
Impact of Sex and Gender on Clinical Management of Patients with Advanced Chronic Liver Disease and Type 2 Diabetes
 , , and
, , and 
Abstract
:1. Introduction
2. Sex- and Gender-Related Differences in T2D
3. Sex and Gender Differences in Chronic Liver Diseases and T2D
3.1. Alcoholic Liver Disease
3.2. Non-Alcoholic Fatty Liver Disease
3.3. Chronic Viral Infection: Hepatitis B and Hepatitis C
3.4. Autoimmune Hepatitis
3.5. Hepatocellular Carcinoma
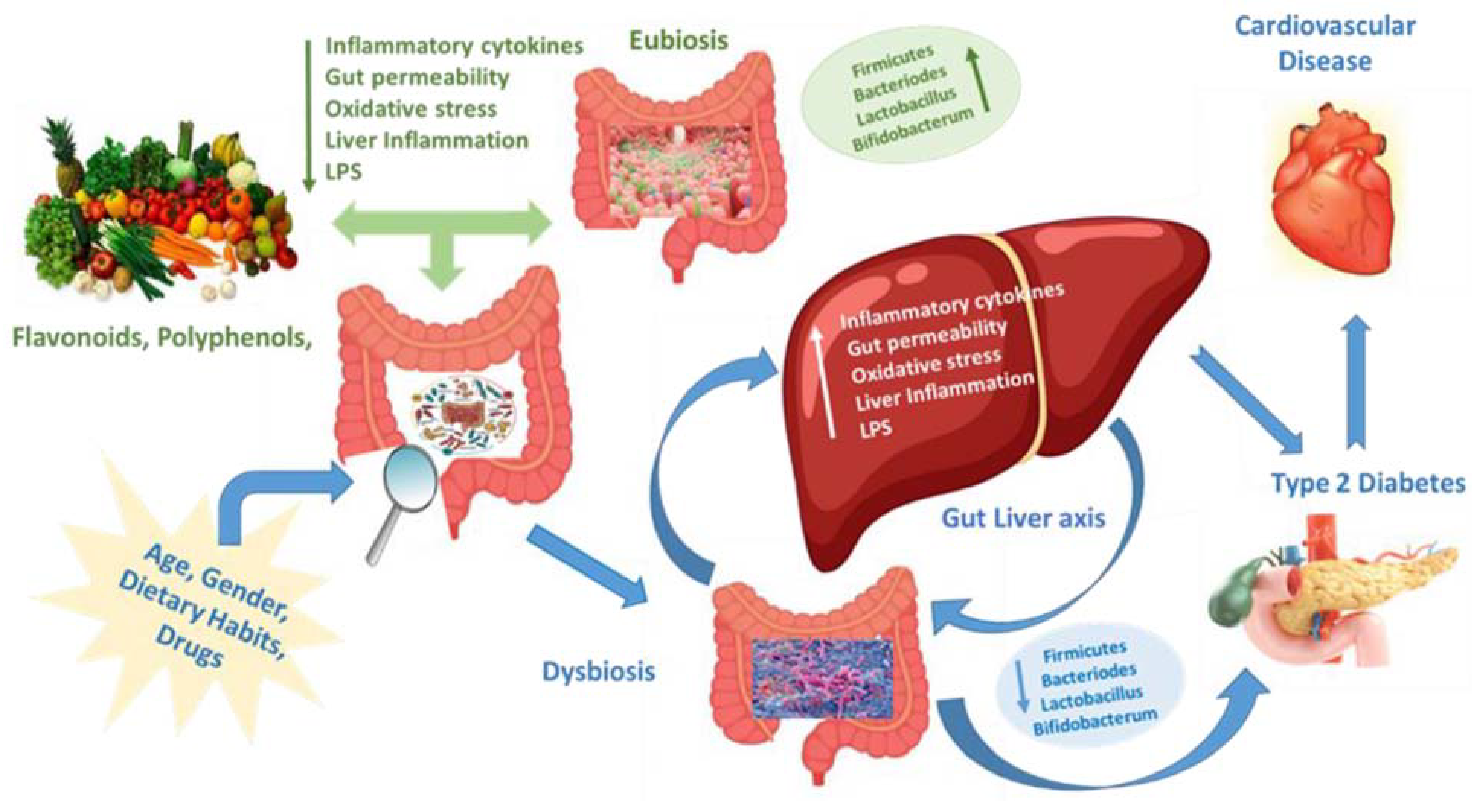
4. Sex- and Gender-Related Differences in the Gut Microbiota of Patients with NAFLD and T2D
5. Sex- and Gender-Related Differences in the Management of Chronic Liver Diseases and T2D
5.1. Non-Pharmacological Therapy
5.2. Statins
5.3. Ezetimibe
5.4. Fibrates
5.5. Pioglitazone
5.6. Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitors
5.7. Metformin
5.8. Dipeptidyl Peptidase-4 (DPP-4) Inhibitors
5.9. Glucagon-like Peptide-1 Receptor Agonists (GLP-1 RAs)
5.10. Sodium–Glucose Cotransporter 2 Inhibitors (SGLT-2i)
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Neill Epperson, C.; Ramaswamy, G.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Raparelli, V.; Santilli, F.; Marra, A.M.; Romiti, G.F.; Succurro, E.; Licata, A.; Buzzetti, E.; Piano, S.; Masala, M.; Suppressa, P.; et al. The SIMI Gender ‘5 Ws’ Rule for the integration of sex and gender-related variables in clinical studies towards internal medicine equitable research. Intern. Emerg. Med. 2022, 17, 1969–1976. [Google Scholar] [CrossRef]
- Russo, G.T.; Manicardi, V.; Rossi, M.C.; Orsi, E.; Solini, A. Sex- and gender-differences in chronic long-term complications of type 1 and type 2 diabetes mellitus in Italy. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2297–2309. [Google Scholar] [CrossRef]
- Magliano, D.J.; Boyko, E.J. IDF Diabetes Atlas 10th edition scientific committee. In IDF DIABETES ATLAS [Internet], 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar] [PubMed]
- Logue, J.; Walker, J.J.; Colhoun, H.M.; Leese, G.P.; Lindsay, R.S.; McKnight, J.A.; Morris, A.D.; Pearson, D.W.; Petrie, J.R.; Philip, S.; et al. Scottish Diabetes Research Network Epidemiology Group. Do men develop type 2 diabetes at lower body mass indices than women? Diabetologia 2011, 54, 3003–3006. [Google Scholar] [CrossRef] [Green Version]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [Green Version]
- Imbalzano, E.; Russo, G.T.; Giandalia, A.; Sciacqua, A.; Orlando, L.; Russo, V.; Perticone, M.; Cicero, A.F.G.; Versace, A.G.; Di Micco, P.; et al. Sex-Specific Impact of Different Obesity/Metabolic Phenotypes on Long-Term Cardiovascular Outcomes in Acute Coronary Syndrome Patients. Biomedicines 2022, 10, 424. [Google Scholar] [CrossRef]
- Russo, G.T.; Giandalia, A.; Romeo, E.L.; Muscianisi, M.; Ruffo, M.C.; Alibrandi, A.; Bitto, A.; Forte, F.; Grillone, A.; Asztalos, B.; et al. HDL subclasses and the common CETP TaqIB variant predict the incidence of microangiopatic complications in type 2 diabetic women: A 9 years follow-up study. Diabetes Res. Clin. Pract. 2017, 132, 108–117. [Google Scholar] [CrossRef]
- Peters, S.A.; Huxley, R.R.; Sattar, N.; Woodward, M. Sex differences in the excess risk of cardiovascular diseases associated with type 2 diabetes: Potential explanations and clinical implications. Curr. Cardiovasc. Risk Rep. 2015, 9, 36. [Google Scholar] [CrossRef] [Green Version]
- Fourny, N.; Beauloye, C.; Bernard, M.; Horman, S.; Desrois, M.; Bertrand, L. Sex Differences of the Diabetic Heart. Front. Physiol. 2021, 12, 661297. [Google Scholar] [CrossRef]
- Rossi, M.C.; Cristofaro, M.R.; Gentile, S.; Lucisano, G.; Manicardi, V.; Mulas, M.F.; Napoli, A.; Nicolucci, A.; Pellegrini, F.; Suraci, C.; et al. Sex disparities in the quality of diabetes care: Biological and cultural factors may play a different role for different outcomes: A cross sectional observational study from AMD annal initiative. Diabetes Care 2013, 10, 3162–3168. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Interheart Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Ballotari, P.; Venturelli, F.; Greci, M.; Giorgi Rossi, P.; Manicardi, V. Sex Differences in the Effect of Type 2 Diabetes on Major Cardiovascular Diseases: Results from a Population-Based Study in Italy. Int. J. Endocrinol. 2017, 2017, 6039356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.A.; Huxley, R.R.; Woodward, M. Diabetes as a risk factor for stroke in women compared with men: A systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet 2014, 383, 1973–1980. [Google Scholar] [CrossRef]
- Chatterjee, S.; Peters, S.A.; Woodward, M.; Mejia Arango, S.; Batty, G.D.; Beckett, N.; Beiser, A.; Borenstein, A.R.; Crane, P.K.; Haan, M.; et al. Type 2 diabetes as a risk factor for dementia in women compared with men: A pooled analysis of 2.3 million people comprising more than 100,000 cases of dementia. Diabetes Care 2016, 39, 300–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roche, M.M.; Wang, P.P. Sex Differences in All-Cause and Cardiovascular Mortality, Hospitalization for Individuals with and Without Diabetes, and Patients with Diabetes Diagnosed Early and Late. Diabetes Care 2013, 36, 2582–2590. [Google Scholar] [CrossRef] [Green Version]
- Bouthoorn, S.; Valstar, G.B.; Gohar, A.; den Ruijter, H.M.; Reitsma, H.B.; Hoes, A.W.; Rutten, F.H. The prevalence of left ventricular diastolic dysfunction and heart failure with preserved ejection fraction in men and women with type 2 diabetes: A systematic review and meta-analysis. Diabetes Vasc. Dis. Res. 2018, 15, 477–493. [Google Scholar] [CrossRef] [Green Version]
- Brand, F.N.; Abbott, R.D.; Kannel, W.B. Diabetes, intermittent claudication, and risk of cardiovascular events. The Framingham Study. Diabetes 1989, 38, 504–509. [Google Scholar] [CrossRef]
- Lombardo, F.L.; Maggini, M.; De Bellis, A.; Seghieri, G.; Anichini, R. Lower extremity amputations in persons with and without diabetes in Italy: 2001–2010. PLoS ONE 2014, 9, e86405. [Google Scholar] [CrossRef] [Green Version]
- Giandalia, A.; Giuffrida, A.E.; Gembillo, G.; Cucinotta, D.; Squadrito, G.; Santoro, D.; Russo, G.T. Gender Differences in Diabetic Kidney Disease: Focus on Hormonal, Genetic and Clinical Factors. Int. J. Mol. Sci. 2021, 22, 5808. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R. Gender difference in cardiovascular outcomes with SGLT-2 inhibitors and GLP-1 receptor agonist in type 2 diabetes: A systematic review and meta-analysis of cardio-vascular outcome trials. Diabetes Metab. Syndr. 2020, 14, 181–187. [Google Scholar] [CrossRef]
