

Circadian Fluctuation Changes in Intraocular Pressure Measured Using a Contact Lens Sensor in Patients with Glaucoma after the Adjunctive Administration of Ripasudil: A Prospective Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
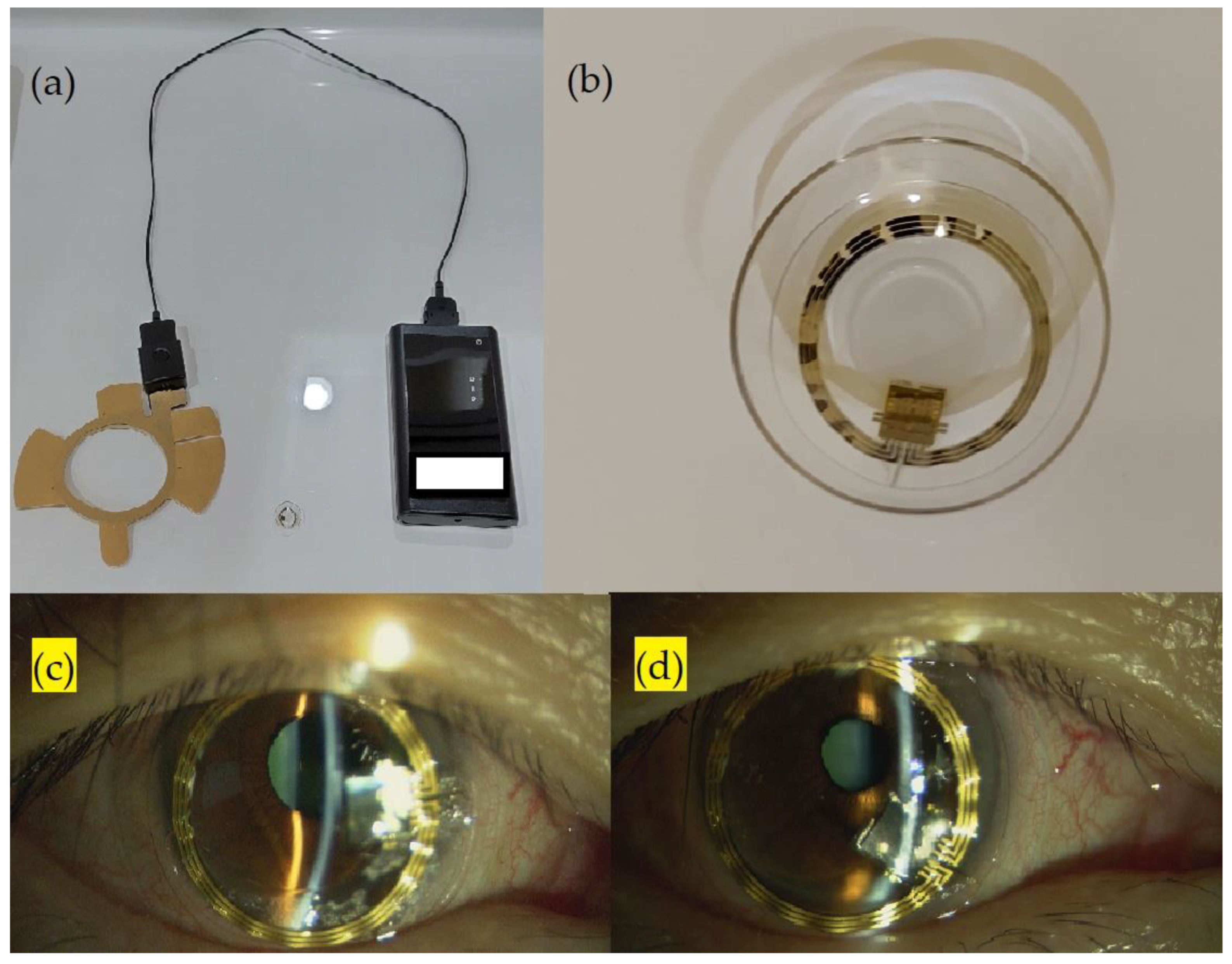
2.2. Parameters of Contact Lens Sensor Measurements
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinreb, R.N.; Khaw, P.T. Primary Open-Angle Glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Weinreb, R.N.; Medeiros, F.A. Is 24-h Intraocular Pressure Monitoring Necessary in Glaucoma? Semin. Ophthalmol. 2013, 28, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Bouligny, R.P.; Kripke, D.F.; Weinreb, R.N. Nocturnal Elevation of Intraocular Pressure is Detectable in the Sitting Position. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4439–4442. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Zhang, X.; Kripke, D.F.; Weinreb, R.N. Twenty-Four-Hour Intraocular Pressure Pattern Associated with Early Glaucomatous Changes. Investig. Ophthalmol. Vis. Sci. 2003, 44, 1586–1590. [Google Scholar] [CrossRef]
- Arora, N.; McLaren, J.W.; Hodge, D.O.; Sit, A.J. Effect of Body Position on Epsicleral Venous Pressure in Healthy Subjects. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5151–5156. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Weinreb, R.N. Monitoring Intraocular Pressure for 24 h. Br. J. Ophthalmol. 2011, 95, 599–600. [Google Scholar] [CrossRef]
- Inoue, T.; Tanihara, H. Ripasudil Hydrochloride Hydrate: Targeting Rho Kinase in the Treatment of Glaucoma. Expert Opin. Pharmacother. 2017, 18, 1669–1673. [Google Scholar] [CrossRef]
- Kusuhara, S.; Nakamura, M. Ripasudil Hydrochloride Hydrate in the Treatment of Glaucoma: Safety, Efficacy, and Patient Selection. Clin. Ophthalmol. 2020, 14, 1229–1236. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Suganami, H.; Araie, M. Intra-Ocular Pressure-Lowering Effects of a Rho Kinase Inhibitor, Ripasudil (K-115), over 24 h in Primary Open-Angle Glaucoma and Ocular Hypertension: A Randomized, Open-Label, Crossover Study. Acta Ophthalmol. 2015, 93, e254–e260. [Google Scholar] [CrossRef]
- Lorenz, K.; Korb, C.; Herzog, N.; Vetter, J.M.; Elflein, H.; Keilani, M.M.; Pfeiffer, N. Tolerability of 24-h Intraocular Pressure Monitoring of a Pressure-Sensitive Contact Lens. J. Glaucoma 2013, 22, 311–316. [Google Scholar] [CrossRef]
- Mansouri, K.; Shaarawy, T. Continuous Intraocular Pressure Monitoring with a Wireless Ocular Telemetry Sensor: Initial Clinical Experience in Patients with Open Angle Glaucoma. Br. J. Ophthalmol. 2011, 95, 627–629. [Google Scholar] [CrossRef]
