
The Clinical Significance of Serum Biomarkers of the Intestinal Barrier in Systemic Sclerosis: A Cross-Sectional Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Clinical Assessment
2.3. Laboratory Assessment
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Patients’ Characteristics
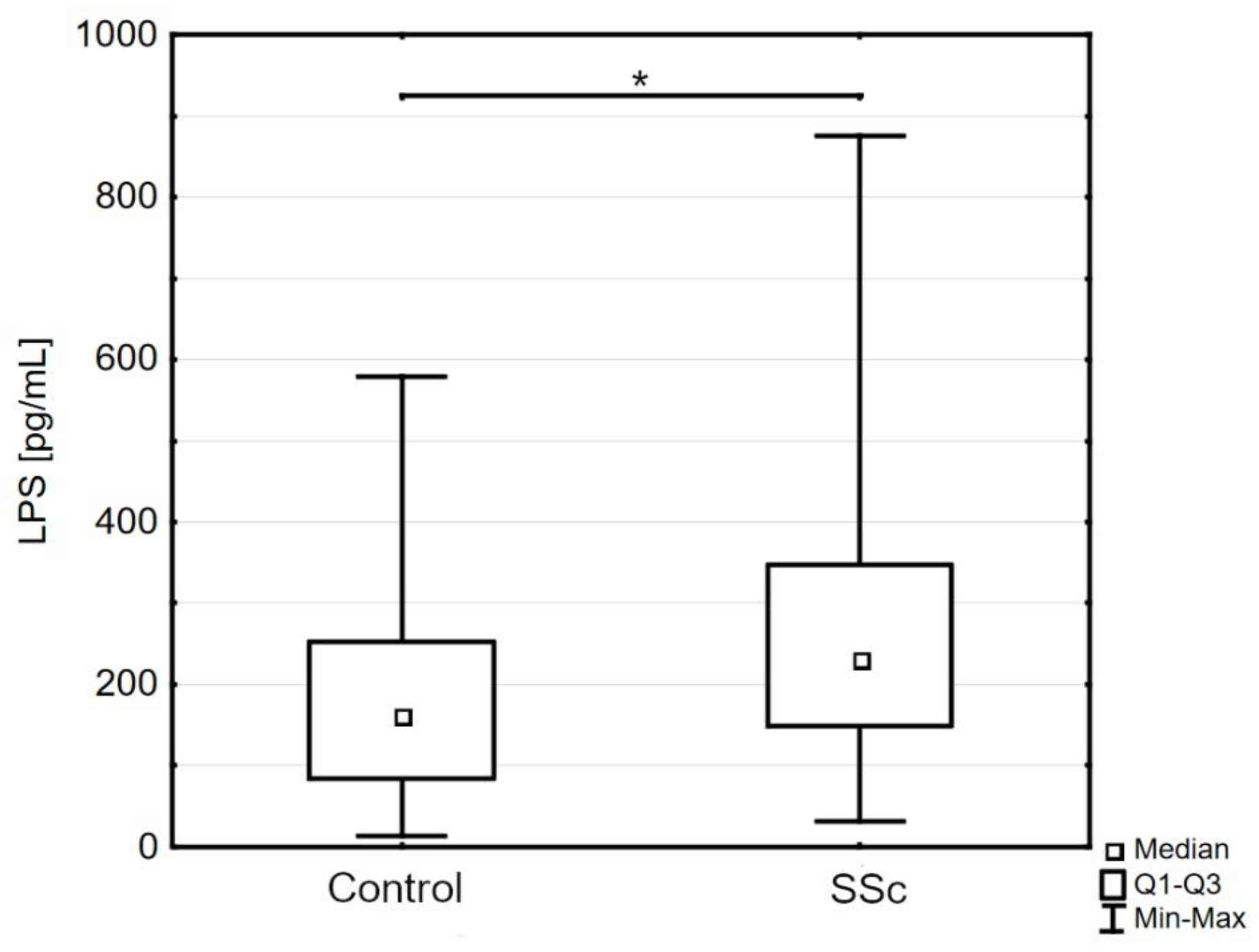
3.2. Markers of Intestinal Permeability in Systemic Sclerosis
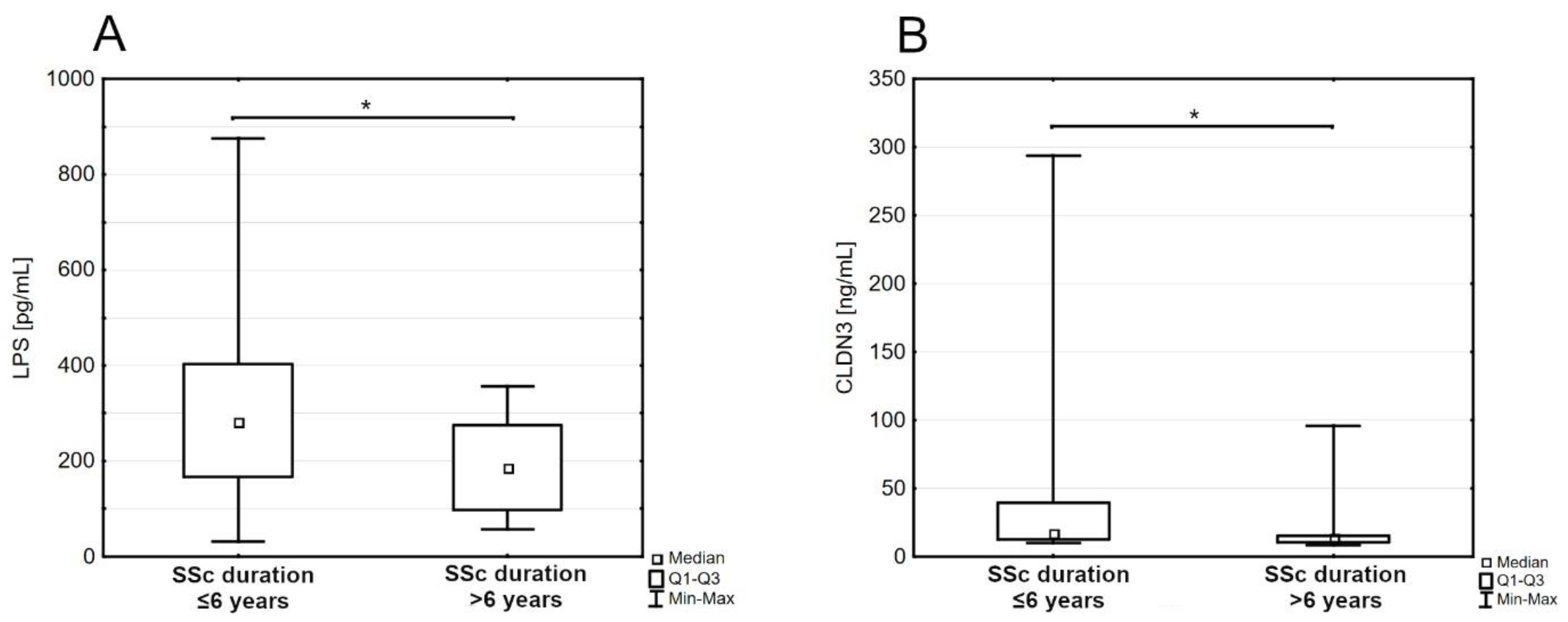
3.3. Markers of Intestinal Permeability in Subgroups of Disease Duration
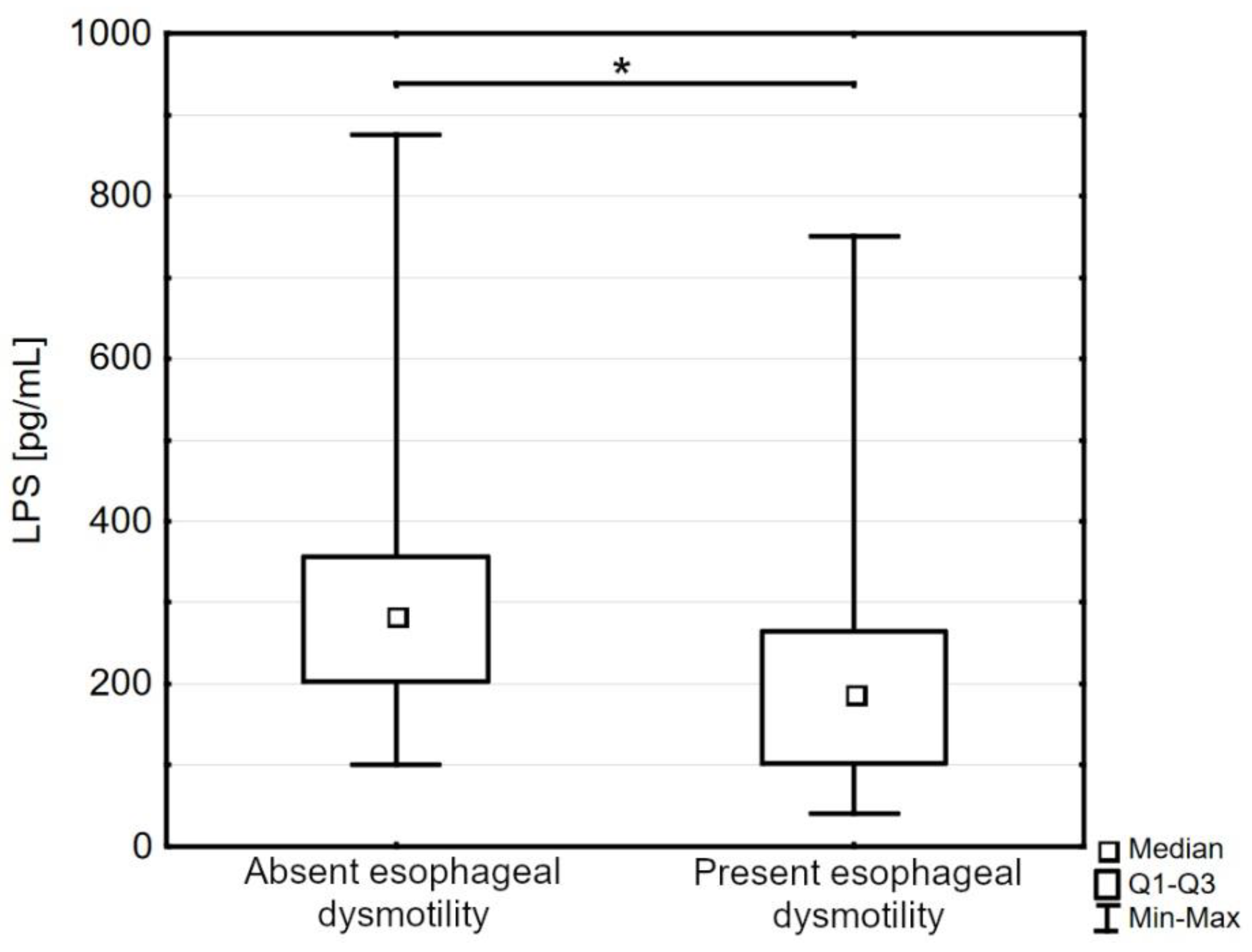
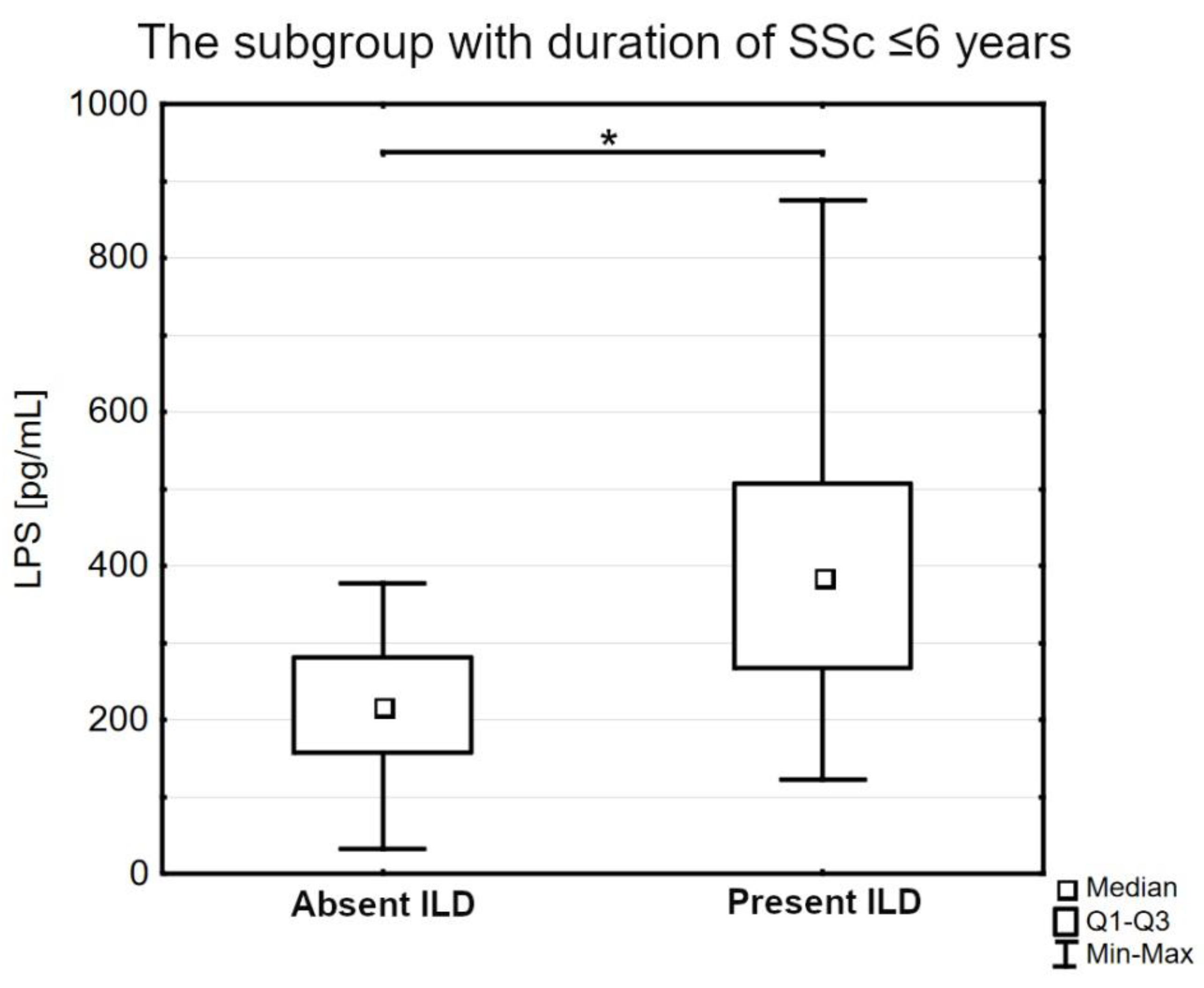
3.4. Lipopolysaccharides (LPS) in Specific Comorbidities of Systemic Sclerosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef] [PubMed]
- Volkmann, E.R.; Hoffmann-Vold, A.M.; Chang, Y.L.; Jacobs, J.P.; Tillisch, K.; Mayer, E.A.; Clements, P.J.; Hov, J.R.; Kummen, M.; Midtvedt, Ø.; et al. Systemic sclerosis is associated with specific alterations in gastrointestinal microbiota in two independent cohorts. BMJ Open Gastroenterol. 2017, 4, e000134. [Google Scholar] [CrossRef] [PubMed]
- Andreasson, K.; Lee, S.M.; Lagishetty, V.; Wu, M.; Howlett, N.; English, J.; Hesselstrand, R.; Clements, P.J.; Jacobs, J.P.; Volkmann, E.R. Disease Features and Gastrointestinal Microbial Composition in Patients with Systemic Sclerosis from Two Independent Cohorts. ACR Open Rheumatol. 2022, 4, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, H.J.; Lee, S.I. The Microbiome in Systemic Sclerosis: Pathophysiology and Therapeutic Potential. Int. J. Mol. Sci. 2022, 23, 16154. [Google Scholar] [CrossRef]
