
Improving the Classification of PCNSL and Brain Metastases by Developing a Machine Learning Model Based on 18F-FDG PET
 ,
,
Abstract
:1. Instruction
2. Materials and Methods
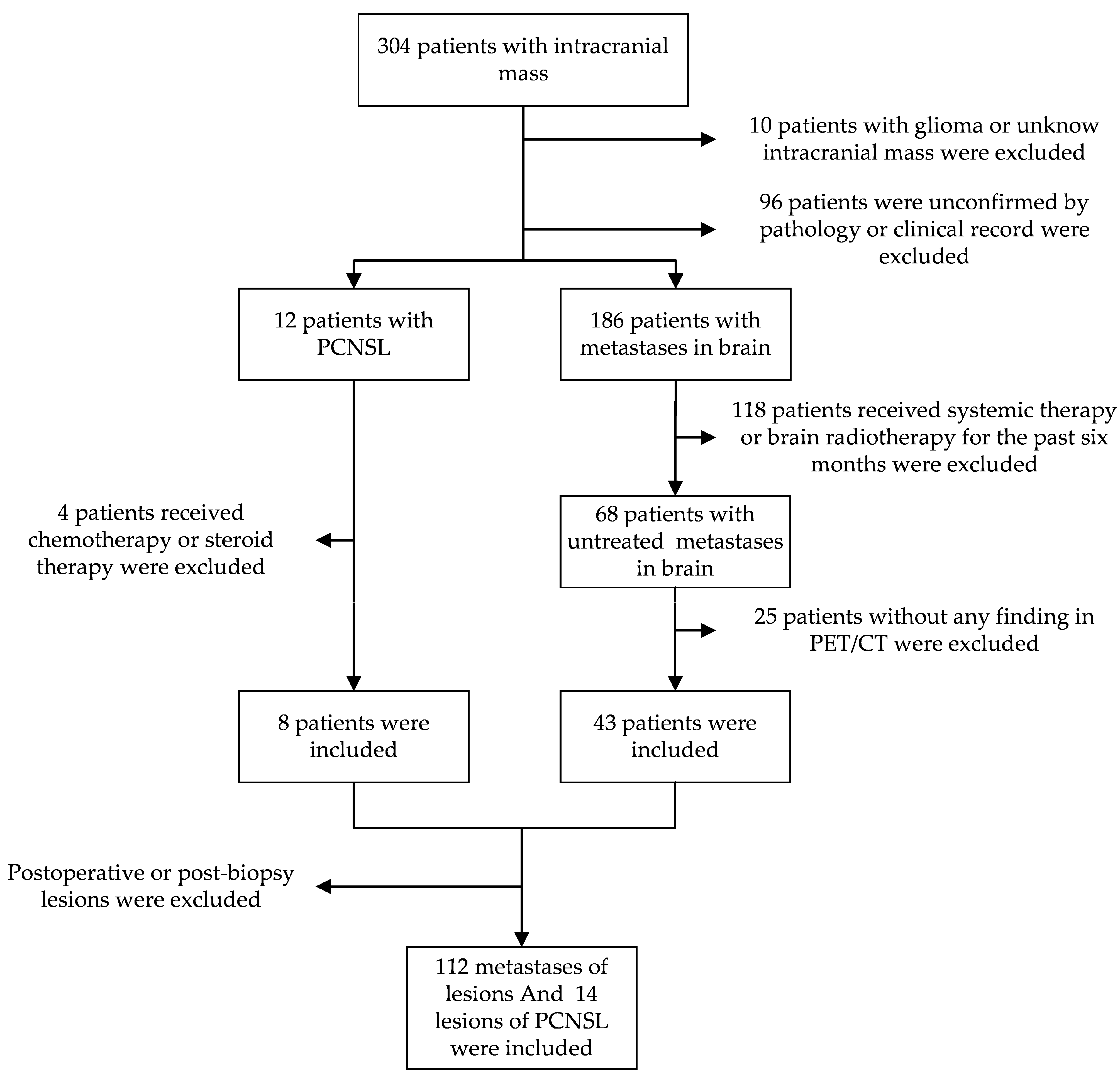
2.1. Study Participants
2.2. 18F-FDG PET/CT Protocol
2.3. Segmentation of Images
2.4. Feature Extraction
2.5. Model Training and Validation
2.5.1. Statistical Analysis
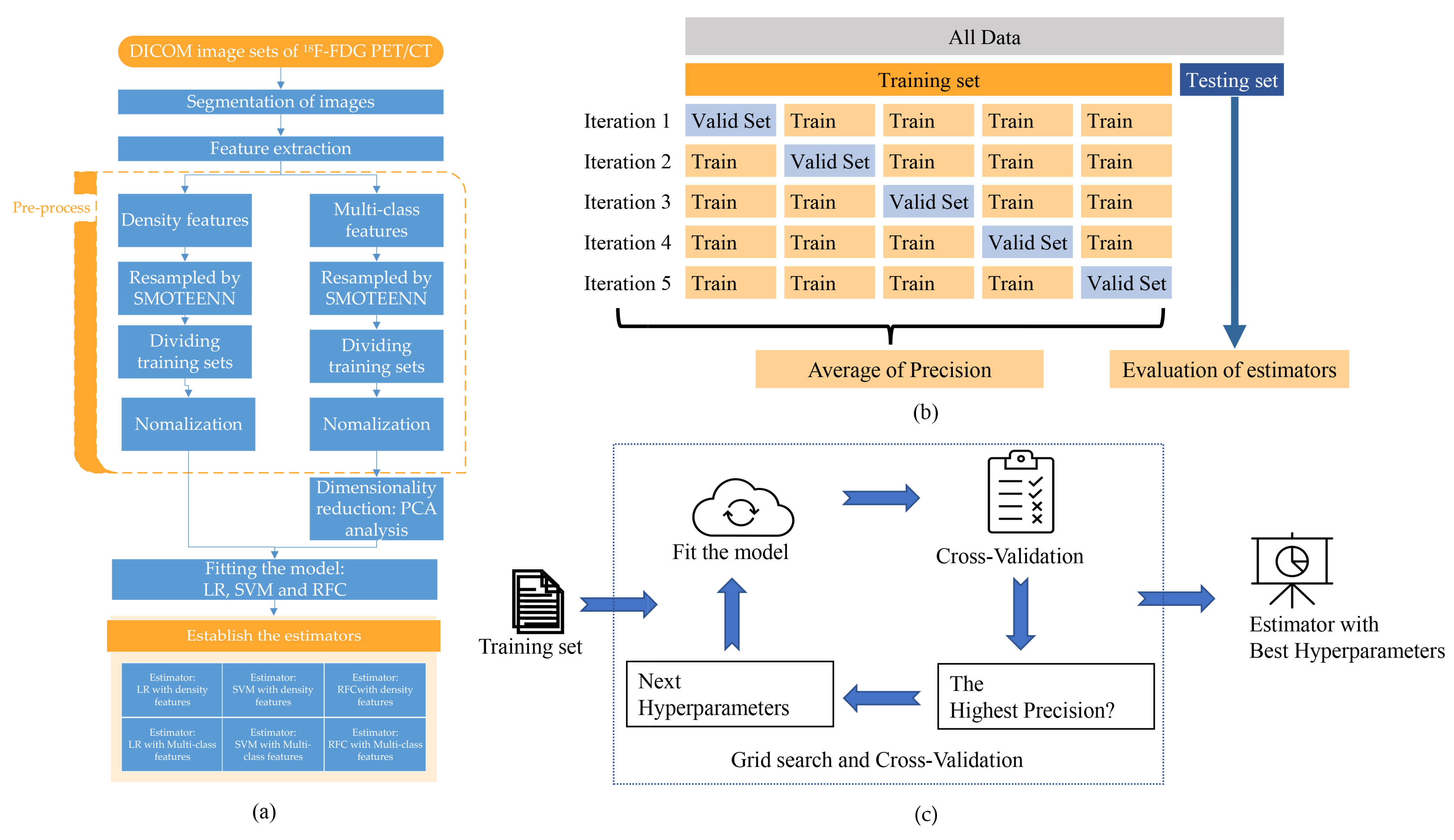
2.5.2. Pre-Process of Datasets
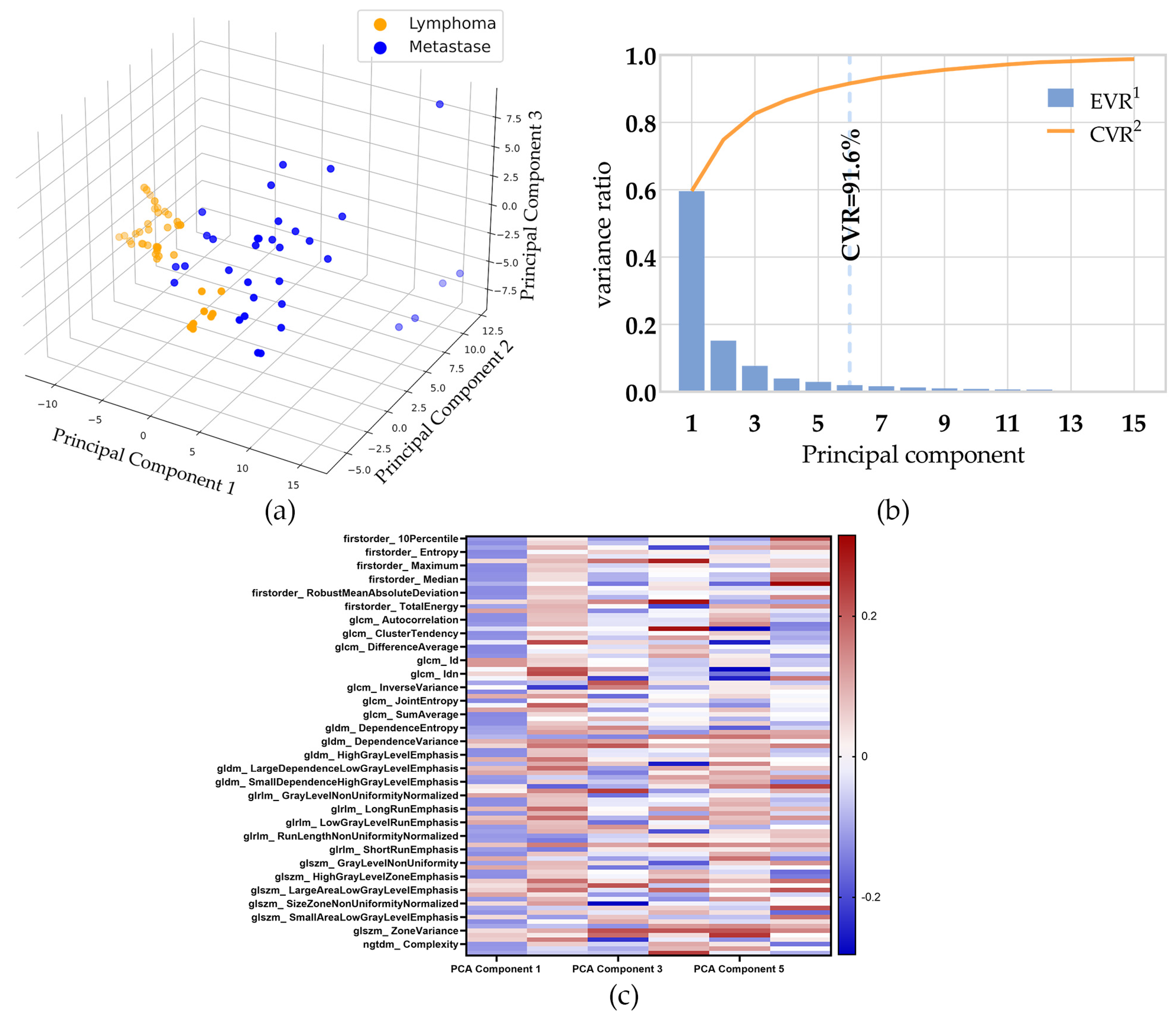
2.5.3. Dimensionality Reduction
2.5.4. Fitting the Model and Internal Cross-Validation
2.5.5. Evaluation of Estimators
3. Result
3.1. Study Participants
3.2. Dimensionality Reduction
3.3. Modeling and Validating
3.3.1. Fit the Model and Internal Cross-Validation
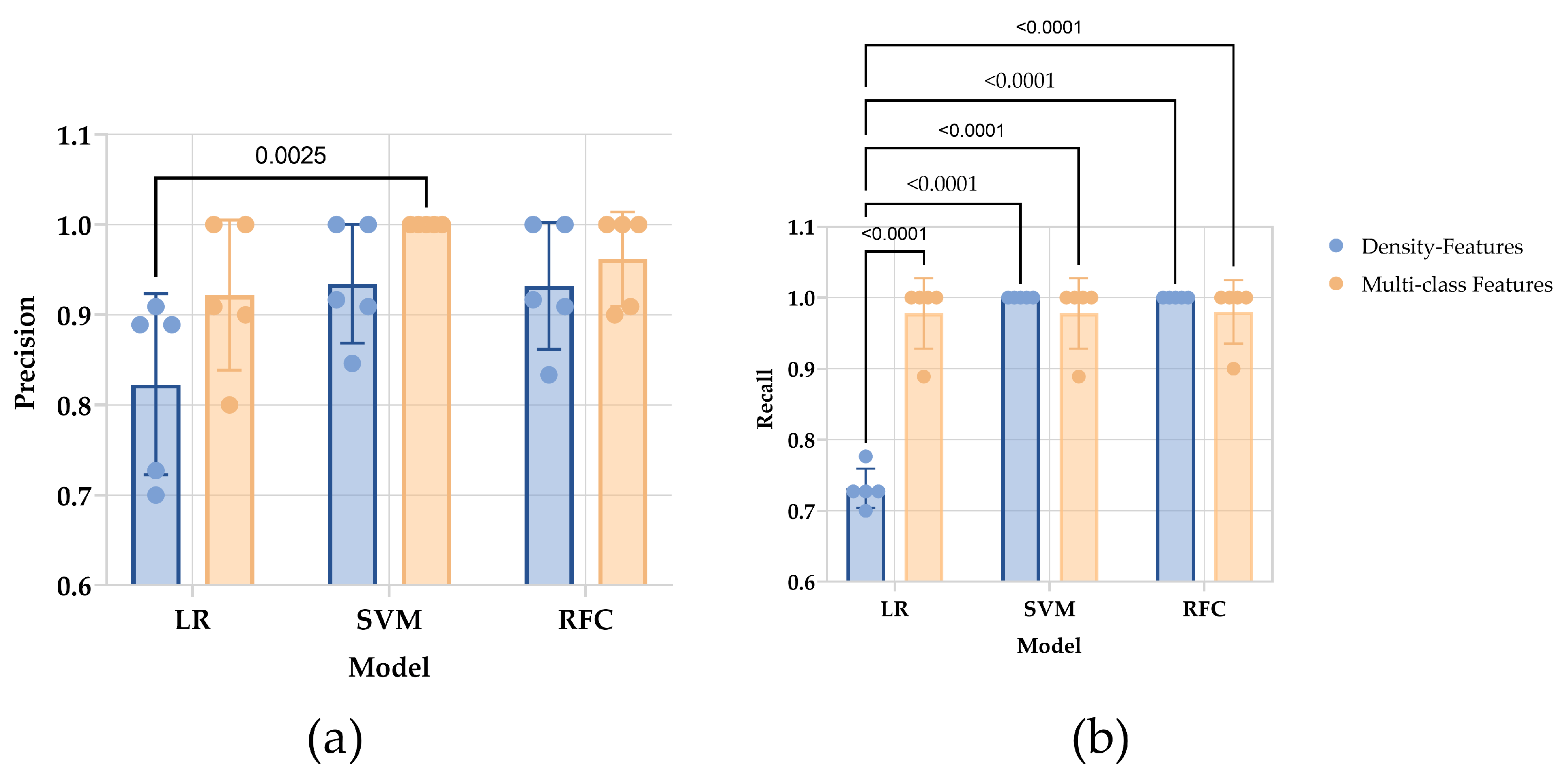
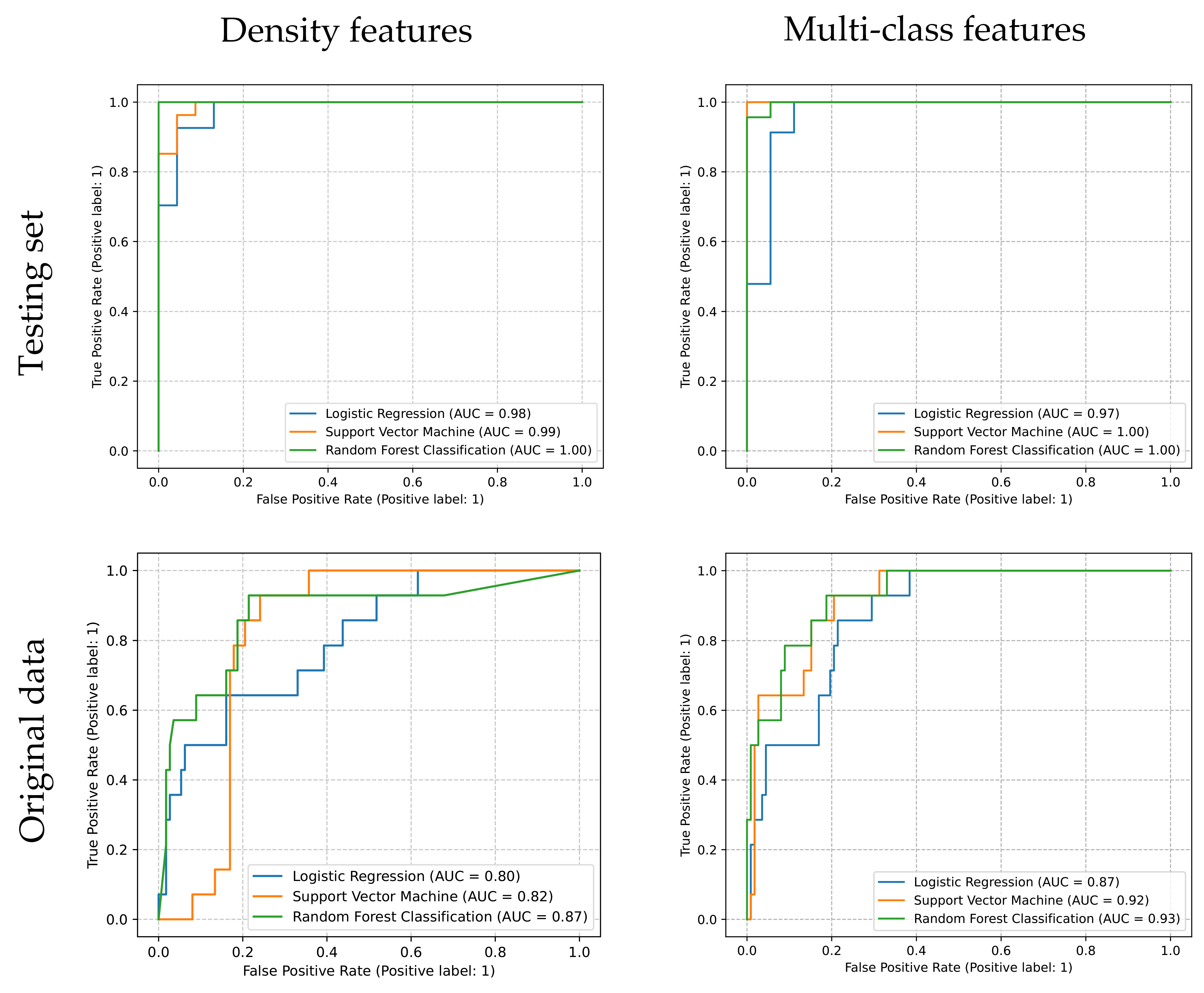
3.3.2. Evaluation of Estimators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pietrzak, A.; Marszałek, A.; Kunikowska, J.; Piotrowski, T.; Medak, A.; Pietrasz, K.; Wojtowicz, J.; Cholewiński, W. Detection of clinically silent brain lesions in [18F]FDG PET/CT study in oncological patients: Analysis of over 10,000 studies. Sci. Rep. 2021, 11, 18293. [Google Scholar] [CrossRef]
- Zhao, C.; Zhang, Y.; Wang, J. A meta-analysis on the diagnostic performance of (18)F-FDG and (11)C-methionine PET for differentiating brain tumors. Am. J. Neuroradiol. 2014, 35, 1058–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; He, M.Z.; Li, T.; Yang, X. MRI combined with PET-CT of different tracers to improve the accuracy of glioma diagnosis: A systematic review and meta-analysis. Neurosurg. Rev. 2019, 42, 