
Ceftriaxone Administration Associated with Lithiasis in Children: Guilty or Not? A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
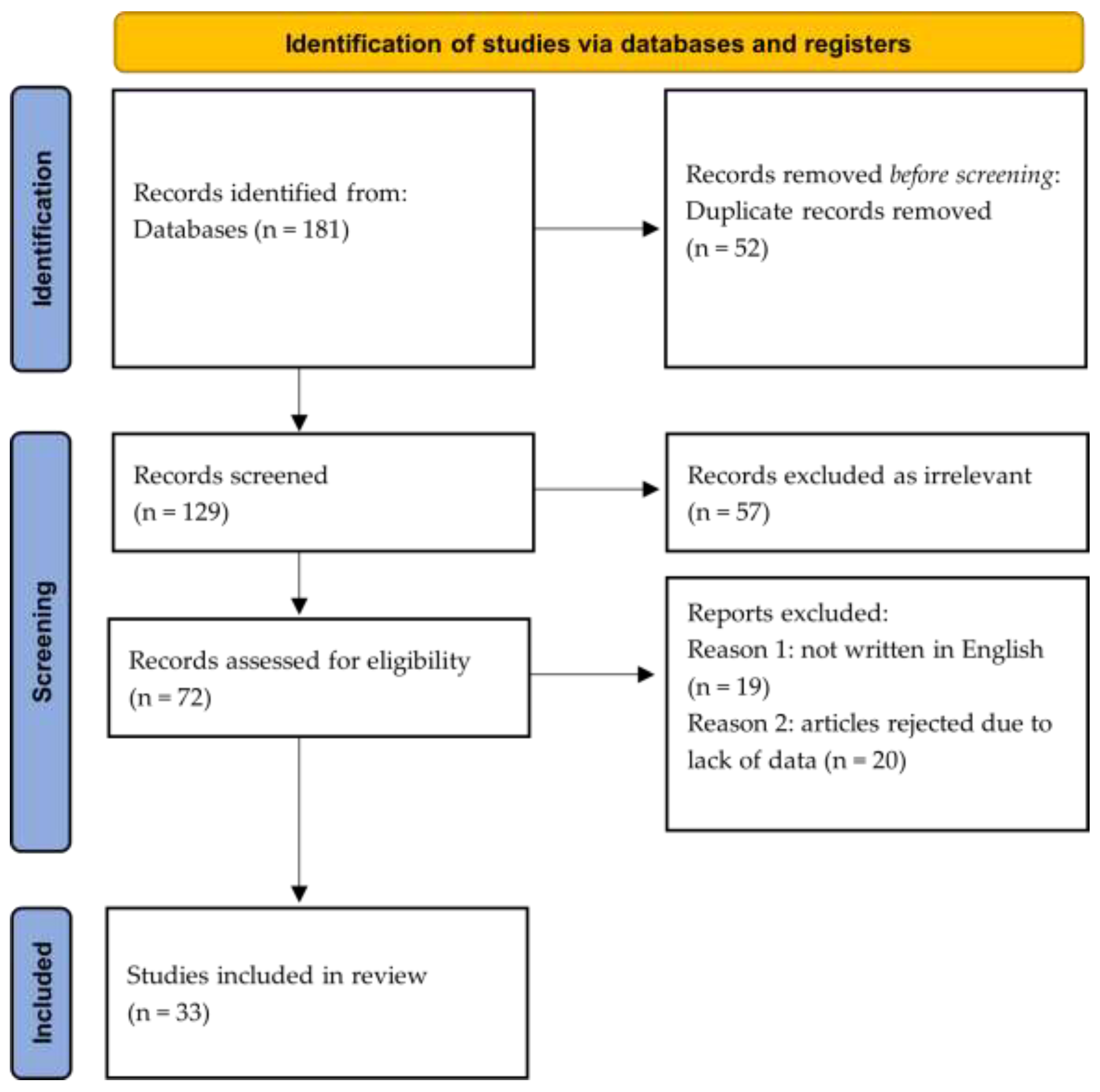
2. Methods
3. Results
4. Discussion
4.1. Biliary Tract Lithiasis
4.2. Urinary Tract Lithiasis
4.3. Combined Biliary and Urinary Tract Lithiasis
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCracken, G.H., Jr.; Siegel, J.D.; Threlkeld, N.; Thomas, M. Ceftriaxone pharmacokinetics in newborn infants. Antimicrob. Agents Chemother. 1983, 23, 341–343. [Google Scholar] [CrossRef]
- Patel, I.H.; Chen, S.; Parsonnet, M.; Hackman, M.R.; Brooks, M.A.; Konikoff, J.; Kaplan, S.A. Pharmacokinetics of ceftriaxone in humans. Antimicrob. Agents Chemother. 1981, 20, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, M.L.; Keith, F.B.; Moore, E.W. Pathogenesis of ceftriaxone-associated biliary sludge. In vitro studies of calcium-ceftriaxone binding and solubility. Gastroenterology 1990, 99, 1772–1778. [Google Scholar] [CrossRef] [PubMed]
- Herek, O.; Pakdemirli, E.; Koçer, N. Ceftriaxone-associated biliary pseudolithiasis in children. Eur. Radiol. 2001, 11, 902. [Google Scholar] [CrossRef] [PubMed]
- Meng, D.; Cao, Y.; Fu, J.; Chen, R.; Lu, L.; Tu, Y. Sonographic assessment of ceftriaxone-associated biliary pseudolithiasis in Chinese children. J. Int. Med. Res. 2010, 38, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Biner, B.; Oner, N.; Celtik, C.; Bostancioglu, M.; Tuncbilek, N.; Guzel, A.; Karasalihoglu, S. Ceftriaxone-associated biliary pseudolithiasis in children. J. Clin. Ultrasound. 2006, 34, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Cuzzolin, L.; Oggiano, A.M.; Clemente, M.G.; Locci, C.; Antonucci, L.; Antonucci, R. Ceftriaxone-associated biliary pseudolithiasis in children: Do we know enough? Fundam. Clin. Pharmacol. 2021, 35, 40–52. [Google Scholar] [CrossRef]
- Doi, Y.; Takii, Y.; Ito, H.; Jingu, N.; To, K.; Kimura, S.; Kimura, K.; Sanefuji, K.; Ikeda, H.; Tachibana, S.; et al. Usefulness of endoscopic managements in patients with ceftriaxone-induced pseudolithiasis causing biliary obstruction. Case Rep. Med. 2017, 2017, 3835825. [Google Scholar] [CrossRef]
- Kim, S.; Gura, K.M.; Puder, M. Acute necrotizing cholecystitis: A rare complication of ceftriaxone-associated pseudo-lithiasis. Pediatr. Surg. Int. 2006, 22, 562–564. [Google Scholar] [CrossRef]
- Gokce, S.; Yıldırım, M.; Erdogan, D. A retrospective review of children with gallstone: Single-center experience from Central Anatolia. Turk. J. Gastroenterol. 2014, 25, 46–53. [Google Scholar] [CrossRef]
- Murata, S.; Aomatsu, T.; Yoden, A.; Tamai, H. Fasting and bed rest, even for a relatively short period, are risk factors for ceftriaxone-associated pseudolithiasis. Pediatr. Int. 2015, 57, 942–946. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Bor, O.; Kebapci, M.; Aydogdu, S.D. Ceftriaxone-associated cholelithiasis: 30 min drip infusion versus bolus injection. Pediatr. Int. 2010, 52, 890. [Google Scholar] [CrossRef]
- Troyano-Luque, J.; Padilla-Perez, A.; Martinez-Wallin, I.; Alvarez de la Rosa, M.; Mastrolia, S.A.; Trujillo, J.L.; Perez-Medina, T. Short and long term outcomes associated with fetal cholelithiasis: A report of two cases with antenatal diagnosis and postnatal follow-up. Case Rep. Obstet. Gynecol. 2014, 2014, 714271. [Google Scholar] [CrossRef] [PubMed]
- de Moor, R.A.; Egberts, A.C.; Schröder, C.H. Ceftriaxone-associated nephrolithiasis and biliary pseudolithiasis. Eur. J. Pediatr. 1999, 158, 975–977. [Google Scholar] [CrossRef]
- Tasic, V.; Sofijanova, A.; Avramoski, V. Nephrolithiasis in a child with acute pyelonephritis. Ceftriaxone-induced nephrolithiasis and biliary pseudolithiasis. Pediatr. Nephrol. 2005, 20, 1510–1513. [Google Scholar] [CrossRef] [PubMed]
- Akl, K.F.; Masri, A.T.; Hjazeen, M.M. Acute urine retention induced by ceftriaxone. Saudi J. Kidney Dis. Transplant. 2011, 22, 1226–1228. [Google Scholar]
- Kimata, T.; Kaneko, K.; Takahashi, M.; Hirabayashi, M.; Shimo, T.; Kino, M. Increased urinary calcium excretion caused by ceftriaxone: Possible association with urolithiasis. Pediatr. Nephrol. 2012, 27, 605–609. [Google Scholar] [CrossRef]