- Sikora, M.; Stec, A.; Chrabaszcz, M.; Knot, A.; Waskiel-Burnat, A.; Rakowska, A.; Olszewska, M.; Rudnicka, L. Gut Microbiome in Psoriasis: An Updated Review. Pathogens 2020, 9, 463. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Guo, F.; Huang, Y.; Li, A.; Chen, S.; Chen, J.; Liu, H.F.; Pan, Q. Gut Microbiota Dysbiosis in Systemic Lupus Erythematosus: Novel Insights into Mechanisms and Promising Therapeutic Strategies. Front. Immunol. 2021, 12, 799788. [Google Scholar] [CrossRef]
- De Pessemier, B.; Grine, L.; Debaere, M.; Maes, A.; Paetzold, B.; Callewaert, C. Gut-Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions. Microorganisms 2021, 9, 353. [Google Scholar] [CrossRef]
- Camilleri, M. Leaky gut: Mechanisms, measurement and clinical implications in humans. Gut 2019, 68, 1516–1526. [Google Scholar] [CrossRef]
- Ghosh, S.S.; Wang, J.; Yannie, P.J.; Ghosh, S. Intestinal Barrier Dysfunction, LPS Translocation, and Disease Development. J. Endocr. Soc. 2020, 4, bvz039. [Google Scholar] [CrossRef]
- Vanuytsel, T.; Tack, J.; Farre, R. The Role of Intestinal Permeability in Gastrointestinal Disorders and Current Methods of Evaluation. Front. Nutr. 2021, 8, 717925. [Google Scholar] [CrossRef]
- Gajda, A.M.; Storch, J. Enterocyte fatty acid-binding proteins (FABPs): Different functions of liver and intestinal FABPs in the intestine. Prostaglandins Leukot. Essent. Fat. Acids 2015, 93, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Barmeyer, C.; Fromm, M.; Schulzke, J.D. Active and passive involvement of claudins in the pathophysiology of intestinal inflammatory diseases. Pflug. Arch 2017, 469, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Kell, D.B.; Pretorius, E. The Role of Lipopolysaccharide-Induced Cell Signalling in Chronic Inflammation. Chronic Stress 2022, 6, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Caserta, L.; de Magistris, L.; Secondulfo, M.; Caravelli, G.; Riegler, G.; Cuomo, G.; D’Angelo, S.; Naclerio, C.; Valentini, G.; Carratù, R. Assessment of intestinal permeability and orocecal transit time in patients with systemic sclerosis: Analysis of relationships with epidemiologic and clinical parameters. Rheumatol. Int. 2003, 23, 226–230. [Google Scholar] [CrossRef]
