
Finite Element Analysis of Channel Screw and Conventional Plate Technique in Tile B2 Pelvic Fracture
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Equipment and Design Principles
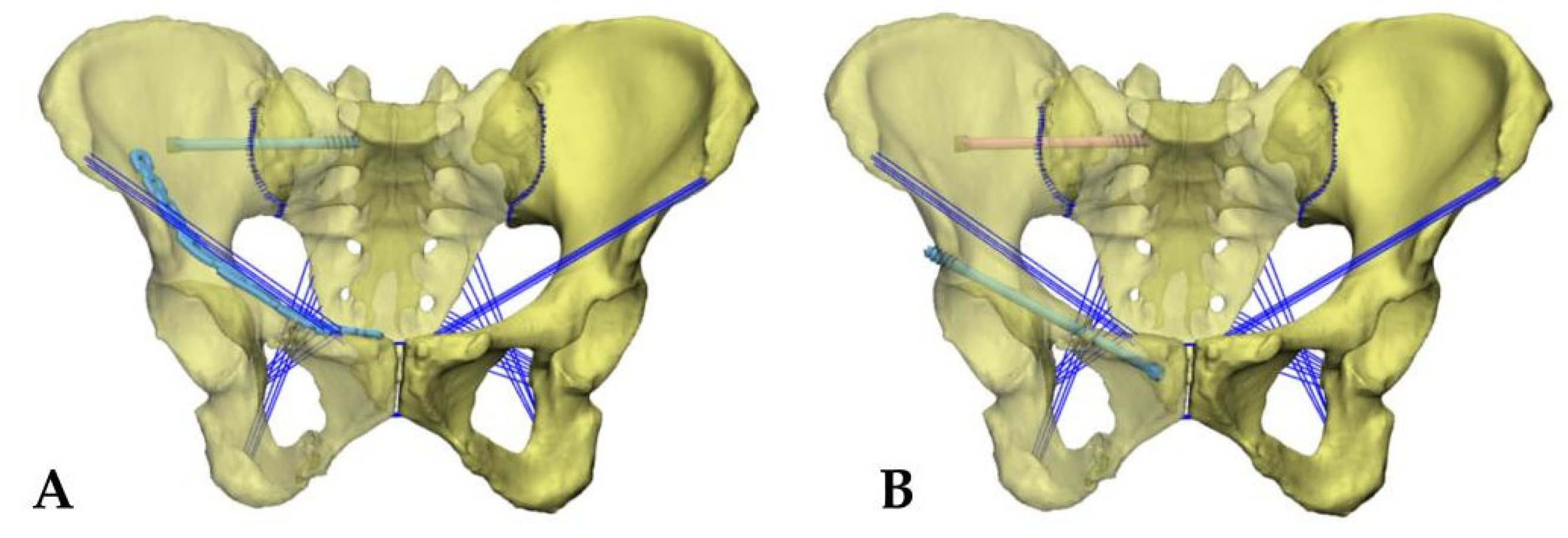
2.2. Simulation of Two Types of Surgical Fixation Models
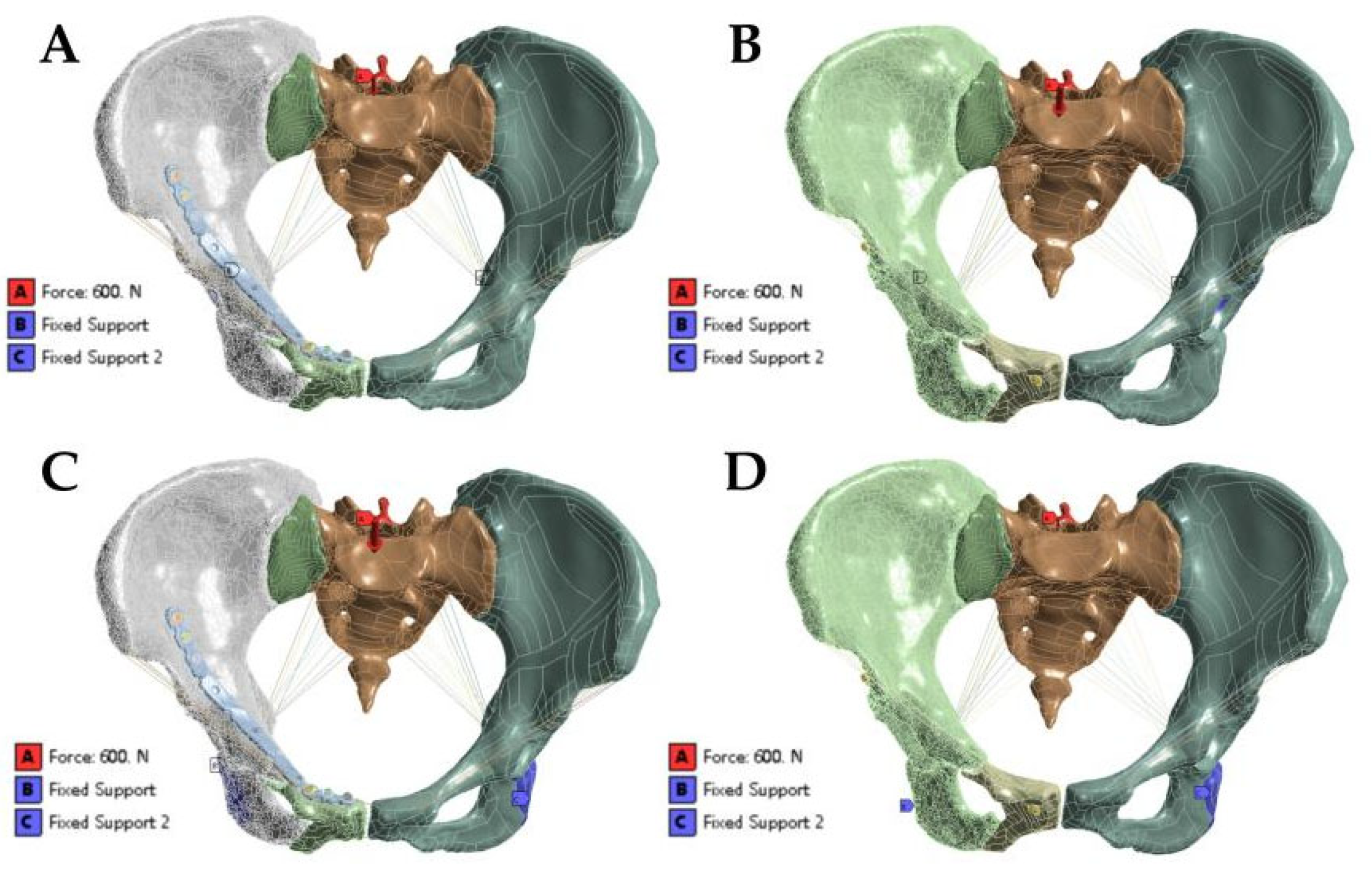
2.3. Loads and Boundary Conditions
3. Results
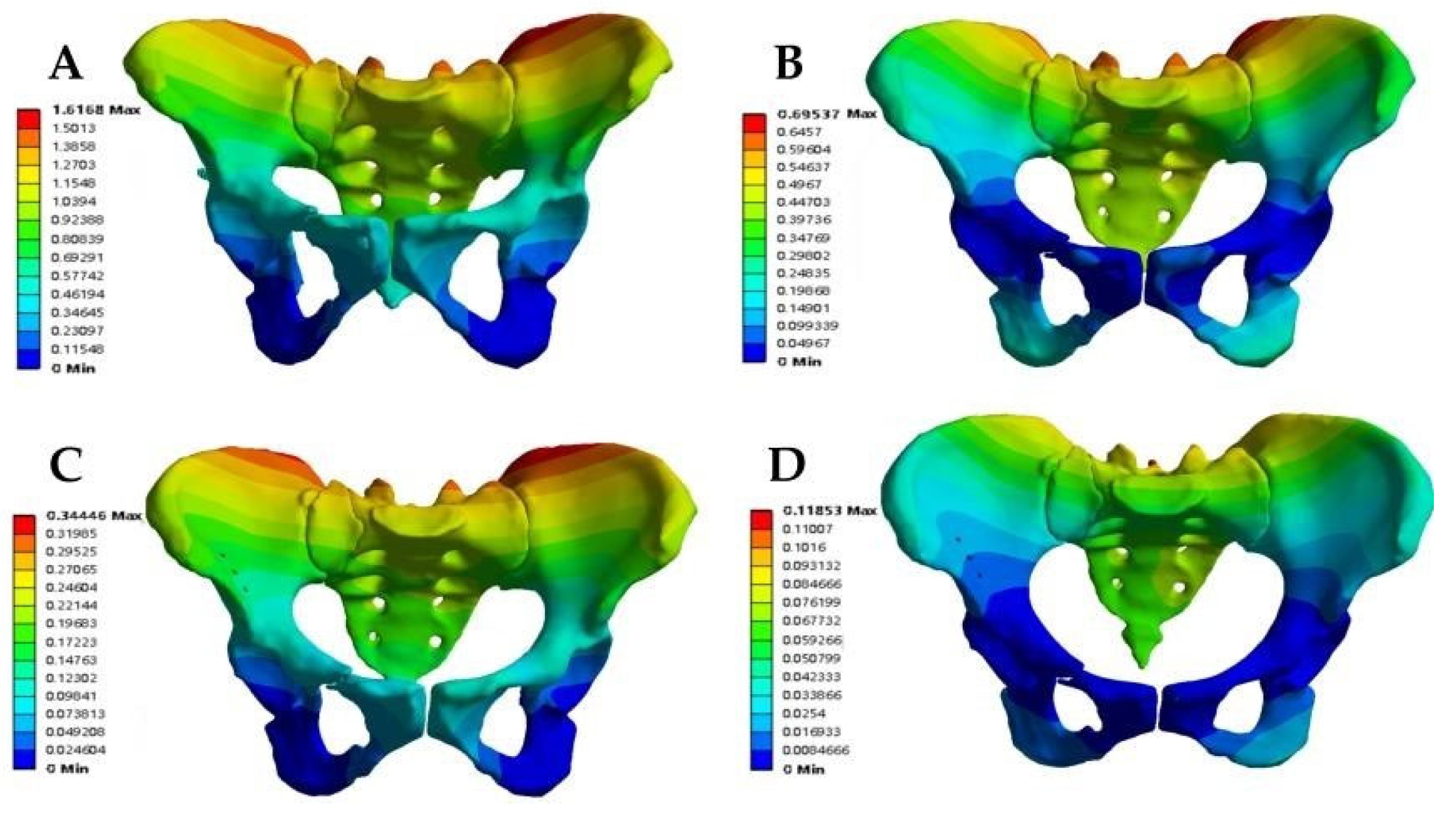
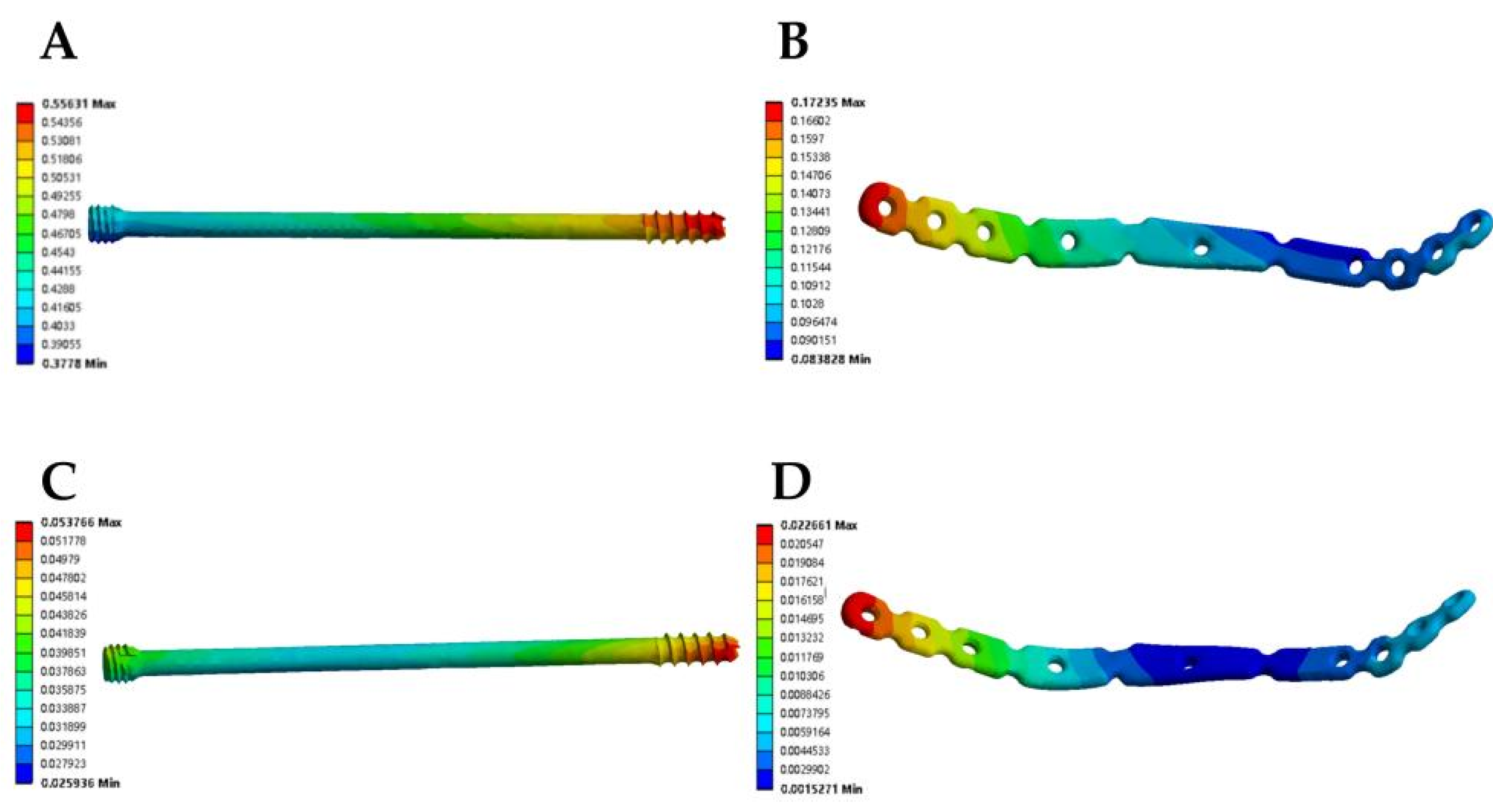
3.1. Displacement Analysis of the Fracture Fixation Model
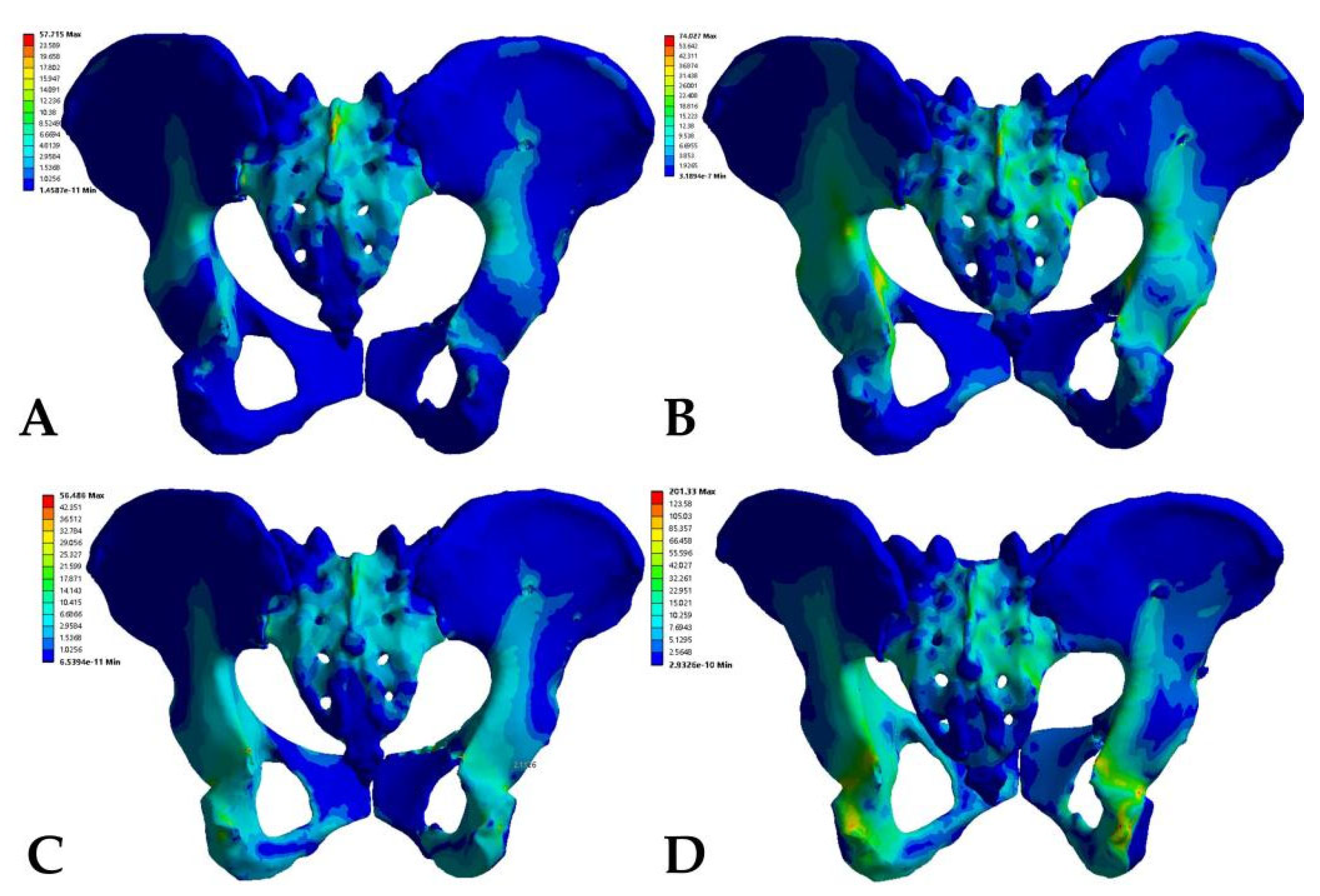
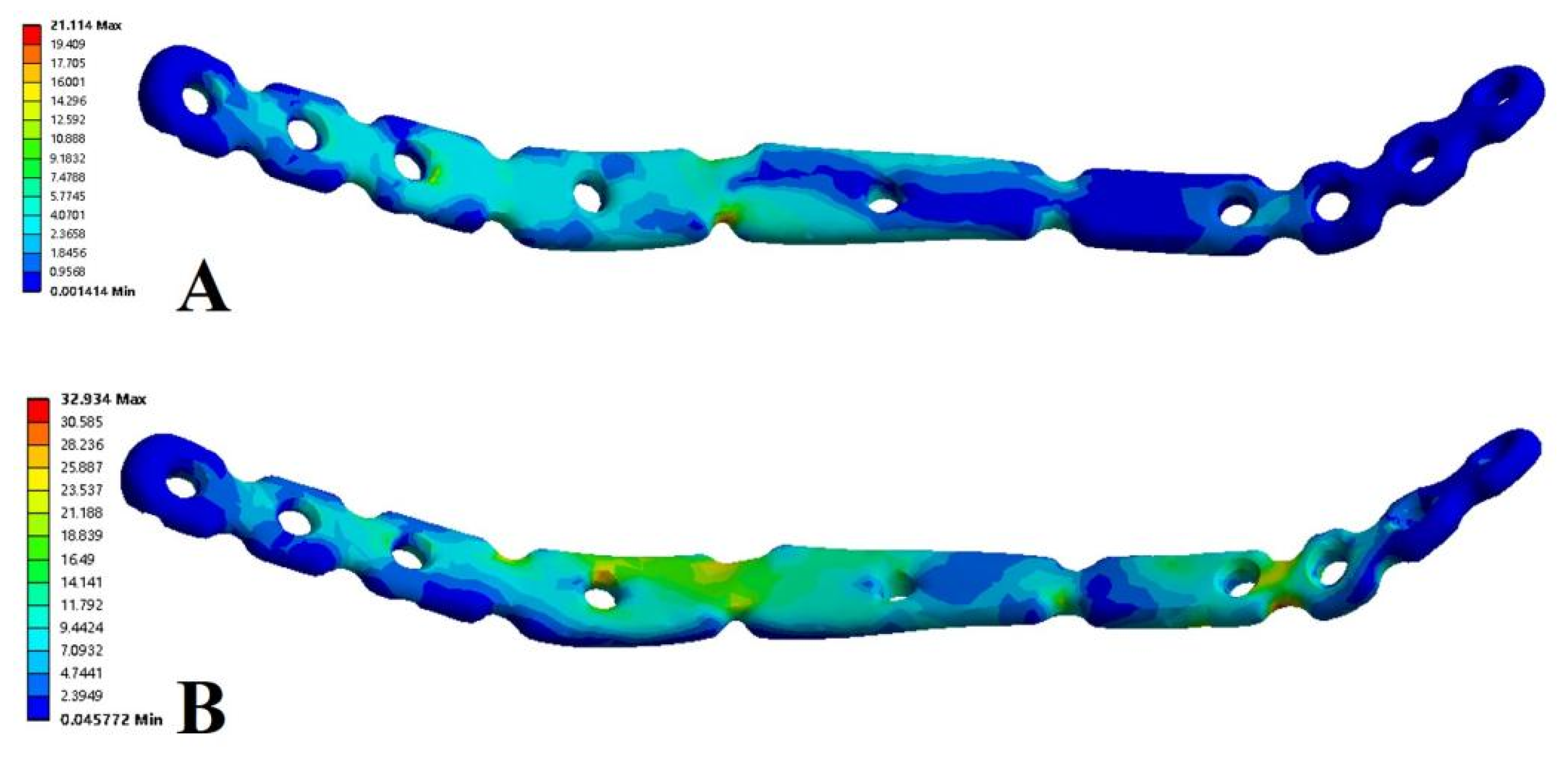
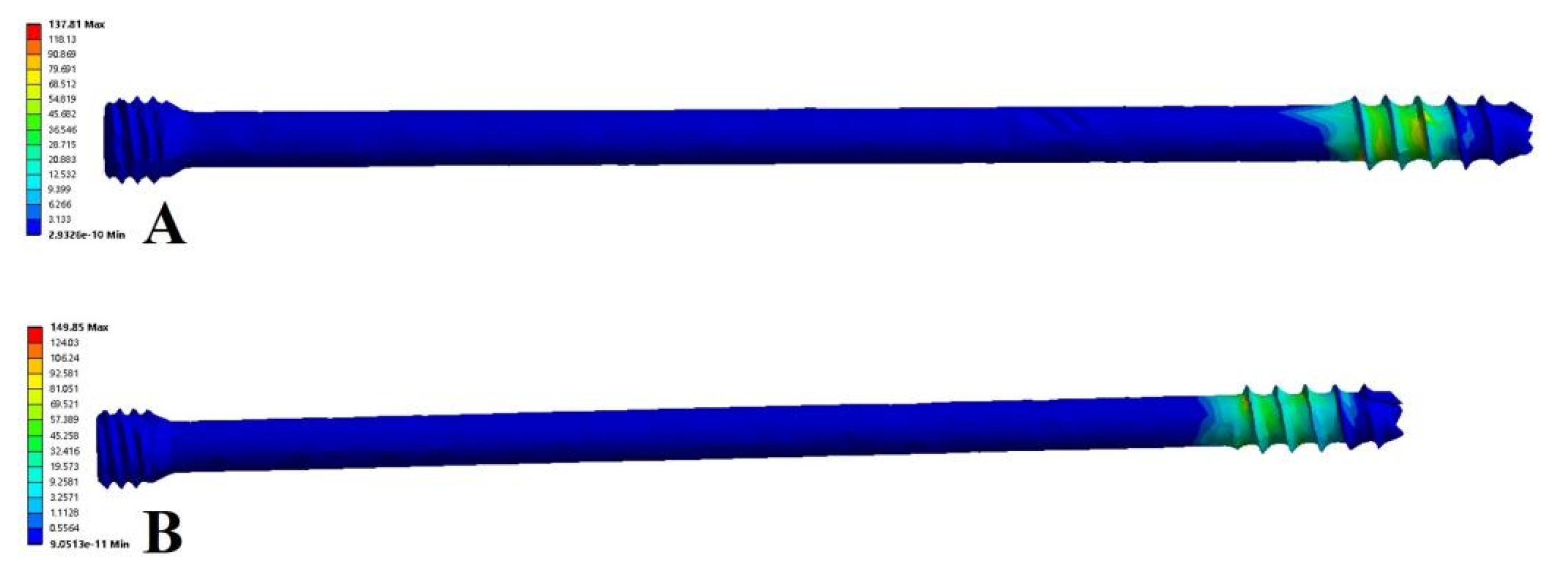
3.2. Stress Analysis of the Fracture Fixation Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villiger, K.; Meier, M.K.; Hasler, R.M.; Bastian, J.D.; Tannast, M.; Exadaktylos, A.K.; Steppacher, S.D. Demographic changes in pelvic fracture patterns at a Swiss academic trauma center from 2007 to 2017. J. Trauma Acute Care Surg. 2022, 92, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Höch, A.; Society, P.I.R.O.T.G.T.; Pieroh, P.; Gras, F.; Hohmann, T.; Märdian, S.; Holmenschlager, F.; Keil, H.; Palm, H.