- Ito, R.; Yoshida, A.; Taguchi, K.; Enoki, Y.; Yokoyama, Y.; Matsumoto, K. Experimental verification of factors influencing calcium salt formation based on a survey of the development of ceftriaxone-induced gallstone-related disorder. J. Infect. Chemother. 2019, 25, 972–978. [Google Scholar] [CrossRef]
- Stojanovic, V.; Djuric Vijatov, G. Nephrolithiasis caused by ceftriaxone in a 3-year-old child with ureteropelvic junction obstruction. Case Rep. Med. 2009, 2009, 365962. [Google Scholar] [CrossRef] [PubMed]
- Tuna Kirsaclioglu, C.; Çuhacı Çakır, B.; Bayram, G.; Akbıyık, F.; Işık, P.; Tunç, B. Risk factors, complications and out-come of cholelithiasis in children: A retrospective, single-centre review. J. Paediatr. Child Health. 2016, 52, 944–949. [Google Scholar] [CrossRef]
- Joshi, S.; Goldfarb, D.S. The use of antibiotics and risk of kidney stones. Curr. Opin. Nephrol. Hypertens. 2019, 28, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Youssef, D.M.; Sherief, L.M.; Sherbiny, H.S.; El Attar, M.Y.; El Sheikh, A.R.M.; Fawzy, F.M.; Adham, T. Prospective study of nephrolithiasis occurrence in children receiving ceftriaxone. Nephrology 2016, 21, 432–437. [Google Scholar] [CrossRef]
- Du, Y.; Wang, Y.; Xie, J.; Ma, R.; Gao, M.; Xue, J.; Li, X. Ceftriaxone associated biliary pseudolithiasis in a child: A case report and review of the literature. Int. J. Clin. Exp. Med. 2018, 11, 7502–7509. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Alemayehu, H.; Desai, A.A.; Thomas, P.; Sharp, S.W.; St Peter, S.D. Ceftriaxone-induced pseudolithiasis in children treated for perforated appendicitis. Pediatr. Surg. Int. 2014, 30, 323–326. [Google Scholar] [CrossRef]
- Araz, N.; Okan, V.; Demirci, M.; Araz, M. Pseudolithiasis due to ceftriaxone treatment for meningitis in children: Report of 8 cases. Tohoku J. Exp. Med. 2007, 211, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Bor, O.; Dinleyici, E.C.; Kebapci, M.; Aydogdu, S.D. Ceftriaxone-associated biliary sludge and pseudocholelithiasis during childhood: A prospective study. Pediatr. Int. 2004, 46, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Ceran, C.; Oztoprak, I.; Cankorkmaz, L.; Gumus, C.; Yildiz, T.; Koyluoglu, G. Ceftriaxone-associated biliary pseudolithiasis in paediatric surgical patients. Int. J. Antimicrob. Agents 2005, 25, 256–259. [Google Scholar] [CrossRef]
- Dooki, M.R.; Norouzi, A. Cholelithiasis in childhood: A cohort study in north of Iran. Iran J. Pediatr. 2013, 23, 588–592. [Google Scholar]
- Fretzayas, A.; Liapi, O.; Papadopoulou, A.; Nicolaidou, P.; Stamoulakatou, A. Is Ceftriaxone-induced biliary pseudolithiasis influenced by UDP-Glucuronosyltransferase 1A1 gene polymorphisms? Case Rep. Med. 2011, 2011, 730250. [Google Scholar] [CrossRef]
- Krzemien, G.; Ksiazczyk, T.; Szmigielska, A.; Bombinski, P.; Roszkowska-Blaim, M.; Werner, B.; Brzewski, M. Ceftriaxone-associated acute gallbladder enlargement—An unexpected diagnosis in the child with urinary tract infection. Dev. Period. Med. 2015, 19, 182–185. [Google Scholar]
- Kutuya, N.; Ozaki, Y.; Okazaki, T. A symptomatic child with ceftriaxone-associated biliary pseudolithiasis. J. Med. Ultrason. 2008, 35, 125–128. [Google Scholar] [CrossRef]
- Lemberg, D.; Day, A.S.; Wyeth, B. Biliary colic: Is it gallstones? J. Paediatr. Child Health 2005, 41, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, A.; Kaya, M.; Zeyrek, D.; Ozturk, E.; Kat, N.; Ziylan, S.Z. Ultrasonographic findings in ceftriaxone: Associated biliary sludge and pseudolithiasis in children. Acta Radiol. 2005, 46, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Palanduz, A.; Yalçin, I.; Tonguç, E.; Guler, N.; Ones, U.; Salman, N.; Somer, A. Sonographic assessment of ceftriaxone-associated biliary pseudolithiasis in children. J. Clin. Ultrasound. 2000, 28, 166–168. [Google Scholar] [CrossRef]
- Rozmanic, V.; Banac, S.; Ivosevic, D.; Cace, N. Biliary colic and sonographic evidence of pseudocholelithiasis 36 h after treatment with ceftriaxone. J. Paediatr. Child Health 2006, 42, 658–659. [Google Scholar] [CrossRef]