- Catanoso, M.; Lo Gullo, R.; Giofré, M.R.; Pallio, S.; Tortora, A.; Lo Presti, M.; Frisina, N.; Bagnato, G.; Fries, W. Gastro-intestinal permeability is increased in patients with limited systemic sclerosis. Scand. J. Rheumatol. 2001, 30, 77–81. [Google Scholar] [CrossRef]
- Medsger, T.A., Jr. Natural history of systemic sclerosis and the assessment of disease activity, severity, functional status, and psychologic well-being. Rheum. Dis. Clin. North Am. 2003, 29, 255–273. [Google Scholar] [CrossRef]
- Yanaba, K. Strategy for treatment of fibrosis in systemic sclerosis: Present and future. J. Dermatol. 2016, 43, 46–55. [Google Scholar] [CrossRef]
- Hendel, L.; Kobayasi, T.; Petri, M. Ultrastructure of the small intestinal mucosa in progressive systemic sclerosis (PSS). Acta Pathol. Microbiol. Immunol. Scand A 1987, 95, 41–46. [Google Scholar] [CrossRef]
- O’Reilly, S. Toll-like receptor triggering in systemic sclerosis: Time to target. Rheumatology 2023, 62, SI12–SI19. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Kelley, K.; Melichian, D.S.; Tamaki, Z.; Fang, F.; Su, Y.; Feng, G.; Pope, R.M.; Budinger, G.R.; Mutlu, G.M.; et al. Toll-like receptor 4 signaling augments transforming growth factor-beta responses: A novel mechanism for maintaining and amplifying fibrosis in scleroderma. Am. J. Pathol. 2013, 182, 192–205. [Google Scholar] [CrossRef]
- Li, X.P.; Liu, P.; Li, Y.F.; Zhang, G.L.; Zeng, D.S.; Liu, D.L. LPS induces activation of the TLR4 pathway in fibroblasts and promotes skin scar formation through collagen I and TGF-β in skin lesions. Int. J. Clin. Exp. Pathol. 2019, 12, 2121–2129. [Google Scholar]
