
Pain Trajectory after Short-Stay Anorectal Surgery: A Prospective Observational Study

Abstract
:1. Introduction
2. Methods
2.1. Anesthesia and Analgesia
2.2. Data Collection
2.2.1. Sociodemographic and Clinical Measures
2.2.2. Pain Assessment
2.2.3. Outcome Measures
2.3. Statistical Analysis
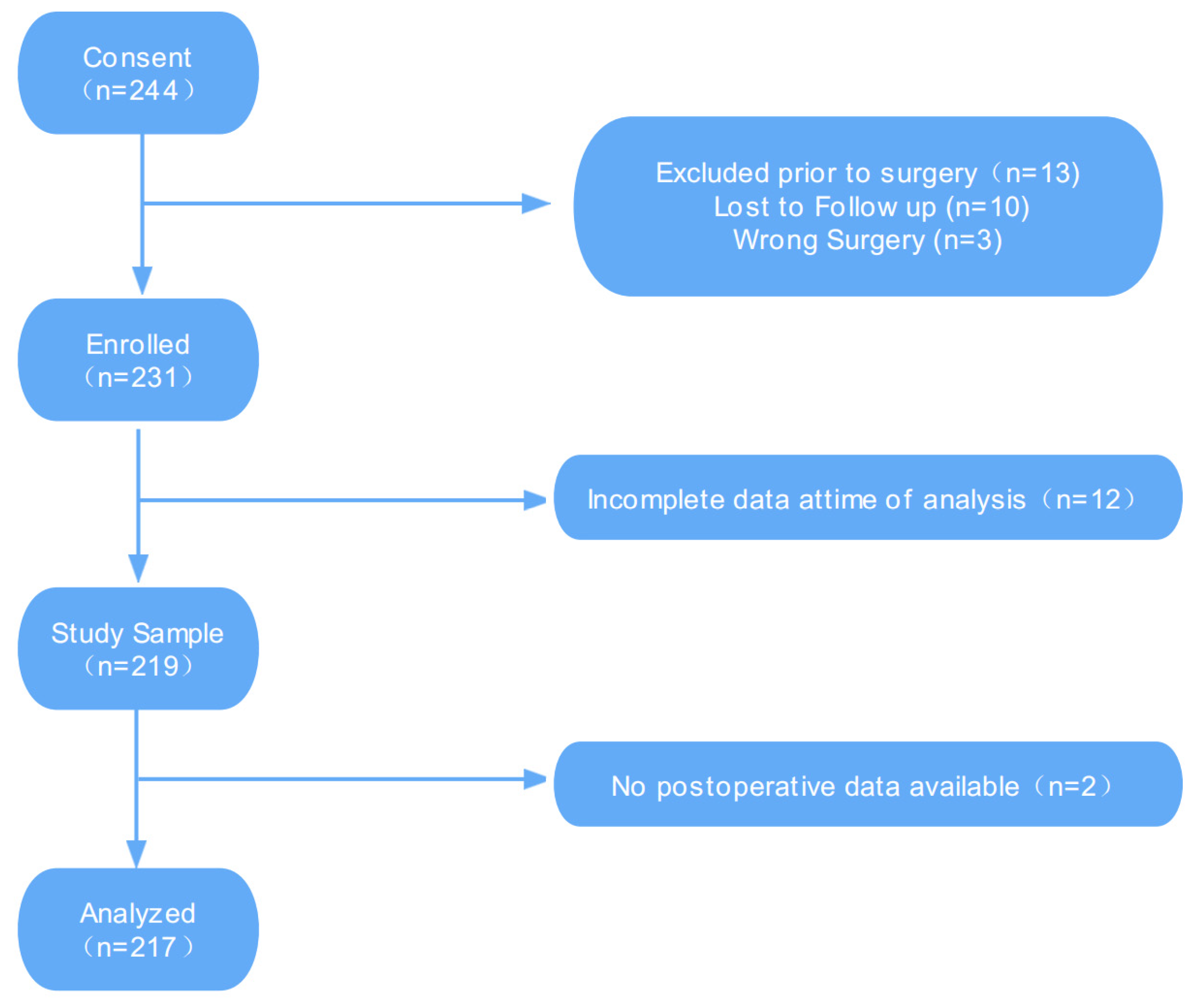
3. Results
3.1. Patient Characteristics
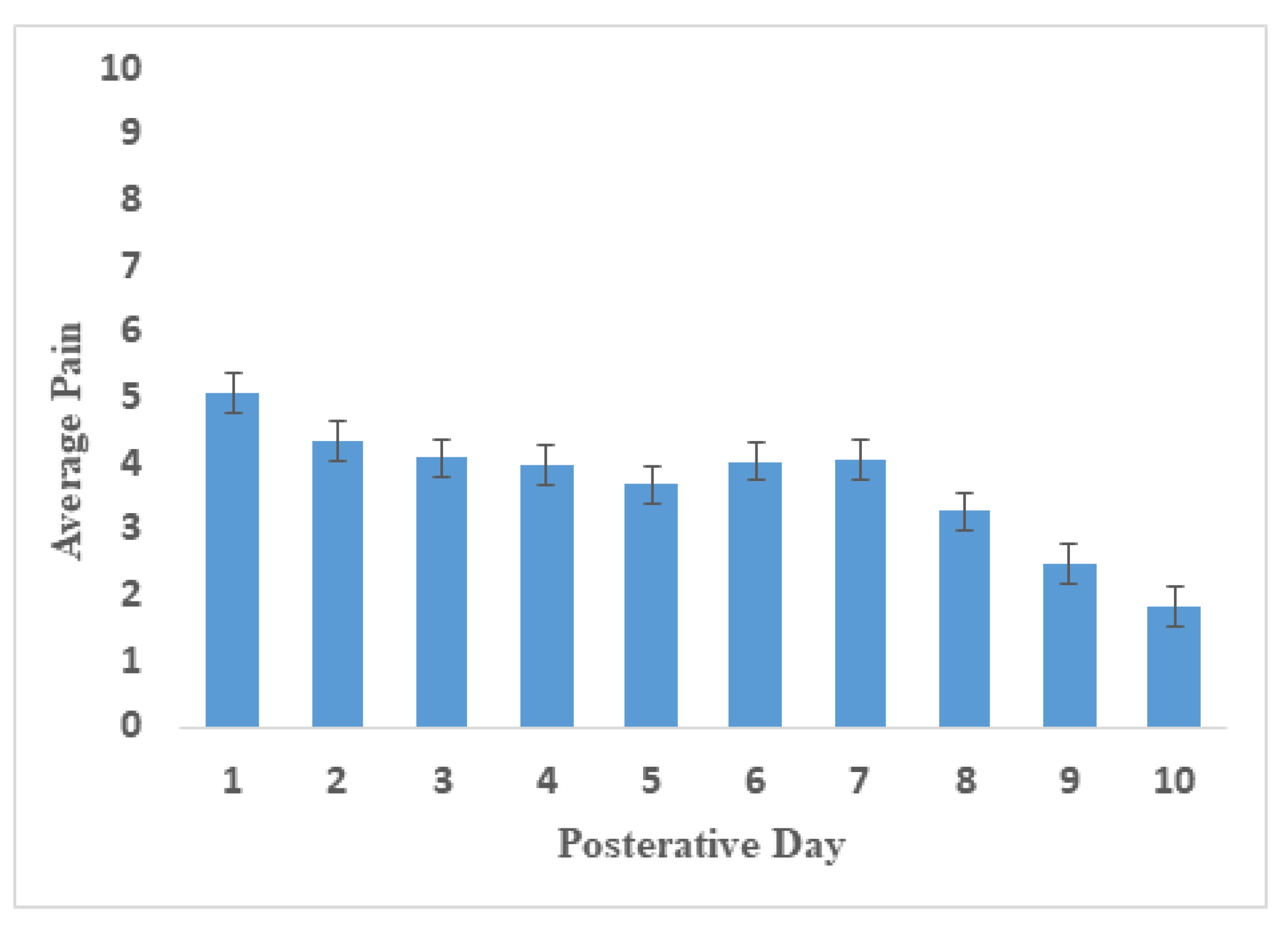
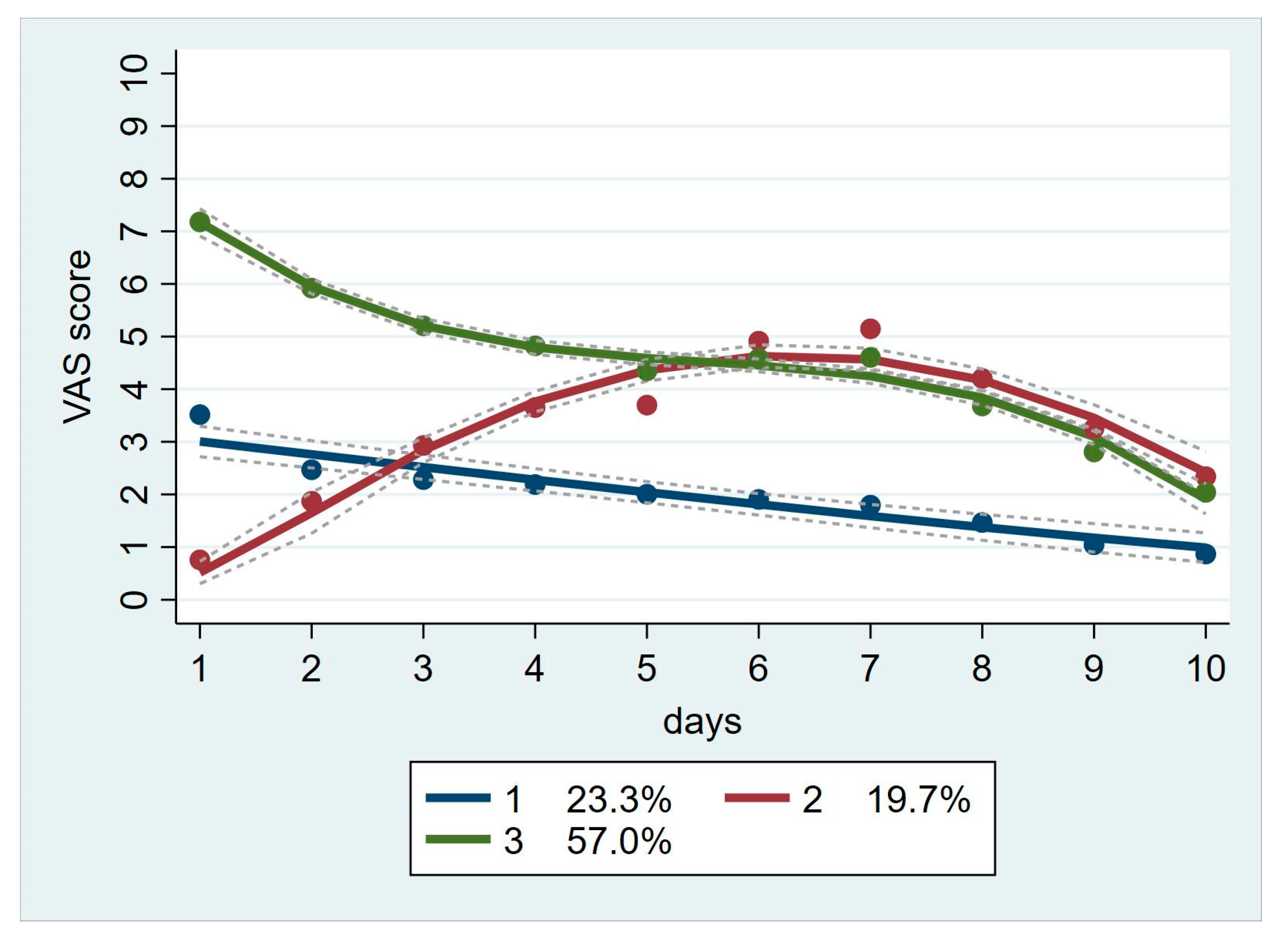
3.2. Daily Pain and Group-Based Trajectory Analysis
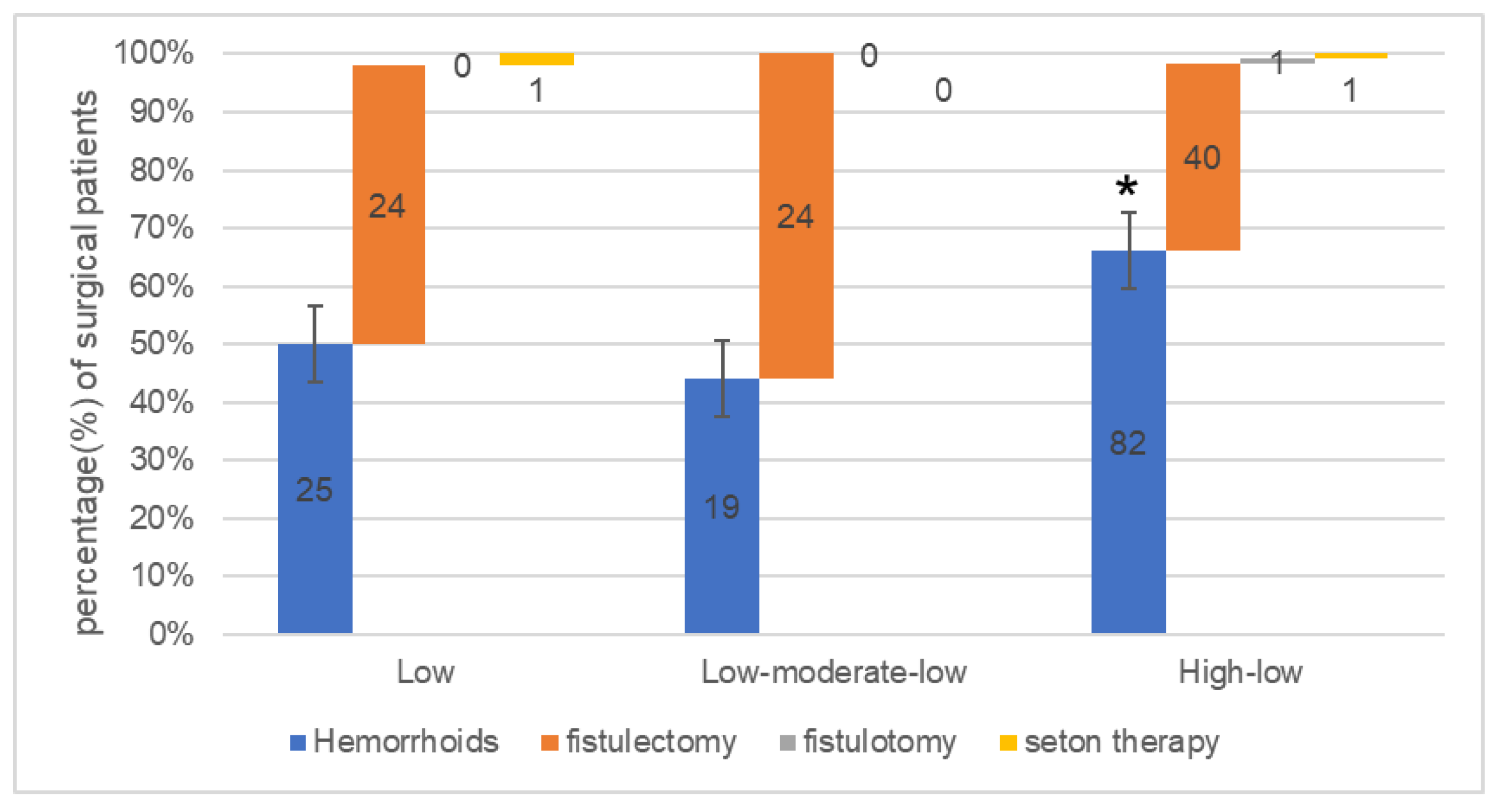
3.3. Multivariable Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parés, D.; Abcarian, H. Management of Common Benign Anorectal Disease: What All Physicians Need to Know. Am. J. Med. 2018, 131, 745–751. [Google Scholar] [CrossRef]
- Abcarian, H. Anorectal infection: Abscess-fistula. Clin. Colon Rectal Surg. 2011, 24, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohsiriwat, V. Hemorrhoids: From basic pathophysiology to clinical management. World J. Gastroenterol. 2012, 18, 2009–2017. [Google Scholar] [CrossRef] [PubMed]
- Riss, S.; Weiser, F.A.; Schwameis, K.; Riss, T.; Mittlböck, M.; Steiner, G.; Stift, A. The prevalence of hemorrhoids in adults. Int. J. Color. Dis. 2012, 27, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Bottini, C.; De Nardi, P.; Giamundo, P.; Lauretta, A.; Realis Luc, A.; Piloni, V. Evaluation and management of perianal abscess and anal fistula: SICCR position statement. Tech. Coloproctol. 2020, 24, 127–143. [Google Scholar] [CrossRef]