- Soysal, A.; Eraşov, K.; Akpinar, I.; Bakir, M. Biliary precipitation during ceftriaxone therapy: Frequency and risk factors. Turk. J. Pediatr. 2007, 49, 404–407. [Google Scholar]
- von Martels, J.Z.H.; Van de Meeberg, E.K.; Holman, M.; Ligtenberg, J.J.; Ter Maaten, J.C. Pseudolithiasis after recent use of ceftriaxone: An unexpected diagnosis in a child with abdominal pain. Am. J. Emerg. Med. 2013, 31, 1294.e5–1294.e6. [Google Scholar] [CrossRef] [PubMed]
- Avci, Z.; Koktener, A.; Uras, N.; Catal, F.; Karadag, A.; Tekin, O.; Degirmencioglu, H.; Baskin, E. Nephrolithiasis associated with ceftriaxone therapy: A prospective study in 51 children. Arch. Dis. Child. 2004, 89, 1069–1072. [Google Scholar] [CrossRef]
- Lozanovski, V.J.; Gucev, Z.; Avramoski, V.J.; Kirovski, I.; Makreski, P.; Tasic, V. Ceftriaxone associated urolithiasis in a child with hypercalciuria. Hippokratia 2011, 15, 181–183. [Google Scholar]
- Mohkam, M.; Karimi, A.; Gharib, A.; Daneshmand, H.; Khatami, A.; Ghojevand, N.; Sharifian, M. Ceftriaxone associated nephrolithiasis: A prospective study in 284 children. Pediatr. Nephrol. 2007, 22, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Liu, W.; Fang, X.; Jia, J.; Lin, H.; Xu, M.; Geng, H. Acute kidney injury caused by ceftriaxone-induced urolithiasis in children: A single-institutional experience in diagnosis, treatment, and follow-up. Int. Urol. Nephrol. 2014, 46, 1909–1914. [Google Scholar] [CrossRef] [PubMed]
- Acun, C.; Erdem, L.O.; Sogut, A.; Erdem, C.Z.; Tomac, N.; Gundogdu, S. Ceftriaxone-induced biliary pseudolithiasis, and urinary bladder sludge. Pediatr. Int. 2004, 46, 368–370. [Google Scholar] [CrossRef] [PubMed]
- Fesharakinia, A.; Ehsanbakhsh, A.R.; Ghorashadizadeh, N. Ceftriaxone-associated nephrolithiasis in children. Iran J. Pediatr. 2013, 23, 643–647. [Google Scholar] [PubMed]
- Prince, J.S.; Senac, M.O., Jr. Ceftriaxone-associated nephrolithiasis, and biliary pseudolithiasis in a child. Pediatr. Radiol. 2003, 33, 648–651. [Google Scholar] [CrossRef]
- Ustyol, L.; Bulut, M.D.; Agengin, K.; Bala, K.A.; Yavuz, A.; Bora, A.; Demiroren, K.; Dogan, M. Comparative evaluation of ceftriaxone-and cefotaxime-induced biliary pseudolithiasis or nephrolithiasis: A prospective study in 154 children. Hum. Exp. Toxicol. 2017, 36, 547–553. [Google Scholar] [CrossRef]
- Chandra, P.; Brouwer, K.L. The complexities of hepatic drug transport: Current knowledge and emerging concepts. Pharm. Res. 2004, 21, 719–735. [Google Scholar] [CrossRef]
- Bogue, C.O.; Murphy, A.J.; Gerstle, J.T.; Moineddin, R.; Daneman, A. Risk factors, complications, and outcomes of gallstones in children: A single-center review. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 303–308. [Google Scholar] [CrossRef]
- Daudon, M.; Frochot, V.; Bazin, D.; Paul Jungers, P. Drug-Induced kidney stones and crystalline nephropathy: Pathophysiology, prevention, and treatment. Drugs 2018, 78, 163–201. [Google Scholar] [CrossRef]
- Lehr, D. Clinical toxicity of sulfonamides. Ann. N. Y. Acad. Sci. 1957, 69, 417–447. [Google Scholar] [CrossRef]
- Daudon, M.; Jungers, P. Drug-induced renal calculi: Epidemiology, prevention, and management. Drugs 2004, 64, 245–275. [Google Scholar] [CrossRef]
- Matlaga, B.R.; Shah, O.D.; Assimos, D.G. Drug-induced urinary calculi. Rev. Urol. 2003, 5, 227–231. [Google Scholar] [PubMed]
- Karliczek, S.B.; Döring, S.; Vogt, S.; Beintker, M.; Berg, W.; Misselwitz, J. Ceftriaxone-associated nephrolithiasis: Two case reports. Monatsschr. Kinderheilkd. 1996, 144, 702–706. [Google Scholar]
- Rapado, A.; Traba, M.L.; Caycho, C.; Cifuentes-Delatte, L. Drug-induced renal stones: Incidence, clinical expression and stone analysis. Contrib. Nephrol. 1987, 58, 25–29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Citation | Study Type | Study Patients (n) | Age, Gender | Clinical Information, Treatment | Main Outcomes |
|---|---|---|---|---|---|
