
Total Cholesterol Variability and the Risk of Osteoporotic Fractures: A Nationwide Population-Based Cohort Study

Abstract
:1. Introduction
2. Methods
2.1. Dataset
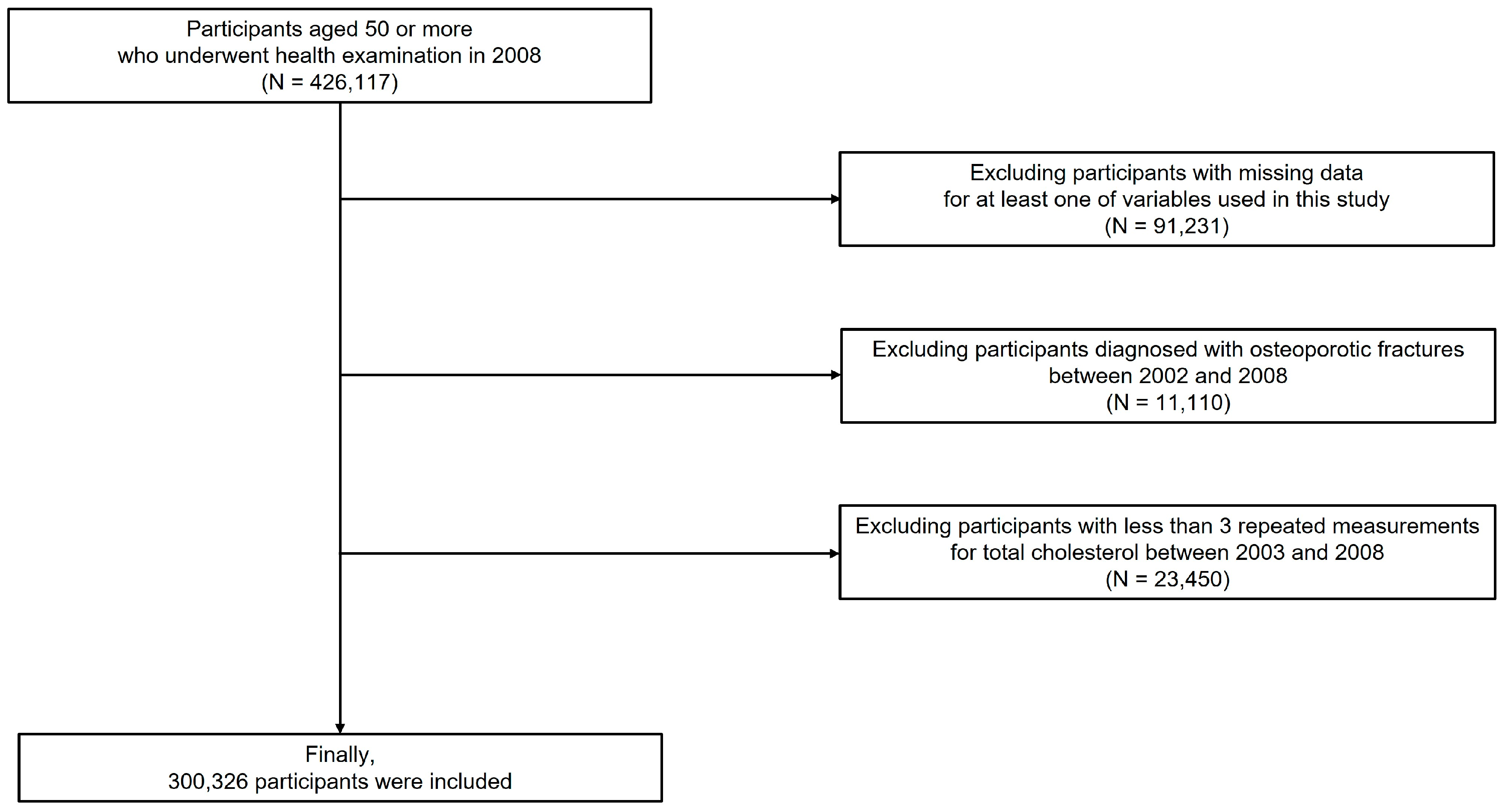
2.2. Study Population
2.3. Assessment of Total Cholesterol Variability
2.4. Study Endpoints
2.5. Variables
2.6. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
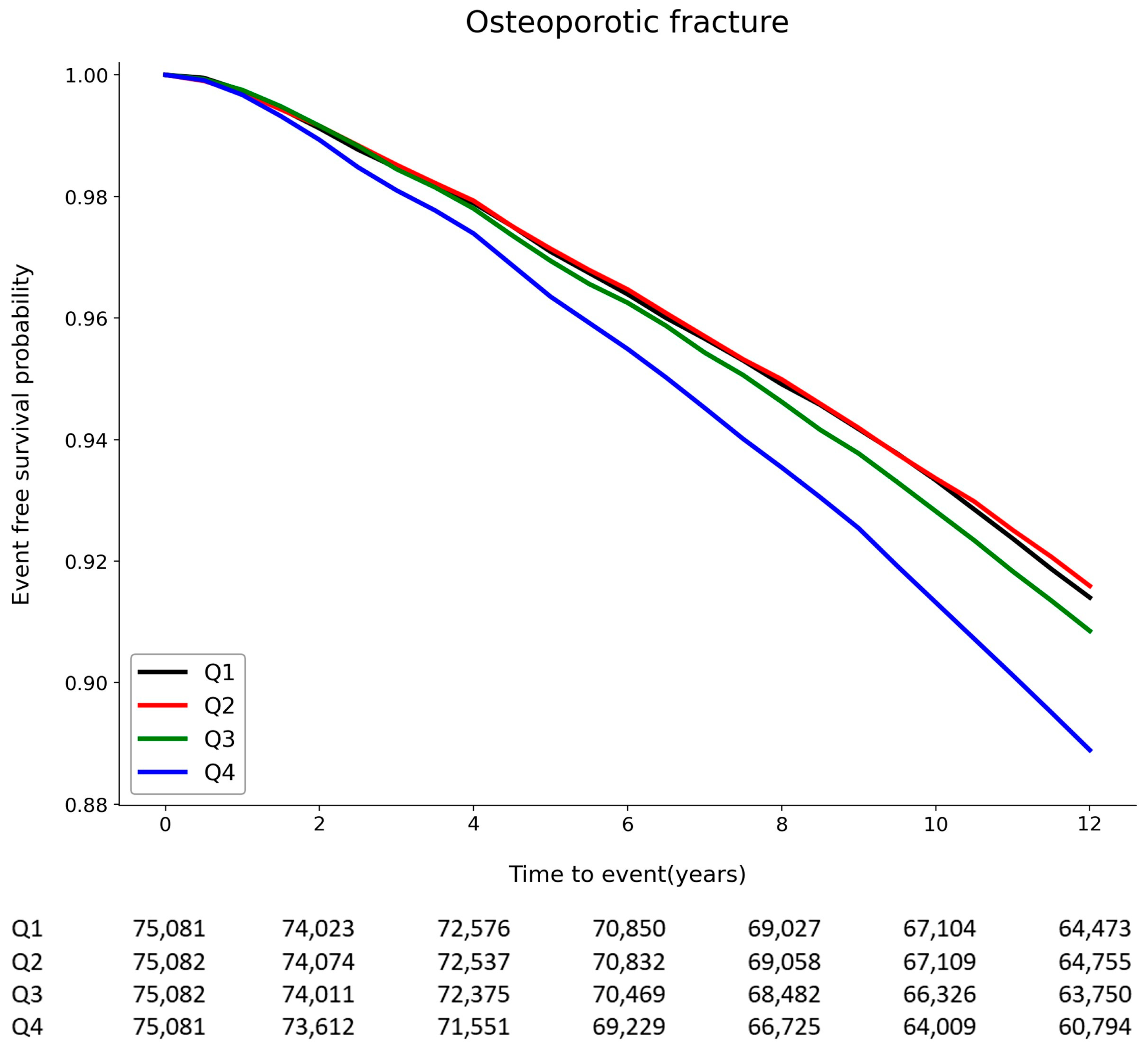
3.2. Association between Total Cholesterol Variability and Osteoporotic Fractures
3.3. Subgroup Analyses
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnell, O.; Kanis, J. Epidemiology of osteoporotic fractures. Osteoporos. Int. 2004, 16, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet 1999, 353, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A.; Odén, A.; Sernbo, I.; Redlund-Johnell, I.; Petterson, C.; De Laet, C.; Jönsson, B. Mortality after osteoporotic fractures. Osteoporos. Int. 2003, 15, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J. Adverse Outcomes of Osteoporotic Fractures in the General Population. J. Bone Miner. Res. 2003, 18, 1139–1141. [Google Scholar] [CrossRef]
- Kanis, J.A. Diagnosis of osteoporosis and assessment of fracture risk. Lancet 2002, 359, 1929–1936. [Google Scholar] [CrossRef]
- Hatzigeorgiou, C.; Jackson, J. Hydroxymethylglutaryl-coenzyme A reductase inhibitors and osteoporosis: A meta-analysis. Osteoporos. Int. 2005, 16, 990–998. [Google Scholar] [CrossRef]
- An, T.; Hao, J.; Sun, S.; Li, R.; Yang, M.; Cheng, G.; Zou, M. Efficacy of statins for osteoporosis: A systematic review and meta-analysis. Osteoporos. Int. 2017, 28, 47–57. [Google Scholar] [CrossRef]
- Uzzan, B.; Cohen, R.; Nicolas, P.; Cucherat, M.; Perret, G.-Y. Effects of statins on bone mineral density: A meta-analysis of clinical studies. Bone 2007, 40, 1581–1587. [Google Scholar] [CrossRef]
- Bookstein, L.; Gidding, S.S.; Donovan, M.; Smith, F.A. Day-to-Day Variability of Serum Cholesterol, Triglyceride, and High-Density Lipoprotein Cholesterol Levels. Arch. Intern. Med. 1990, 150, 1653–1657. [Google Scholar] [CrossRef]