185–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, B.P.; Decker, P.A.; Tieu, C.; Cerhan, J.R. The changing incidence of primary central nervous system lymphoma is driven primarily by the changing incidence in young and middle-aged men and differs from time trends in systemic diffuse large B-cell non-Hodgkin’s lymphoma. Am. J. Hematol. 2013, 88, 997–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brastianos, P.K.; Batchelor, T.T. Primary Central Nervous System Lymphoma. In Encyclopedia of the Neurological Sciences, 2nd ed.; Aminoff, M.J., Daroff, R.B., Eds.; Academic Press: Oxford, UK, 2014; pp. 971–977. ISBN 978-0-12-385158-1. [Google Scholar]
- Puhakka, I.; Kuitunen, H.; Jäkälä, P.; Sonkajärvi, E.; Turpeenniemi-Hujanen, T.; Rönkä, A.; Selander, T.; Korhonen, M.; Kuittinen, O. Primary central nervous system lymphoma high incidence and poor survival in Finnish population-based analysis. BMC Cancer 2022, 22, 236. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.P.; Phillips, E.H.; Smith, J.; Linton, K.; Gallop-Evans, E.; Hemmaway, C.; Auer, D.P.; Fuller, C.; Davies, A.J.; McKay, P.; et al. Guidelines for the diagnosis and management of primary central nervous system diffuse large B-cell lymphoma. Br. J. Haematol. 2019, 184, 348–363. [Google Scholar] [CrossRef] [Green Version]
- Proescholdt, M.A.; Schodel, P.; Doenitz, C.; Pukrop, T.; Hohne, J.; Schmidt, N.O.; Schebesch, K.M. The Management of Brain Metastases-Systematic Review of Neurosurgical Aspects. Cancers 2021, 13, 1616. [Google Scholar] [CrossRef]