- Cutolo, M.; Sulli, A.; Smith, V. Assessing microvascular changes in systemic sclerosis diagnosis and management. Nat. Rev. Rheumatol. 2010, 6, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Zhan, S.; Li, N.; Liu, C.; Mao, R.; Wu, D.; Li, T.; Chen, M.; Zhuang, X.; Zeng, Z. Intestinal Fibrosis and Gut Microbiota: Clues From Other Organs. Front. Microbiol. 2021, 12, 694967. [Google Scholar] [CrossRef] [PubMed]
- Domscheit, H.; Hegeman, M.A.; Carvalho, N.; Spieth, P.M. Molecular Dynamics of Lipopolysaccharide-Induced Lung Injury in Rodents. Front. Physiol. 2020, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Nojiri, T.; Hosoda, H.; Shintani, Y.; Inoue, M.; Miyazato, M.; Okumura, M.; Kangawa, K. Exacerbation of bleomycin-induced injury by lipopolysaccharide in mice: Establishment of a mouse model for acute exacerbation of interstitial lung diseases. Eur. J. Cardiothorac. Surg. 2015, 48, e85–e91. [Google Scholar] [CrossRef] [PubMed]
- Crestani, B.; Seta, N.; De Bandt, M.; Soler, P.; Rolland, C.; Dehoux, M.; Boutten, A.; Dombret, M.C.; Palazzo, E.; Kahn, M.F.; et al. Interleukin 6 secretion by monocytes and alveolar macrophages in systemic sclerosis with lung involvement. Am. J. Respir. Crit. Care Med. 1994, 149, 1260–1265. [Google Scholar] [CrossRef]
- Cardoneanu, A.; Burlui, A.M.; Macovei, L.A.; Bratoiu, I.; Richter, P.; Rezus, E. Targeting Systemic Sclerosis from Pathogenic Mechanisms to Clinical Manifestations: Why IL-6? Biomedicines 2022, 10, 318. [Google Scholar] [CrossRef]
- Kawaguchi, Y. Contribution of Interleukin-6 to the Pathogenesis of Systemic Sclerosis. J. Scleroderma Relat. Disord. 2017, 2, S6–S12. [Google Scholar] [CrossRef]
- Marie, I.; Leroi, A.M.; Gourcerol, G.; Levesque, H.; Menard, J.F.; Ducrotte, P. Fructose Malabsorption in Systemic Sclerosis. Medicine 2015, 94, e1601. [Google Scholar] [CrossRef]