- Kim, M.K.; Han, K.; Park, Y.-M.; Kwon, H.-S.; Kang, G.; Yoon, K.-H.; Lee, S.-H. Associations of Variability in Blood Pressure, Glucose and Cholesterol Concentrations, and Body Mass Index with Mortality and Cardiovascular Outcomes in the General Population. Circulation 2018, 138, 2627–2637. [Google Scholar] [CrossRef]
- Kim, M.K.; Han, K.; Kim, H.-S.; Park, Y.-M.; Kwon, H.-S.; Yoon, K.-H.; Lee, S.-H. Cholesterol variability and the risk of mortality, myocardial infarction, and stroke: A nationwide population-based study. Eur. Hear. J. 2017, 38, 3560–3566. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.; Nicholls, S.J.; John, J.S.; Elshazly, M.B.; Kapadia, S.R.; Tuzcu, E.M.; E Nissen, S.; Puri, R. Visit-to-visit cholesterol variability correlates with coronary atheroma progression and clinical outcomes. Eur. Hear. J. 2018, 39, 2551–2558. [Google Scholar] [CrossRef] [PubMed]
- Bangalore, S.; Breazna, A.; DeMicco, D.A.; Wun, C.-C.; Messerli, F.H. Visit-to-Visit Low-Density Lipoprotein Cholesterol Variability and Risk of Cardiovascular Outcomes. J. Am. Coll. Cardiol. 2015, 65, 1539–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Wang, H.; Liu, F.; Yu, X.; Liang, Y.; Yin, H.; Liu, Y.; Jiang, C.; Wang, Y.; Bai, B. The Effect of Total Cholesterol Variability on Clinical Outcomes After Percutaneous Coronary Intervention. Front. Public Health 2022, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Li, H.; Yuan, J.; Zuo, Y.; Zhang, Y.; Chen, S.; Wu, S.; Wang, Y. Visit-to-Visit Variability of Lipids Measurements and the Risk of Stroke and Stroke Types: A Prospective Cohort Study. J. Stroke 2020, 22, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-H.; Lee, C.-W.; Nam, M.J.; Kim, H.; Kwon, D.-Y.; Yoo, J.W.; Na Lee, K.; Han, K.; Jung, J.-H.; Park, Y.-G.; et al. Association of High-Density Lipoprotein Cholesterol Variability and the Risk of Developing Parkinson Disease. Neurology 2021, 96, e1391–e1401. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Han, K.; Koh, E.S.; Kim, H.-S.; Kwon, H.-S.; Park, Y.-M.; Yoon, K.-H.; Lee, S.-H. Variability in Total Cholesterol Is Associated with the Risk of End-Stage Renal Disease. Arter. Thromb. Vasc. Biol. 2017, 37, 1963–1970. [Google Scholar] [CrossRef] [Green Version]
