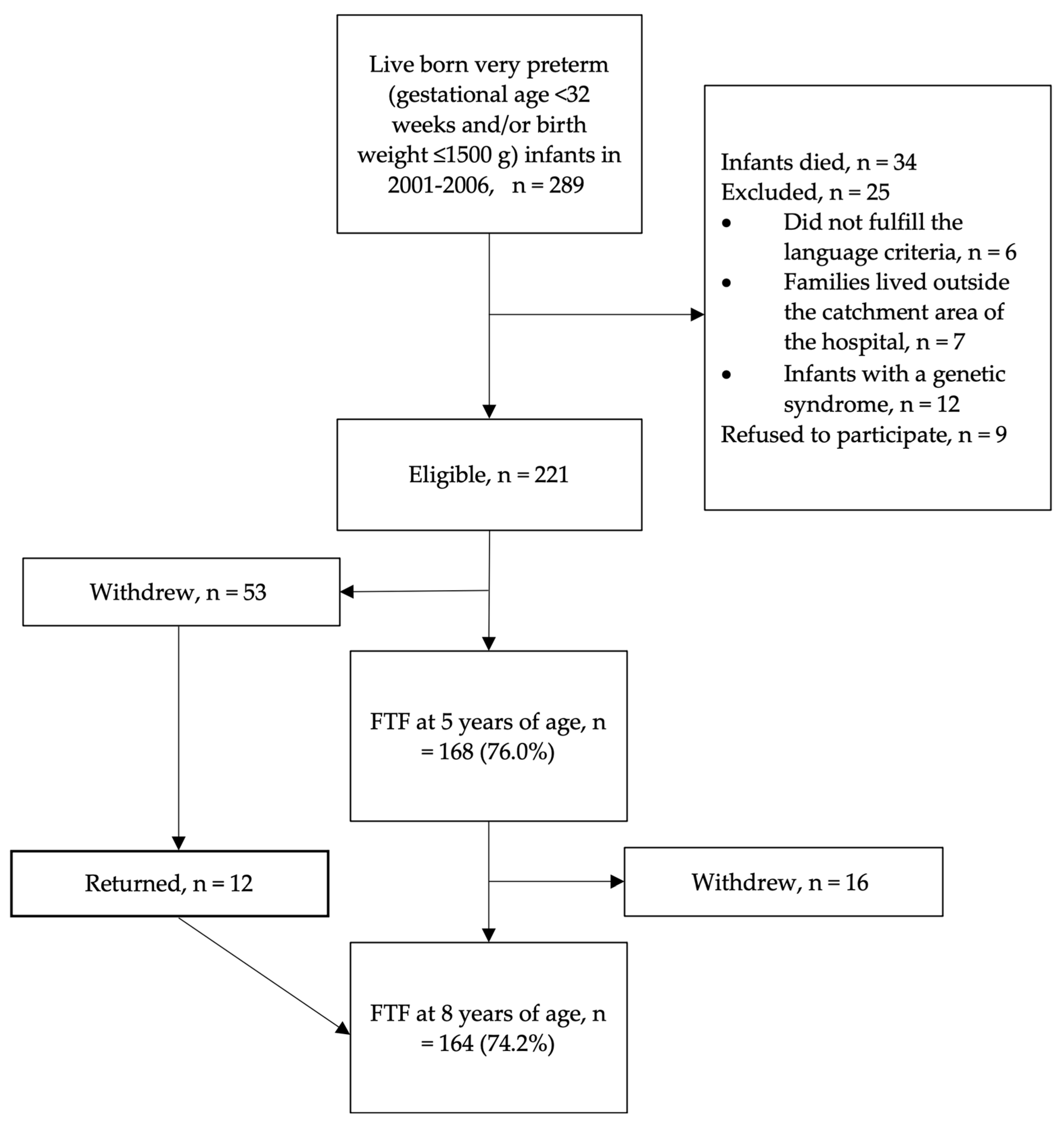
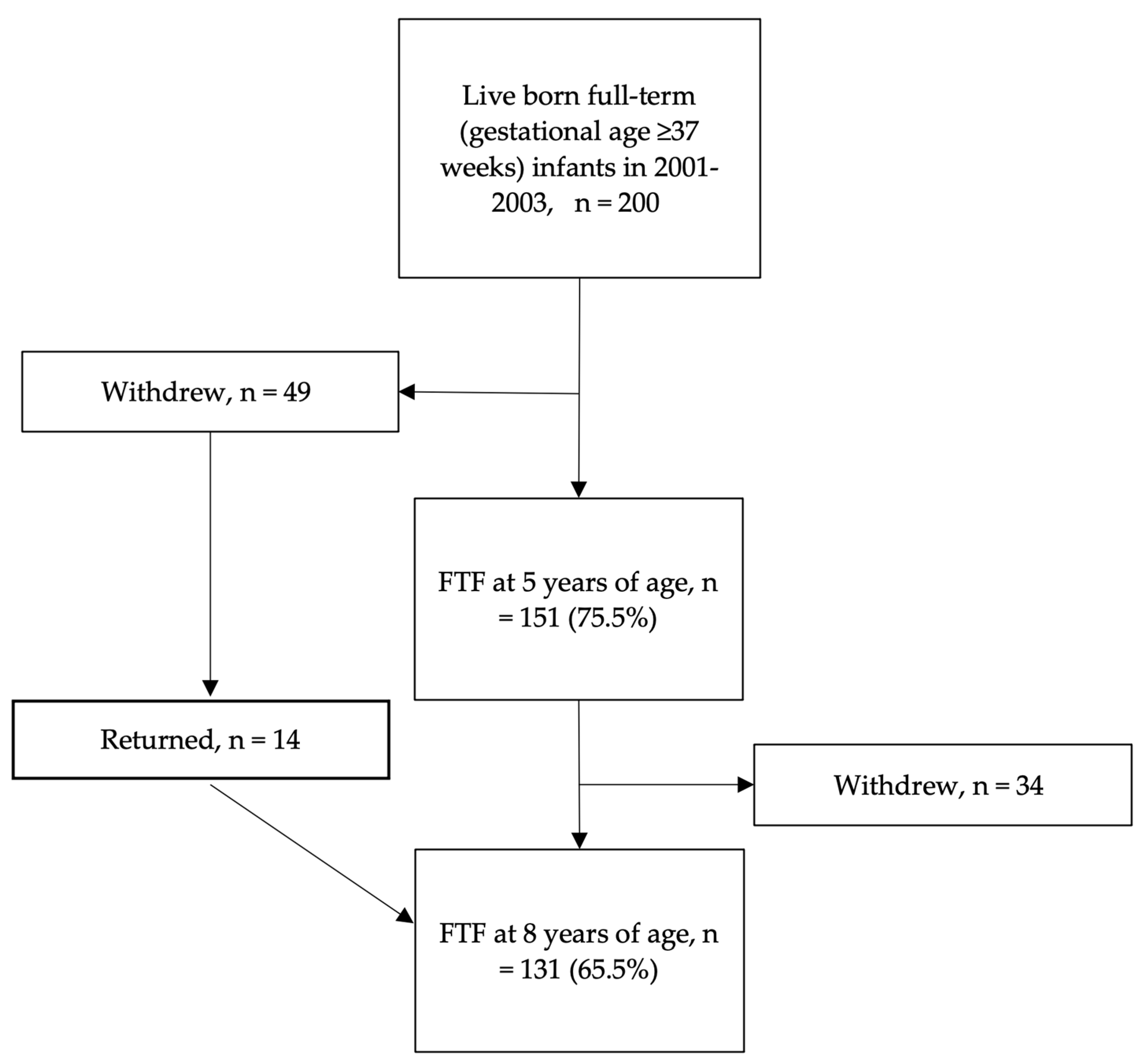
2.2. Participants
2.3. Evaluations
2.4. Data Analysis
3. Results
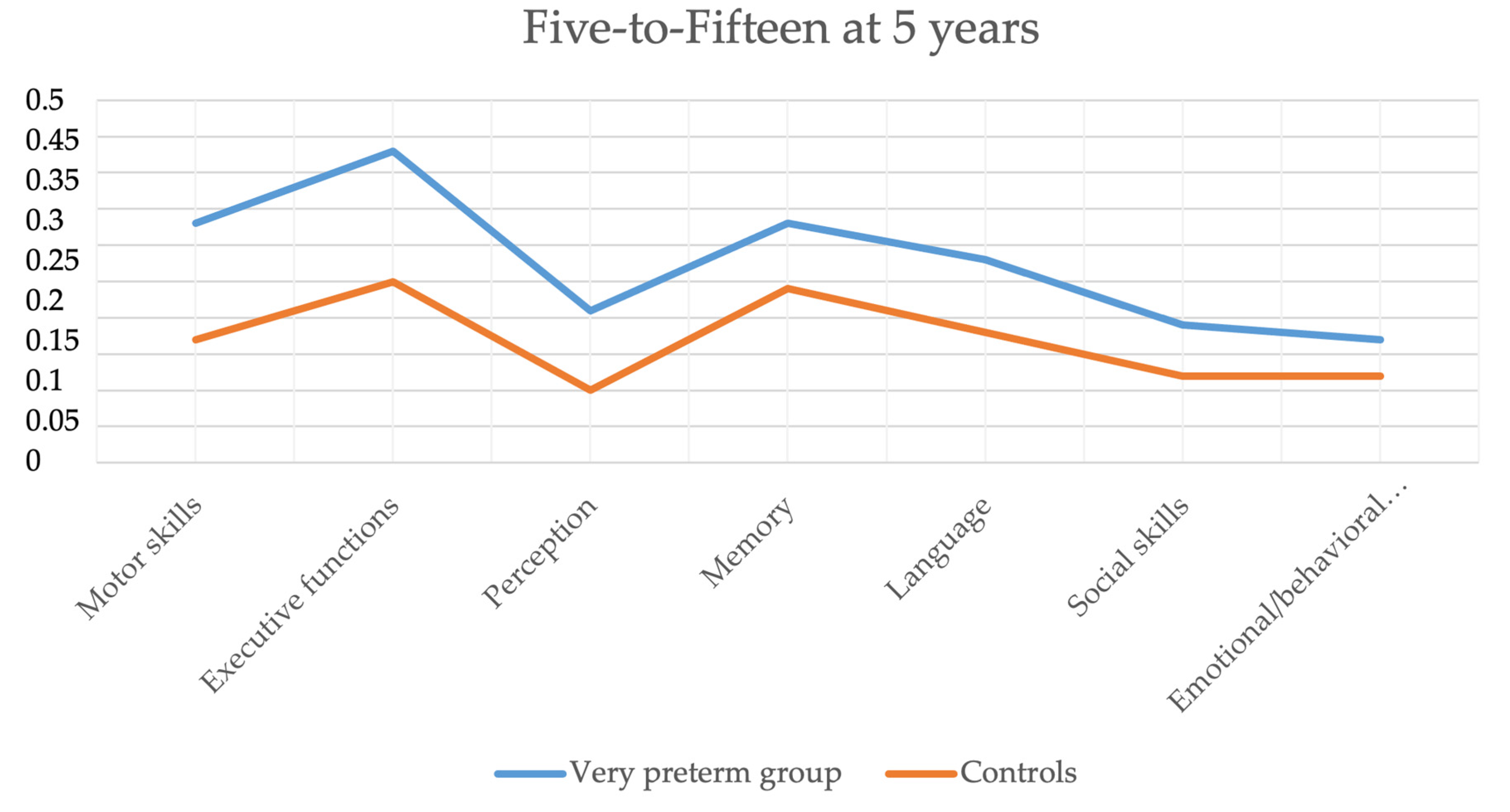
3.1. Five-to-Fifteen at 5 Years
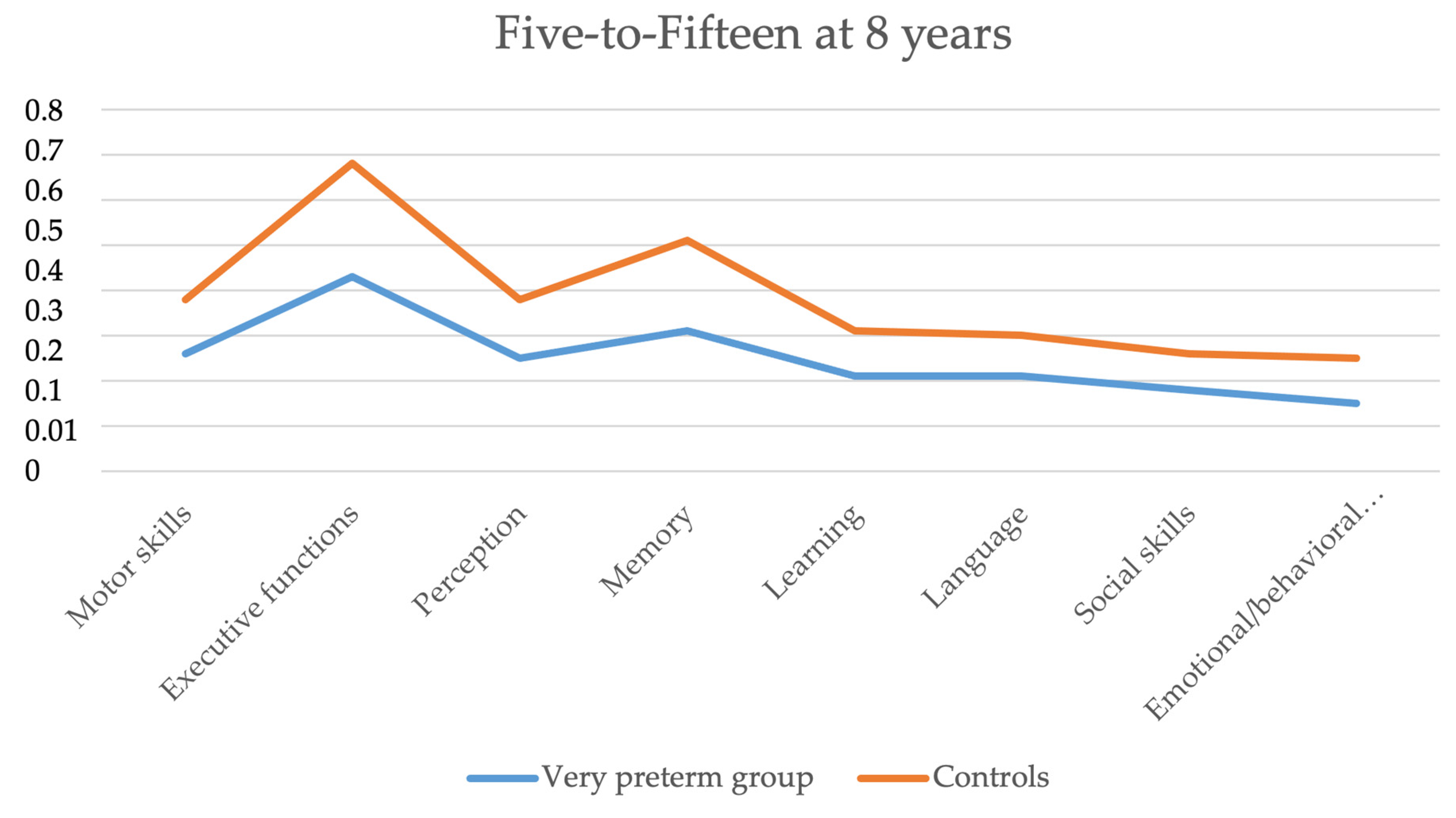
3.2. Five-to-Fifteen at 8 Years
3.3. Correlation between Age Points
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.H.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Sellier, E.; Platt, M.J.; Andersen, G.L.; Krägeloh-Mann, I.; De La Cruz, J.; Cans, C.; Surveillance of Cerebral Palsy Network. Decreasing prevalence in cerebral palsy: A multi-site European population-based study, 1980 to 2003. Dev. Med. Child Neurol. 2016, 58, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, C.; Ehlinger, V.; Delobel-Ayoub, M.; Klapouszczak, D.; Perra, O.; Hensey, O.; Neubauer, D.; Hollódy, K.; Virella, D.; Rackauskaite, G.; et al. Trends in Prevalence and Severity of Pre/Perinatal Cerebral Palsy among Children Born Preterm from 2004 to 2010: A SCPE Collaboration Study. Front. Neurol. 2021, 12, 710. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Cameron, K.; Doyle, L.W.; Cheong, J.L.; Victorian Infant Collaborative Study Group. Motor Impairment Trends in Extremely Preterm Children: 1991–2005. Pediatrics 2018, 141, e20173410. [Google Scholar] [CrossRef]
- Williams, J.; Lee, K.J.; Anderson, P.J. Prevalence of motor-skill impairment in preterm children who do not develop cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2010, 52, 232–237. [Google Scholar] [CrossRef]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef]