- Raparelli, V.; Elharram, M.; Moura, C.S.; Abrahamowicz, M.; Bernatsky, S.; Behlouli, H.; Pilote, L. Sex Differences in Cardiovascular Effectiveness of Newer Glucose-Lowering Drugs Added to Metformin in Type 2 Diabetes Mellitus. J. Am. Heart Assoc. 2020, 9, e012940. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.T.; Giandalia, A.; Romeo, E.L.; Nunziata, M.; Muscianisi, M.; Ruffo, M.C.; Catalano, A.; Cucinotta, D. Fracture Risk in Type 2 Diabetes: Current Perspectives and Gender Differences. Int. J. Endocrinol. 2016, 2016, 1615735, Erratum in: Int. J. Endocrinol. 2017, 2017, 4576102. [Google Scholar] [CrossRef] [Green Version]
- Kirkman, M.S.; Rowan-Martin, M.T.; Levin, R.; Fonseca, V.A.; Schmittdiel, J.A.; Herman, W.H.; Aubert, R.E. Determinants of adherence to diabetes medications: Findings from a large pharmacy claims database. Diabetes Care 2015, 38, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholes, S.; Bann, D. Education-related disparities in reported physical activity during leisure-time, active transportation, and work among US adults: Repeated cross-sectional analysis from the National Health and Nutrition Examination Surveys, 2007 to 2016. BMC Public Health 2018, 18, 926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimpin, L.; Cortez-Pinto, H.; Negro, F.; Corbould, E.; Lazarus, J.V.; Webber, L.; Sheron, N. EASL HEPAHEALTH Steering Committee. Burden of liver disease in Europe: Epidemiology and analysis of risk factors to identify prevention policies. J. Hepatol. 2018, 69, 718–735. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Gower, E.; Estes, C.; Blach, S.; Razavi-Shearer, K.; Razavi, H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J. Hepatol. 2014, 61 (Suppl. 1), S45–S57. [Google Scholar] [CrossRef] [Green Version]
- Frank, V.A.; Herold, M.D.; Antin, T.; Hunt, G. Gendered perspectives on young adults, alcohol consumption and intoxication. Int. J. Drug Policy 2020, 81, 102780. [Google Scholar] [CrossRef]
- Cacciola, I.; Scoglio, R.; Alibrandi, A.; Squadrito, G.; Raimondo, R.; SIMG-Messina Hypertransaminasemia Study Group. Evaluation of liver enzyme levels and identification of asymptomatic liver disease patients in primary care. Intern. Emerg. Med. 2017, 12, 181–186. [Google Scholar] [CrossRef]
- Ilham, M.A.; Cookson, A.; Dheerendra, S.; Rizzello, A.; Cacciola, R.; Chavez, R. Idiopathic severe elevation of serum alkaline phosphatase following adult renal transplantation: Case reports. Transpl. Proc. 2008, 40, 2059–2061. [Google Scholar] [CrossRef]
- Giandalia, A.; Romeo, E.L.; Ruffo, M.C.; Muscianisi, M.; Giorgianni, L.; Forte, F.; Cucinotta, D.; Russo, G.T. Clinical correlates of persistently elevated liver enzymes in type 2 diabetic outpatients. Prim. Care Diabetes 2017, 11, 226–232. [Google Scholar] [CrossRef]
- Sagnelli, E.; Stroffolini, T.; Sagnelli, C.; Pirisi, M.; Babudieri, S.; Colloredo, G.; Russello, M.; Coppola, N.; Gaeta, G.B.; Cacopardo, B.; et al. Gender differences in chronic liver diseases in two cohorts of 2001 and 2014 in Italy. Infection 2018, 46, 93–101. [Google Scholar] [CrossRef]
- Oloruntoba, O.O.; Moylan, C.A. Gender-based disparities in access to and outcomes of liver transplantation. World J. Hepatol. 2015, 7, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, C.; Gutiérrez-Domingo, T.; Luque, B.; García-Vázquez, O.; Cuadrado, E. Protective Behavioral Strategies and Alcohol Consumption: The Moderating Role of Drinking-Group Gender Composition. Int. J. Environ. Res. Public Health 2019, 16, 900. [Google Scholar] [CrossRef] [Green Version]
- Singal, A.K.; Bataller, R.; Ahn, J.; Kamath, P.S.; Shah, V.H. ACG Clinical Guideline: Alcoholic Liver Disease. Am. J. Gastroenterol. 2018, 113, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Stickel, F.; Datz, C.; Hampe, J.; Bataller, R. Pathophysiology and Management of Alcoholic Liver Disease: Update 2016. Gut Liver 2017, 11, 173–188. [Google Scholar] [CrossRef]
- Thomson, A.D.; Bird, G.L.; Saunders, J.B. Alcoholic liver disease. Gut 1991, 32, S97–S103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, B.; Bataller, R. Alcoholic liver disease: Pathogenesis and new therapeutic targets. Gastroenterology 2011, 141, 1572–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgendy, R.; Deschênes, S.S.; Burns, R.J.; Levy, M.; Schmitz, N. Alcohol consumption, depressive symptoms, and the incidence of diabetes-related complications. J. Diabetes 2019, 11, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, C.; Cowell, A.J.; Dowd, W.N. Alcohol Consumption in Response to the COVID-19 Pandemic in the United States. J. Addict. Med. 2021, 15, 341–344. [Google Scholar] [CrossRef]
- Murthy, P.; Narasimha, V.L. Effects of the COVID-19 pandemic and lockdown on alcohol use disorders and complications. Curr. Opin. Psychiatry 2021, 34, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Marques-Vidal, P.; Vollenweider, P.; Waeber, G. Alcohol consumption and incidence of type 2 diabetes. Results from the CoLaus study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 75–84. [Google Scholar] [CrossRef]
- Beulens, J.W.; van der Schouw, Y.T.; Bergmann, M.M.; Rohrmann, S.; Schulze, M.B.; Buijsse, B.; Grobbee, D.E.; Arriola, L.; Cauchi, S.; Tormo, M.-J.; et al. Alcohol consumption and risk of type 2 diabetes in European men and women: Influence of beverage type and body size the EPIC-InterAct study. J. Intern. Med. 2012, 272, 358e70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoglia, M.P.; Gormaz, J.G.; Libuy, M.; Sanhueza, D.; Gajardo, A.; Srur, A.; Wallbaum, M.; Erazo, M. The population impct of obesity, sedentary lifestyle, and tobacco and alcohol consumption on the prevalence of type 2 diabetes: Analysis of a health population survey in Chile, 2010. PLoS ONE 2017, 12, e0178092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Liu, X.; Liao, W.; Kang, N.; Dong, X.; Abdulai, T.; Zhai, Z.; Wang, C.; Wang, X.; Li, Y. Prevalence and characteristics of alcohol consumption and risk of type 2 diabetes mellitus in rural China. BMC Public Health 2021, 21, 1644. [Google Scholar] [CrossRef]
- Wang, S.H.; Chen, P.J.; Yeh, S.H. Gender disparity in chronic hepatitis B: Mechanisms of sex hormones. J. Gastroenterol. Hepatol. 2015, 30, 1237–1245. [Google Scholar] [CrossRef] [Green Version]
