
Validation and Application of a Spanish Version of the ALR-RSI Scale (Ankle Ligament Reconstruction—Return to Sport after Injury) in an Active Non-Athlete Population

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Scale
Procedure
- ¿Está seguro de que puede practicar deporte en un nivel anterior a la lesión?Nada seguro (0)…totalmente seguro (10)
- ¿Cree que es probable que vuelva a lesionarse el tobillo al practicar algún deporte?Muy probable (0)…no es probable en absoluto (10)
- ¿Está nervioso por practicar deporte?Extremadamente nervioso (0)…en absoluto nervioso (10)
- ¿Estás seguro de que su tobillo no cederá al practicar su actividad deportiva?Nada seguro (0)…Totalmente confiado (10)
- ¿Estás seguro de que podría practicar su deporte sin preocuparse por su tobillo?Nada seguro (0)…Totalmente confiado (10)
- ¿Le resulta frustrante tener que estar pendiente de su tobillo con respecto a la práctica deportiva (por si vuelve a ocasionar problemas)?Extremadamente frustrante (0)…Nada frustrante (10)
- ¿Tiene miedo de volver a lesionarse el tobillo practicando su deporte?Miedo extremo (0)…Sin miedo en absoluto (10)
- ¿Confía en que su tobillo resista bajo presión?Nada seguro (0)…Totalmente confiado (10)
- ¿Tiene miedo de lesionarse accidentalmente el tobillo al practicar su deporte?Extremadamente asustado (0)…No tengo miedo (10)
- ¿La idea de tener que someterse a una cirugía y rehabilitación le impide practicar su deporte?Todo el tiempo (0)…Ninguna vez (10)
- ¿Confía en su capacidad para la práctica deportiva?Nada seguro (0)…Totalmente confiado (10)
- ¿Se siente relajado/a al practicar deporte?Nada relajado (0)…Completamente relajado (10)
2.3. Statistical Analysis
3. Results
3.1. Exploratory Factor Analysis (EFA)
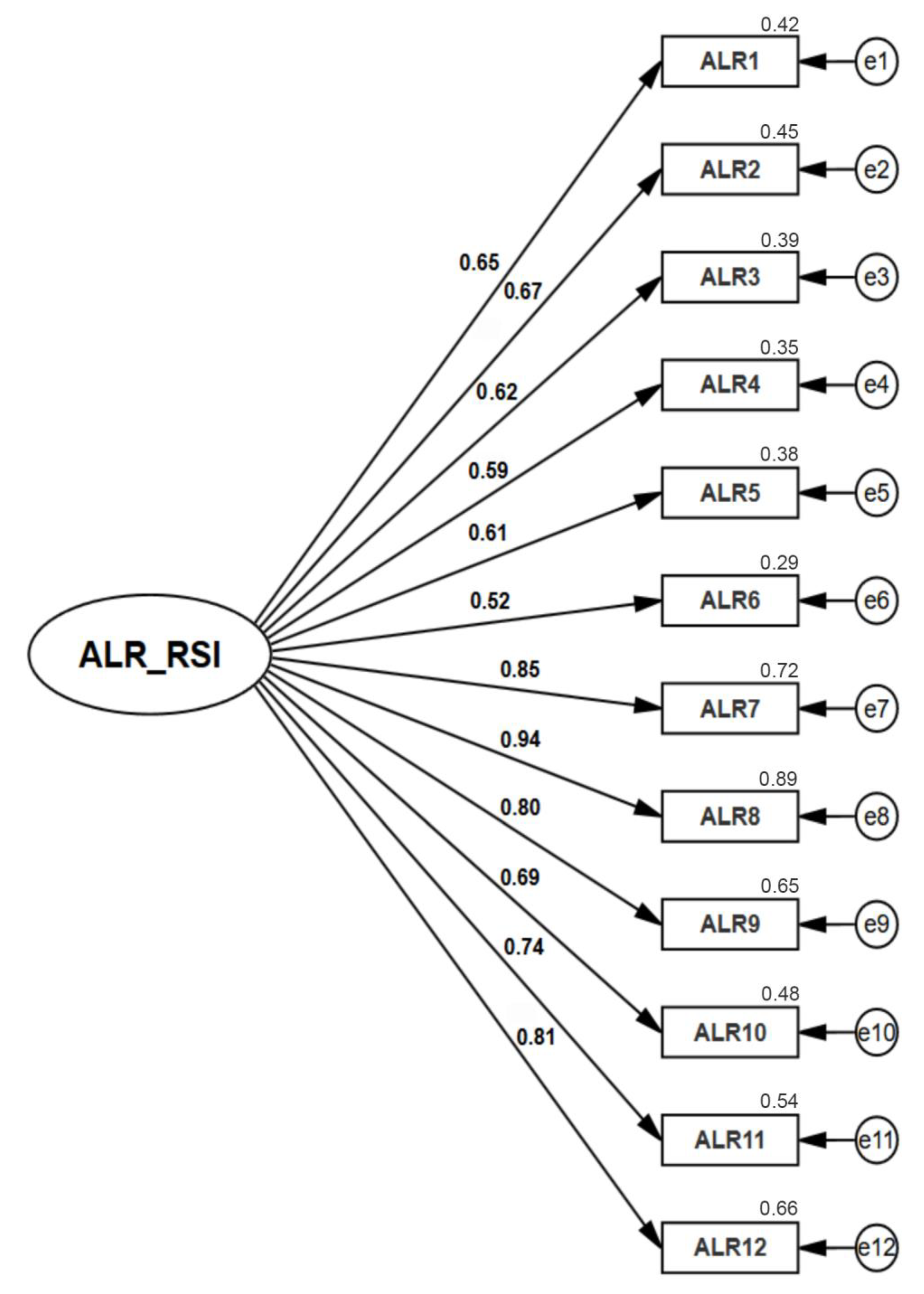
3.2. Confirmatory Factor Analysis (CFA)
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kannus, P.; Renstrom, P. Current concept review: Treatment for scute tears of the lateral ligaments of the ankle. J. Bone Jt. Surg. 1991, 73, 305–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Povacz, P.; Unger, S.F.; Miller, W.K.; Tockner, R.; Resch, H. A randomized, prospective study of operative and non-operative treatment of injuries of the fibular collateral ligaments of the ankle. J. Bone Jt. Surg. Am. 1998, 80, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Nightingale, E.J.; Raymond, J.; Kilbreath, S.L.; Burns, J.; Black, D.A.; Refshauge, K.M. Prevalence and impact of chronic musculoskeletal ankle disorders in the community. Arch. Phys. Med. Rehabil. 2012, 93, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- McCriskin, B.J.; Cameron, K.L.; Orr, J.D.; Waterman, B.R. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J. Orthop. 2015, 6, 161–171. [Google Scholar] [CrossRef]