- Scheichel, F.; Marhold, F.; Pinggera, D.; Kiesel, B.; Rossmann, T.; Popadic, B.; Woehrer, A.; Weber, M.; Kitzwoegerer, M.; Geissler, K.; et al. Influence of preoperative corticosteroid treatment on rate of diagnostic surgeries in primary central nervous system lymphoma: A multicenter retrospective study. BMC Cancer 2021, 21, 754. [Google Scholar] [CrossRef]
- Kuker, W.; Nagele, T.; Korfel, A.; Heckl, S.; Thiel, E.; Bamberg, M.; Weller, M.; Herrlinger, U. Primary central nervous system lymphomas (PCNSL): MRI features at presentation in 100 patients. J. Neuro-Oncol. 2005, 72, 169–177. [Google Scholar] [CrossRef]
- Haldorsen, I.S.; Espeland, A.; Larsson, E.M. Central nervous system lymphoma: Characteristic findings on traditional and advanced imaging. Am. J. Neuroradiol. 2011, 32, 984–992. [Google Scholar] [CrossRef] [Green Version]
- Kawai, N.; Miyake, K.; Yamamoto, Y.; Nishiyama, Y.; Tamiya, T. 18F-FDG PET in the diagnosis and treatment of primary central nervous system lymphoma. Biomed Res. Int. 2013, 2013, 247152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, X.; Tan, D.; Liu, Z.; Liao, M.; Kan, Y.; Yao, R.; Zhang, L.; Nie, L.; Liao, R.; Chen, S.; et al. Differentiating solitary brain metastases from glioblastoma by radiomics features derived from MRI and 18F-FDG-PET and the combined application of multiple models. Sci. Rep. 2022, 12, 5722. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Qiao, Z.; Zhao, X.; Li, X.; Wang, X.; Wu, T.; Chen, Z.; Fan, D.; Chen, Q.; Ai, L. Individualized discrimination of tumor recurrence from radiation necrosis in glioma patients using an integrated radiomics-based model. Eur. J. Nucl. Med. Mol. 2020, 47, 1400–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Bmj-Br. Med. J. 2015, 350, g7594. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Jentzen, W.; Freudenberg, L.; Eising, E.G.; Heinze, M.; Brandau, W.; Bockisch, A. Segmentation of PET Volumes by Iterative Image Thresholding. Soc. Nucl. Med. 2007, 48, 108–114. [Google Scholar]