- Marie, I.; Leroi, A.M.; Gourcerol, G.; Levesque, H.; Menard, J.F.; Ducrotte, P. Lactose malabsorption in systemic sclerosis. Aliment. Pharmacol. Ther. 2016, 44, 1123–1133. [Google Scholar] [CrossRef]
- McMahan, Z.H.; Kulkarni, S.; Chen, J.; Chen, J.Z.; Xavier, R.J.; Pasricha, P.J.; Khanna, D. Systemic sclerosis gastrointestinal dysmotility: Risk factors, pathophysiology, diagnosis and management. Nat. Rev. Rheumatol. 2023, 19, 166–181. [Google Scholar] [CrossRef] [PubMed]
- den Braber-Ymker, M.; Vonk, M.C.; Grunberg, K.; Lammens, M.; Nagtegaal, I.D. Intestinal hypomotility in systemic sclerosis: A histological study into the sequence of events. Clin. Rheumatol. 2021, 40, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Pokeerbux, M.R.; Giovannelli, J.; Dauchet, L.; Mouthon, L.; Agard, C.; Lega, J.C.; Allanore, Y.; Jego, P.; Bienvenu, B.; Berthier, S.; et al. Survival and prognosis factors in systemic sclerosis: Data of a French multicenter cohort, systematic review, and meta-analysis of the literature. Arthritis Res. Ther. 2019, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Stec, A.; Sikora, M.; Maciejewska, M.; Paralusz-Stec, K.; Michalska, M.; Sikorska, E.; Rudnicka, L. Bacterial Metabolites: A Link between Gut Microbiota and Dermatological Diseases. Int. J. Mol. Sci. 2023, 24, 3494. [Google Scholar] [CrossRef]
- Gou, H.Z.; Zhang, Y.L.; Ren, L.F.; Li, Z.J.; Zhang, L. How do intestinal probiotics restore the intestinal barrier? Front. Microbiol. 2022, 13, 929346. [Google Scholar] [CrossRef]
- Fortea, M.; Albert-Bayo, M.; Abril-Gil, M.; Ganda Mall, J.P.; Serra-Ruiz, X.; Henao-Paez, A.; Exposito, E.; Gonzalez-Castro, A.M.; Guagnozzi, D.; Lobo, B.; et al. Present and Future Therapeutic Approaches to Barrier Dysfunction. Front. Nutr. 2021, 8, 718093. [Google Scholar] [CrossRef]