- Chen, E.; McInnis, K.; Borg-Stein, J. Ankle Sprains: Evaluation, Rehabilitation, and Prevention. Curr. Sports Med. Rep. 2019, 18, 217–223. [Google Scholar] [CrossRef]
- MacAuley, D. Ankle injuries: Same joint, different sports. Med. Sci. Sports Exerc. 1999, 31, 409–411. [Google Scholar] [CrossRef]
- Ananda Coomarasamy, A.; Barnsley, L. Long term outcomes of inversion ankle injuries. Br. J. Sports Med. 2005, 39, 14. [Google Scholar] [CrossRef] [Green Version]
- Verhagen EA, L.M.; Van Tulder, M.; van der Beek, A.J.; Bouter, L.M.; Van Mechelen, W. An economic evaluation of a proprioceptive balance board training programme for the prevention of ankle sprains in volleyball. Br. J. Sports Med. 2005, 39, 111–115. [Google Scholar] [CrossRef]
- Kaminski, T.W.; Hertel, J.; Amendola, N.; Docherty, C.L.; Dolan, M.G.; Hopkins, J.T.; Nussbaum, E.; Poppy, W.; Richie, D. National Athletic Trainers’ Association position statement: Conservative management and prevention of ankle sprains in athletes. J. Athl. Train. 2013, 48, 528–545. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; et al. Consensus statement in return to sport from the First World Congress in Sports Physical Therapy. Bern. Br. J. Sports Med. 2016, 50, 853–864. [Google Scholar] [CrossRef] [Green Version]
- Bjordal, J.M.; Arnly, F.; Hannestad, B.; Strand, T. Epidemiology of anterior cruciate ligament injuries in soccer. Am. J. Sports Med. 1997, 25, 341–345. [Google Scholar] [CrossRef]
- Hamada, M.; Shino, K.; Horibe, S.; Mitsuoka, T.; Miyama, T.; Toritsuka, Y. Preoperative anterior knee laxity did not influence postoperative stability restored by anterior cruciate ligament reconstruction. Arthroscopy 2000, 16, 477–482. [Google Scholar] [CrossRef]
- Kvist, J. Rehabilitation following anterior cruciate ligament injury: Current recommendations for sports participation. Sports Med. 2004, 34, 269–280. [Google Scholar] [CrossRef]
- Mikkelsen, C.; Werner, S.; Eriksson, E. Closed kinetic chain alone compared to combined open and closed kinetic chain exercises for quadriceps strengthening after anterior cruciate ligament reconstruction with respect to return to sports: A prospective matched follow-up study. Knee Surg. Sports Traumatol. Arthrosc. 2000, 8, 337–342. [Google Scholar] [CrossRef]
- VicHealth. Building Health Through Sport: VicHealth Action Plan 2010–2013 Victorian Health Promotion Foundation (VicHealth); VicHealth: Melbourne, Australia, 2010.