- Smit, R.A.; Trompet, S.; Sabayan, B.; le Cessie, S.; Van Der Grond, J.; Van Buchem, M.A.; De Craen, A.J.; Jukema, J.W. Higher visit-to-visit low-density lipoprotein cholesterol variability is associated with lower cognitive performance, lower cerebral blood flow, and greater white matter hyperintensity load in older subjects. Circulation 2016, 134, 212–221. [Google Scholar] [CrossRef]
- Parhami, F.; Garfinkel, A.; Demer, L.L. Role of Lipids in Osteoporosis. Arter. Thromb. Vasc. Biol. 2000, 20, 2346–2348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, J.-H.; Park, J.H.; Oh, C.; Chung, J.K.; Song, J.Y.; Kim, S.; Lee, S.-H.; Jang, J.-W.; Kim, Y.-J. Dementia is Associated with an Increased Risk of Hip Fractures: A Nationwide Analysis in Korea. J. Clin. Neurol. 2019, 15, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.-D.; Kang, M.J.; Kim, G.S.; Lee, J.H.; Suh, S.H.; Lee, K.-Y. National Trends in Clinical Outcomes of Endovascular Therapy for Ischemic Stroke in South Korea between 2008 and 2016. J. Stroke 2020, 22, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.-W.; Park, J.H.; Kim, S.; Lee, S.-H.; Lee, S.-H.; Kim, Y.-J. Prevalence and Incidence of Dementia in South Korea: A Nationwide Analysis of the National Health Insurance Service Senior Cohort. J. Clin. Neurol. 2021, 17, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Park, S.-M.; Park, S.Y.; Yoo, J.-I.; Jung, H.-S.; Nho, J.-H.; Kim, S.H.; Lee, Y.-K.; Ha, Y.-C.; Jang, S.; et al. Osteoporosis and Osteoporotic Fracture Fact Sheet in Korea. J. Bone Metab. 2020, 27, 281–290. [Google Scholar] [CrossRef]
- Chang, Y.; Woo, H.G.; Lee, J.S.; Song, T. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 2021, 92, 87–94. [Google Scholar] [CrossRef]
- Woo, H.G.; Chang, Y.; Lee, J.S.; Song, T.-J. Association of Tooth Loss with New-Onset Parkinson’s Disease: A Nationwide Population-Based Cohort Study. Park. Dis. 2020, 2020, 4760512. [Google Scholar] [CrossRef]
- Park, J.-H.; Chang, Y.; Kim, J.-W.; Song, T.-J. Improved Oral Health Status Is Associated with a Lower Risk of Venous Thromboembolism: A Nationwide Cohort Study. J. Pers. Med. 2022, 13, 20. [Google Scholar] [CrossRef]
- Park, J.-H.; Kim, J.-W.; Lee, H.; Hong, I.; Song, T.-J. Better Oral Hygiene Is Associated with a Decreased Risk of Meniere’s Disease: A Nationwide Cohort Study. J. Pers. Med. 2022, 13, 80. [Google Scholar] [CrossRef]
