
High Homocysteine Levels Are Associated with Cognitive Impairment in Patients Who Recovered from COVID-19 in the Long Term

Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Hematological Analysis
Homocysteine
2.3. Data Collection Tools
2.3.1. Beck Depression Inventory (BDI)
2.3.2. Montreal Cognitive Assessment (MoCA)
2.4. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 1 February 2023).
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Monje, M.; Iwasaki, A. The neurobiology of long COVID. Neuron 2022, 110, 3484–3496. [Google Scholar] [CrossRef]
- Finkelstein, J.D.; Martin, J.J. Homocysteine. Int. J. Biochem. Cell Biol. 2000, 32, 385–389. [Google Scholar] [CrossRef]
- Carpenè, G.; Negrini, D.; Henry, B.M.; Montagnana, M.; Lippi, G. Homocysteine in coronavirus disease (COVID-19): A systematic literature review. Diagnosis 2022, 9, 306–310. [Google Scholar] [CrossRef]
- Baszczuk, A.; Kopczyński, Z. Hyperhomocysteinemia in patients with cardiovascular disease. Postepy Hig. Med. Dosw. 2014, 68, 579–589. [Google Scholar] [CrossRef]
- Tawfik, A.; Elsherbiny, N.M.; Zaidi, Y.; Rajpurohit, P. Homocysteine and Age-Related Central Nervous System Diseases: Role of Inflammation. Int. J. Mol. Sci. 2021, 22, 6259. [Google Scholar] [CrossRef]
- Folstein, M.; Liu, T.; Peter, I.; Buell, J.; Arsenault, L.; Scott, T.; Qiu, W.W. The homocysteine hypothesis of depression. Am. J. Psychiatry 2007, 164, 861–867. [Google Scholar] [CrossRef]
- Setién-Suero, E.; Suárez-Pinilla, M.; Suárez-Pinilla, P.; Crespo-Facorro, B.; Ayesa-Arriola, R. Homocysteine and cognition: A systematic review of 111 studies. Neurosci. Biobehav. Rev. 2016, 69, 280–298. [Google Scholar] [CrossRef] [Green Version]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Inoue, S.; Hatakeyama, J.; Kondo, Y.; Hifumi, T.; Sakuramoto, H.; Kawasaki, T.; Taito, S.; Nakamura, K.; Unoki, T.; Kawai, Y.; et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Med. Surg. 2019, 6, 233–246. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; You, D.; Wang, H.; Yang, Y.; Zhang, D.; Lv, J.; Luo, S.; Liao, R.; Ma, L. Association between homocysteine and obesity: A meta-analysis. J. Evid. Based Med. 2021, 14, 208–217. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Hisli, N. Beck Depresyon Envanteri’nin üniversite öğrencileri için geçerliği, güvenirliği. Psikoloji Dergisi. 1989, 7, 3–13. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Selekler, K.; Cangöz, B.; Uluç, S. Power of discrimination of Montreal Cognitive Assessment (MOCA) scale in Turkish patients with mild cognitive impairement and Alzheimer’s disease. Turk. Geriatri. Derg. 2010, 13, 166–171. [Google Scholar]
- Ponti, G.; Roli, L.; Oliva, G.; Manfredini, M.; Trenti, T.; Kaleci, S.; Iannella, R.; Balzano, B.; Coppola, A.; Fiorentino, G.; et al. Homocysteine (Hcy) assessment to predict outcomes of hospitalized COVID-19 patients: A multicenter study on 313 COVID-19 patients. Clin. Chem. Lab. Med. 2021, 59, e354–e357. [Google Scholar] [CrossRef]
- Ponti, G.; Ruini, C.; Tomasi, A. Homocysteine as a potential predictor of cardiovascular risk in patients with COVID-19. Med. Hypotheses. 2020, 143, 109859. [Google Scholar] [CrossRef]
- Previtali, E.; Bucciarelli, P.; Passamonti, S.M.; Martinelli, I. Risk factors for venous and arterial thrombosis. Blood Transfus. 2011, 9, 120–138. [Google Scholar] [CrossRef]
- Vezzoli, A.; Dellanoce, C.; Caimi, T.M.; Vietti, D.; Montorsi, M.; Mrakic-Sposta, S.; Accinni, R. Influence of Dietary Supplementation for Hyperhomocysteinemia Treatments. Nutrients 2020, 12, 1957. [Google Scholar] [CrossRef] [PubMed]
- Karst, M.; Hollenhorst, J.; Achenbach, J. Life-threatening course in coronavirus disease 2019 (COVID-19): Is there a link to methylenetetrahydrofolic acid reductase (MTHFR) polymorphism and hyperhomocysteinemia? Med. Hypotheses. 2020, 144, 110234. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Pastorino, L.; Manfredini, M.; Ozben, T.; Oliva, G.; Kaleci, S.; Iannella, R.; Tomasi, A. COVID-19 spreading across world correlates with C677T allele of the methylenetetrahydrofolate reductase (MTHFR) gene prevalence. J. Clin. Lab. Anal. 2021, 35, e23798. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bolettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Renaud-Charest, O.; Lui, L.M.W.; Eskander, S.; Ceban, F.; Ho, R.; Vincenzo, J.D.D.; Rosenblat, J.D.; Lee, Y.; Subramaniapillai, M.; McIntyre, R.S. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 2021, 144, 129–137. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nematiet, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID syndrome-associated brain fog. J. Med. Virol. 2022, 94, 979–984. [Google Scholar] [CrossRef]