- Caravale, B.; Herich, L.; Zoia, S.; Capone, L.; Voller, F.; Carrozzi, M.; Chiandotto, V.; Balottin, U.; Lacchei, M.; Croci, I.; et al. Risk of Developmental Coordination Disorder in Italian very preterm children at school age compared to general population controls. Eur. J. Paediatr. Neurol. 2019, 23, 296–303. [Google Scholar] [CrossRef]
- Dewey, D.; Kaplan, B.J.; Crawford, S.G.; Wilson, B.N. Developmental coordination disorder: Associated problems in attention, learning, and psychosocial adjustment. Hum. Mov. Sci. 2002, 21, 905–918. [Google Scholar] [CrossRef]
- Van Hus, J.W.; Potharst, E.S.; Jeukens-Visser, M.; Kok, J.H.; Van Wassenaer-Leemhuis, A.G. Motor impairment in very preterm-born children: Links with other developmental deficits at 5 years of age. Dev. Med. Child Neurol. 2014, 56, 587–594. [Google Scholar] [CrossRef]
- Hemgren, E.; Persson, K. Deficits in motor co-ordination and attention at 3 years of age predict motor deviations in 6.5-year-old children who needed neonatal intensive care. Child Care Health Dev. 2009, 35, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, A.; Hägglöf, B.; Serenius, F. Behaviours related to executive functions and learning skills at 11 years of age after extremely preterm birth: A Swedish national prospective follow-up study. Acta Paediatr. 