- van Griethuysen, J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Orlhac, F.; Soussan, M.; Chouahnia, K.; Martinod, E.; Buvat, I. 18F-FDG PET-Derived Textural Indices Reflect Tissue-Specific Uptake Pattern in Non-Small Cell Lung Cancer. PLoS ONE 2015, 10, e145063. [Google Scholar] [CrossRef]
- Baesens, B.; Viaene, S.; Van Gestel, T.; Suykens, J.A.K.; Dedene, G.; De Moor, B.; Vanthienen, J. Least Squares Support Vector Machine Classifiers: An Empirical Evaluation. TEW Res. Rep. 0003 2000, 1–16. [Google Scholar]
- Menard, S. Six Approaches to Calculating Standardized Logistic Regression Coefficients. Am. Stat. 2004, 58, 218–223. [Google Scholar] [CrossRef]
- Liaw, A.; Wiener, M.C. Classification and Regression by Randomforest. R News 2002, 2, 18–22. [Google Scholar]
- Tre, G.L.I.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn Res. 2017, 18, 1–5. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Rao, R.B.; Fung, G.; Rosales, R. On the Dangers of Cross-Validation. An Experimental Evaluation. In Proceedings of the SIAM International Conference on Data Mining, Atlanta, GA, USA, 24–26 April 2008; p. 588. [Google Scholar]
- Wu, C.; Xue, X.; Song, Y. Research on Cancer Diagnosis Method Based on LightGBM-Gridsearchcv. In Proceedings of the 4th International Conference on Big Data Engineering, Beijing, China, 26–28 May 2022; pp. 122–126. [Google Scholar]