- Mansouri, K.; Weinreb, R.N.; Liu, J.H. Efficacy of a Contact Lens Sensor for Monitoring 24-h Intraocular Pressure Related Patterns. PLoS ONE 2015, 10, e0125530. [Google Scholar] [CrossRef] [PubMed]
- Vitish-Sharma, P.; Acheson, A.G.; Stead, R.; Sharp, J.; Abbas, A.; Hovan, M.; Maxwell-Armstrong, C.; Guo, B.; King, A.J. Can the SENSIMED Triggerfish® lens data be used as an accurate measure of intraocular pressure? Acta Ophthalmol. 2018, 96, e242–e246. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, G.E.; Shen, B.Y.; Aref, A.A. The Sensimed Triggerfish Contact Lens Sensor: Efficacy, Safety, and Patient Perspectives. Clin. Ophthalmol. 2017, 11, 875–882. [Google Scholar] [CrossRef]
- Konstas, A.G.P.; Mantziris, D.A.; Cate, E.A.; Stewart, W.C. Effect of Timolol on the Diurnal Intraocular Pressure in Exfoliation and Primary Open-Angle Glaucoma. Arch. Ophthalmol. 1997, 115, 975–979. [Google Scholar] [CrossRef]
- Liu, J.H.; Kripke, D.F.; Weinreb, R.N. Comparison of the Nocturnal Effects of Once-Daily Timolol and Latanoprost on Intraocular Pressure. Am. J. Ophthalmol. 2004, 138, 389–395. [Google Scholar] [CrossRef]
- Krag, S.; Andersen, H.B.; Sørensen, T. Circadian Intraocular Pressure Variation with Beta-Blockers. Acta Ophthalmol. Scand. 1999, 77, 500–503. [Google Scholar] [CrossRef]
- Toris, C.B.; Zhan, G.L.; Yablonski, M.E.; Camras, C.B. Effects on Aqueous Flow of Dorzolamide Combined with Either Timolol or Acetazolamide. J. Glaucoma 2004, 13, 210–215. [Google Scholar] [CrossRef]
- Bagga, H.; Liu, J.H.; Weinreb, R.N. Intraocular Pressure Measurements throughout the 24 h. Curr. Opin. Ophthalmol. 2009, 20, 79–83. [Google Scholar] [CrossRef]
- Gulati, V.; Fan, S.; Zhao, M.; Maslonka, M.A.; Gangahar, C.; Toris, C.B. Diurnal and Nocturnal Variations in Aqueous Humor Dynamics of Patients with Ocular Hypertension Undergoing Medical Therapy. Arch. Ophthalmol. 2012, 130, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Maus, T.L.; McLaren, J.W.; Shepard, J.W., Jr.; Brubaker, R.F. The Effects of Sleep on Circulating Catecholamines and Aqueous Flow in Human Subjects. Exp. Eye Res. 1996, 62, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.C.; Konstas, A.G.; Nelson, L.A.; Kruft, B. Meta-analysis of 24-h Intraocular Pressure Studies Evaluating the Efficacy of Glaucoma Medicines. Ophthalmology 2008, 115, 1117–1122.e1. [Google Scholar] [CrossRef]