2013, 102, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Fawke, J.; Hennessy, E.; Rowell, V.; Thomas, S.; Wolke, D.; Marlow, N. Neurodevelopmental Disability Through 11 Years of Age in Children Born Before 26 Weeks of Gestation. Pediatrics 2009, 124, e249–e257. [Google Scholar] [CrossRef] [PubMed]
- Holsti, A.; Adamsson, M.; Hägglöf, B.; Farooqi, A.; Serenius, F. Chronic Conditions and Health Care Needs of Adolescents Born at 23 to 25 Weeks’ Gestation. Pediatrics 2017, 139, e20162215. [Google Scholar] [CrossRef] [PubMed]
- Flamant, C.; Branger, B.; Tich, S.N.T.; de La Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-Completed Developmental Screening in Premature Children: A Valid Tool for Follow-Up Programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef]
- Korkman, M.; Jaakkola, M.; Ahlroth, A.; Pesonen, A.-E.; Turunen, M.-M. Screening of developmental disorders in five-year-olds using the FTF (Five to Fifteen) questionnaire: A validation study. Eur. Child Adolesc. Psychiatry 2004, 13 (Suppl. 3), iii31–iii38. [Google Scholar] [CrossRef]
- Janols, L.-O.; Korkman, M.; Mickelsson, K.; Strand, G.; Trillingsgaard, A.; Gillberg, C. The FTF (Five to Fifteen): The development of a parent questionnaire for the assessment of ADHD and comorbid conditions. Eur. Child Adolesc. Psychiatry 2004, 13 (Suppl. 3), iii3–iii13. [Google Scholar] [CrossRef]
- Lambek, R.; Trillingsgaard, A. Elaboration, validation and standardization of the five to fifteen (FTF) questionnaire in a Danish population sample. Res. Dev. Disabil. 2015, 38, 161–170. [Google Scholar] [CrossRef]