- Owen, H.A.; Buchanan, G.N.; Schizas, A.; Cohen, R.; Williams, A.B. Quality of life with anal fistula. Ann. R. Coll. Surg. Engl. 2016, 98, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Márquez, M.; Espínola-Cortés, N.; Reina-Duarte, A.; Granero-Molina, J.; Fernández-Sola, C.; Hernández-Padilla, J.M. Design and Psychometric Evaluation of the Quality of Life in Patients With Anal Fistula Questionnaire. Dis. Colon Rectum 2017, 60, 1083–1091. [Google Scholar] [CrossRef]
- Lee, P.C.; Hu, Y.W.; Hung, M.H.; Chen, C.C.; Lin, H.C.; Lee, F.Y.; Hung, Y.P.; Yi-Fong Su, V.; Yen, S.H.; Tzeng, C.H.; et al. The risk of cancer in patients with benign anal lesions: A nationwide population-based study. Am. J. Med. 2013, 126, 1143.e9–1143.e18. [Google Scholar] [CrossRef]
- Medina-Gallardo, A.; Curbelo-Peña, Y.; De Castro, X.; Roura-Poch, P.; Roca-Closa, J.; De Caralt-Mestres, E. Is the severe pain after Milligan-Morgan hemorrhoidectomy still currently remaining a major postoperative problem despite being one of the oldest surgical techniques described? A case series of 117 consecutive patients. Int. J. Surg. Case Rep. 2017, 30, 73–75. [Google Scholar] [CrossRef]
- Cohee, M.W.; Hurff, A.; Gazewood, J.D. Benign Anorectal Conditions: Evaluation and Management. Am. Fam. Physician 2020, 101, 24–33. [Google Scholar]