- Fretheim, H.; Chung, B.K.; Didriksen, H.; Baekkevold, E.S.; Midtvedt, O.; Brunborg, C.; Holm, K.; Valeur, J.; Tennoe, A.H.; Garen, T.; et al. Fecal microbiota transplantation in systemic sclerosis: A double-blind, placebo-controlled randomized pilot trial. PLoS ONE 2020, 15, e0232739. [Google Scholar] [CrossRef]
- Marighela, T.F.; Arismendi, M.I.; Marvulle, V.; Brunialti, M.K.C.; Salomao, R.; Kayser, C. Effect of probiotics on gastrointestinal symptoms and immune parameters in systemic sclerosis: A randomized placebo-controlled trial. Rheumatology 2019, 58, 1985–1990. [Google Scholar] [CrossRef]
- Low, A.H.L.; Teng, G.G.; Pettersson, S.; de Sessions, P.F.; Ho, E.X.P.; Fan, Q.; Chu, C.W.; Law, A.H.N.; Santosa, A.; Lim, A.Y.N.; et al. A double-blind randomized placebo-controlled trial of probiotics in systemic sclerosis associated gastrointestinal disease. Semin. Arthritis Rheum. 2019, 49, 411–419. [Google Scholar] [CrossRef]
- Strahm, N.; Didriksen, H.; Fretheim, H.; Molberg, O.; Midtvedt, O.; Farstad, I.N.; Midtvedt, T.; Lundin, K.E.A.; Aabakken, L.; Blyszczuk, P.; et al. Effects of faecal microbiota transplantation on small intestinal mucosa in systemic sclerosis. Rheumatology 2023. [Google Scholar] [CrossRef]
- Frech, T.M.; Khanna, D.; Maranian, P.; Frech, E.J.; Sawitzke, A.D.; Murtaugh, M.A. Probiotics for the treatment of systemic sclerosis-associated gastrointestinal bloating/distention. Clin. Exp. Rheumatol. 2011, 29, S22–S25. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systemic Sclerosis (n = 50) | Control (n = 30) | p-Value | |
|---|---|---|---|
| General characteristics | |||
| Age, years | 57 [48–65] | 54 [49–59] | 0.22 |
| Sex, women, n (%) | 42 (84.00%) | 25 (83.33%) | 0.94 |
| Body mass index, kg/m2 | 23.56 [21.31–27.44] | 25.29 [22.35–26.25] | 0.67 |