- Sayaf, K.; Gabbia, D.; Russo, F.P.; De Martin, S. The Role of Sex in Acute and Chronic Liver Damage. Int. J. Mol. Sci. 2022, 23, 10654. [Google Scholar] [CrossRef]
- Moroni, L.; Bianchi, I.; Lleo, A. Geoepidemiology, gender and autoimmune disease. Autoimmun. Rev. 2012, 11, A386–A392. [Google Scholar] [CrossRef]
- Sahebjam, F.; Vierling, J.M. Autoimmune hepatitis. Front. Med. 2015, 9, 187–219. [Google Scholar] [CrossRef]
- Kerkar, N.; Chan, A. Autoimmune Hepatitis, Sclerosing Cholangitis, and Autoimmune Sclerosing Cholangitis or Overlap Syndrome. Clin. Liver Dis. 2018, 22, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Sucher, E.; Sucher, R.; Gradistanac, T.; Brandacher, G.; Schneeberger, S.; Berg, T. Autoimmune Hepatitis-Immunologically Triggered Liver Pathogenesis-Diagnostic and Therapeutic Strategies. J. Immunol. Res. 2019, 2019, 9437043. [Google Scholar] [CrossRef] [Green Version]
- Burra, P.; Bizzaro, D.; Gonta, A.; Shalaby, S.; Gambato, M.; Morelli, M.C.; Trapani, S.; Floreani, A.; Marra, F.; Brunetto, M.R.; et al. Special Interest Group Gender in Hepatology of the Italian Association for the Study of the Liver (AISF). Clinical impact of sexual dimorphism in non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH). Liver Int. 2021, 41, 1713–1733. [Google Scholar] [CrossRef] [PubMed]
- Morán-Costoya, A.; Proenza, A.M.; Gianotti, M.; Lladó, I.; Valle, A. Sex Differences in Nonalcoholic Fatty Liver Disease: Estrogen Influence on the Liver-Adipose Tissue Crosstalk. Antioxid. Redox Signal. 2021, 35, 753–774. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a sexual dimorphic disease: Role of gender and reproductive status in the development and progression of nonalcoholic fatty liver disease and inherent cardiovascular risk. Adv. Ther. 2017, 34, 1291e326. [Google Scholar] [CrossRef]
- Hashimoto, E.; Tokushige, K. Prevalence, gender, ethnic variations, and prognosis of NAS.H. J. Gastroenterol. 2011, 46 (Suppl. 1), 63–69. [Google Scholar] [CrossRef]
- Myers, S.; Neyroud-Caspar, I.; Spahr, L.; Gkouvatsos, K.; Fournier, E.; Giostra, E.; Magini, G.; Frossard, J.L.; Bascaron, M.E.; Vernaz, N.; et al. NAFLD and MAFLD as emerging causes of HCC: A populational study. JHEP Rep. 2021, 3, 100231. [Google Scholar] [CrossRef] [PubMed]
- Marengo, A.; Rosso, C.; Bugianesi, E. Liver Cancer: Connections with Obesity, Fatty Liver, and Cirrhosis. Annu. Rev. Med. 2016, 67, 103–117. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D. Nonalcoholic fatty liver disease: A novel cardiometabolic risk factor for type 2 diabetes and its complications. J. Clin. Endocrinol. Metab. 2013, 98, 483e95. [Google Scholar] [CrossRef] [Green Version]
- Wu, E.M.; Wong, L.L.; Hernandez, B.Y.; Ji, J.F.; Jia, W.; Kwee, S.A.; Kalathil, S. Gender differences in hepatocellular cancer: Disparities in nonalcoholic fatty liver disease/steatohepatitis and liver transplantation. Hepatoma Res. 2018, 4, 66. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis. Gut 2022, 71, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.A.; Lee, J.H.; Lim, S.Y.; Ha, H.S.; Kwon, H.S.; Park, Y.M.; Lee, W.C.; Kang, M.I.; Yim, H.W.; Yoon, K.H.; et al. Metabolic syndrome as a predictor of type 2 diabetes, and its clinical interpretations and usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef]
- Rashti, R.; Sharafi, H.; Alavian, S.M.; Moradi, Y.; Mohamadi Bolbanabad, A.; Moradi, G. Systematic Review and Meta-Analysis of Global Prevalence of HBsAg and HIV and HCV Antibodies among People Who Inject Drugs and Female Sex Workers. Pathogens 2020, 9, 432. [Google Scholar] [CrossRef]
- Cacciola, I.; Russo, G.; Filomia, R.; Pitrone, C.; Caccamo, G.; Giandalia, A.; Alibrandi, A.; Franzè, M.S.; Porcari, S.; Maimone, S.; et al. Over time evaluation of glycemic control in direct-acting antiviral-treated hepatitis C virus/diabetic individuals with chronic hepatitis or with cirrhosis. Liver Int. 2021, 41, 2059–2067. [Google Scholar] [CrossRef]
- Li, J.; Gordon, S.C.; Zhou, Y.; Boscarino, J.A.; Schmidt, M.A.; Daida, Y.G.; Rupp, L.B.; Trudeau, S.; Lu, M.; CHeCS Investigators. Sex Differences in Extrahepatic Outcomes After Antiviral Treatment for Hepatitis, C. Am. J. Gastroenterol. 2021, 116, 576–583. [Google Scholar] [CrossRef]
- Yin, X.; Kong, L.; Du, P.; Jung, J. Effects of direct-acting antiviral treatment on reducing mortality among Medicare beneficiaries with HIV and HCV coinfection. AIDS Care 2022, 34, 1330–1337. [Google Scholar] [CrossRef]
- Park, H.; Lo-Ciganic, W.H.; Huang, J.; Wu, Y.; Henry, L.; Peter, J.; Sulkowski, M.; Nelson, D.R. Machine learning algorithms for predicting direct-acting antiviral treatment failure in chronic hepatitis C: An HCV-TARGET analysis. Hepatology 2022, 76, 483–491. [Google Scholar] [CrossRef]
- Ascione, A.; ·De Luca, M.; Melazzini, M. Safety and efficacy of ombitasvir/paritaprevir/ritonavir/dasabuvir plus ribavirin in patients over 65 years with HCV genotype 1 cirrhosis. Infection 2018, 46, 607–615. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Li, L.; Zhao, J.; Ungvari, G.S.; Ng, C.H.; Duan, Z.; Zheng, S.J.; Xiang, Y.T. Gender differences in demographic and clinical characteristics in patients with HBV-related liver diseases in China. Peer J. 2022, 10, e13828. [Google Scholar] [CrossRef]
- Ruggieri, A.; Gagliardi, M.C.; Anticoli, S. Sex-Dependent Outcome of Hepatitis B and C Viruses Infections: Synergy of Sex Hormones and Immune Responses? Front. Immunol. 2018, 9, 2302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baden, R.; Rockstroh, J.K.; Buti, M. Natural history and management of hepatitis C: Does sex play a role? J. Infect. Dis. 2014, 209 (Suppl. 3), S81–S85. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Chen, S.C.; Lo, T.C.; Kuo, H.W. Dual Infection with Hepatitis B Virus and Hepatitis C Virus Correlated with Type 2 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2020, 128, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Cheng, P.N.; Kao, J.H. Systematic review: Chronic viral hepatitis and metabolic derangement. Aliment. Pharmacol. Ther. 2020, 51, 216–230. [Google Scholar] [CrossRef]