- Sivas, F.; Alemdaroğlu, E.; Elverici, E.; Kuluğ, T.; Özoran, K. Serum lipid profile: Its relationship with osteoporotic vertebrae fractures and bone mineral density in Turkish postmenopausal women. Rheumatol. Int. 2009, 29, 885–890. [Google Scholar] [CrossRef]
- Trimpou, P.; Odén, A.; Simonsson, T.; Wilhelmsen, L.; Landin-Wilhelmsen, K. High serum total cholesterol is a long-term cause of osteoporotic fracture. Osteoporos. Int. 2010, 22, 1615–1620. [Google Scholar] [CrossRef]
- Yamauchi, M.; Yamaguchi, T.; Nawata, K.; Tanaka, K.-I.; Takaoka, S.; Sugimoto, T. Increased low-density lipoprotein cholesterol level is associated with non-vertebral fractures in postmenopausal women. Endocrine 2014, 48, 279–286. [Google Scholar] [CrossRef]
- Wang, Y.; Dai, J.; Zhong, W.; Hu, C.; Lu, S.; Chai, Y. Association between Serum Cholesterol Level and Osteoporotic Fractures. Front. Endocrinol. 2018, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Bagger, Y.Z.; Rasmussen, H.B.; Alexandersen, P.; Werge, T.; Christiansen, C.; Tankó, L.B.; PERF Study Group. Links between cardiovascular disease and osteoporosis in postmenopausal women: Serum lipids or atherosclerosis per se? Osteoporos. Int. 2007, 18, 505–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarlane, S.I.; Muniyappa, R.; Shin, J.J.; Bahtiyar, G.; Sowers, J.R. Osteoporosis and Cardiovascular Disease: Brittle Bones and Boned Arteries, Is There a Link? Endocrine 2004, 23, 1–10. [Google Scholar] [CrossRef]
- Laroche, M.; Pouilles, J.M.; Ribot, C.; Bendayan, P.; Bernard, J.; Boccalon, H.; Mazières, B. Comparison of the bone mineral content of the lower limbs in men with ischaemic atherosclerotic disease. Clin. Rheumatol. 1994, 13, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Värri, M.; Tuomainen, T.-P.; Honkanen, R.; Rikkonen, T.; Niskanen, L.; Kröger, H.; Tuppurainen, M.T. Carotid intima-media thickness and calcification in relation to bone mineral density in postmenopausal women—The OSTPRE-BBA study. Maturitas 2014, 78, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Hmamouchi, I.; Allali, F.; Khazzani, H.; Bennani, L.; El