- Davis, B.R.; Lee-Kong, S.A.; Migaly, J.; Feingold, D.L.; Steele, S.R. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis. Colon Rectum 2018, 61, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Vogel, J.D.; Johnson, E.K.; Morris, A.M.; Paquette, I.M.; Saclarides, T.J.; Feingold, D.L.; Steele, S.R. Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula. Dis. Colon Rectum 2016, 59, 1117–1133. [Google Scholar] [CrossRef] [PubMed]
- Shouler, P.J.; Grimley, R.P.; Keighley, M.R.; Alexander-Williams, J. Fistula-in-ano is usually simple to manage surgically. Int. J. Color. Dis. 1986, 1, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Ivatury, S.J.; Swarup, A.; Wilson, M.Z.; Wilson, L.R. Prospective Evaluation of a Standardized Opioid Reduction Protocol after Anorectal Surgery. J. Surg. Res. 2020, 256, 564–569. [Google Scholar] [CrossRef]
- Sammour, T.; Barazanchi, A.W.; Hill, A.G. Evidence-Based Management of Pain After Excisional Haemorrhoidectomy Surgery: A PROSPECT Review Update. World J. Surg. 2017, 41, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J. Testing for and the role of anal and rectal sensation. Bailliere’s Clin. Gastroenterol. 1992, 6, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Luedi, M.M.; Schober, P.; Hammoud, B.; Andereggen, L.; Hoenemann, C.; Doll, D. Preoperative Pressure Pain Threshold Is Associated with Postoperative Pain in Short-Stay Anorectal Surgery: A Prospective Observational Study. Anesth. Analg. 2021, 132, 656–662. [Google Scholar] [CrossRef]