- Taha, A.A.; Hanbury, A. Metrics for evaluating 3D medical image segmentation: Analysis, selection, and tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Suh, C.H.; Kim, H.S.; Park, J.E.; Jung, S.C.; Choi, C.G.; Kim, S.J. Primary Central Nervous System Lymphoma: Diagnostic Yield of Whole-Body CT and FDG PET/CT for Initial Systemic Imaging. Radiology 2019, 292, 440–446. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Hirata, K.; Kobayashi, H.; Shiga, T.; Manabe, O.; Kobayashi, K.; Motegi, H.; Terasaka, S.; Houkin, K. The diagnostic role of (18)F-FDG PET for primary central nervous system lymphoma. Ann. Nucl. Med. 2014, 28, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Kawai, N.; Miyake, K.; Okada, M.; Yamamoto, Y.; Nishiyama, Y.; Tamiya, T. Usefulness and limitation of FDG-PET in the diagnosis of primary central nervous system lymphoma. No Shinkei Geka 2013, 41, 117–126. [Google Scholar]
- Kong, Z.; Jiang, C.; Zhu, R.; Feng, S.; Wang, Y.; Li, J.; Chen, W.; Liu, P.; Zhao, D.; Ma, W.; et al. 18F-FDG-PET-based radiomics features to distinguish primary central nervous system lymphoma from glioblastoma. NeuroImage Clin. 2019, 23, 101912. [Google Scholar] [CrossRef] [PubMed]
- Kunimatsu, A.; Kunimatsu, N.; Kamiya, K.; Watadani, T.; Mori, H.; Abe, O. Comparison between Glioblastoma and Primary Central Nervous System Lymphoma Using MR Image-based Texture Analysis. Magn. Reason. Med. Sci. 2018, 17, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, H.B.; Choi, Y.S.; Bae, S.; Ahn, S.S.; Chang, J.H.; Kang, S.G.; Kim, E.H.; Kim, S.H.; Lee, S.K. Primary central nervous system lymphoma and atypical glioblastoma: Differentiation using radiomics approach. Eur. Radiol. 2018, 28, 3832–3839. [Google Scholar] [CrossRef]