-G.; Herath, S.C.; et al. Age and “general health”—Beside fracture classification—Affect the therapeutic decision for geriatric pelvic ring fractures: A German pelvic injury register study. Int. Orthop. 2019, 43, 2629–2636. [Google Scholar] [CrossRef] [PubMed]
- Osterhoff, G.; Ossendorf, C.; Wanner, G.A.; Simmen, H.-P.; Werner, C.M. Posterior screw fixation in rotationally unstable pelvic ring injuries. Injury 2011, 42, 992–996. [Google Scholar] [CrossRef]
- Hua, X.; Yan, S.G.; Cui, Y.; Yin, Z.; Schreiner, A.J.; Schmidutz, F. Minimally invasive internal fixator for unstable pelvic ring injuries with a pedicle screw–rod system: A retrospective study of 23 patients after 13.5 months. Arch. Orthop. Trauma Surg. 2019, 139, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Jäckle, K.; Spering, C.; Seitz, M.-T.; Höller, S.; Meier, M.-P.; Hahn, F.M.; Acharya, M.R.; Lehmann, W. Correction to: Anatomic reduction of the sacroiliac joint in unstable pelvic ring injuries and its correlation with functional outcome. Eur. J. Trauma Emerg. Surg. 2022, 48, 1499. [Google Scholar] [CrossRef]
- Liu, L.; Fan, S.; Zeng, D.; Chen, Y.; Song, H.; Zeng, L.; Jin, D. Clinical application of anterior ring internal fixator system combined with sacroiliac screw fixation in Tile C pelvic fracture treatment. J. Orthop. Surg. Res. 2021, 16, 715. [Google Scholar] [CrossRef]
- Ellis, J.D.M.; Shah, N.S.M.; Archdeacon, M.T.M.; Sagi, H.C.M. Anterior Pelvic Ring Fracture Pattern Predicts Subsequent Displacement in Lateral Compression Sacral Fractures. J. Orthop. Trauma 2022, 36, 550–556. [Google Scholar] [CrossRef]
- Yu, X.; Tang, M.; Zhou, Z.; Peng, X.; Wu, T.; Sun, Y. Minimally invasive treatment for pubic ramus fractures combined with a sacroiliac joint complex injury. Int. Orthop. 2013, 37, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Rommens, P.M.; Wagner, D.; Arand, C.; Boudissa, M.; Hopf, J.; Hofmann, A. Minimally invasive stabilization of fragility fractures of the pelvis with transsacral bar and retrograde transpubic screw. Oper. Orthop. Traumatol. 