- Baba, T.; Hirooka, K.; Nii, H.; Kiuchi, Y. Responsiveness to Ripasudil May Be a Potential Outcome Marker for Selective Laser Trabeculoplasty in Patients with Primary Open-Angle Glaucoma. Sci. Rep. 2021, 11, 5812. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Sakemi, F.; Marumoto, T. Intraocular Pressure-Lowering Effects of Ripasudil, a Rho-Kinase Inhibitor, and Selective Laser Trabeculoplasty as Adjuvant Therapy in Patients with Uncontrolled Glaucoma. Int. Ophthalmol. 2021, 41, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Tojo, N.; Oka, M.; Miyakoshi, A.; Ozaki, H.; Hayashi, A. Comparison of Fluctuations of Intraocular Pressure before and after Selective Laser Trabeculoplasty in Normal-Tension Glaucoma Patients. J. Glaucoma 2014, 23, e138–e143. [Google Scholar] [CrossRef]
- Hoban, K.; Peden, R.; Megaw, R.; Halpin, P.; Tatham, A.J. 24-h Contact Lens Sensor Monitoring of Intraocular Pressure-Related Profiles in Normal-Tension Glaucoma and Rates of Disease Progression. Ophthalmic Res. 2017, 57, 208–215. [Google Scholar] [CrossRef]
- Tojo, N.; Hayashi, A.; Otsuka, M. Correlation between 24-h Continuous Intraocular Pressure Measurement with a Contact Lens Sensor and Visual Field Progression. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 175–182. [Google Scholar] [CrossRef]
- Kim, Y.W.; Kim, J.S.; Lee, S.Y.; Ha, A.; Lee, J.; Park, Y.J.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Twenty-Four-Hour Intraocular Pressure-Related Patterns from Contact Lens Sensors in Normal-Tension Glaucoma and Healthy Eyes: The Exploring Nyctohemeral Intraocular Pressure Related Pattern for Glaucoma Management (ENIGMA) Study. Ophthalmology 2020, 127, 1487–1497. [Google Scholar] [CrossRef]
- Mansouri, K.; Medeiros, F.A.; Tafreshi, A.; Weinreb, R.N. Continuous 24-h monitoring of intraocular pressure patterns with a contact lens sensor: Safety, tolerability, and reproducibility in patients with glaucoma. Arch. Ophthalmol. 2012, 130, 1534–1539. [Google Scholar] [CrossRef]
- Tanihara, H.; Kakuda, T.; Sano, T.; Kanno, T.; Imada, R.; Shingaki, W.; Gunji, R. Safety and Efficacy of Ripasudil in Japanese Patients with Glaucoma or Ocular Hypertension: 3-Month Interim Analysis of ROCK-J, a Post-Marketing Surveillance Study. Adv. Ther. 2019, 36, 333–343. [Google Scholar] [CrossRef]
- Inazaki, H.; Kobayashi, S.; Anzai, Y.; Satoh, H.; Sato, S.; Inoue, M.; Yamane, S.; Kadonosono, K. One-Year Efficacy of Adjunctive Use of Ripasudil, a Rho-Kinase Inhibitor, in Patients with Glaucoma Inadequately Controlled with Maximum Medical Therapy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 2009–2015. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.E.; Yoo, C.; Lin, S.C.; Kim, Y.Y. Effect of Different Head Positions in Lateral Decubitus Posture on Intraocular Pressure in Treated Patients with Open-Angle Glaucoma. Am. J. Ophthalmol. 2015, 160, 929–936.e4. [Google Scholar] [CrossRef] [PubMed]