- Shiffman, M.L.; Gunn, N.T. Impact of hepatitis C virus therapy on metabolism and public health. Liver Int. 2017, 37 (Suppl. 1), 13–18. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferrari, S.M.; Giuggioli, D.; Di Domenicantonio, A.; Ruffilli, I.; Corrado, A.; Fabiani, S.; Marchi, S.; Ferri, C.; Ferrannini, E.; et al. Hepatitis C virus infection and type 1 and type 2 diabetes mellitus. World J. Diabetes 2014, 5, 586–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukla, M.; Piotrowski, D.; Waluga, M.; Hartleb, M. Insulin resistance and its consequences in chronic hepatitis C. Clin. Exp. Hepatol. 2015, 1, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Shen, Y.; Cai, H.; Liu, Y.M.; Qin, G. Hepatitis B virus infection status and risk of type 2 diabetes mellitus: A meta-analysis. Hepatol. Res. 2015, 45, 1100–1109. [Google Scholar] [CrossRef]
- de Sousa, G.; Prinz, N.; Becker, M.; Dürr, R.; Faller, U.; Meraner, D.; Heise, N.; Engelmann, I.; Bruckmayer, H.; Wiemann, D.; et al. Diabetes Mellitus and Autoimmune Hepatitis: Demographical and Clinical Description of a Relatively Rare Phenotype. Horm. Metab. Res. 2018, 50, 568–574. [Google Scholar] [CrossRef]
- Biswas, S.; Ghose, S. Divergent impact of gender in advancement of liver injuries, diseases, and carcinogenesis. Front. Biosci. 2018, 10, 65–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, B.; Zhu, Y.J.; Wang, H.Y.; Chen, L. Gender disparity in hepatocellular carcinoma (HCC): Multiple underlying mechanisms. Sci. China Life Sci. 2017, 60, 575–584. [Google Scholar] [CrossRef]
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Siddiqui, M.K.; Ambery, P.; Armisen, J.; Challis, B.G.; Haefliger, C.; Pearson, E.R.; Doney, A.S.F.; Dillon, J.F.; Palmer, C.N.A. Metabolic dysfunction-related liver disease as a risk factor for cancer. BMJ Open Gastroenterol. 2022, 9, e000817. [Google Scholar] [CrossRef]
- Teng, Y.X.; Xie, S.; Guo, P.P.; Deng, Z.J.; Zhang, Z.Y.; Gao, W.; Zhang, W.G.; Zhong, J.H. Hepatocellular Carcinoma in Non-alcoholic Fatty Liver Disease: Current Progresses and Challenges. J. Clin. Transl. Hepatol. 2022, 10, 955–964. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127 (Suppl. 1), S35–S50. [Google Scholar] [CrossRef] [PubMed]
- Bashir Hamidu, R.; Chalikonda, D.M.; Hann, H.W. Gender Disparity in Host Responses to Hepatitis B-Related Hepatocellular Carcinoma: A Case Series. Vaccines 2021, 9, 838. [Google Scholar] [CrossRef]
- Yu, L.; Liu, X.; Wang, X.; Dang, Z.; Jiang, Y.; Wang, X.; Yang, Z. Impact of gender as a prognostic factor in HBV-related Hepatocellular Carcinoma: The survival strength of female patients in BCLC stage 0-B. J. Cancer 2019, 10, 4237–4244. [Google Scholar] [CrossRef]
- Szabo, G.; Petrasek, J. Inflammasome activation and function in liver disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Miele, L.; Valenza, V.; La Torre, G.; Montalto, M.; Cammarota, G.; Ricci, R.; Mascianà, R.; Forgione, A.; Gabrieli M., L.; Perotti, G.; et al. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Hepatology 2009, 49, 1877. [Google Scholar] [CrossRef]
- Dominianni, C.; Sinha, R.; Goedert, J.J.; Pei, Z.; Yang, L.; Hayes, R.B.; Ahn, J. Sex, body mass index, and dietary fiber intake influence the human gut microbiome. PLoS ONE 2015, 10, e0124599. [Google Scholar] [CrossRef] [Green Version]
- Haro, C.; Rangel-Zúñiga, O.A.; Alcalá-Díaz, J.F.; Gómez-Delgado, F.; Pérez-Martínez, P.; Delgado-Lista, J.; Quintana-Navarro, G.M.; Landa, B.B.; Navas-Cortés, J.A.; Tena-Sempere, M.; et al. Intestinal microbiota is influenced by gender and body mass index. PLoS ONE 2016, 11, e0154090. [Google Scholar] [CrossRef] [Green Version]
- Diamant, M.; Blaak, E.E.; de Vos, W.M. Do nutrient-gut-microbiota interactions play a role in human obesity, insulin resistance and type 2 diabetes? Obes. Rev. 2011, 12, 272–281. [Google Scholar] [CrossRef]
- Troseid, M.; Andersen, G.O.; Broch, K.; Hov, J.R. The gut microbiome in coronary artery disease and heart failure: Current knowledge and future directions. EBioMedicine 2020, 52, 102649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, N.; Vogensen, F.K.; van den Berg, F.W.; Nielsen, D.S.; Andreasen, A.S.; Pedersen, B.K.; Al-Soud, W.A.; Sorensen, S.J.; Hansen, L.H.; Jakobsen, M. Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS ONE 2010, 5, e9085. [Google Scholar] [CrossRef] [PubMed]
- Mamic, P.; Chaikijurajai, T.; Tang, W.H.W. Gut microbiome—A potential mediator of pathogenesis in heart failure and its comorbidities: State-of-the-art review. J. Mol. Cell Cardiol. 2021, 152, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [Green Version]
- Tsai, H.J.; Tsai, W.C.; Hung, W.C.; Hung, W.W.; Chang, C.C.; Dai, C.Y.; Tsai, Y.C. Gut Microbiota and Subclinical Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus. Nutrients 2021, 13, 2679. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.R.; Jaiswal, S.; Ravindra, P. Modulation of gut microbiota by bioactive compounds for prevention and management of type 2 diabetes. Biomed. Pharmacother. 2022, 152, 113148. [Google Scholar] [CrossRef]
- Arpón, A.; Riezu-Boj, J.I.; Milagro, F.I.; Marti, A.; Razquin, C.; Martínez-González, M.A.; Corella, D.; Estruch, R.; Casas, R.; Fitó, M.; et al. Adherence to Mediterranean diet is associated with methylation changes in inflammation-related genes in peripheral blood cells. J. Physiol. Biochem. 2016, 73, 445–455. [Google Scholar] [CrossRef] [Green Version]
- Fischer, L.M.; da Costa, K.A.; Kwock, L.; Galanko, J.; Zeisel, S.H. Dietary choline requirements of women: Effects of estrogen and genetic variation. Am. J. Clin. Nutr. 2010, 92, 1113–1119. [Google Scholar] [CrossRef] [Green Version]
- Voisin, S.; Eynon, N.; Yan, X.; Bishop, D.J. Exercise training and DNA methylation in humans. Acta Physiol. 2015, 213, 39–59. [Google Scholar] [CrossRef]
- Zhang, F.F.; Cardarelli, R.; Carroll, J.; Fulda, K.G.; Kaur, M.; Gonzalez, K.; Vishwanatha, J.K.; Santella, R.M.; Morabia, A. Significant differences in global genomic DNA methylation by gender and race/ethnicity in peripheralblood. Epigenetics 2011, 6, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Berzigotti, A.A.A.; Villanueva, C.; Genescà, J.; Ardevol, A.; Augustin, S.; Calleja, J.L.; Bañares, R.; Garcia-Pagan, J.C.; Mesonero, F.; Bosch, J. Lifestyle intervention by a 16-week programme of supervised diet and physical exercise ameliorates portal hypertension in patients with cirrhosis and obesity: The SportdietStudy. Hepatology 2014, 60 (Suppl. 1), 32A–91A. [Google Scholar]
- Molloy, J.W.; Calcagno, C.J.; Williams, C.D.; Jones, F.J.; Torres, D.M.; Harrison, S.A. Association of coffee and caffeine consumption with fatty liver disease, nonalcoholic steatohepatitis, and degree of hepatic fibrosis. Hepatology 2012, 55, 429–436. [Google Scholar] [CrossRef]