| Alemayehu et al. [25] | Retrospective | n = 71 Stones or calcification in the gallbladder were found in n = 10 (14%) patients. mean age 10.0 ± 4.9 y. | Mean age: 10.8 ± 3.8 yr Gender undefined | Ceftriaxone 50 mg/kg, max. dose 2 g, infusion over 10 min. Mean duration of treatment: 8.7 ± 3.8 d. Postoperative administration for laparoscopic appendectomy. | Ultrasound on 11.5 ± 10.3 d of treatment showed biliary lithiasis. Nonsignificant difference in duration of ceftriaxone treatment between patients who presented gallbladder lithiasis compared to those that did not. Duration of administration was considered not important for lithiasis. Lack of uniformity in the timing of repeat imaging after initiation of treatment. Resolution except for one symptomatic patient who underwent cholecystectomy. |
| Araz et al. [26] | Case Reports | n = 8 | Age range: 3–9 yr Mean: 6 ± 2 yr Females: n = 1 Males n = 7 | Ceftriaxone 100 mg/kg/d bolus, n = 8 patients. Sultamicillin 100–200 mg/kg/d: n = 2 patients. Penicillin-G 100.000 U/kg/d: n = 2 patients. Meningitis. | Ultrasound on 7 ± 1 d of treatment. Biliary calcification: n = 1. Gallstones: n = 3. Biliary calcification and gallstones: n = 4. Normal ultrasound in all patients at 41 ± 23 d after discontinuation of ceftriaxone treatment. High summer temperature (n = 6 patients) inferred as possible risk factor of lithiasis. |
| Bor et al. [27] | Prospective | n = 38 Patients with lithiasis: n = 14 (36.8%). Gender undefined. | Females: n = 37 Males: n = 13 | Ceftriaxone 100 mg/kg/d in two equal bolus doses, infusion time 1–2 min. Meningitis, salmonellosis, gastroenteritis, urinary tract infections, respiratory tract infections, fever of unknown origin. | Abnormal ultrasound after 10 d: n = 14 (36.8%). Cholelithiasis n = 11 (28.9%) and biliary calcification: n = 3 (7.9%). Cholelithiasis after 30 d in patients with abnormal ultrasound: n = 2. Cholelithiasis on 60 d: n = 1. All cases resolved spontaneously during a maximum period of 90 d. |
| Ceran et al. [28] | Prospective | n = 50 Lithiasis was present in 13 (26%), with an age range of 6.8 ± 4.5 yr. | Age range: 6 mo–16 yr Females: n = 14 Males: n = 18 | Ceftriaxone 100 mg/kg/d in two bolus doses for 3–10 d. Pediatric surgical patients were exposed to starvation because of surgery. | Ultrasonographic biliary pathology: n = 13 Resolution of ultrasound findings 7 d after ceftriaxone discontinuation. Duration of administration, age, starvation, and gender were nonsignificant factors for lithiasis. |
| Dinleyici et al. [12] | Prospective | n = 32 Abnormal gallbladder: n = 9, 28.1%. Cholelithiasis: n = 3, 9.3%. Biliary calcification: n = 6, 18.7%. | Ceftriaxone 100 mg/kg/d in 2 doses of drip infusion (30 min). Community-acquired pneumonia, urinary tract infection, meningitis. | Ultrasound at 10 d performed 4–8 h after fasting. Cholelithiasis persisted on ultrasound in male patients of 7 yr with bacterial meningitis (3.1%) and resolved 60 d after therapy. Compared to bolus (older study), drip infusion resulted in significantly less abnormal gallbladder and cholelithiasis. | |
| Dooki et al. [29] | Retrospective | n = 66 Cholelithiasis: n = 18 (27.3%). | Age range: 2 mo–17 yr Mean: 6.6 ± 4.5 yr Females: n = 27 Males: n = 39 | Study on ultrasound follow-up of cholelithiasis of different etiologies. | Ceftriaxone administration was the most common predisposing factor of pediatric cholelithiasis among a variety of aetiology. |
| Du et al. [23] | Case report | n = 1 | Male, 9 yr | Fungal pneumonia and central nervous system infection. Free history of lithiasis prior. Administered ceftriaxone 2 g/d for 50 d, together with fluconazole, ambroxol hydrochloride, and vancomycin. Ursodeoxycholic acid administered 2 wk before hospital discharge. | Hepatic dysfunction, gallbladder sediment, and pathologic biochemical liver tests. CT scan showed reduction in gallbladder volume 5 d after ceftriaxone discontinuation. Gallbladder abnormalities disappeared after 4 mo. |