- Beltran-Agulló, L.; Buys, Y.M.; Jahan, F.; Shapiro, C.M.; Flanagan, J.G.; Cheng, J.; Trope, G.E. Twenty-Four Hour Intraocular Pressure Monitoring with the SENSIMED Triggerfish Contact Lens: Effect of Body Posture During Sleep. Br. J. Ophthalmol. 2017, 101, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Hubanova, R.; Aptel, F.; Chiquet, C.; Mottet, B.; Romanet, J.P. Effect of Overnight Wear of the Triggerfish(®) Sensor on Corneal Thickness Measured by Visante(®) Anterior Segment Optical Coherence Tomography. Acta Ophthalmol. 2014, 92, e119–e123. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age, years (mean ± SD) | 58.33 ± 13.89 |
| Sex (n) | |
| Male | 4 |
| Female | 2 |
| Ancestry (n) | |
| Asian | 6 |
| SER, D (mean ± SD) | −2.96 ± 1.6 |
| CCT, µm (mean ± SD) | 516.5 ± 28.85 |
| IOP, mmHg (mean ± SD) | 13.167 ± 2.714 |
| Visual field parameters (mean ± SD) | |
| MD, dB | −4.78 ± 3.3 |
| PSD, dB | 6.56 ± 4.54 |
| VFI, % | 88.33 ± 8.31 |
| OCT parameters | |
| RNFL thickness, µm (mean ± SD) | 71.08 ± 9.36 |
| Medication number (mean ± SD) | 2 ± 1.09 |
| CLS Parameter, GAT IOP | Before Ripasudil | After Ripasudil | p-Value |
|---|---|---|---|
| 24 h average IOP, mVeq | 218.760 ± 80.100 | 102.311 ± 97.784 | 0.0265 * |
| 24 h IOP fluctuation, mVeq | 433.467 ± 135.872 | 407.867 ± 90.102 | 0.3337 |
| 24 h IOP maximum, mVeq | 407.300 ± 147.486 | 337.150 ± 91.250 | 0.1331 |
| Sleep time average IOP, mVeq | 296.774 ± 106.009 | 216.554 ± 110.489 | 0.0551 |
| Sleep time average IOP before 3 a.m., mVeq | 297.879 ± 125.821 | 221.780 ± 125.879 | 0.0855 |
| Sleep time IOP fluctuation, mVeq | 173.817 ± 70.431 | 146.133 ± 35.187 | 0.2529 |
| Sleep time IOP fluctuation before 3 a.m., mVeq | 166.250 ± 73.625 | 118.500 ± 28.613 | 0.1358 |
| Sleep time IOP maximum value, mVeq | 396.719 ± 148.986 | 291.650 ± 114.563 | 0.0723 |
| Awake time average IOP, mVeq | 178.478 ± 67.601 | 89.808 ± 71.734 | 0.0093 * |
| Awake time average IOP before 3 p.m., mVeq | 94.717 ± 55.398 | 31.599 ± 121.857 | 0.1039 |
| Awake time IOP fluctuation, mVeq | 386.400 ± 153.716 | 370.67 ± 112.953 | 0.3828 |
| Awake time IOP fluctuation before 3 p.m., mVeq | 158.867 ± 44.401 | 142.033 ± 39.801 | 0.0647 |
| Awake time IOP maximum value, mVeq | 360.217 ± 160.586 | 299.300 ± 98.133 | 0.1439 |
| 24 h IOP SD, mVeq | 105.442 ± 49.723 | 102.602 ± 36.562 | 0.4453 |