Mansouri, L.; Ichchou, L.; Cherkaoui, M.; Abouqal, R.; Hajjaj-Hassouni, N. Low bone mineral density is related to atherosclerosis in postmenopausal Moroccan women. BMC Public Heal. 2009, 9, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyder, J.A.; Allison, M.; Wong, N.; Papa, A.; Lang, T.; Sirlin, C.; Gapstur, S.M.; Ouyang, P.; Carr, J.; Criqui, M.H. Association of Coronary Artery and Aortic Calcium with Lumbar Bone Density: The MESA Abdominal Aortic Calcium Study. Am. J. Epidemiology 2009, 169, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tankó, L.B.; Christiansen, C.; Cox, D.A.; Geiger, M.J.; McNabb, M.A.; Cummings, S.R. Relationship Between Osteoporosis and Cardiovascular Disease in Postmenopausal Women. J. Bone Miner. Res. 2005, 20, 1912–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsartsalis, A.; Dokos, C.; Kaiafa, G.; Tsartsalis, D.; Kattamis, A.; Hatzitolios, A.; Savopoulos, C. Statins, bone formation and osteoporosis: Hope or hype? Hormones 2012, 11, 126–139. [Google Scholar] [CrossRef]
- Mundy, G.; Garrett, R.; Harris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of bone formation in vitro and in rodents by statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef]
- Chen, H.; Ren, J.-Y.; Xing, Y.; Zhang, W.-L.; Liu, X.; Wu, P.; Wang, R.-J.; Luo, Y. Short-term withdrawal of simvastatin induces endothelial dysfunction in patients with coronary artery disease: A dose–response effect dependent on endothelial nitric oxide synthase. Int. J. Cardiol. 2009, 131, 313–320. [Google Scholar] [CrossRef]
- Roh, E.; Chung, H.S.; Lee, J.S.; Kim, J.A.; Lee, Y.-B.; Hong, S.-H.; Kim, N.H.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; et al. Total cholesterol variability and risk of atrial fibrillation: A nationwide population-based cohort study. PLoS ONE 2019, 14, e0215687. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Lee, J.S.; Kim, J.A.; Roh, E.; Bin Lee, Y.; Hong, S.H.; Kim, N.H.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; et al. Variability in total cholesterol concentration is associated with the risk of dementia: A nationwide population-based cohort study. Front. Neurol. 