- Kantartzis, K.; Thamer, C.; Peter, A.; Machann, J.; Schick, F.; Schraml, C.; Königsrainer, A.; Königsrainer, I.; Kröber, S.; Niess, A.; et al. High cardiorespiratory fitness is an independent predictor of the reduction in liver fat during a lifestyle intervention in non-alcoholic fatty liver disease. Gut 2009, 58, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, D.E.; Serper, M.A.; Mehta, R.; Fox, R.; Binu, J.; Aytaman, A.; Baytarian, M.; Hunt, K.; Albrecht, J.; Njei, B.; et al. Effects of hypercholesterolemia and statin exposure on survival in a large national cohort of patients with cirrhosis. Gastroenterology 2019, 156, 1693–1706.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Singh, P.P.; Singh, A.G.; Murad, M.H.; Sanchez, W. Statins are associated with a reduced risk of hepatocellular cancer: A systematic review and meta-analysis. Gastroenterology 2013, 144, 323–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakade, Y.; Murotani, K.; Inoue, T.; Kobayashi, Y.; Yamamoto, T.; Ishii, N.; Ohashi, T.; Ito, K.; Fukuzawa, Y.; Yoneda, M. Ezetimibe for the treatment of non-alcoholic fatty liver disease: A meta-analysis. Hepatol. Res. 2017, 47, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Rhee, H.; Kim, Y.E.; Lee, M.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Choi, J.Y.; Lee, Y.H. Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: An open-label randomized controlled trial (ESSENTIAL study). BMC Med. 2022, 20, 93. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, R.; Iwasa, M.; Eguchi, A.; Tamai, Y.; Shigefuku, R.; Fujiwara, N.; Tanaka, H.; Kobayashi, Y.; Ikoma, J.; Kaito, M.; et al. Effect of pemafibrate on liver enzymes and shear wave velocity in non-alcoholic fatty liver disease patients. Front. Med. 2023, 10, 1073025. [Google Scholar] [CrossRef]
- Yoon, M.; Jeong, S.; Nicol, C.J.; Lee, H.; Han, M.; Kim, J.-J.; Seo, Y.-J.; Ryu, C.; Oh, G.T. Fenofibrate regulates obesity and lipid metabolism with sexual dimorphism. Exp. Mol. Med. 2002, 34, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 10, 1097. [Google Scholar] [CrossRef]
- Yan, H.; Wu, W.; Chang, X.; Xia, M.; Ma, S.; Wang, L.; Gao, J. Gender differences in the efficacy of pioglitazone treatment in nonalcoholic fatty liver disease patients with abnormal glucose metabolism. Biol. Sex Differ. 2021, 12, 1. [Google Scholar] [CrossRef]
- Momtazi-Borojeni, A.A.; Banach, M.; Ruscica, M.; Sahebkar, A. The role of PCSK9 in NAFLD/NASH and therapeutic implications of PCSK9 inhibition. Expert Rev. Clin. Pharmacol. 2022, 15, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Feder, S.; Wiest, R.; Weiss, T.S.; Aslanidis, C.; Schacherer, D.; Krautbauer, S.; Liebisch, G.; Buechler, C. Proprotein convertase subtilisin/kexin type 9 (PCSK9) levels are not associated with severity of liver disease and are inversely related to cholesterol in a cohort of thirty eight patients with liver cirrhosis. Lipids Health Dis. 2021, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Jia, F.; Fei, S.F.; Tong, D.B.; Xue, C.; Li, J.J. Sex difference in circulating PCSK9 and its clinical implications. Front. Pharmacol. 2022, 13, 953845. [Google Scholar] [CrossRef]
- Zou, J.; Hong, L.; Luo, C.; Li, Z.; Zhu, Y.; Huang, T.; Zhang, Y.; Yuan, H.; Hu, Y.; Wen, T.; et al. Metformin inhibits estrogen-dependent endometrial cancer cell growth by activating the AMPK-FOXO1 signal pathway. Cancer Sci. 2016, 107, 1806–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, F.S.; Huang, Y.H.; Hou, M.C.; Hwu, C.M.; Lo, Y.R.; Shin, S.J.; Hsu, C.C. Metformin use and cirrhotic decompensation in patients with type 2 diabetes and liver cirrhosis. Br. J. Clin. Pharmacol. 2022, 88, 311–322. [Google Scholar] [CrossRef]
- Schütt, M.; Zimmermann, A.; Hood, R.; Hummel, M.; Seufert, J.; Siegel, E.; Tytko, A.; Holl, R.W.; DPV initiative; German BMBF Competence Network Diabetes Mellitus. Gender-specific Effects of Treatment with Lifestyle, Metformin or Sulfonylurea on Glycemic Control and Body Weight: A German Multicenter Analysis on 9 108 Patients. Exp. Clin. Endocrinol. Diabetes 2015, 123, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Zhang, H.; Wei, W.; Fang, T. Gender-related different effects of a combined therapy of Exenatide and Metformin on overweight or obesity patients with type 2 diabetes mellitus. J. Diabetes Complicat. 2016, 30, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Kosi-Trebotic, L.; Thomas, A.; Harreiter, J.; Chmelik, M.; Trattnig, S.; Kautzky-Willer, A. Gliptin therapy reduces hepatic and myocardial fat in type 2 diabetic patients. Eur. J. Clin. Investig. 2017, 47, 829–838. [Google Scholar] [CrossRef]
- Macauley, M.; Hollingsworth, K.G.; Smith, F.E.; Thelwall, P.E.; Al-Mrabeh, A.; Schweizer, A.; Foley, J.E.; Taylor, R. Effect of vildagliptin on hepatic steatosis. J. Clin. Endocrinol. Metab. 2015, 100, 1578–1585. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; LEAN trial team; Abouda., G.; et al. Liraglutide safety and efficacy in patients with nonalcoholic steatohepatitis (LEAN): A multicenter, double-blind randomized, placebo-controlled phase 2 study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef] [Green Version]
- Kalra, S.; Das, A.K.; Sahay, R.K.; Baruah M., P.; Tiwaskar, M.; Das, S.; Chatterjee, S.; Saboo, B.; Bantwal, G.; Bhattacharya, S.; et al. Consensus recommendations on GLP-1 RA use in the management of type 2 diabetes mellitus: South asian task force. Diabetes Ther. 2019, 10, 1645–1717. [Google Scholar] [CrossRef] [Green Version]
- Anichini, R.; Cosimi, S.; Di Carlo, A.; Orsini, P.; De Bellis, A.; Seghieri, G.; Franconi, F.; Baccetti, F. Gerder difference in response predictors after 1-year exenatide therapy twice daily in type 2 diabetic patients: A real world experience. Diabetes Metab. Syndr. Obes. 2013, 6, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Saffo, S.; Taddei, T. SGLT2 inhibitors and cirrhosis: A unique perspective on the comanagement of diabetes mellitus and ascites. Clin. Liver Dis. 2018, 11, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Staplin, N.; Roddick, A.J.; Emberson, J.; Reith, C.; Riding, A.; Wonnacott, A.; Kuverji, A.; Bhandari, S.; Baigent, C.; Haynes, R.; et al. Net effects of sodium-glucose co-transporter-2 inhibition in different patient groups: A meta-analysis of large placebo-controlled randomized trials. EClinicalMedicine 2021, 41, 101163. [Google Scholar] [CrossRef]