- Lind, A.; The PIPARI Study Group; Haataja, L.; Rautava, L.; Väliaho, A.; Lehtonen, L.; Lapinleimu, H.; Parkkola, R.; Korkman, M. Relations between brain volumes, neuropsychological assessment and parental questionnaire in prematurely born children. Eur. Child Adolesc. Psychiatry 2010, 19, 407–417. [Google Scholar] [CrossRef]
- Bolk, J.; Farooqi, A.; Hafström, M.; Åden, U.; Serenius, F. Developmental Coordination Disorder and Its Association With Developmental Comorbidities at 6.5 Years in Apparently Healthy Children Born Extremely Preterm. JAMA Pediatr. 2018, 172, 765–774. [Google Scholar] [CrossRef]
- Huhtala, M.; Korja, R.; Lehtonen, L.; Haataja, L.; Lapinleimu, H.; Rautava, P.; PIPARI Study Group. Associations between parental psychological well-being and socio-emotional development in 5-year-old preterm children. Early Hum. Dev. 2014, 90, 119–124. [Google Scholar] [CrossRef]
- Rautava, L.; Andersson, S.; Gissler, M.; Hallman, M.; Häkkinen, U.; Korvenranta, E.; Korvenranta, H.; Leipälä, J.; Tammela, O.; Lehtonen, L. Development and behaviour of 5-year-old very low birthweight infants. Eur. Child Adolesc. Psychiatry 2010, 19, 669–677. [Google Scholar] [CrossRef]
- Manual 5-15R (Five-To-Fifteen-Revised), Nordic Questionnaire for Evaluation of Development and Behavior in Children and Adolescents. 2018. Available online: www.5-15.org (accessed on 28 March 2023).