| Fretzayas et al. [30] | Case Report | n = 3 | Female: (n = 1), 5.5 mo, Males: (n (n = 2), 18 mo, and 4 yr | Ceftriaxone 100 mg/kg/d for 10–14 d. Urinary tract infection. Genetic anomalies. | All patients presented gallbladder pseudolithiasis. Ultrasound findings: intense, mobile, and echogenic material with acoustic shadow. Reduced function of UDP-glucuronosyltransferase encoded by UGT1A1 gene (due to UGT1A1 gene polymorphisms found in all patients) seems to be compatible with pseudolithiasis. |
| Gokce et al. [10] | Retrospective | n = 124 Cephalosporin was administered in n = 16 asymptomatic and n = 7 symptomatic patients with lithiasis. | Mean age: 9 yr Females: n = 63 (Mean: 10.5 yr) Males: n = 61 (Mean: 7 yr) | Study on patients with cholelithiasis of various etiologies. Symptomatic lithiasis: n = 76 (61%). Asymptomatic lithiasis: n = 48 (39%). Ceftriaxone was studied as a possible risk factor. | The risk factors of lithiasis in the symptomatic infant subgroup (n = 7) were ceftriaxone use in one (14.3%), prematurity plus ceftriaxone use in one (14.3%), and dehydration plus ceftriaxone use in one (14.3%). In the asymptomatic infant subgroup (n = 11), ceftriaxone was administered in 4 (36.4%) patients, as it was considered a risk factor as well. |
| Ito et al. [18] | Retrospective | n = 136 Gallstones presented within 14 d (median 9 d) after administration in 75% of patients in both groups. | Females: n = 76 Males: n = 57 Nondetermined gender: n = 3 Patients under 10 yr: n = 53 | The study aimed to clarify the factors that favor ceftriaxone and calcium binding and to investigate ceftriaxone-calcium salt formation in vitro. Maximum dose of ceftriaxone: adults: 2 g/d, children: 60 mg/kg/d, which were considered as the upper limits of the normal dose. The study included both children and adults divided into two groups according to age. | Excessive dosage of ceftriaxone was associated with lithiasis. Calcium and pH were factors influencing salt formation. Gender did not affect lithiasis. It is of interest that dose was above normal in 73% of the younger group. Lithiasis occurred more frequently in children compared to adults. Clinical outcomes were tested in vitro. |
| Krzemien et al. [31] | Case Report | n = 1 | Male, 5 mo | Ceftriaxone 100 mg/kg/d. Acute pyelonephritis. | After 5 and 11 d of treatment, there was gallbladder enlargement. Therapy continued for 10 d. Gallbladder size became normal after 6 wk. |
| Kutuya et al. [32] | Case Report | n = 1 | Male, 5 y | Ceftriaxone 2 g/d in two doses. Pneumonia. | Abdominal pain after 1 wk of treatment. Ultrasound showed a hyperechoic band within a collapsed gallbladder. Therapy was disrupted after diagnosis of lithiasis. At 8 d of treatment, ultrasound showed echoes within the gallbladder neck and the common bile duct and dilatation of the bile duct. At 11 d, there was calcification in the gallbladder. At 13 d, ultrasound findings were normal. |
| Lemberg et al. [33] | Case Report | n = 1 | Female, 6 y | Empiric treatment with ceftriaxone and acyclovir. Presumptive meningitis. | Abdominal pain 4 d after hospital admission, with positive Murphy’s sign and high fever. Ultrasound showed a gallstone within the gallbladder. Normal ultrasound findings 3 wk after discharge. |
| Meng et al. [5] | Prospective | n = 108 Ceftriaxone 30–80 mg/kg/d for 1–3 wk in n = 58 patients (32 with biliary tract infection and 26 with pneumonia). | Age range: 9 mo–11 yr Mean: 33 mo Females: n = 52 Males: n = 56 | Cephalosporins were administered for biliary tract infection and pneumonia. Ceftazidime 50–100 mg/kg/d for equal period in n = 50 patients (29 with biliary tract infection and 21 with pneumonia). | Biliary gallstones and calcification were detected in 25 patients under ceftriaxone and 1 patient under ceftazidime. Gallstone formation was significantly higher in the ceftriaxone group. Resolution of symptoms occurred 1–2 d after discontinuation of treatment. Resolution of ultrasound findings occurred 7–14 d after discontinuation of treatment. |