- Hambleton, R.K. Adaptación de tests para su uso en diferentes idiomas y culturas: Fuentes de error, posibles soluciones y directrices practices. In Psicometría; Fernández, J.M., Ed.; Complutense University of Madrid: Madrid, Spain, 1996. [Google Scholar]
- Johnston, L.H.; Carroll, D. The context of emotional responses to athletic injury: A qualitative analysis. J. Sport Rehabil. 1998, 7, 208–220. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.M.; Scott, S.G.; O’Fallon, W.M.; Young, M.L. Emotional responses of athletes to injury. Mayo Clin. Proc. 1990, 65, 38–50. [Google Scholar] [CrossRef]
- Junge, A. The influence of psychological factors on sports injuries: Review of the literature. Am. J. Sports Med. 2002, 28, 10–15. [Google Scholar] [CrossRef]
- French, D.J.; France, C.R.; Vigneau, F.; French, J.A.; Evans, R.T. Fear of movement/(re)injury in chronic pain: A psychometric assessment of the original English version of the Tampa scale for kinesiophobia (TSK). Pain 2007, 127, 42–51. [Google Scholar] [CrossRef]
- Thomee, P.; Wahrborg, P.; Borjesson, M.; Thomee, R.; Eriksson, B.I.; Karlsson, J. A new instrument for measuring self-efficacy in patients with an anterior cruciate ligament injury. Scand. J. Med. Sci. Sports 2006, 16, 181–187. [Google Scholar] [CrossRef]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- Murphy, G.C.; Foreman, P.E.; Simpson, C.A.; Molloy, G.N.; Molloy, E.K. The development of a locus of control measure predictive of injured athletes’ adherence to treatment. J. Sci. Med. Sport 1999, 2, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A.; Lambros, C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys. Ther. Sport 2008, 9, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Harput, G.; Tok, D.; Ulusoy, B.; Eraslan, L.; Yildiz, T.I.; Turgut, E.; Demirci, S.; Duzgun, I.; Tunay, V.B.; Baltaci, G.; et al. Translation and cross-cultural adaptation of the anterior cruciate ligament-return to sport after injury (ACL-RSI) scale into Turkish. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Thiebat, G.; Cucchi, D.; Spreafico, A.; Muzzi, S.; Viganò, M.; Visconti, L.; Facchini, F.; de Girolamo, L. Italian version of the anterior cruciate ligament-return to sport after injury scale (IT ACL-RSI): Translation, cross-cultural adaptation, validation and ability to predict the return to sport at medium-term follow-up in a population of sport patients. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 270–279. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef]
- Sala-Barat, E.; Álvarez-Díaz, P.; Alentorn-Geli, E.; Webster, K.E.; Cugat, R.; Tomás-Sabado, J. Translation, cross-cultural adaptation, validation, and measurement properties of the Spanish version of the anterior cruciate ligament-return to sport after injury (ACL-RSI-Sp) scale. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 833–839. [Google Scholar] [CrossRef]
- Slagers, A.J.; Reininga, I.H.; van den Akker-Scheek, I. The Dutch language anterior cruciate ligament return to sport after injury scale (ACL-RSI)—Validity and reliability. J. Sports Sci. 2017, 35, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef]