2019, 10, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Han, K.; Cho, H.; Park, Y.M.; Kwon, H.S.; Kang, G.; Yoon, K.H.; Kim, M.K. Variability in metabolic parameters and risk of dementia: A nationwide population-based study 11 Medical and Health Sciences 1117 Public Health and Health Services. Alzheimers. Res. Ther. 2018, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.R.; Seo, M.H.; Han, K.D.; Jung, J.; Hwang, I.C. Waist circumference and risk of 23 site-specific cancers: A population-based cohort study of Korean adults. Br. J. Cancer 2018, 119, 1018–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.G.; Han, K.-D.; Kim, D.Y.; Choi, Y.Y.; Choi, H.Y.; Roh, S.-Y.; Shim, J.; Kim, J.S.; Choi, J.-I.; Kim, Y.-H. Different Influence of Blood Pressure on New-Onset Atrial Fibrillation in Pre- and Postmenopausal Women. Hypertension 2021, 77, 1500–1509. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total | Q1 | Q2 | Q3 | Q4 | p-Value |
|---|---|---|---|---|---|---|
| Number of participants (%) | 300,326 | 75,081 (25.0) | 75,082 (25.0) | 75,082 (25.0) | 75,081 (25.0) | |
| Age, years | 56.25 ± 5.92 | 56.17 ± 5.89 | 55.75 ± 5.57 | 55.98 ± 5.69 | 57.11 ± 6.41 | <0.001 |
| Sex | <0.001 | |||||
| Male | 221,339 (73.7) | 57,057 (76.0) | 57,313 (76.3) | 55,397 (73.8) | 51,572 (68.7) | |
| Female | 78,987 (26.3) | 18,024 (24.0) | 17,769 (23.7) | 19,685 (26.2) | 23,509 (31.3) | |
| Body mass index (kg/m2) | 23.98 ± 2.76 | 23.93 ± 2.73 | 23.91 ± 2.72 | 23.94 ± 2.75 | 24.13 ± 2.85 | <0.001 |
| Household income | <0.001 | |||||
| Q1, lowest | 80,324 (26.7) | 18,443 (24.6) | 18,554 (24.7) | 20,248 (27.0) | 23,079 (30.7) | |
| Q2 | 83,315 (27.7) | 19,805 (26.4) | 20,194 (26.9) | 21,123 (28.1) | 22,193 (29.6) | |
| Q3 | 71,441 (23.8) | 18,058 (24.1) | 18,121 (24.1) | 17,934 (23.9) | 17,328 (23.1) | |
| Q4, highest | 65,246 (21.7) | 18,775 (25.0) | 18,213 (24.3) | 15,777 (21.0) | 12,481 (16.6) | |
| Smoking status | <0.001 | |||||
| Never | 179,488 (59.8) | 43,722 (58.2) | 43,499 (57.9) | 45,013 (60.0) | 47,254 (62.9) | |
| Former | 47,434 (15.8) | 12,676 (16.9) | 12,429 (16.6) | 11,625 (15.5) | 10,704 (14.3) | |
| Current | 73,404 (24.4) | 18,683 (24.9) | 19,154 (25.5) | 18,444 (24.6) | 17,123 (22.8) | |
| Alcohol consumption (days/week) | <0.001 | |||||