- Teratani, T.; Tomita, K.; Suzuki, T.; Oshikawa, T.; Yokoyama, H.; Shimamura, K.; Tominaga, S.; Hiroi, S.; Irie, R.; Okada, Y.; et al. A high-cholesterol diet exacerbates liver fibrosis in mice via accumulation of free cholesterol in hepatic stellate cells. Gastroenterology 2012, 142, 152–164. [Google Scholar] [CrossRef]
- Trebicka, J.; Hennenberg, M.; Laleman, W.; Shelest, N.; Biecker, E.; Schepke, M.; Nevens, F.; Sauerbruch, T.; Heller, J. Atorvastatin lowers portal pressure in cirrhotic rats by inhibition of RhoA/Rho-kinase and activation of endothelial nitric oxide synthase. Hepatology 2007, 46, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Grace, N.D.; Qamar, A.A. Statin use in patients with cirrhosis: A retrospective cohort study. Dig. Dis. Sci. 2014, 59, 1958–1965. [Google Scholar] [CrossRef]
- Motzkus-Feagans, C.; Pakyz, A.L.; Ratliff, S.M.; Bajaj, J.S.; Lapane, K.L. Statin use and infections in Veterans with cirrhosis. Aliment. Pharmacol. Ther. 2013, 38, 611–618. [Google Scholar] [CrossRef]
- Bittner, V.; Deng, L.; Rosenson, R.S.; Taylor, B.; Glasser, S.P.; Kent, S.T.; Farkouh, M.E.; Muntner, P. Trends in the Use of Nonstatin Lipid-Lowering Therapy Among Patients With Coronary Heart Disease: A Retrospective Cohort Study in the Medicare Population 2007 to 2011. J. Am. Coll. Cardiol. 2015, 66, 1864–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 132. Karalis, D.G.; Wild, R.A.; Maki, K.C.; Gaskins, R.; Jacobson, T.A.; Sponseller, C.A.; Cohen, J.D. Gender differences in side effects and attitudes regarding statin use in the Understanding Statin Use in America and Gaps in Patient Education (USAGE) study. J. Clin. Lipidol. 2016, 10, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.; Pintaudi, B.; Giorda, C.; Lucisano, G.; Nicolucci, A.; Cristofaro, M.R.; Suraci, C.; Mulas, M.F.; Napoli, A.; Rossi, M.C.; et al. Age- and Gender-Related Differences in LDL-Cholesterol Management in Outpatients with Type 2 Diabetes Mellitus. Int. J. Endocrinol. 2015, 2015, 957105. [Google Scholar] [CrossRef]
- Shigematsu, E.; Yamakawa, T.; Taguri, M.; Morita, S.; Tokui, M.; Miyamoto, K.; Funae, O.; Takatuka, Y.; Kadonosono, K.; Shigematsu, H.; et al. Efficacy of ezetimibe is associated with gender and baseline lipid levels in patients with type 2 diabetes. J. Atheroscler. Thromb. 2012, 19, 846–853. [Google Scholar] [CrossRef] [Green Version]
- Oliver, W.; Giugliano, R.P. Benefit of Combination Ezetimibe/Simvastatin Among High-Risk Populations: Lessons from the IMPROVE-IT Trial. Curr. Atheroscler. Rep. 2023, 25, 85–93. [Google Scholar] [CrossRef]
- Nakajima, A.; Eguchi, Y.; Yoneda, M.; Imajo, K.; Tamaki, N.; Suganami, H.; Nojima, T.; Tanigawa, R.; Iizuka, M.; Iida, Y.; et al. Randomised clinical trial: Pemafibrate, a novel selective peroxisome proliferator-activated receptor a modulator (SPPARMa), versus placebo in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2021, 54, 1263–1277. [Google Scholar] [CrossRef]
- Yamashita, S.; Masuda, D.; Matsuzawa, Y. Pemafibrate, a New Selective PPARa Modulator: Drug Concept and Its Clinical Applications for Dyslipidemia and Metabolic Diseases. Curr. Atheroscler. Rep. 2020, 22, 5. [Google Scholar] [CrossRef] [Green Version]
- Shinozaki, S.; Tahara, T.; Miura, K.; Lefor, A.K.; Yamamoto, H. Pemafibrate therapy for non-alcoholic fatty liver disease is more effective in lean patients than obese patients. Clin. Exp. Hepatol. 2022, 8, 278–283. [Google Scholar] [CrossRef]
- Kusunoki, M.; Sakazaki, T.; Tsutsumi, K.; Miyata, T.; Oshida, Y. The Effects of Pemafibrate in Japanese Patients with Type 2 Diabetes Receiving HMG-CoA Reductase Inhibitors. Endocr. Metab. Immune Disord Drug Targets 2021, 21, 919–924. [Google Scholar] [CrossRef]
- Das Pradhan, A.; Glynn, R.I.; Fruchart, J.C.; MacFadyen, J.G.; Zaharris, E.S.; Everett, B.M.; Campbell S., E.; Oshima, R.; Amarenco, P.; Blom, D.J.; et al. Triglyceride Lowering with Pemafibrate to Reduce Cardiovascular Risk. N. Engl. J. Med. 2022, 387, 1923–1934. [Google Scholar] [CrossRef]
- Ismini, T.; Aris, P.; Michael, A.; Kostapano, S. Is there a role of lipid-lowering therapies in the management of fatty liver disease? World J. Hepatol. 2022, 14, 119. [Google Scholar]
- Cusi, K.; Orsak, B.; Bril, F.; Lomonaco, R.; Hecht, J.; Ortiz-Lopez, C.; Tio, F.; Hardies, J.; Darland, C.; Musi, N.; et al. Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus: A randomized trial. Ann. Intern. Med. 2016, 165, 305–315. [Google Scholar] [CrossRef]
- Lv, Z.; Guo, Y. Metformin and Its Benefits for Various Diseases. Front. Endocrinol. 2020, 11, 191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Harmsen, W.S.; Mettler, T.A.; Kim, W.R.; Roberts, R.O.; Therneau, T.M.; Roberts, L.R.; Chaiteerakij, R. Continuation of metformin use after a diagnosis of cirrhosis significantly improves survival of patients with diabetes. Hepatology 2014, 60, 2008–2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkontchou, G.; Cosson, E.; Aout, M.; Mahmoudi, A.; Bourcier, V.; Charif, I.; Ganne-Carrie, N.; Grando-Lemaire, V.; Vicaut, E.; Trinchet, J.C.; et al. Impact of metformin on the prognosis of cirrhosis induced by viral hepatitis C in diabetic patients. J. Clin. Endocrinol. Metab. 2011, 96, 2601–2608. [Google Scholar] [CrossRef] [Green Version]
- Anisimov, V.N.; Piskunova, T.S.; Popovich, I.G.; Zabezhinski, M.A.; Tyndyk, M.L.; Egormin, P.A.; Yurova, M.V.; Rosenfeld, S.V.; Semenchenko, A.V.; Kovalenko, I.G.; et al. Gender differences in metformin effect on aging, life span and spontaneous tumorigenesis in 129/Sv mice. Aging 2010, 2, 945–958. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Compean, D.; Jaquez-Quintana, J.O.; Gonzalez-Gonzalez, J.A.; Maldonado-Garza, H. Liver cirrhosis and diabetes: Risk factors, pathophysiology, clinical implications and management. World J. Gastroenterol. 2009, 15, 280–288. [Google Scholar] [CrossRef]
- Cheang, K.I.; Huszar, J.M.; Best, A.M.; Sharma, S.; Essah, P.A.; Nestler, J.E. Long-term effect of metformin on metabolic parameters in the polycystic ovary syndrome. Diabetes Vasc. Dis. Res. 2009, 6, 110–119. [Google Scholar] [CrossRef] [Green Version]
- De Vries, S.T.; Denig, P.; Ekhart, C.; Mol, P.G.M.; van Puijenbroek, E.P. Sex Differences in Adverse Drug Reactions of Metformin: A Longitudinal Survey Study. Drug Saf. 2020, 43, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Misbin, R.I.; Green, L.; Stadel, B.V.; Gueriguian, J.L.; Gubbi, A.; Fleming, G.A. Lactic acidosis in patients with diabetes treated with metformin. N. Engl. J. Med. 1998, 338, 265–266. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Paolini, E.; Corsini, A.; Sirtori, C.R.; Ruscica, M. Nonalcoholic fatty liver disease or metabolic dysfunction-associated fatty liver disease diagnoses and cardiovascular diseases: From epidemiology to drug approaches. Eur. J. Clin. Investig. 2021, 51, e13519. [Google Scholar] [CrossRef]