- Maunu, J.; Parkkola, R.; Rikalainen, H.; Lehtonen, L.; Haataja, L.; Lapinleimu, H.; PIPARI Group. Brain and ventricles in very low birth weight infants at term: A comparison among head circumference, ultrasound, and magnetic resonance imaging. Pediatrics 2009, 123, 617–626. [Google Scholar] [CrossRef]
- Setänen, S.; Haataja, L.; Parkkola, R.; Lind, A.; Lehtonen, L.; the PIPARI Study Group. Predictive value of neonatal brain MRI on the neurodevelopmental outcome of preterm infants by 5 years of age. Acta Paediatr. 2013, 102, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Lind, A.; Korkman, M.; Lehtonen, L.; Lapinleimu, H.; Parkkola, R.; Matomäki, J.; Haataja, L.; The Pipari Study Group. Cognitive and neuropsychological outcomes at 5 years of age in preterm children born in the 2000s. Dev. Med. Child Neurol. 2011, 53, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.; Berube, M.; Erlandson, K.; Haug, S.; Johnstone, H.; Meagher, M.; Sarkodee-Adoo, S.; Zwicker, J.G. Developmental Coordination Disorder in School-Aged Children Born Very Preterm and/or at Very Low Birth Weight: A Systematic Review. J. Dev. Behav. Pediatr. 2011, 32, 678–687. [Google Scholar] [CrossRef]
- Uusitalo, K.; Haataja, L.; Nyman, A.; Ripatti, L.; Huhtala, M.; Rautava, P.; Lehtonen, L.; Parkkola, R.; Lahti, K.; Koivisto, M.; et al. Preterm children’s developmental coordination disorder, cognition and quality of life: A prospective cohort study. BMJ Paediatr. Open 2020, 4, e000633. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Dewey, D.; Nguyen, T.-N.; Ellis, R.; Burnett, A.; Kwong, A.; Lee, K.; Cheong, J.L.; Doyle, L.W.; Anderson, P.J. Rates of Developmental Coordination Disorder in Children Born Very Preterm. J. Pediatr. 2021, 231, 61–67. [Google Scholar] [CrossRef]
- Helin, M.; Karukivi, M.; Haataja, L.; Rautava, P.; Junttila, N.; Salomäki, S.; Lehtonen, L.; Setänen, S. Motor Performance in Association with Perceived Loneliness and Social Competence in 11-Year-Old Children Born Very Preterm. Children 2022, 9, 660. [Google Scholar] [CrossRef]
- Joensuu, E.; Munck, P.; Setänen, S.; Lipsanen, J.; Huhtala, M.; Lapinleimu, H.; Stolt, S.K.J. Associations between Language at 2 Years and Literacy Skills at 7 Years in Preterm Children Born at Very Early Gestational Age and/or with Very Low Birth Weight. Children 2021, 8, 510. [Google Scholar] [CrossRef]
- Farooqi, A.; Adamsson, M.; Serenius, F.; Hägglöf, B. Executive Functioning and Learning Skills of Adolescent Children Born at Fewer than 26 Weeks of Gestation. PLoS ONE 2016, 11, e0151819. [Google Scholar] [CrossRef] [PubMed]
- Aanes, S.; Bjuland, K.J.; Sripada, K.; Sølsnes, A.E.; Grunewaldt, K.H.; Håberg, A.; Løhaugen, G.C.; Skranes, J. Reduced hippocampal subfield volumes and memory function in school-aged children born preterm with very low birthweight (VLBW). NeuroImage Clin. 2019, 23, 101857. [Google Scholar] [CrossRef] [PubMed]
- Retzler, J.; Johnson, S.; Groom, M.J.; Cragg, L. A comparison of simultaneous and sequential visuo-spatial memory in children born very preterm. Child Neuropsychol. 2022, 28, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Dean, B.; Ginnell, L.; Boardman, J.P.; Fletcher-Watson, S. Social cognition following preterm birth: A systematic review. Neurosci. Biobehav. Rev. 2021, 124, 151–167. [Google Scholar] [CrossRef]
- Mossad, S.I.; Vandewouw, M.M.; Smith, M.L.; Taylor, M.J. The preterm social brain: Altered functional networks for Theory of Mind in very preterm children. Brain Commun. 2021, 3, fcaa237. [Google Scholar] [CrossRef]
- Ni, Y.; Mendonça, M.; Baumann, N.; Eves, R.; Kajantie, E.; Hovi, P.; Tikanmäki, M.; Räikkönen, K.; Heinonen, K.; Indredavik, M.S.; et al. Social Functioning in Adults Born Very Preterm: Individual Participant Meta-analysis. Pediatrics 2021, 148, e2021051986. [Google Scholar] [CrossRef]