| None | 200,543 (66.8) | 49,662 (66.1) | 49,269 (65.6) | 49,959 (66.5) | 51,653 (68.8) | |
| 1–4 | 90,419 (30.1) | 23,267 (31.0) | 23,667 (31.5) | 22,802 (30.4) | 20,683 (27.6) | |
| ≥5 | 9364 (3.1) | 2152 (2.9) | 2146 (2.9) | 2321 (3.1) | 2745 (3.7) | |
| Regular physical activity (days/week) | <0.001 | |||||
| None | 121,585 (40.5) | 29,165 (38.8) | 29,600 (39.4) | 30,347 (40.4) | 32,473 (43.3) | |
| 1–4 | 150,934 (50.3) | 39,025 (52.0) | 38,734 (51.6) | 37,922 (50.5) | 35,253 (47.0) | |
| ≥5 | 27,807 (9.3) | 6891 (9.2) | 6748 (9.0) | 6813 (9.1) | 7355 (9.8) | |
| Comorbidities | ||||||
| Hypertension | 114,971 (38.3) | 25,271 (33.7) | 25,546 (34.0) | 27,677 (36.9) | 36,477 (48.6) | <0.001 |
| Diabetes mellitus | 58,940 (19.6) | 11,809 (15.7) | 12,276 (16.4) | 13,823 (18.4) | 21,032 (28.0) | <0.001 |
| Dyslipidemia | 93,928 (31.3) | 16,905 (22.5) | 18,251 (24.3) | 22,175 (29.5) | 36,597 (48.7) | <0.001 |
| Stroke | 7880 (2.6) | 1479 (2.0) | 1487 (2.0) | 1778 (2.4) | 3136 (4.2) | <0.001 |
| Atrial fibrillation | 2739 (0.9) | 555 (0.7) | 521 (0.7) | 618 (0.8) | 1045 (1.4) | <0.001 |
| Renal disease | 7700 (2.6) | 1386 (1.9) | 1445 (1.9) | 1707 (2.3) | 3162 (4.2) | <0.001 |
| Cancer | 13,489 (4.5) | 2942 (3.9) | 3072 (4.1) | 3305 (4.4) | 4170 (5.6) | <0.001 |
| On lipid-lowering agents | 29,287 (9.8) | 5410 (7.2) | 5658 (7.5) | 6874 (9.2) | 11,345 (15.1) | <0.001 |
| Mean TC (mg/dL) | 198.66 ± 31.16 | 199.22 ± 28.61 | 198.02 ± 28.52 | 197.56 ± 29.09 | 199.84 ± 37.44 | <0.001 |
| TC variability | ||||||
| CV (%) | 10.11 ± 6.13 | 4.8 ± 1.3 | 7.81 ± 0.72 | 10.56 ± 0.93 | 17.28 ± 7.89 | <0.001 |
| SD | 20.41 ± 23.66 | 9.57 ± 2.94 | 15.54 ± 2.65 | 20.89 ± 3.59 | 35.71 ± 42.84 | <0.001 |
| VIM (%) | 21.22 ± 22.53 | 9.46 ± 2.86 | 15.45 ± 2.54 | 20.85± 3.51 | 35.68 ± 42.79 | <0.001 |
| Multivariable Model (1) | Multivariable Model (2) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Participants | Number of Events | Event Rate (%) (95% CI) | Person-Years | Incidence Rate (Per 1000 Person-Years) | Adjusted HR (95% CI) | p-Value | p-Value for Trend | Adjusted HR (95% CI) | p-Value | p-Value for Trend | |
| CV | <0.001 | <0.001 | |||||||||