- Alonso-Lana, S.; Marquié, M.; Ruiz, A.; Boada, M. Cognitive and Neuropsychiatric Manifestations of COVID-19 and Effects on Elderly Individuals With Dementia. Front. Aging Neurosci. 2020, 12, 588872. [Google Scholar] [CrossRef]
- Burdick, K.E.; Millett, C.E. The impact of COVID-19 on cognition in severe cases highlights the need for comprehensive neuropsychological evaluations in all survivors. Neuropsychopharmacology 2021, 46, 2225. [Google Scholar] [CrossRef]
- Jaywant, A.; Vanderlind, W.M.; Alexopoulos, G.S.; Fridman, C.B.; Perlis, R.H.; Gunning, F.M. Frequency and profile of objective cognitive deficits in hospitalized patients recovering from COVID-19. Neuropsychopharmacology 2021, 46, 2235–2240. [Google Scholar] [CrossRef]
- Perry, A.; Wen, W.; Kochan, N.A.; Thalamuthu, A.; Sachdev, P.S.; Breakspear, M. The independent influences of age and education on functional brain networks and cognition in healthy older adults. Hum. Brain Mapp. 2017, 38, 5094–5114. [Google Scholar] [CrossRef] [Green Version]
- Obeid, R.; Herrmann, W. Mechanisms of homocysteine neurotoxicity in neurodegenerative diseases with special reference to dementia. FEBS Lett. 2006, 580, 2994–3005. [Google Scholar] [CrossRef] [Green Version]
- Kamath, A.F.; Chauhan, A.K.; Kisucka, J.; Dole, V.S.; Loscalzo, J.; Handy, D.E.; Wagner, D.D. Elevated levels of homocysteine compromise blood–brain barrier integrity in mice. Blood 2006, 107, 591–593. [Google Scholar] [CrossRef] [Green Version]
- Moafmashhadi, P.; Koski, L. Limitations for interpreting failure on individual subtests of the Montreal cognitive assessment. J. Geriatr. Psychiatry 2012, 26, 19–28. [Google Scholar] [CrossRef]
- Tasci, B.; Tasci, G.; Dogan, S.; Tuncer, T. A novel ternary pattern-based automatic psychiatric disorders classification using ECG signals. Cogn. Neurodynamics 2022, 1–14. [Google Scholar] [CrossRef]
- Macin, G.; Tasci, B.; Tasci, I.; Faust, O.; Barua, P.D.; Dogan, S.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. An accurate multiple sclerosis detection model based on exemplar multiple parameters local phase quantization: ExMPLPQ. Appl. Sci. 2022, 12, 4920. [Google Scholar] [CrossRef]