- Linsell, L.; Johnson, S.; Wolke, D.; Morris, J.; Kurinczuk, J.J.; Marlow, N. Trajectories of behavior, attention, social and emotional problems from childhood to early adulthood following extremely preterm birth: A prospective cohort study. Eur. Child Adolesc. Psychiatry 2019, 28, 531–542. [Google Scholar] [CrossRef]
- Bogičević, L.; Verhoeven, M.; Van Baar, A.L. Toddler skills predict moderate-to-late preterm born children’s cognition and behaviour at 6 years of age. PLoS ONE 2019, 14, e0223690. [Google Scholar] [CrossRef]
- Bartal, T.; Adams, M.; Natalucci, G.; Borradori-Tolsa, C.; Latal, B.; Swiss Neonatal Network and Follow-up Group. Behavioral problems in very preterm children at five years of age using the Strengths and Difficulties Questionnaire: A multicenter cohort study. Early Hum. Dev. 2020, 151, 105200. [Google Scholar] [CrossRef]
- Stene-Larsen, K.; Lang, A.M.; Landolt, M.A.; Latal, B.; Vollrath, M.E. Emotional and behavioral problems in late preterm and early term births: Outcomes at child age 36 months. BMC Pediatr. 2016, 16, 196. [Google Scholar] [CrossRef]
- Koivisto, A.; Klenberg, L.; Tommiska, V.; Lano, A.; Laine, M.; Fellman, V.; Haavisto, A.; the Finnish ELBW Cohort Study Group (FinELBW). Parents tend to underestimate cognitive deficits in 10- to 13-year-olds born with an extremely low birth weight. Acta Paediatr. 2015, 104, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Norberg, H.; Kowalski, J.; Maršál, K.; Norman, M. Timing of antenatal corticosteroid administration and survival in extremely preterm infants: A national population-based cohort study. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1567–1574. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Background Characteristics | Children Born VeryPreterm | Controls | ||
|---|---|---|---|---|
| at 5 Years, n = 168 | at 8 Years, n = 164 | at 5 Years, n = 151 | at 8 Years, n = 131 | |
| Gestational age, mean (SD), weeks | 28.9 (2.8) | 28.9 (2.8) | ||
| Birth weight, mean (SD), grams | 1104.7 (315.9) | 1122.5 (323.8) | 3652.7 (450.3) | 3636.0 (437.4) |
| Birth weight z-score a, mean (SD) | −1.4 (1.4) | −1.4 (1.5) | ||
| Small for gestational age (<−2 SD), n (%) | 55 (32.7) | 53 (32.3) | ||
| Prenatal corticosteroids, n (%) | 161 (95.8) | 154 (93.9) | ||
| Multiple birth, n (%) | 55 (32.7) | 53 (32.3) | ||
| Cesarean delivery, n (%) | 107 (63.7) | 98 (59.8) | 23 (15.2) | 21 (16.0) |
| Male, n (%) | 93 (55.4) | 77 (47.0) | 69 (45.7) | 61 (46.6) |
| Patent ductus arteriosus, operated, n (%) | 22/167 (13.2) | 17 (10.4) | ||
| Bronchopulmonary dysplasia, n (%) | 25 (14.9) | 22 (13.4) | ||
| Operated necrotizing enterocolitis, n (%) | 9 (5.4) | 8 (4.9) | ||
| Sepsis, n (%) | 35 (20.8) | 31 (18.9) | ||
| Laser-treated retinopathy of prematurity, n (%) | 7/157 (4.5) | 4/153 (2.6) | ||
| Major brain pathology in MRI b at term, n (%) | 38/166 (22.9) | 40/160 (25.0) | ||
| Mother’s education > 12 years, n (%) | 76/158 (48.1) | 72/155 (46.5) | 50 (33.1) | 46 (35.1) |
| Father’s education > 12 years, n (%) | 42/158 (26.6) | 39/155 (25.2) | 43 (28.5) | 37 (28.2) |
| Neurodevelopmental impairment, n (%) | 12 (7.1) | 14 (8.5) | ||
| Cerebral palsy, n (%) | 8 (4.8) | 9 (5.5) | ||
| Severe hearing impairment, n (%) | 3 (1.8) | 3 (1.8) | ||
| Severe visual impairment, n (%) | 0 (0) | 0 (0) | ||
| Severe cognitive impairment c, n (%) | 4/155 (2.6) | 4/146 (2.7) | ||
| Full-scale intelligence quotient, mean (SD) | 102.1 (16.7) | 101.9 (17.6) | ||
| Five-to-Fifteen at 5 Years | Children Born Very Preterm, n = 168 Mean (Unadjusted) | Controls, n = 151 Mean (Unadjusted) | Adjusted RR | 95% CI | p-Value |