2022, 34, 153–171. [Google Scholar] [CrossRef]
- Phillips, A.T.M.; Pankaj, P.; Howie, C.R.; Usmani, A.S.; Simpson, A.H.R.W. Finite element modelling of the pelvis: Inclusion of muscular and ligamentous boundary conditions. Med. Eng. Phys. 2007, 29, 739–748. [Google Scholar] [CrossRef]
- Sohn, S.; Park, T.H.; Chung, C.K.; Kim, Y.J.; Jang, J.W.; Han, I.-B.; Lee, S.J. Biomechanical characterization of three iliac screw fixation techniques: A finite element study. J. Clin. Neurosci. 2018, 52, 109–114. [Google Scholar] [CrossRef]
- Li, L.; Lu, J.; Yang, L.; Zhang, K.; Jin, J.; Sun, G.; Wang, X.; Jiang, Q. Stability evaluation of anterior external fixation in patient with unstable pelvic ring fracture: A finite element analysis. Ann. Transl. Med. 2019, 7, 303. [Google Scholar] [CrossRef]
- van Vugt, A.B.; van Kampen, A. An unstable pelvic ring: The killing fracture. J. Bone Joint Surg. Br. 2006, 88, 427–433. [Google Scholar] [CrossRef]
- Li, P.; Liu, F.; Li, Q.; Zhou, D.; Dong, J.; Wang, D. Role of pelvic packing in the first attention given to hemodynamically unstable pelvic fracture patients: A meta-analysis. J. Orthop. Traumatol. 2022, 23, 29. [Google Scholar] [CrossRef]
- Wakayama, Y.; Higashi, T.; Kobayashi, N.; Choe, H.; Matsumoto, M.; Abe, T.; Takeuchi, I.; Inaba, Y. Clinical utility of minimally invasive posterior internal fixation within the pelvic ring using S2 alar iliac screws for unstable pelvic ring fracture. Injury 2022, 53, 3371–3376. [Google Scholar] [CrossRef]
- Herteleer, M.; Boudissa, M.; Hofmann, A.; Wagner, D.; Rommens, P.M. Plate fixation of the anterior pelvic ring in patients with fragility fractures of the pelvis. Eur. J. Trauma Emerg. Surg. 2022, 48, 3711–3719. [Google Scholar] [CrossRef]
- Cole, P.A.; Dyskin, E.A.; Gilbertson, J.A. Minimally-invasive fixation for anterior pelvic ring disruptions. Injury 2015, 46 (Suppl. 3), S27–S34. [Google Scholar] [CrossRef]