| Characteristics of systemic sclerosis | |||
| Modified Rodnan skin score | 4 [2–9] | - | - |
| Limited cutaneous systemic sclerosis, n (%) | 27 (54%) | - | - |
| Diffuse cutaneous systemic sclerosis, n (%) | 23 (46%) | - | - |
| Systemic sclerosis duration, years | 6 [4–13] | - | - |
| Autoantibody positivity | |||
| Anticentromere (ACA), n (%) | 23 (46%) | - | - |
| Antitopoisomerase I (ATA), n (%) | 19 (38%) | - | - |
| Anti-RNA polymerase III, n (%) | 5 (10%) | - | - |
| Current treatment | |||
| Methotrexate, n (%) | 12 (24%) | - | - |
| Mycophenolate mofetil, n (%) | 14 (28%) | - | - |
| Calcium channel blockers, n (%) | 9 (18%) | - | - |
| Sildenafil, n (%) | 25 (50%) | - | - |
| Sulodexide, n (%) | 29 (58%) | - | - |
| Prostaglandins, n (%) | 45 (90%) | - | - |
| Pentoxifylline, n (%) | 4 (8%) | - | - |
| Shorter Duration of the Disease (≤6 Years; n = 28) | Longer Duration of the Disease (>6 years; n = 22) | p-Value | |
|---|---|---|---|
| General characteristics | |||
| Age, years | 55.9 ± 11.7 | 57.0 ± 12.3 | 0.70 |
| Sex, women, n (%) | 21 (75.0%) | 21 (95.5%) | 0.12 |
| Body mass index, kg/m2 | 23.1 [21.1–27.5] | 23.8 [21.9–27.4] | 0.70 |
| Characteristics of systemic sclerosis | |||
| Limited cutaneous systemic sclerosis, n (%) | 16 (57.1%) | 11 (50.0%) | 0.62 |
| Diffuse cutaneous systemic sclerosis, n (%) | 12 (42.9%) | 11 (50.0%) | 0.62 |
| Modified Rodnan skin score | 4 [2–6] | 4.5 [2–9] | 0.41 |
| Interstitial lung disease, n (%) | 14 (50.0%) | 19 (86.4%) | 0.02 |
| Diffusing capacity of the lungs for carbon monoxide (DLCO), % | 71.14 ± 21.08 | 72.96 ± 13.62 | 0.62 |
| Left ventricular ejection fraction (LVEF), % | 65 [60–67] | 65 [60–65] | 0.99 |
| Esophageal dysmotility, n (%) | 13 (46.4%) | 14 (63.6%) | 0.55 |
| Autoantibody positivity | |||