- Ceulemans, A.; De Looze, D.; Van de Putte, D.; Stiers, E.; Coppens, M. High post-operative pain scores despite multimodal analgesia in ambulatory anorectal surgery: A prospective cohort study. Acta Chir. Belg. 2019, 119, 224–230. [Google Scholar] [CrossRef]
- Richards, S.J.; Nepomuceno, C.; Riles, M.; Suer, Z. Assessing pain behavior: The UAB Pain Behavior Scale. Pain 1982, 14, 393–398. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, X.; Hu, T.; Zhang, F.; Pan, L.; Luo, Y.; Wang, Z. Development and psychometric validity of the perioperative anxiety scale-7 (PAS-7). BMC Psychiatry 2021, 21, 358. [Google Scholar] [CrossRef]
- Vasilopoulos, T.; Wardhan, R.; Rashidi, P.; Fillingim, R.B.; Wallace, M.R.; Crispen, P.L.; Parvataneni, H.K.; Prieto, H.A.; Machuca, T.N.; Hughes, S.J.; et al. Patient and Procedural Determinants of Postoperative Pain Trajectories. Anesthesiology 2021, 134, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Vasilopoulos, T.; Morey, T.E.; Dhatariya, K.; Rice, M.J. Limitations of Significance Testing in Clinical Research: A Review of Multiple Comparison Corrections and Effect Size Calculations with Correlated Measures. Anesth. Analg. 2016, 122, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Mohamedahmed, A.Y.Y.; Stonelake, S.; Mohammed, S.S.S.; Zaman, S.; Ahmed, H.; Albarade, M.; Hajibandeh, S. Haemorrhoidectomy under local anaesthesia versus spinal anaesthesia: A systematic review and meta-analysis. Int. J. Color. Dis. 2020, 35, 2171–2183. [Google Scholar] [CrossRef] [PubMed]