- Kang, D.; Park, J.E.; Kim, Y.H.; Kim, J.H.; Oh, J.Y.; Kim, J.; Kim, Y.; Kim, S.T.; Kim, H.S. Diffusion radiomics as a diagnostic model for atypical manifestation of primary central nervous system lymphoma: Development and multicenter external validation. Neuro-Oncology 2018, 20, 1251–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Loeffler, J.S. Management of brain metastases. Oncology 1999, 13, 941–954. [Google Scholar] [PubMed]
- Batista, G.E.A.P.; Prati, R.C.; Monard, M.C. A Study of the Behavior of Several Methods for Balancing Machine Learning Training Data. SIGKDD Explor. Newsl. 2004, 6, 20–29. [Google Scholar] [CrossRef]
- Wang, H.; Li, X.; Yuan, Y.; Tong, Y.; Zhu, S.; Huang, R.; Shen, K.; Guo, Y.; Wang, Y.; Chen, X. Association of machine learning ultrasound radiomics and disease outcome in triple negative breast cancer. Am. J. Cancer Res. 2022, 12, 152–164. [Google Scholar] [PubMed]
- Ji, W.; Zhang, Y.; Cheng, Y.; Wang, Y.; Zhou, Y. Development and validation of prediction models for hypertension risks: A cross-sectional study based on 4,287,407 participants. Front. Cardiovasc. Med. 2022, 9, 928948. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto-Roth, E.; Surendra, A.; Lavallée-Adam, M.; Bennett, S.; Čuperlović-Culf, M. METAbolomics data Balancing with Over-sampling Algorithms (Meta-BOA): An online resource for addressing class imbalance. Bioinformatics 2022, 38, 5326–5327. [Google Scholar] [CrossRef]
- Ullah, Z.; Saleem, F.; Jamjoom, M.; Fakieh, B.; Kateb, F.; Ali, A.M.; Shah, B. Detecting High-Risk Factors and Early Diagnosis of Diabetes Using Machine Learning Methods. Comput. Intell. Neurosc. 2022, 2022, 2557795. [Google Scholar] [CrossRef]