- Tasci, G.; Loh, H.W.; Barua, P.D.; Baygin, M.; Tasci, B.; Dogan, S.; Tuncer, T.; Palmer, E.E.; Tan, R.-S.; Acharya, U.R. Automated accurate detection of depression using twin Pascal’s triangles lattice pattern with EEG Signals. Knowl.-Based Syst. 2023, 260, 110190. [Google Scholar] [CrossRef]
- Dogan, S.; Baygin, M.; Tasci, B.; Loh, H.W.; Barua, P.D.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. Primate brain pattern-based automated Alzheimer’s disease detection model using EEG signals. Cogn. Neurodyn. 2022, 1–13. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Recovered from COVID-19 Group | Control Group | Total | p | |||||
|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | |||
| Gender | Male | 31 | 50.0% | 33 | 51.6% | 64 | 50.8% | χ2 = 0.031 p = 0.501 |
| Female | 31 | 50.0% | 31 | 48.4% | 62 | 49.2% | ||
| Socio- Economic Status | Low | 34 | 55.8% | 37 | 57.8 | 71 | 56.3% | χ2 = 1.176 p = 0.249 |
| Middle | 17 | 27.4% | 15 | 23.4 | 32 | 25.4% | ||
| High | 11 | 16.8% | 12 | 18.8 | 23 | 18.3% | ||
| Mean ± SD | Mean ± SD | t | p | |||||
| Age | 39.74 ± 9.42 | 40.51 ± 9.18 | −0.46 | 0.642 | ||||
| Years of formal education | 7.04 ± 5.78 | 6.06 ± 5.34 | 0.99 | 0.322 | ||||
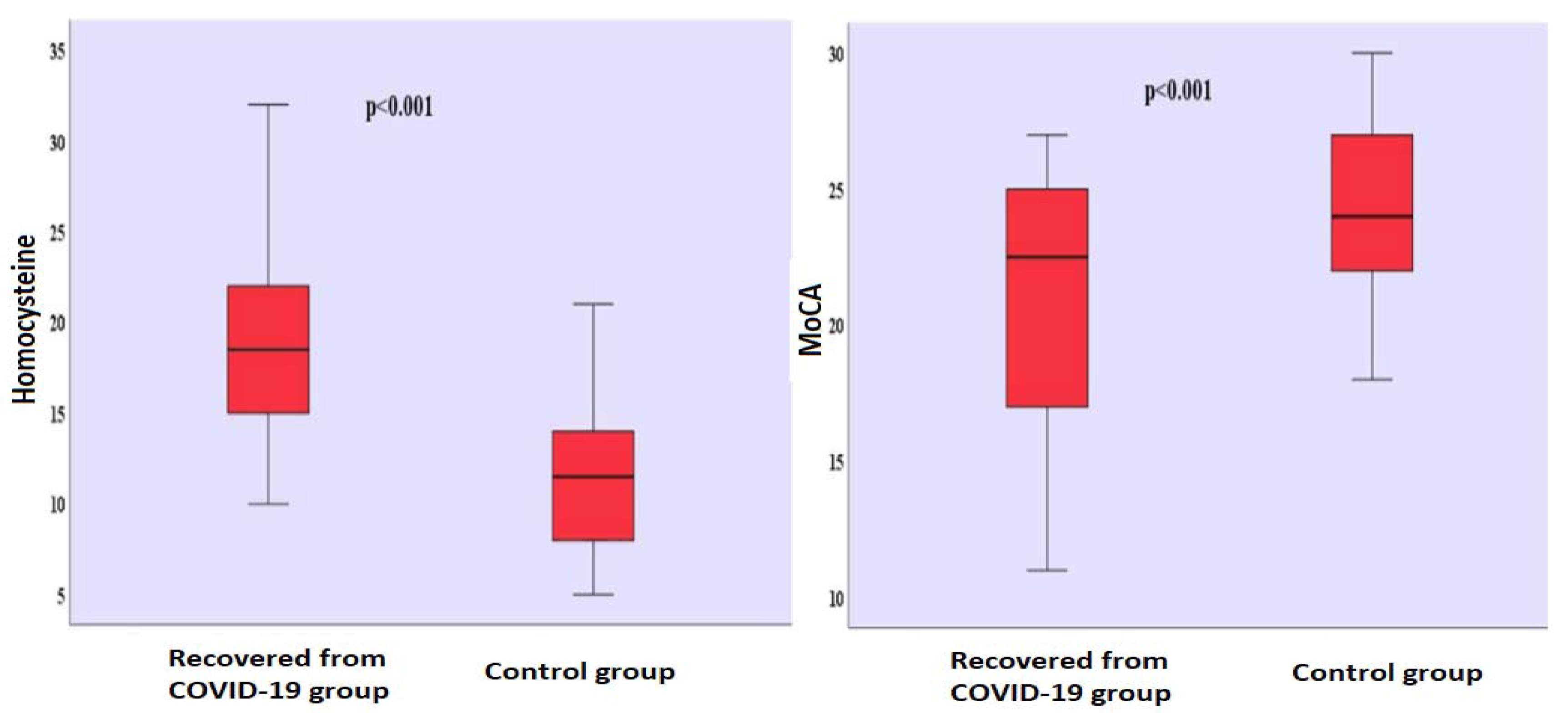
| Homocysteine (µmol/L) | 19.06 ± 4.68 | 11.31 ± 3.72 | 10.30 | <0.001 | ||||
| BDI | 4.27 ± 2.73 | 3.51 ± 2.61 | 1.59 | 0.115 | ||||
| MoCA | 20.77 ± 4.47 | 24.29 ± 3.13 | −5.13 | <0.001 | ||||
| Vitamin B (ng/L) | 184 ± 7.25 | 201 ± 10,43 | −0.58 | 0.593 | ||||
| Folic acid (µg/L) | 5.47 ± 0.71 | 6.19 ± 0.86 | −1.21 | 0.275 | ||||
| The time that passed after positive RT-PCR test (Months) | 10.43 ± 5.18 | - | - | - | ||||
| Homocysteine (µmol/L) | MoCA | |||
|---|---|---|---|---|
| R | p | r | p | |
| Age | 0.247 | 0.053 | 0.252 | 0.048 * |
| Years of formal education | - | - | 0.253 | 0.048 * |
| The time that passed after positive RT-PCR test (Months) | 0.020 | 0.879 | −0.071 | 0.581 |
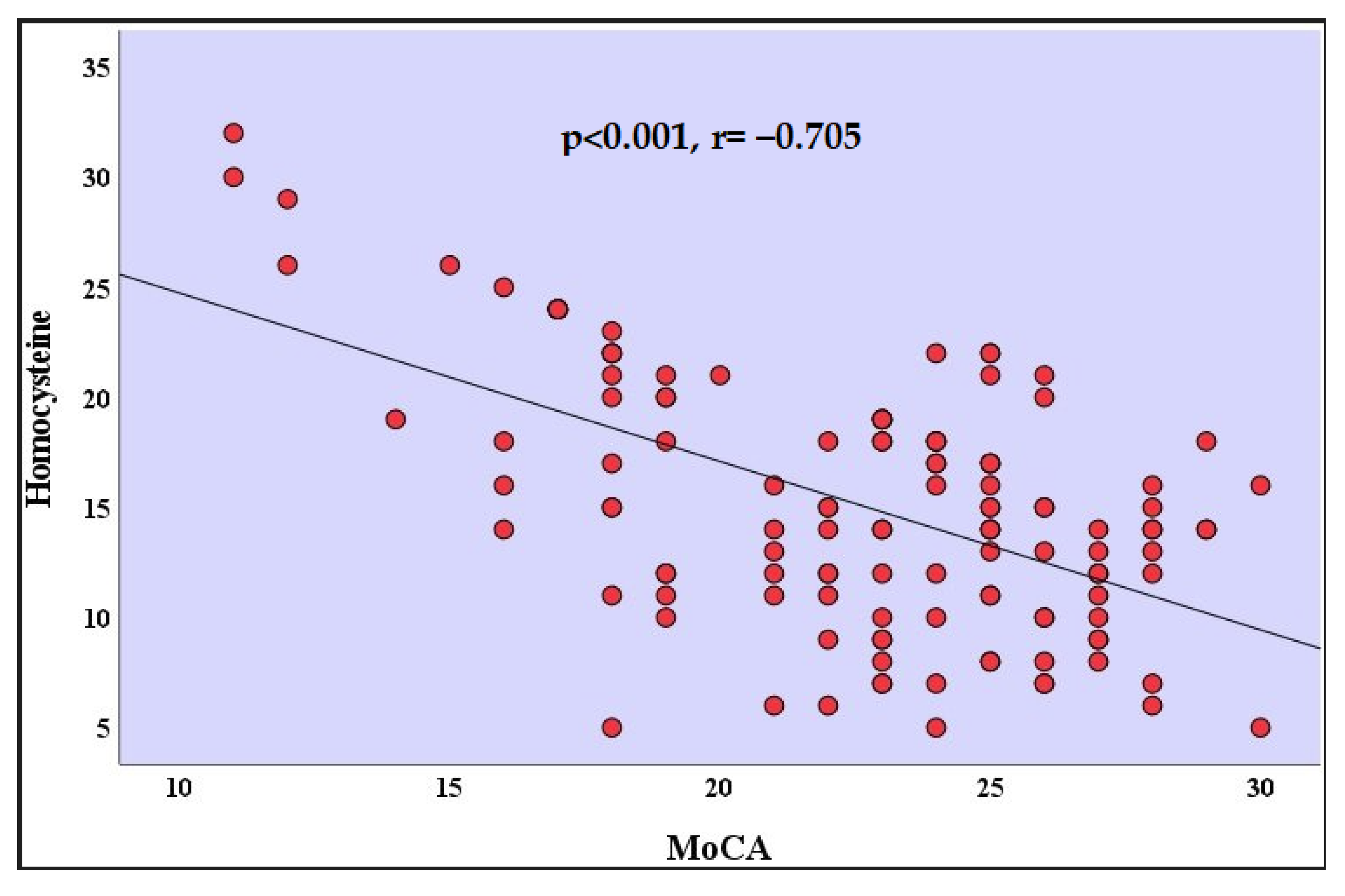
| MoCA | −0.705 ** | <0.001 | - | - |
| Homocysteine (µmol/L) | MoCA | |||
|---|---|---|---|---|
| r | p | r | p | |
| Age | −0.040 | 0.753 | −0.077 | 0.547 |