|---|---|---|---|---|---|
| Motor skills | 0.33 | 0.17 | 2.3 1.9 * | 1.8–3.0 1.5–2.5 | <0.001 <0.001 |
| Gross motor skills | 0.31 | 0.13 | 2.5 2.0 * | 1.9–3.4 1.4–2.7 | <0.001 <0.001 |
| Fine motor skills | 0.36 | 0.20 | 1.9 1.7 * | 1.4–2.5 1.3–2.2 | <0.001 <0.001 |
| Executive functions | 0.43 | 0.25 | 1.7 1.6 * | 1.3–2.2 1.3–2.2 | <0.001 <0.001 |
| Attention and concentration | 0.42 | 0.22 | 1.9 1.9 * | 1.5–2.6 1.4–2.5 | <0.001 <0.001 |
| Overactivity and impulsivity | 0.53 | 0.36 | 1.4 1.4 * | 1.1–1.8 1.1–1.8 | 0.01 0.02 |
| Passivity and inactivity | 0.21 | 0.09 | 2.3 2.0 * | 1.5–3.4 1.3–3.0 | <0.001 0.001 |
| Planning and organizing | 0.41 | 0.25 | 1.5 1.4 * | 1.1–2.1 1.0–2.0 | 0.02 0.04 |
| Perception | 0.21 | 0.10 | 1.9 1.8 * | 1.4–2.5 1.3–2.3 | <0.001 <0.001 |
| Perception of space and direction | 0.22 | 0.11 | 1.9 1.6 * | 1.3–2.6 1.1–2.3 | <0.001 0.007 |
| Perception of own body | 0.18 | 0.11 | 1.5 1.5 * | 1.1–2.2 1.1–2.2 | 0.02 0.02 |
| Perception of visual forms and figures | 0.25 | 0.08 | 2.7 2.5 * | 1.8–4.1 1.7–3.7 | <0.001 <0.001 |
| Memory | 0.33 | 0.24 | 1.3 1.2 * | 1.0–1.7 0.9–1.6 | 0.08 0.2 |
| Language | 0.28 | 0.18 | 1.5 1.3 * | 1.1–1.9 1.0–1.7 | 0.003 0.03 |
| Comprehension of spoken language | 0.31 | 0.18 | 1.6 1.5 * | 1.2–2.2 1.1–2.0 | 0.002 0.02 |
| Expressive language | 0.27 | 0.19 | 1.4 1.2 * | 1.0–1.8 1.0–1.6 | 0.02 0.1 |
| Verbal communication | 0.31 | 0.17 | 1.8 1.6 * | 1.3–2.6 1.1–2.4 | 0.001 0.009 |
| Social skills | 0.19 | 0.12 | 1.4 1.3 * | 1.1–1.8 1.0–1.6 | 0.02 0.1 |
| Emotional/behavioral difficulties | 0.17 | 0.12 | 1.2 1.2 * | 0.9–1.5 0.9–1.6 | 0.2 0.2 |
| Internalization | 0.13 | 0.09 | 1.5 1.4 * | 1.1–2.0 1.0–1.9 | 0.02 0.02 |
| Acting out | 0.24 | 0.18 | 1.1 1.2 * | 0.9–1.5 0.9–1.5 | 0.4 0.3 |
| Obsessive actions or thoughts | 0.09 | 0.05 | 1.6 1.6 * | 1.1–2.4 1.1–2.3 | 0.01 0.03 |
| Five-to-Fifteen at 8 Years | Children Born Very Preterm, n = 164 Mean (Unadjusted) | Controls, n = 131 Mean (Unadjusted) | Adjusted RR | 95% CI | p-Value |
|---|---|---|---|---|---|
| Motor skills | 0.26 | 0.12 | 2.2 1.9 * | 1.7–2.9 1.4–2.5 | <0.001 <0.001 |
| Gross motor skills | 0.29 | 0.11 | 2.7 2.2 * | 2.0–3.8 1.6–3.0 | <0.001 <0.001 |
| Fine motor skills | 0.24 | 0.12 | 1.9 1.7 * | 1.4–2.6 1.2–2.3 | <0.001 0.001 |
| Executive functions | 0.43 | 0.25 | 1.5 1.5 * | 1.2–2.0 1.1–1.9 | 0.001 0.005 |
| Attention and concentration | 0.52 | 0.30 | 1.7 1.6 * | 1.3–2.2 1.2–2.1 | <0.001 0.002 |
| Overactivity and impulsivity | 0.39 | 0.24 | 1.6 1.5 * | 1.2–2.1 1.2–2.0 | 0.002 0.003 |
| Passivity and inactivity | 0.28 | 0.16 | 1.7 1.6 * | 1.2–2.4 1.1–2.3 | 0.003 0.008 |
| Planning and organizing | 0.45 | 0.23 | 1.8 1.5 * | 1.3–2.6 1.0–2.1 | 0.001 0.03 |
| Perception | 0.25 | 0.13 | 1.9 1.7 * | 1.5–2.5 1.3–2.3 | <0.001 <0.001 |
| Perception of space and direction | 0.19 | 0.07 | 2.7 2.5 * | 1.8–4.0 1.6–3.8 | <0.001 <0.001 |
| Concepts of time | 0.52 | 0.33 | 1.6 1.5 * | 1.2–2.2 1.1–2.1 | 0.002 0.006 |
| Perception of own body | 0.18 | 0.10 | 1.8 1.5 * | 1.2–2.6 1.0–2.3 | 0.004 0.04 |
| Perception of visual forms and figures | 0.13 | 0.03 | 4.1 3.1 * | 2.3–7.3 1.7–5.7 | <0.001 <0.001 |
| Memory | 0.31 | 0.20 | 1.5 1.5 * | 1.2–2.0 1.1–2.0 | 0.002 0.007 |
| Learning | 0.21 | 0.10 | 1.9 1.8 * | 1.4–2.6 1.3–2.5 | <0.001 <0.001 |
| Reading and writing | 0.37 | 0.26 | 1.4 1.3 * | 1.1–1.9 1.0–1.8 | 0.02 0.06 |
| Arithmetic | 0.35 | 0.21 | 2.0 1.9 * | 1.4–2.8 1.3–2.7 | <0.001 <0.001 |
| General learning | 0.24 | 0.10 | 2.3 2.2 * | 1.6–3.4 1.4–3.2 | <0.001 <0.001 |
| Coping with learning | 0.44 | 0.25 | 1.8 1.7 * | 1.4–2.4 1.3–2.2 | <0.001 <0.001 |
| Language | 0.21 | 0.09 | 2.2 2.1 * | 1.7–2.9 1.6–2.8 | <0.001 <0.001 |