| Q1 | 75,081 | 6704 | 8.93 (8.72, 9.14) | 874,299.98 | 7.67 | 1 (reference) | 1 (reference) | ||||
| Q2 | 75,082 | 6603 | 8.79 (8.58, 9.01) | 874,827.89 | 7.55 | 1.02 (0.99, 1.06) | 0.230 | 1.02 (0.99, 1.05) | 0.282 | ||
| Q3 | 75,082 | 7121 | 9.48 (9.26, 9.70) | 869,543.07 | 8.19 | 1.06 (1.03, 1.10) | <0.001 | 1.06 (1.02, 1.09) | 0.001 | ||
| Q4 | 75,081 | 8616 | 11.48 (11.23, 11.72) | 852,157.80 | 10.11 | 1.11 (1.08, 1.15) | <0.001 | 1.10 (1.07, 1.14) | <0.001 | ||
| SD | <0.001 | <0.001 | |||||||||
| Q1 | 75,095 | 6767 | 9.01 (8.80, 9.23) | 872,764.30 | 7.75 | 1 (reference) | 1 (reference) | ||||
| Q2 | 75,062 | 6522 | 8.69 (8.48, 8.90) | 874,326.38 | 7.46 | 0.99 (0.95, 1.02) | 0.459 | 0.99 (0.96, 1.03) | 0.724 | ||
| Q3 | 75,087 | 7117 | 9.48 (9.26, 9.70) | 869,819.28 | 8.18 | 1.03 (0.99, 1.06) | 0.153 | 1.04 (1.00, 1.07) | 0.027 | ||
| Q4 | 75,082 | 8638 | 11.50 (11.26, 11.75) | 853,918.79 | 10.12 | 1.07 (1.04, 1.11) | <0.001 | 1.10 (1.06, 1.13) | <0.001 | ||
| VIM | <0.001 | <0.001 | |||||||||
| Q1 | 75,081 | 6767 | 9.01 (8.80, 9.23) | 872,602.28 | 7.75 | 1 (reference) | 1 (reference) | ||||
| Q2 | 75,082 | 6522 | 8.69 (8.48, 8.90) | 874,563.86 | 7.46 | 0.99 (0.95, 1.02) | 0.444 | 0.99 (0.96, 1.03) | 0.704 | ||
| Q3 | 75,082 | 7117 | 9.48 (9.26, 9.70) | 869,749.16 | 8.18 | 1.03 (0.99, 1.06) | 0.156 | 1.04 (1.00, 1.07) | 0.027 | ||
| Q4 | 75,081 | 8638 | 11.50 (11.26, 11.75) | 853,913.44 | 10.12 | 1.07 (1.04, 1.11) | <0.001 | 1.10 (1.06, 1.13) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Kim, J.H.; Song, T.-J. Total Cholesterol Variability and the Risk of Osteoporotic Fractures: A Nationwide Population-Based Cohort Study. J. Pers. Med. 2023, 13, 509. https://doi.org/10.3390/jpm13030509
Kim D, Kim JH, Song T-J. Total Cholesterol Variability and the Risk of Osteoporotic Fractures: A Nationwide Population-Based Cohort Study. Journal of Personalized Medicine. 2023; 13(3):509. https://doi.org/10.3390/jpm13030509
Chicago/Turabian StyleKim, Dongyeop, Jee Hyun Kim, and Tae-Jin Song. 2023. "Total Cholesterol Variability and the Risk of Osteoporotic Fractures: A Nationwide Population-Based Cohort Study" Journal of Personalized Medicine 13, no. 3: 509. https://doi.org/10.3390/jpm13030509