| Years of formal education | - | - | 0.303 * | 0.015 |
| MoCA | −0.260 * | 0.038 | - | - |
| Unstandardized Coefficients | Standardized Coefficients | t | p | ||
|---|---|---|---|---|---|
| B | Std. Error | β | |||
| (Constant) | 34.388 | 2.399 | 14.336 | <0.0001 | |
| Age | −0.054 | 0.043 | −0.114 | −1.265 | 0.211 |
| Gender | −0.098 | 0.828 | −0.011 | −0.118 | 0.906 |
| Years of formal education | 0.218 | 0.070 | 0.282 | 3.134 | 0.003 |
| Homocysteine (µmol/L) | −0.650 | 0.085 | −0.681 | −7.607 | <0.0001 |
| The time that passed after positive RT-PCR test (Months) | −0.043 | 0.078 | −0.050 | −0.559 | 0.578 |
| Unstandardized Coefficients | Standardized Coefficients | t | p | ||
|---|---|---|---|---|---|
| B | Std. Error | β | |||
| (Constant) | 30.216 | 1.897 | 15.926 | <0.001 | |
| Age | −0.057 | 0.033 | −0.125 | −1.706 | 0.091 |
| Gender | 0.220 | 0.618 | 0.026 | 0.355 | 0.723 |
| Years of formal education | 0.107 | 0.056 | 0.141 | 1.912 | 0.058 |
| Homocysteine (µmol/L) | −0.423 | 0.054 | −0.574 | −7.806 | <0.001 |
| Unstandardized Coefficients | Standardized Coefficients | t | p | ||
|---|---|---|---|---|---|
| B | Std. Error | β | |||
| (Constant) | 29.648 | 1.718 | 17.255 | <0.0001 | |
| Age | −0.040 | 0.030 | −0.088 | −1.335 | 0.184 |
| Gender | 0.416 | 0.556 | 0.050 | 0.749 | 0.455 |
| Years of formal education | 0.175 | 0.050 | 0.231 | 3.497 | 0.001 |
| Homocysteine (µmol/L) | −0.479 | 0.048 | −0.650 | −9.893 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oner, P.; Yilmaz, S.; Doğan, S. High Homocysteine Levels Are Associated with Cognitive Impairment in Patients Who Recovered from COVID-19 in the Long Term. J. Pers. Med. 2023, 13, 503. https://doi.org/10.3390/jpm13030503
Oner P, Yilmaz S, Doğan S. High Homocysteine Levels Are Associated with Cognitive Impairment in Patients Who Recovered from COVID-19 in the Long Term. Journal of Personalized Medicine. 2023; 13(3):503. https://doi.org/10.3390/jpm13030503
Chicago/Turabian StyleOner, Pinar, Seda Yilmaz, and Serpil Doğan. 2023. "High Homocysteine Levels Are Associated with Cognitive Impairment in Patients Who Recovered from COVID-19 in the Long Term" Journal of Personalized Medicine 13, no. 3: 503. https://doi.org/10.3390/jpm13030503