- Oommen, T.; Misra, D.; Twarakavi, N.K.C.; Prakash, A.; Sahoo, B.; Bandopadhyay, S. An Objective Analysis of Support Vector Machine Based Classification for Remote Sensing. Math. Geosci. 2008, 40, 409–424. [Google Scholar] [CrossRef]
- Ballabio, D. A MATLAB toolbox for Principal Component Analysis and unsupervised exploration of data structure. Chemometr. Intell. Lab. 2015, 149, 1–9. [Google Scholar] [CrossRef]
- Jeni, L.A.; Cohn, J.F.; De La Torre, F. Facing Imbalanced Data--Recommendations for the Use of Performance Metrics. In Proceedings of the 2013 Humaine Association Conference on Affective Computing and Intelligent Interaction, Geneva, Switzerland, 2–5 September 2013; pp. 245–251. [Google Scholar]
- Takahashi, K.; Yamamoto, K.; Kuchiba, A.; Koyama, T. Confidence interval for micro-averaged F 1 and macro-averaged F 1 scores. Appl. Intell. 2022, 52, 4961–4972. [Google Scholar] [CrossRef]
- Kernbach, J.M.; Staartjes, V.E. Foundations of Machine Learning-Based Clinical Prediction Modeling: Part II—Generalization and Overfitting. Acta Neurochir. Suppl. 2022, 134, 15–21. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PCNSL | Metastases | p Value |
|---|---|---|---|
| Sex | 0.0986 2 | ||
| Male | 3 | 31 | |
| Female | 5 | 12 | |
| Age | 56.00 ± 13.98 | 59.49 ± 11.74 | 0.4570 3 |
| SUVmax 1 | 20.14 ± 7.58 | 12.80 ± 4.84 | 0.0006 3 |
| Pathology | |||
| B cell lymphoma | 8 | ||
| Squamous carcinoma 4 | 12 | ||
| Adenocarcinoma 4 | 22 | ||
| Melanoma 4 | 3 | ||
| Renal clear cell cancer 4 | 2 | ||
| Neuroendocrine carcinoma 4 | 2 |
| Density Features | Multi-Class Features | |||
|---|---|---|---|---|
| Hyperparameters | Precision | Hyperparameters | Precision | |