- Bailey, K.M.; Howard, J.J.; El-Hawary, R.; Chorney, J. Pain Trajectories Following Adolescent Idiopathic Scoliosis Correction: Analysis of Predictors and Functional Outcomes. JBJS Open Access 2021, 6, e20. [Google Scholar] [CrossRef] [PubMed]
- Panzenbeck, P.; von Keudell, A.; Joshi, G.P.; Xu, C.X.; Vlassakov, K.; Schreiber, K.L.; Rathmell, J.P.; Lirk, P. Procedure-specific acute pain trajectory after elective total hip arthroplasty: Systematic review and data synthesis. Br. J. Anaesth. 2021, 127, 110–132. [Google Scholar] [CrossRef]
- Previtali, D.; Andriolo, L.; Di Laura Frattura, G.; Boffa, A.; Candrian, C.; Zaffagnini, S.; Filardo, G. Pain Trajectories in Knee Osteoarthritis—A Systematic Review and Best Evidence Synthesis on Pain Predictors. J. Clin. Med. 2020, 9, 2828. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Tetangco, E.P. Anorectal Disorders: An Update. J. Clin. Gastroenterol. 2020, 54, 606–613. [Google Scholar] [CrossRef]
- Walding, M.F. Pain, anxiety and powerlessness. J. Adv. Nurs. 1991, 16, 388–397. [Google Scholar] [CrossRef]
- Gorczyca, R.; Filip, R.; Walczak, E. Psychological aspects of pain. Ann. Agric. Environ. Med. AAEM 2013, 20, 23–27. [Google Scholar]
- Gan, T.J.; Habib, A.S.; Miller, T.E.; White, W.; Apfelbaum, J.L. Incidence, patient satisfaction, and perceptions of post-surgical pain: Results from a US national survey. Curr. Med. Res. Opin. 2014, 30, 149–160. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linares-Gil, M.J.; Valls, J.; Hereu-Boher, P.; Nebot, F.J.; De-Ramón, B.; Diaz-Munió, E.; Sanzol, R.; De-Oca, J.; Pérez-Lozano, P.; Suñé-Negre, J.M.; et al. Topical Analgesia with Lidocaine Plus Diclofenac Decreases Pain in Benign Anorectal Surgery: Randomized, Double-blind, and Controlled Clinical Trial. Clin. Transl. Gastroenterol. 2018, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Radojčić, M.R.; Arden, N.K.; Yang, X.; Strauss, V.Y.; Birrell, F.; Cooper, C.; Kluzek, S. Pain trajectory defines knee osteoarthritis subgroups: A prospective observational study. Pain 2020, 161, 2841–2851. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Brooks, C., 2nd; Dhruva, S.S.; Lu, Y.; Spatz, E.S.; Dey, P.; Zhang, Y.; Chaudhry, S.I.; Geirsson, A.; Allore, H.G.; et al. Trajectories of Pain After Cardiac Surgery: Implications for Measurement, Reporting, and Individualized Treatment. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007781. [Google Scholar] [CrossRef]
- Gjeilo, K.H.; Oksholm, T.; Follestad, T.; Wahba, A.; Rustøen, T. Trajectories of Pain in Patients Undergoing Lung Cancer Surgery: A Longitudinal Prospective Study. J. Pain Symptom Manag. 2020, 59, 818–828.e811. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency/Average | Percent (%) | ||
|---|---|---|---|
| Age, mean years ±SD | 41.0 ± 12.0 | ||
| Sex | Female | 68 | 31.3 |
| Male | 149 | 68.7 | |
| Height, mean cm ± SD | 168.7 ± 8.8 | ||
| Weight, mean kg ± SD | 70.1 ± 14.0 | ||
| BMI, mean ± SD | 24.5 ± 3.8 | ||
| Marital status | Unmarried | 24 | 11.1 |