- Herzog, M.M.; Kerr, Z.Y.; Marshall, S.W.; Wikstrom, E.A. Epidemiology of Ankle Sprains and Chronic Ankle Instability. J. Athl. Train. 2019, 54, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Bohu, Y.; Klouche, S.; Lefevre, N.; Webster, K.; Herman, S. Translation, cross-cultural adaptation and validation of the French version of the anterior cruciate ligament-return to sport after injury (ACL-RSI) scale. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1192–1196. [Google Scholar] [CrossRef]
- Podlog, L.; Heil, J.; Schulte, S. Psychosocial factors in sports injury rehabilitation and return to play. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 915–930. [Google Scholar] [CrossRef]
- Ardern, C.L.; Bizzini, M.; Bahr, R. It is time for consensus onreturn to play after injury: Five key questions. Br. J. Sports Med. 2016, 50, 506–508. [Google Scholar] [CrossRef]


{kind=link}
| n | % | |
|---|---|---|
| Academic training | ||
| Vocational training | 12 | 4.7 |
| Secondary studies | 23 | 8.9 |
| University studies | 222 | 86.4 |
| Weekly physical activity (h) | ||
| 1–5 | 102 | 39.7 |
| 6–10 | 96 | 37.4 |
| 11–15 | 41 | 16 |
| 16–20 | 18 | 7 |
| Fitness | ||
| Good | 180 | 70.1 |
| Average | 71 | 27.6 |
| Poor | 6 | 2.3 |
| Item | Communality | Factor |
|---|---|---|
| ALR1 | 0.731 | 0.703 |
| ALR2 | 0.721 | 0.756 |
| ALR3 | 0.722 | 0.698 |
| ALR4 | 0.8 | 0.852 |
| ALR5 | 0.715 | 0.771 |
| ALR6 | 0.659 | 0.628 |
| ALR7 | 0.723 | 0.732 |
| ALR8 | 0.847 | 0.817 |
| ALR9 | 0.671 | 0.664 |
| ALR10 | 0.668 | 0.805 |
| ALR11 | 0.746 | 0.864 |
| ALR12 | 0.863 | 0.926 |
| χ2 (g.l.) | p | χ2/g.l. | GFI | AGFI | CFI | NFI | TLI | RMSEA (I.C. 90%) |
|---|---|---|---|---|---|---|---|---|
| 154.19 (54) | <0.001 | 2.86 | 0.97 | 0.95 | 0.96 | 0.94 | 0.97 | 0.036 (0.032–0.044) |
| Variable | Skewness | Kurtosis |
|---|---|---|
| ALR1 | −1.999 | 3.548 |
| ALR2 | −0.065 | −1.093 |
| ALR3 | −1.402 | 1.166 |
| ALR4 | −0.742 | −0.09 |
| ALR5 | −1.165 | 0.918 |
| ALR6 | −0.773 | −0.713 |
| ALR7 | −0.515 | −0.833 |
| ALR8 | −0.646 | −0.243 |
| ALR9 | −0.285 | −1.286 |
| ALR10 | −1.464 | 0.9 |
| ALR11 | −1.527 | 2.068 |
| ALR12 | −1.001 | −0.256 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez- de la Cruz, S. Validation and Application of a Spanish Version of the ALR-RSI Scale (Ankle Ligament Reconstruction—Return to Sport after Injury) in an Active Non-Athlete Population. J. Pers. Med. 2023, 13, 606. https://doi.org/10.3390/jpm13040606
Pérez- de la Cruz S. Validation and Application of a Spanish Version of the ALR-RSI Scale (Ankle Ligament Reconstruction—Return to Sport after Injury) in an Active Non-Athlete Population. Journal of Personalized Medicine. 2023; 13(4):606. https://doi.org/10.3390/jpm13040606
Chicago/Turabian StylePérez- de la Cruz, Sagrario. 2023. "Validation and Application of a Spanish Version of the ALR-RSI Scale (Ankle Ligament Reconstruction—Return to Sport after Injury) in an Active Non-Athlete Population" Journal of Personalized Medicine 13, no. 4: 606. https://doi.org/10.3390/jpm13040606