| Murata et al. [11] | Retrospective | n = 60 Biliary pseudolithiasis: n = 11 (18.3%). | Age range: 2–13 yr Females: n = 37 Males: n = 23 | Ceftriaxone 100 mg/kg/d administered over 30 min for acute otitis media, gastroenteritis, tonsillitis, upper urinary tract infection, Kawasaki disease, phlegmon, peritonsillar abscess, cervical lymphadenitis. Fasting and bed rest were studied factors. | Pseudolithiasis occurred even in lower doses < 60 mg/kg/d. Higher risk of lithiasis was shown in patients who fasted (presented at 4–8 d) and bed rest (1–5 d). |
| Ozturk et al. [34] | Prospective | n = 33 Pseudolithiasis and gallbladder calcification: n = 19 (57.5%). | Mean: 76.2 ± 54.8 mo Females: n = 14 Males: n = 19 | Ceftriaxone 100 mg/kg/d administered for postoperative prophylaxis (n = 13) and infection (n = 30). | Lithiasis presentation occurred between 4–8 d. Spontaneous resolution occurred within 4–21 d. |
| Palanduz et al. [35] | Retrospective | n = 118 Total gallbladder abnormalities detected: n = 20 (17%), including calcification (n = 8) and pseudolithiasis (n = 12). | Age range: 3 mo–14 yr Females: n = 66 Males: n = 52 | Ceftriaxone 100 mg/kg/d in 2 doses over 30 min for 1–3 wk for severe infection. Study on biliary lithiasis in two groups of abnormal and normal ultrasound findings. | Detection period: 5–11 d (mean 9.1 ± 1.2 d). Resolution period: 2 wk (mean 8.2 ± 3.4 d). Age, gender, and duration of treatment were not significant factors. |
| Rozmanic et al. [36] | Case report | n = 1 | Female, 9 yr | Ceftriaxone 90 mg/kg/d in a daily bolus dose for bacterial infection. | Cholelithiasis presentation after 35 h of treatment. Spontaneous resolution 2 d after treatment was discontinued. |
| Soysal et al. [37] | Randomized Controlled Trial | n = 114 At 5 d, there was biliary calcification (n = 14) and biliary lithiasis (n = 10). At 10 d, there was biliary calcification in 20 and lithiasis in 15 patients. In total, 35 patients (31%) presented biliary precipitations | Age range: 2–180 mo Mean age: 47.5 ± 46.3 mo Females: n = 56 Males: n = 58 | Ceftriaxone infused over 30 min (n = 47), bolus over 2 min (n = 47) or intramuscular (n = 20). Mean duration of treatment: 7 d (3–14 d). Biliary ultrasonography was performed at the time of randomization before treatment was started at 5 and 10 d, and at the end of the treatment. If calcification was detected, weekly ultrasound follow-up until resolution. | Resolution occurred 10–45 d after discontinuation of treatment. Age over 12 mo, dose of more than 2 g, and duration of therapy longer than 5 d were associated with biliary precipitations. |
| Tuna Kirsaclioglu et al. [20] | Retrospective | n = 254 51 patients presented ceftriaxone-related cholelithiasis, and 7 of them presented cholecystitis. | Age range: 0.08–18 yr Mean: 8.9 ± 5.2 yr Females: n = 134 Males: n = 120 | 150 patients presented symptomatic and 159 asymptomatic cases of cholelithiasis of different etiologies, with ceftriaxone-related cases among them. Symptomatic patients were significantly older than the asymptomatic ones. 64 patients presented drug-related cholelithiasis. | Patients whose gallstones dissolved were significantly younger (mean age 8 ± 5.2 yr) compared to older (mean age 9.5 ± 5 yr). Ultrasound showed 40 patients under ceftriaxone with gallstones and 11 with calcification. Ceftriaxone-related cholelithiasis presented significant greater tendency for resolution compared to other etiologies. Ursodeoxycholic acid did not affect resolution time. |
| von Martels et al. [38] | Case Report | n = 1 | Male, 14 yr | Abdominal pain started 4 d after discontinuation of ceftriaxone administration and continued for additional 7 d. History of ceftriaxone 4 g/d for 2 wk for Lyme arthritis. | ERCP performed Dilated intrahepatic ducts and multiple biliary precipitations in the gallbladder. After 4 mo, no gallbladder abnormalities were detected. Resolution upon ceftriaxone discontinuation. |
| Citation | Study Type | Study Patients (n) | Age, Gender | Clinical Information, Treatment | Main Outcomes |
|---|---|---|---|---|---|