| Married | 183 | 84.3 | |
| Divorce | 10 | 4.6 | |
| Type of Surgery | PPH | 126 | 58.1 |
| Fistulectomy | 88 | 40.5 | |
| Fistulotomy | 1 | 0.5 | |
| Seton therapy | 2 | 0.9 | |
| Preoperative anxiety score, mean ± SD | 1.3 ± 0.9 | ||
| Preoperative pain behavior score, mean ± SD | 2.2 ± 1.0 | ||
| Hospital length of stay, mean d ± SD | 4.6 ± 1.8 |
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | BICs (n = 217) | |
|---|---|---|---|---|---|---|
| 2 groups | 0.98 | 0.98 | −4055.30 | |||
| 3 groups | 0.98 | 0.96 | 0.99 | −3825.37 | ||
| 4 groups | 0.96 | 0.98 | 0.91 | 0.97 | −3762.18 | |
| 5 groups | 0.97 | 0.97 | 0.93 | 0.95 | 0.97 | −3706.50 |
| Patient Demographics | Low (n = 50) | Low-Moderate-Low (n = 43) | High-Low (n = 124) | p-Value | |
|---|---|---|---|---|---|
| Age, mean, yr ± SD | 41.8 ± 11.7 | 39.1 ± 11.1 | 41.4 ± 12.4 | 0.402 | |
| Sex | Female | 18 (36%) | 13 (30.2%) | 37 (29.8%) | 0.719 |
| Male | 32 (64%) | 30 (69.8%) | 87 (70.2%) | ||
| BMI, mean ± SD | 25.1 ± 3.7 | 24.8 ± 3.5 | 24.1 ± 3.9 | 0.077 | |
| Type of Surgery | PPH | 25 (50%) | 19 (44.2%) | 82 (66.1%) | 0.018 |
| Fistulectomy | 24 (48%) | 24 (55.8%) | 40 (32.3%) | ||
| Fistulotomy | 0 | 0 | 1 (0.8%) | ||
| Seton therapy | 1 (2%) | 0 | 1 (0.8%) | ||
| Surgeon * | Chief physician | 24 (48%) | 16 (42%) | 48 (41%) | 0.678 |
| Attending physicians | 26 (52%) | 22 (58%) | 70 (59%) | ||
| Preoperative anxiety score, mean ± SD | 0.7 ± 0.5 | 1.0 ± 0.6 | 1.7 ± 0.9 | 0.001 | |