| Anticentromere (ACA), n (%) | 16 (57.1%) | 7 (31.8%) | 0.13 |
| Antitopoisomerase I (ATA), n (%) | 9 (32.1%) | 10 (45.5%) | 0.50 |
| Anti-RNA polymerase III, n (%) | 3 (10.7%) | 2 (9.1%) | 0.78 |
| Intestinal barrier parameters | |||
| Intestinal fatty acid binding protein (IFABP), pg/mL | 1375.0 [1060.0–1828.5] | 1534.0 [1108.0–1885.0] | 0.61 |
| Claudin-3 (CLDN3), ng/mL | 16.99 [12.41–39.59] | 13.54 [10.29–15.47] | 0.02 |
| Lipopolysaccharides (LPS), pg/mL | 280.75 [167.30–403.40] | 186.00 [98.12–275.90] | 0.02 |
| Laboratory parameters | |||
| Erythrocyte sedimentation rate, mm/h | 13.0 [6.0–21.0] | 8.5 [7.0–12.0] | 0.41 |
| Estimated glomerular filtration rate (eGFR), mL/min./1.73 m2 | 87.41 ± 19.49 | 79.19 ± 18.28 | 0.15 |
| N-terminal pro b-type natriuretic peptide (NT-proBNP), pg/mL | 126 [74–230] | 145 [64.5–206.5] | 0.90 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stec, A.; Maciejewska, M.; Zaremba, M.; Paralusz-Stec, K.; Michalska, M.; Rudnicka, L.; Sikora, M. The Clinical Significance of Serum Biomarkers of the Intestinal Barrier in Systemic Sclerosis: A Cross-Sectional Study. J. Pers. Med. 2023, 13, 678. https://doi.org/10.3390/jpm13040678
Stec A, Maciejewska M, Zaremba M, Paralusz-Stec K, Michalska M, Rudnicka L, Sikora M. The Clinical Significance of Serum Biomarkers of the Intestinal Barrier in Systemic Sclerosis: A Cross-Sectional Study. Journal of Personalized Medicine. 2023; 13(4):678. https://doi.org/10.3390/jpm13040678
Chicago/Turabian StyleStec, Albert, Magdalena Maciejewska, Michał Zaremba, Karolina Paralusz-Stec, Milena Michalska, Lidia Rudnicka, and Mariusz Sikora. 2023. "The Clinical Significance of Serum Biomarkers of the Intestinal Barrier in Systemic Sclerosis: A Cross-Sectional Study" Journal of Personalized Medicine 13, no. 4: 678. https://doi.org/10.3390/jpm13040678