| LR | C: 1.0 dual: True multi_class: ovr penalty: l2 solver: liblinear | 0.822 ± 0.090 | C: 1.4 dual: False multi_class: ovr penalty: l1 solver: liblinear | 0.921 ± 0.074 |
| SVM | C: 2.81 gamma: 2.21 kernel: rbf | 0.934 ± 0.060 | C: 7.01 gamma: 0.21 kernel: poly | 1.0 ± 0.0 |
| RFC | bootstrap: False max_depth: 20 max_features: log2 min_samples_leaf: 4 min_samples_split: 16 n_estimators: 500 | 0.932 ± 0.063 | bootstrap: False max_depth: 5 max_features: sqrt min_samples_leaf: 2 min_samples_split: 8 n_estimators: 500. | 0.962 ± 0.047 |
| Density Features | Multi-Class Features | |||
|---|---|---|---|---|
| Testing Set | Original Data | Testing Set | Original Data | |
| LR | 0.86 | 0.79 | 0.93 | 0.82 |
| SVM | 0.96 | 0.78 | 0.98 | 0.83 |
| RFC | 1.00 | 0.82 | 0.98 | 0.85 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, C.; Yao, X.; Xu, L.; Chao, Y.; Hu, Y.; Zhao, S.; Hu, Y.; Zhang, J. Improving the Classification of PCNSL and Brain Metastases by Developing a Machine Learning Model Based on 18F-FDG PET. J. Pers. Med. 2023, 13, 539. https://doi.org/10.3390/jpm13030539
Cui C, Yao X, Xu L, Chao Y, Hu Y, Zhao S, Hu Y, Zhang J. Improving the Classification of PCNSL and Brain Metastases by Developing a Machine Learning Model Based on 18F-FDG PET. Journal of Personalized Medicine. 2023; 13(3):539. https://doi.org/10.3390/jpm13030539
Chicago/Turabian StyleCui, Can, Xiaochen Yao, Lei Xu, Yuelin Chao, Yao Hu, Shuang Zhao, Yuxiao Hu, and Jia Zhang. 2023. "Improving the Classification of PCNSL and Brain Metastases by Developing a Machine Learning Model Based on 18F-FDG PET" Journal of Personalized Medicine 13, no. 3: 539. https://doi.org/10.3390/jpm13030539