- Ge, S.; Zhang, L.; Zhou, Z.; Jia, S.; Zheng, L. TiRobot-assisted surgery by O-arm navigation system for percutaneous minimally invasive treatment of posterior pelvic ring injury. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2022, 36, 934–939. [Google Scholar]
- Lu, S.; Yang, K.; Lu, C.; Wei, P.; Gan, Z.; Zhu, Z.; Tan, H. O-arm navigation for sacroiliac screw placement in the treatment for posterior pelvic ring injury. Int. Orthop. 2021, 45, 1803–1810. [Google Scholar] [CrossRef]
- Maslov, L.B.; Dmitryuk, A.Y.; Zhmaylo, M.A.; Tarasenko, F.D.; Kovalenko, A.N. Strength analysis in a hip endoprosthesis made of polymeric material. Russ. J. Biomech. 2022, 4, 14–28. [Google Scholar]
- Borovkov, A.I.; Maslov, L.B.; Zhmaylo, M.A.; Zelinskiy, I.A.; Voinov, I.B.; Keresten, I.A.; Mamchits, D.V.; Tikhilov, R.M.; Kovalenko, A.N.; Bilyk, S.S.; et al. Finite element stress analysis of a total hip replacement in two-legged standing. Russ. J. Biomech. 2018, 22, 382–400. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area and Material | Young’s Modulus (MPa) | Poisson’s Ratio |