| Avci et al. [39] | Prospective | n = 51 Nephrolithiasis: n = 4 (7.8%). | Age: 1 mo–14 yr Mean: 3.1 yr Females: n = 30 Males: n = 21 | Ceftriaxone 100 mg/kg/d. Administered in two daily doses: n = 24. Administered in a single daily dose: n = 27. Ultrasound performed prior to and after treatment of pneumonia, pyelonephritis, lymphadenitis, meningitis, mastoiditis. | Ultrasound findings: small, echogenic calculi within dilated calices. Resolution of lithiasis occurred 3 wk after discontinuation of treatment. One patient’s stone was still present 7 mo after treatment. |
| Kimata et al. [17] | Retrospective | n = 83 | Age: 3 mo–8.9 yr Mean: 30 mo Females: n = 43 Males: n = 40 | Administered for bacterial pneumonia. Study in two groups: Ceftriaxone group: n = 43, mean dose of 91 ± 10 mg/kg/d. Amoxicillin group: n = 40, mean dose of 107 ± 12 mg/kg/d. Serum and urine calcium-to-creatinine ratios were measured. | Urine calcium and calcium-to-creatinine ratio were significantly higher in the ceftriaxone group. This increase occurred after ceftriaxone administration exclusively. |
| Lozanovski et al. [40] | Case Report | n = 1 | Male, 5 yr | Ceftriaxone: 45 mg/kg/d. Pneumonia. | After 7 d of treatment, ceftriaxone was changed to oral cephalosporin, and there was moderate hypercalciuria without abnormal ultrasound findings. After 9 d of treatment, there were three calculi of calcium ceftriaxonate and hypercalciuria. |
| Mohkam et al. [41] | Prospective | n = 284 Ultrasound findings at 10 d: renal lithiasis in 4 patients (1.4%). | Age: 2 mo–12 yr Mean: 2.67 ± 2.10 yr Females: n = 185 Males: n = 99 | Ceftriaxone: 75 mg/kg/d for at least 10 d. Pyelonephritis. | Normal ultrasound after 3 mo. Spontaneous resolution of lithiasis occurred in all patients. |
| Shen et al. [42] | Retrospective | n = 15 Multiple calculi in the upper urinary tract. Bilateral ureteral stones (n = 9, 60%). | Age: 5 mo–11 yr Mean: 4.76 ± 3.74 yr Females: n = 3 Males: n = 12 | Ceftriaxone 1 g in one dose for 5 d. Acute kidney injury from ceftriaxone-induced urolithiasis. | No stones in ureters and kidneys 5 d after intervention (n = 5, 33.3%). One patient operated. All patients were followed up for 11 mo–5 yr. No recurrent urolithiasis was found. |
| Stojanovic et al. [19] | Care Report | n = 1 | Male, 3 yr | Henoch Schönlein purpura complicated with pneumonia. Ceftriaxone: 100 mg/kg/d. | After 6 d of ceftriaxone administration, abdominal pain and vomit presented. Ultrasound showed calculi in the renal calyces. Immediate discontinuation of antibiotic treatment resulted in resolution of symptoms. No urinary calculi 3 wk after end of ceftriaxone administration. |
| Youssef et al. [22] | Prospective | n = 120 In the ceftriaxone group, 5 patients presented small calculi, spontaneously eliminated after 3 wk, except in one patient with renal stones after 9 mo of treatment. | Mean age: 6.93 ± 1.56 yr (ceftriaxone group) Females: n = 57 Males: n = 63 | A group of 60 patients received ceftriaxone 80 mg/kg/d for 5 d and was compared to an equal number with other antibiotics. Ceftriaxone-related nephrolithiasis was studied. The 5 patients with ceftriaxone-associated nephrolithiasis had gastroenteritis (n = 2), meningitis, bronchopneumonia, and secondary infection after tonsillectomy. | All patients with lithiasis were asymptomatic, and urine calcium levels were normal. Mean age of nephrolithiasis (8.2 yr) was significantly higher than the group without (3.5 yr), showing older age as a possible risk factor. The study concluded that the incidence of renal stones is higher in the patients who receive ceftriaxone compared to other antibiotics. |
| Citation | Study Type | Study Patients (n) | Age, Gender | Clinical Information, Treatment | Main Outcomes |
|---|---|---|---|---|---|
| Acun et al. [43] | Case Report | One patient with ceftriaxone-induced biliary pseudolithiasis and urinary bladder calcification. | Female 5 yr | Ceftriaxone: 100 mg/kg/d in 2 doses. Infusion time over 20 min. Meningitis. | Abdominal pain after 9 d of treatment. Ultrasound: mobile gallbladder stone 1.5 mm in diameter. At 5 d, after ceftriaxone discontinuation: multiple echogenic foci in the gallbladder and calcification in the urinary bladder. At 12 d, after discontinuation: normal ultrasound findings. Urinary bladder calcification has not been reported previously. |