| Sleep time IOP SD, mVeq | 39.647 ± 16.677 | 32.808 ± 6.187 | 0.2306 |
| Sleep time IOP SD before 3 a.m., mVeq | 39.729 ± 20.588 | 25.244 ± 8.132 | 0.1250 |
| Awake time IOP SD, mVeq | 103.148 ± 60.864 | 94.902 ± 44.280 | 0.3716 |
| Awake time IOP SD before 3 p.m., mVeq | 36.601 ± 6.086 | 31.726 ± 14.034 | 0.1305 |
| Difference between sleep time average IOP and awake time average IOP, mVeq | 118.296 ± 46.641 | 126.745 ± 54.248 | 0.6553 |
| Amplitude of cosine fit curve, mVeq | 122.184 ± 67.493 | 116.234 ± 60.533 | 0.4136 |
| Sleep time AUC of cosine fit curve/ID interval number | 297.668 ± 112.092 | 205.650 ± 124.905 | 0.0570 |
| GAT, mmHg | 13.167 ± 2.714 | 12.333 ± 1.751 | 0.1446 |
| CLS Parameter | Case Number 1 | Case Number 3 | Average |
|---|---|---|---|
| Awake-time maximum, mVeq | 71.5/383.95 (18.6%) | 134.3/335.55 (39.9%) | 29.25% |
| Awake-time fluctuation, mVeq | 194.8/445.6 (43.7%) | 153.9/399.45 (38.5%) | 41.1% |
| Sleep-time maximum, mVeq | 24.6/352.5 (7%) | 56.1/311.35 (18.0%) | 12.5% |
| Sleep-time fluctuation, mVeq | 37.1/125.35 (29.6%) | 21/99.1 (21.2%) | 25.4% |
| Case Number 1 | Case Number 4 | |
|---|---|---|
| Pearson’s correlation between CLS IOP and ic200 IOP | 0.370 | 0.558 |
| Circadian IOP fluctuation of ic200, mmHg | 5.9 | 4.1 |
| Amplitude of cosine fit curve of CLS, mVeq | 184.13 | 109.52 |
| Circadian IOP fluctuation of ic200/amplitude of CLS | 0.032 | 0.037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-K.; Ishii, M.; Mizuki, Y.; Kawagoe, T.; Takeuchi, M.; Nomura, E.; Mizuki, N. Circadian Fluctuation Changes in Intraocular Pressure Measured Using a Contact Lens Sensor in Patients with Glaucoma after the Adjunctive Administration of Ripasudil: A Prospective Study. J. Pers. Med. 2023, 13, 800. https://doi.org/10.3390/jpm13050800
Huang S-K, Ishii M, Mizuki Y, Kawagoe T, Takeuchi M, Nomura E, Mizuki N. Circadian Fluctuation Changes in Intraocular Pressure Measured Using a Contact Lens Sensor in Patients with Glaucoma after the Adjunctive Administration of Ripasudil: A Prospective Study. Journal of Personalized Medicine. 2023; 13(5):800. https://doi.org/10.3390/jpm13050800
Chicago/Turabian StyleHuang, Shih-Kung, Mai Ishii, Yuki Mizuki, Tatukata Kawagoe, Masaki Takeuchi, Eiichi Nomura, and Nobuhisa Mizuki. 2023. "Circadian Fluctuation Changes in Intraocular Pressure Measured Using a Contact Lens Sensor in Patients with Glaucoma after the Adjunctive Administration of Ripasudil: A Prospective Study" Journal of Personalized Medicine 13, no. 5: 800. https://doi.org/10.3390/jpm13050800