- Delzenne, N.M.; Cani, P.D.; Everard, A.; Neyrinck, A.M.; Bindels, L.B. Gut microorganisms as promising targets for the management of type 2 diabetes. Diabetologia 2015, 58, 2206–2217. [Google Scholar] [CrossRef]
- de la Cuesta-Zuluaga, J.; Mueller, N.T.; Corrales-Agudelo, V.; Velásquez-Mejía, E.P.; Carmona, J.A.; Abad, J.M.; Escobar, J.S. Metformin Is Associated With Higher Relative Abundance of Mucin-Degrading Akkermansia muciniphila and Several Short-Chain Fatty Acid-Producing Microbiota in the Gut. Diabetes Care 2017, 40, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drucker, D.J.; Nauck, M.A. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006, 368, 1696–1705. [Google Scholar] [CrossRef] [PubMed]
- Itou, M.; Kawaguchi, T.; Taniguchi, E.; Sata, M. Dipeptidyl peptidase-4, a key player in chronic liver disease. World J. Gastroenterol. 2013, 19, 2298–2306. [Google Scholar] [CrossRef] [PubMed]
- Bouchi, R.; Fukuda, T.; Takeuchi, T.; Nakano, Y.; Murakami, M.; Minami, I.; Izumiyama, H.; Hashimoto, K.; Yoshimoto, T.; Ogawa, Y. Dipeptidyl peptidase 4 inhibitors attenuates the decline of skeletal muscle mass in patients with type 2 diabetes. Diabetes Metab. Res. Rev. 2018, 34, e2957. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, T.; Sato, K.; Yamazaki, Y.; Hashizume, H.; Horiguchi, N.; Kakizaki, S.; Mori, M.; Kusano, M.; Yamada, M. MK-0626, a selective DPP-4 inhibitor, attenuates hepatic steatosis in ob/ob mice. World J. Gastroenterol. 2014, 20, 16227–16235. [Google Scholar] [CrossRef]
- Miyazaki, M.; Kato, M.; Tanaka, K.; Tanaka, M.; Kohjima, M.; Nakamura, K.; Enjoji, M.; Nakamuta, M.; Kotoh, K.; Takayanagi, R. Increased hepatic expression of dipeptidyl peptidase-4 in non-alcoholic fatty liver disease and its association with insulin resistance and glucose metabolism. Mol. Med. Rep. 2012, 5, 729–733. [Google Scholar] [CrossRef]
- Farilla, L.; Bulotta, A.; Hirshberg, B.; Li Calzi, S.; Khoury, N.; Noushmehr, H.; Bertolotto, C.; Di Mario, U.; Harlan, D.M.; Perfetti, R. Glucagon-like peptide 1 inhibits cell apoptosis and improves glucose responsiveness of freshly isolated human islets. Endocrinology 2003, 144, 5149–5158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.Z.; Hansotia, T.; Yusta, B.; Ris, F.; Halban, P.A.; Drucker, D.J. Glucagon-like peptide-1 receptor signaling modulates beta cell apoptosis. J. Biol. Chem. 2003, 278, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Nauck, M.A.; Kleine, N.; Orskov, C.; Holst, J.J.; Willms, B.; Creutzfeldt, W. Normalization of fasting hyperglycaemia by exogenous glucagon-like peptide 1 (7–36 amide) in type 2 (non-insulin-dependent) diabetic patients. Diabetologia 1993, 36, 741–744. [Google Scholar] [CrossRef] [Green Version]
- Shyangdan, D.S.; Royle, P.L.; Clar, C.; Sharma, P.; Waugh, N.R. Glucagon-like peptide analogues for type 2 diabetes mellitus: Systematic review and meta-analysis. BMC Endocr. Disord. 2010, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.; He, H.; Li, S.; Yang, L. Comparison of the Efficacy of Glucagon-Like Peptide-1 Receptor Agonists in Patients with Metabolic Associated Fatty Liver Disease: Updated Systematic Review and Meta-Analysis. Endocrinology 2021, 11, 622589. [Google Scholar] [CrossRef]
- Flint, A.; Nazzal, K.; Jagielski, P.; Hindsberger, C.; Zdravkovic, M. Influence of hepatic impairment on pharmacokinetics of the human GLP-1 analogue, liraglutide. Br. J. Clin. Pharmacol. 2010, 70, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Giorda, C.B.; Nada, E.; Tartaglino, B. Pharmacokinetics, safety, and efficacy of DPP-4 inhibitors and GLP-1 receptor agonists in patients with type 2 diabetes mellitus and renal or hepatic impairment. A systematic review of the literature. Endocrine 2014, 46, 406–419. [Google Scholar] [CrossRef]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.S.; Harrison, S.A.; NN9931-4296 Investigators. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Leiter, L.A.; Bain, S.C.; Hramiak, I.; Jódar, E.; Madsbad, S.; Gondolf, T.; Hansen, T.; Holst, I.; Lingvay, I. Cardiovascular risk reduction with once-weekly semaglutide in subjects with type 2 diabetes: A post hoc analysis of gender, age, and baseline CV risk profile in the SUSTAIN 6 trial. Cardiovasc Diabetol. 2019, 18, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallwitz, B.; Dagogo-Jack, S.; Thieu, V.; Garcia-Perez, L.E.; Pavo, I.; Yu, M.; Robertson, K.E.; Zhang, N.; Giorgino, F. Effect of once-weekly dulaglutide on glycated haemoglobin (HbA1c) and fasting blood glucose in patient subpopulations by gender, duration of diabetes and baseline HbA1c. Diabetes Obes. Metab. 2018, 20, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Onishi, Y.; Oura, T.; Matsui, A.; Matsuura, J.; Iwamoto, N. Analysis of efficacy and safety of dulaglutide 0.75 mg stratified by sex in patients with type 2 diabetes in 2 randomized, controlled phase 3 studies in Japan. Endocr. J. 2017, 64, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Joung, K.-I.; Jung, G.-W.; Park, H.-H.; Lee, H.; Park, S.-H.; Shin, J.-Y. Gender differences in adverse event reports associated with antidiabetic drugs. Sci. Rep. 2020, 10, 17545. [Google Scholar] [CrossRef]
- Rentzeperi, E.; Pegiou, S.; Koufakis, T.; Grammatiki, M.; Kotsa, K. Sex Differences in Response to Treatment with Glucagon-like Peptide 1 Receptor Agonists: Opportunities for a Tailored Approach to Diabetes and Obesity Care. J. Pers. Med. 2022, 12, 454. [Google Scholar] [CrossRef]
- Tahrani, A.A.; Barnett, A.H.; Bailey, C.J. SGLT inhibitors in management of diabetes. Lancet Diabetes Endocrinol. 2013, 1, 140–151. [Google Scholar] [CrossRef]
- Sattar, N.; Fitchett, D.; Hantel, S.; George, J.T.; Zinman, B. Empagliflozin is associated with improvements in liver enzymes potentially consistent with reductions in liver fat: Results from randomised trials including the EMPA-REG OUTCOME® trial. Diabetologia 2018, 61, 2155–2163. [Google Scholar] [CrossRef] [Green Version]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui K., J.; Singh M., K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: A randomized controlled trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montalvo-Gordon, I.; Chi-Cervera, L.A.; García-Tsao, G. Sodium-Glucose Cotransporter 2 Inhibitors ameliorate ascites and peripheral edema in patients with cirrhosis and diabetes. Hepatology 2020, 72, 1880–1882. [Google Scholar] [CrossRef]