| Comprehension of spoken language | 0.26 | 0.10 | 2.7 2.4 * | 1.8–3.9 1.7–3.6 | <0.001 <0.001 |
| Expressive language | 0.17 | 0.08 | 2.2 2.2 * | 1.6–3.0 1.6–3.0 | <0.001 <0.001 |
| Verbal communication | 0.27 | 0.14 | 1.8 1.8 * | 1.2–2.7 1.2–2.7 | 0.002 0.005 |
| Social skills | 0.18 | 0.08 | 2.1 2.0 * | 1.6–2.7 1.5–2.6 | <0.001 <0.001 |
| Emotional/behavioral difficulties | 0.15 | 0.10 | 1.4 1.3 * | 1.1–1.8 1.0–1.8 | 0.02 0.05 |
| Internalization | 0.14 | 0.09 | 1.6 1.5 * | 1.1–2.1 1.1–2.1 | 0.005 0.008 |
| Acting out | 0.20 | 0.15 | 1.2 1.2 * | 0.9–1.6 0.9–1.6 | 0.2 0.2 |
| Obsessive actions or thoughts | 0.07 | 0.05 | 1.5 1.4 * | 1.0–2.2 0.9–2.1 | 0.08 0.1 |
| FTF Domain | Children Born Very Preterm, n = 146, r (p) | Controls, n = 117, r (p) |
|---|---|---|
| Motor skills | 0.76 (<0.001) 0.66 (<0.001), n = 136 * | 0.70 (<0.001) |
| Gross motor skills | 0.74 (<0.001) 0.62 (<0.001), n = 136 * | 0.72 (<0.001), n = 116 |
| Fine motor skills | 0.65 (<0.001) 0.58 (<0.001), n = 136 * | 0.58 (<0.001) |
| Executive functions | 0.61 (<0.001), n = 145 0.60 (<0.001), n = 135 * | 0.48 (<0.001) |
| Attention and concentration | 0.58 (<0.001), n = 144 0.57 (<0.001), n = 134 * | 0.46 (<0.001), n = 115 |
| Overactivity and impulsivity | 0.59 (<0.001), n = 145 0.57 (<0.001), n = 135 * | 0.44 (<0.001) |
| Passivity and inactivity | 0.48 (<0.001) 0.48 (<0.001), n = 136 * | 0.35 (<0.001) |
| Planning and organizing | 0.49 (<0.001), n = 144 0.48 (<0.001), n = 134 * | 0.42 (<0.001), n = 116 |
| Perception | 0.56 (<0.001), n = 144 0.50 (<0.001), n = 135 * | 0.31 (0.001), n = 116 |
| Perception of space and direction | 0.39 (<0.001) 0.30 (<0.001), n = 136 * | 0.47 (<0.001) |
| Perception of own body | 0.55 (<0.001), n = 144 0.57 (<0.001), n = 135 * | 0.37 (<0.001), n = 116 |
| Perception of visual forms and figures | 0.57 (<0.001), n = 144 0.52 (<0.001), n = 135 * | 0.19 (0.04), n = 116 |
| Memory | 0.61 (<0.001), n = 144 0.62 (<0.001), n = 135 * | 0.62 (<0.001), n = 116 |
| Language | 0.75 (<0.001) 0.77 (<0.001), n = 136 * | 0.44 (<0.001), n = 115 |
| Comprehension of spoken language | 0.44 (<0.001), n = 145 0.45 (<0.001), n = 135 * | 0.27 (0.003), n = 115 |
| Expressive language | 0.77 (<0.001) 0.80 (<0.001), n = 136 * | 0.31 (0.001), n = 115 |
| Verbal communication | 0.56 (<0.001) 0.56 (<0.001), n = 136 * | 0.59 (<0.001), n = 115 |
| Social skills | 0.72 (<0.001) 0.70 (<0.001), n = 136 * | 0.52 (<0.001), n = 116 |
| Emotional/behavioral difficulties | 0.66 (<0.001), n = 145 0.67 (<0.001), n = 135 * | 0.69 (<0.001) |
| Internalization | 0.52 (<0.001), n = 145 0.52 (<0.001), n = 135 * | 0.71 (<0.001) |
| Acting out | 0.70 (<0.001), n = 145 0.70 (<0.001), n = 135 * | 0.68 (<0.001) |
| Obsessive actions or thoughts | 0.54 (<0.001), n = 145 0.59 (<0.001), n = 135 * | 0.31 (0.001), n = 116 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mäkilä, E.; Ekblad, M.O.; Rautava, P.; Lapinleimu, H.; Setänen, S. Five-to-Fifteen—Parental Perception of Developmental Profile from Age 5 to 8 Years in Children Born Very Preterm. J. Pers. Med. 2023, 13, 819. https://doi.org/10.3390/jpm13050819
Mäkilä E, Ekblad MO, Rautava P, Lapinleimu H, Setänen S. Five-to-Fifteen—Parental Perception of Developmental Profile from Age 5 to 8 Years in Children Born Very Preterm. Journal of Personalized Medicine. 2023; 13(5):819. https://doi.org/10.3390/jpm13050819
Chicago/Turabian StyleMäkilä, Eeva, Mikael O. Ekblad, Päivi Rautava, Helena Lapinleimu, and Sirkku Setänen. 2023. "Five-to-Fifteen—Parental Perception of Developmental Profile from Age 5 to 8 Years in Children Born Very Preterm" Journal of Personalized Medicine 13, no. 5: 819. https://doi.org/10.3390/jpm13050819