| Biner et al. [6] | Prospective | n = 156 n = 27 (17%) with bladder complications: Females: n = 13 Males: n = 14 One female patient was found with urolithiasis. | Age: 0.5–16 y, Mean: 4.5 ± 3.3 y Females: n = 92 Males: n = 64 | Ceftriaxone: 100, 75, and 50 mg/kg/d for 7–10 d in short bolus injections. Pyelonephritis, pneumonia, meningitis, lymphadenitis, sepsis. | Gallstones: n = 16 (10.3%), calcification: n = 11 (7.1%), renal lithiasis: n = 1 (0.6%). Time of diagnosis range: 3–7 d of treatment. Complete resolution range: 10–30 d. Strong association between complications and age over 5 y, meningitis, high doses (100 mg/kg/d). |
| Fesharakinia et al. [44] | Prospective | n = 96 Persistent lithiasis after treatment: renal (n = 6), gallbladder (n = 1). | Age: 1 m–13 y Mean: 1.88 ± 1.98 y Females: n = 41 Males: n = 55 | Ceftriaxone: 50–100 mg/kg/d in 2 doses in 15 min per dose. Infections included: gastroenteritis, pneumonia, septicemia, sinusitis, pyelonephritis, and febrile convulsion with acute otitis media. | Male gender significantly related to nephrolithiasis. Follow-up was defective (participants did not reappear for further examinations). |
| Prince et al. [45] | Case report | n = 1 CT scan at 8 d showed high-density material in the gallbladder, both renal pelvises and ureters. | Male, 14 yr | Ceftriaxone: 4 g/d and metronidazole. Sinusitis complicated by epidural abscess. | Immediate discontinuation of ceftriaxone and replacement by meropenem. Cystoscopy, after 9 d, revealed material in the ureters, and ureteral stents were placed. CT scan at 11 d showed decreased amount of biliary calcification and ureteral debris. CT scan after 3 wk showed complete resolution of lithiasis. |
| Ustyol et al. [46] | Prospective | n = 154 In the ceftriaxone group, 13 patients presented with biliary lithiasis, 5 with biliary calcification, and one with nephrolithiasis, while in the cefotaxime group, there were 4 patients with biliary calcification and one with nephrolithiasis. | Age: 2 mo–18 yr Mean: 4.77 ± 4.91 yr (ceftriaxone group) Females: n = 76 Males: n = 78 | One group (n = 86) received ceftriaxone, and a second group (n = 68) cefotaxime. Intravenous ceftriaxone dose was 100 mg/kg/d, divided into two equal doses. Ceftriaxone administration period was 13 ± 5 d. Infections: pneumonia, pyelonephritis, lymphadenitis, bacterial meningitis, bacteraemia, gastroenteritis, peritonitis | Hypercalciuria was found in the two patients with nephrolithiasis. Abnormal ultrasound biliary findings were significantly higher in the ceftriaxone group. ROC analysis of age risk revealed that 4.5 yr was the cut-off age (sensitivity 70% and specificity 40%). According to the ROC analyses, biliary calcification development risk increased when older than 4.5 yr. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louta, A.; Kanellopoulou, A.; Alexopoulou Prounia, L.; Filippas, M.; Tsami, F.F.; Vlachodimitropoulos, A.; Vezakis, A.; Polydorou, A.; Georgopoulos, I.; Gkentzi, D.; et al. Ceftriaxone Administration Associated with Lithiasis in Children: Guilty or Not? A Systematic Review. J. Pers. Med. 2023, 13, 671. https://doi.org/10.3390/jpm13040671
Louta A, Kanellopoulou A, Alexopoulou Prounia L, Filippas M, Tsami FF, Vlachodimitropoulos A, Vezakis A, Polydorou A, Georgopoulos I, Gkentzi D, et al. Ceftriaxone Administration Associated with Lithiasis in Children: Guilty or Not? A Systematic Review. Journal of Personalized Medicine. 2023; 13(4):671. https://doi.org/10.3390/jpm13040671
Chicago/Turabian StyleLouta, Aspasia, Aimilia Kanellopoulou, Loukia Alexopoulou Prounia, Mathiou Filippas, Faidra Foteini Tsami, Athanasios Vlachodimitropoulos, Antonios Vezakis, Andreas Polydorou, Ioannis Georgopoulos, Despoina Gkentzi, and et al. 2023. "Ceftriaxone Administration Associated with Lithiasis in Children: Guilty or Not? A Systematic Review" Journal of Personalized Medicine 13, no. 4: 671. https://doi.org/10.3390/jpm13040671