- Jojima, T.; Tomotsune, T.; Iijima, T.; Akimoto, K.; Suzuki, K.; Aso, Y. Empagliflozin (an SGLT2 inhibitor), alone or in combination with linagliptin (a DPP-4 inhibitor), prevents steatohepatitis in a novel mouse model of non-alcoholic steatohepatitis and diabetes. Diabetol. Metab. Syndr. 2016, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Qiang, S.; Nakatsu, Y.; Seno, Y.; Fujishiro, M.; Sakoda, H.; Kushiyama, A.; Mori, K.; Matsunaga, Y.; Yamamotoya, T.; Kamata, H.; et al. Treatment with the SGLT2 inhibitor luseogliflozin improves nonalcoholic steatohepatitis in a rodent model with diabetes mellitus. Diabetol. Metab. Syndr. 2015, 7, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, M.; Suzuki, K.; Kato, K.; Jojima, T.; Iijima, T.; Murohisa, T.; Iijima, M.; Takekawa, H.; Usui, I.; Hiraishi, H.; et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes. Metab. 2019, 21, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Gurgle, H.E.; White, K.; McAdam-Marx, C. SGLT2 inhibitors or GLP-1 receptor agonists as second-line therapy in type 2 diabetes: Patient selection and perspectives. Vasc. Health Risk Manag. 2016, 12, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Huebschmann, A.G.; Huxley, R.R.; Kohrt, W.M.; Zeitler, P.; Regensteiner, J.G.; Reusch, J.E. Sex differences in the burden of type 2 diabetes and cardiovascular risk across the life course. Diabetologia 2019, 62, 1761–1772. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.K.; Kontopantelis, E.; Emsley, R.; Buchan, I.; Mamas, M.A.; Sattar, N.; Ashcroft, D.M.; Rutter, M.K. Cardiovascular Risk and Risk Factor Management in Type 2 Diabetes Mellitus. Circulation 2019, 139, 2742–2753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patoulias, D.; Papadopoulos, C.; Doumas, M. Surrogate cardiovascular outcomes with sodium-glucose co-transporter-2 inhibitors in women: An updated meta-analysis. Indian Heart J. 2021, 73, 132–134. [Google Scholar] [CrossRef]


{kind=link}
| Male | Female | References | |
|---|---|---|---|
| HBV/HCV-related chronic hepatitis | Androgens promote HBV transcription. | Oestrogens suppress B virus mRNA levels. | [47,48] |
| Alcoholic liver disease | Higher alcohol dehydrogenase concentration; Higher volume distribution; higher access to treatment; Lower influence of genetic and epigenetic factors. | Lower alcohol dehydrogenase concentration; Lower volume distribution; lower access to treatment; Higher influence of genetic and epigenetic factors. | [38,39,40] |
| Autoimmune disease | Lower frequency; Similar access to treatment; Lower influence of genetic and epigenetic factors. | Higher frequency; Similar access to treatment; Higher influence of genetic and epigenetic factors. | [49,50,51,52] |
| NAFLD | Higher visceral fat. | Protective role of estrogens. | [53,54,55] |
| T2D | CLD | References | |||
|---|---|---|---|---|---|
| Male | Female | Male | Female | ||
| Diet/Lifestyle | Low adherence to diet | Healthier than men, higher attention to diet. | Regardless of gender, some caution needs to be taken for cachexia and sarcopenia in cirrhotic patients. | [98,104] | |
| Statins | No gender differences. | No gender differences. | Contraindicated in the data sheet of drugs for cirrhotic patients. Possible positive effect against HCC. | [105,106] | |
| Ezetimibe | No gender differences. | No gender differences. | Safe in NAFLD/NASH; reduction of AT and GGT levels, lower steatosis and hepatocyte ballooning. No effects on hepatic inflammation and fibrosis. Significant improvement in liver fat when combined with rosuvastatin. | [107,108] | |
| Fibrates | Minor protective effect of fenofibrate on CV events in females. | Pemafibrate significantly improves liver function, serum TG and liver stiffness in NAFLD patients. | [109,110] | ||
| Pioglitazone | Greater metabolic benefit (glycaemic control, HOMA IR and lipid improvement). More frequent side effects such as oedema. | Current guidelines indicate Pioglitazone for T2D patients with NASH. | [111,112] | ||
| PCSK9i | No gender differences. | Higher circulating concentrations, especially after menopause. Potential regulatory role played by oestrogens. | Correlation between hepatic fat content and PCSK9 levels in NAFLD early stage, not present in the late stages of liver disease. PCSK9 levels are lower in cirrhotic patients and do not correlate with Child–Pugh score, MELD score, bilirubin or AT. | [113,114,115] | |
| Metformin | Greater gastro-intestinal side effects. | Lower doses needed. | Better glycaemic targets reached. | [116,117,118,119] | |
| Lower doses in cirrhotic patients, especially with an eGFR lower than 30 mL/min/1.73 m2. | |||||
| DPP-4 | Improvement of heart function, blood pressure and body weight. | Caution for hepatotoxicity (Vildagliptin). | [120,121] | ||
| GLP-1 RAs | Great effects on Hb1Ac (Exenatide), not present with Dulaglutide. | Greater side effects; higher weight loss. | Great effectiveness for NASH (Liraglutide). Caution in advanced liver disease, limited data about safety and efficacy. | [122,123,124] | |
| SGLT-2i | Greater CV benefits (heart failure). | Improvement of ALT levels, ascites and oedema in decompensated cirrhosis. | [76,125,126] | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Licata, A.; Russo, G.T.; Giandalia, A.; Cammilleri, M.; Asero, C.; Cacciola, I. Impact of Sex and Gender on Clinical Management of Patients with Advanced Chronic Liver Disease and Type 2 Diabetes. J. Pers. Med. 2023, 13, 558. https://doi.org/10.3390/jpm13030558
Licata A, Russo GT, Giandalia A, Cammilleri M, Asero C, Cacciola I. Impact of Sex and Gender on Clinical Management of Patients with Advanced Chronic Liver Disease and Type 2 Diabetes. Journal of Personalized Medicine. 2023; 13(3):558. https://doi.org/10.3390/jpm13030558
Chicago/Turabian StyleLicata, Anna, Giuseppina T. Russo, Annalisa Giandalia, Marcella Cammilleri, Clelia Asero, and Irene Cacciola. 2023. "Impact of Sex and Gender on Clinical Management of Patients with Advanced Chronic Liver Disease and Type 2 Diabetes" Journal of Personalized Medicine 13, no. 3: 558. https://doi.org/10.3390/jpm13030558