| Preoperative pain behavior score, mean ± SD | 1.9 ± 1.1 | 1.9 ± 1.0 | 2.4 ± 1.0 | 0.005 | |
| Postoperative analgesics, mean, g ± SD | 2.2 ± 0.5 | 2.7 ± 0.5 | 3.2 ± 0.8 | 0.001 | |
| Odds Ratio (95%CI) | ||
|---|---|---|
| Patient Demographics | Low-Moderate-Low | High-Low |
| BMI, kg/cm2 | 0.99 (0.86, 1.14) | 0.95 (0.83, 1.09) |
| Types of Surgery | 6.85 (1.00, 46.93) | 0.15 (0.02, 0.99) |
| Preoperative anxiety score | 1.52 (0.49, 4.73) | 3.26 (1.04, 10.26) |
| Preoperative pain behavior score | 0.47 (0.18, 1.25) | 3.15 (1.23, 8.07) |
| Postoperative analgesics, g | 10.61 (3.37, 33.40) | 12.63 (4.00, 39.90) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Xia, Y.; Yong, Y.; Zhou, Y.; Yin, Z.; Wang, J.; Mei, L.; Song, W.; Wang, J.; Song, J. Pain Trajectory after Short-Stay Anorectal Surgery: A Prospective Observational Study. J. Pers. Med. 2023, 13, 528. https://doi.org/10.3390/jpm13030528
Zhang Y, Xia Y, Yong Y, Zhou Y, Yin Z, Wang J, Mei L, Song W, Wang J, Song J. Pain Trajectory after Short-Stay Anorectal Surgery: A Prospective Observational Study. Journal of Personalized Medicine. 2023; 13(3):528. https://doi.org/10.3390/jpm13030528
Chicago/Turabian StyleZhang, Yujiao, Yangyang Xia, Yue Yong, Yalan Zhou, Zhiyu Yin, Jing Wang, Ling Mei, Wei Song, Jian Wang, and Jiangang Song. 2023. "Pain Trajectory after Short-Stay Anorectal Surgery: A Prospective Observational Study" Journal of Personalized Medicine 13, no. 3: 528. https://doi.org/10.3390/jpm13030528