|---|---|---|
| Sacrum cortical | 17,000 | 0.3 |
| Sacrum cancellous | 150 | 0.2 |
| Ilium cortical | 17,000 | 0.3 |
| Ilium cancellous | 150 | 0.2 |
| Ligament | Stiffness Coefficient (N/mm) | Ligament |
|---|---|---|
| Sacroiliac | 5000 | Sacroiliac |
| Sacrospinous | 1500 | Sacrospinous |
| Sacrotuberous | 1500 | Sacrotuberous |
| Inguinal | 250 | Inguinal |
| Superior pubic | 500 | Superior pubic |
| Arcuate pubic | 500 | Arcuate pubic |
| Model | Pelvis MD (mm) | Anterior Ring Implants MD (mm) |
|---|---|---|
| anterior ring hollow compression screw (sitting) | 1616.80 × 10−3 | 556.31 × 10−3 |
| anterior ring anterior ring plate (sitting) | 344.46 × 10−3 | 172.35 × 10−3 |
| anterior ring hollow compression screw (standing) | 695.37 × 10−3 | 53.77 × 10−3 |
| anterior ring anterior ring plate (standing) | 118.53 × 10−3 | 22.66 × 10−3 |
| Model | Pelvis MS (MPa) | Anterior Ring Implants MS (MPa) |
|---|---|---|
| anterior ring hollow compression screw (sitting) | 201.33 | 149.85 |
| anterior ring anterior ring plate (sitting) | 56.49 | 32.93 |
| anterior ring hollow compression screw (standing) | 74.03 | 137.81 |
| anterior ring anterior ring plate (standing) | 57.72 | 21.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Ren, H.; Zhang, X.; Ao, R.; Yi, C.; Yu, B. Finite Element Analysis of Channel Screw and Conventional Plate Technique in Tile B2 Pelvic Fracture. J. Pers. Med. 2023, 13, 506. https://doi.org/10.3390/jpm13030506
Li D, Ren H, Zhang X, Ao R, Yi C, Yu B. Finite Element Analysis of Channel Screw and Conventional Plate Technique in Tile B2 Pelvic Fracture. Journal of Personalized Medicine. 2023; 13(3):506. https://doi.org/10.3390/jpm13030506
Chicago/Turabian StyleLi, Dejian, Hanru Ren, Xu Zhang, Rongguang Ao, Chengqing Yi, and Baoqing Yu. 2023. "Finite Element Analysis of Channel Screw and Conventional Plate Technique in Tile B2 Pelvic Fracture" Journal of Personalized Medicine 13, no. 3: 506. https://doi.org/10.3390/jpm13030506