
Does the Potocki–Lupski Syndrome Convey the Autism Spectrum Disorder Phenotype? Case Report and Scoping Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical and Behavioral Assessment
2.2. Electroencephalographic Assessment
2.2.1. EEG Recording
2.2.2. EEG Analysis
- The presence and the coverage of diffuse rhythmic activity or the generalized background slowing.
- Epileptiform EEG abnormalities:
- Sporadic wave discharges, spikes, and multi-spikes are classified as a benign focal epileptiform discharge of childhood without clinical correlates.
- Episodic peak–wave or slow spike–wave complexes, which were not accompanied by clinical events and did not show repetitive structure, generalization, or secondary generalization, which correlated (or not) with clinical events. The topography of this activity was also taken into account.
- Typical or atypical epileptiform discharges manifesting with secondary generalized spike–slow wave discharges or spike–wave discharges that correlated (or not) with clinical events.
2.3. Literature Search for Scoping Review
3. Results
3.1. Clinical and Behavioral Assessment
3.1.1. Case Presentation
3.1.2. Core Features of Autism Spectrum Disorder
3.1.3. Language Development
3.1.4. Cognitive Development
3.1.5. Adaptive Functioning
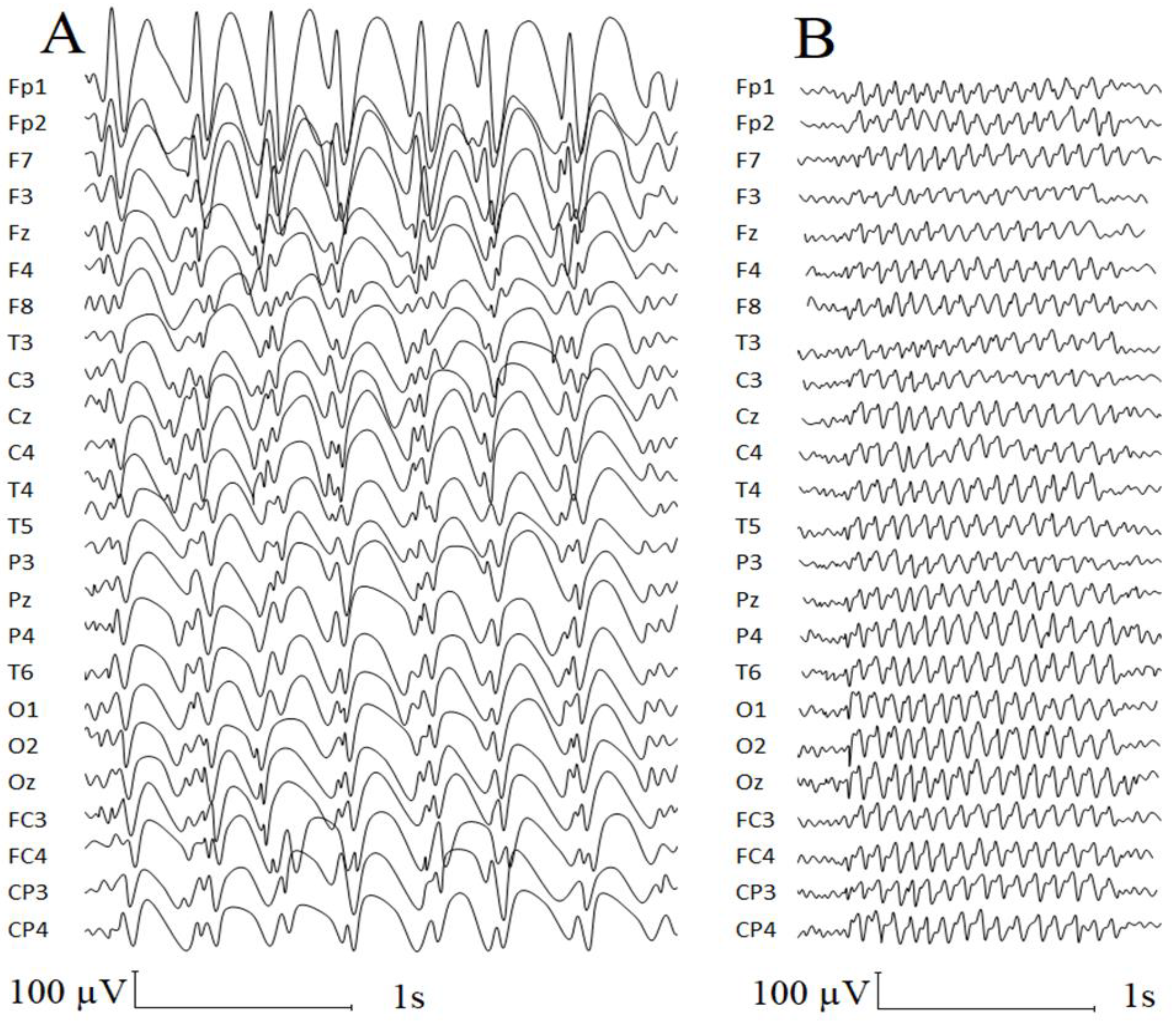
3.2. Electroencephalographic Assessment
3.3. Scoping Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Authors, Year | Number of Patients (Sex) | Age | ASD/ASD Traits Cases | Diagnostic Methods of ASD Identification | Other Developmental Problems (Across Lifespan) | EEG Abnormalities |
|---|---|---|---|---|---|---|
| Stomnaroska & Neskovska, 2021 [36] | 1 (female) | 18 m. | ASD traits (1/1) | NA | Developmental delay; aggressiveness; hyperactivity; inability to establish contacts with family members (1/1) | NA |
| Ciaccio et al., 2020 [3] | 8 (5 females) | 2 yrs 7 mos.–47 yrs. | ASD (1/8) | NA | Anxiety (2/8); developmental delay (7/8); lacking expressive language development (2/8); mild to moderate intellectual impairment (7/8); ADHD features (1/8) | Diffuse rhythmic activity (7/8); sporadic diffuse epileptic anomalies, without clinical correlate (1/8); cortical heterotopia (1/8) |
| Shuib et al., 2017 [37] | 1 (female) | 3 yrs. | NA | NA | Developmental delay; hyperactivity | NA |
| Sanchez-Valle et al., 2011 [29] | 1 (male) | 9 yrs. | No ASD | Multidisciplinary team | Developmental delay; moderate intellectual disability; severe speech and language impairment; repetitive and obsessive–compulsive behaviors | An EEG revealed diffuse changes without a seizure focus; repeat EEG was normal |
| Potocki et al., 2007 [4] | 10 (4 females) | 25 mos.-14.5 yrs. | Autistic traits (9/10) | Multidisciplinary team; ADI-R and ADOS-G in a one case | Developmental delay; cognitive impairment; low adaptive functioning; language impairment; articulation difficulties (10/10) | Abnormal EEG (9/9); slow occipital dominant rhythm (“alpha”) (6/9); generalized and/or focal epileptiform abnormalities (spikes, sharp waves, and spike and slow-wave discharges) (4/9); EEG seizure discharges (0/9) |
| Treadwell-Deering et al., 2010 [1] | 15 (6 females) | 2 yrs. 1 mos. – 14 yrs. 5 mos. | ASD (10/15) | Psychiatric evaluation in 7 cases; psychiatric evaluation, ADOS-G, and ADI-R in 8 cases | Borderline to moderate intellectual disability (13/15); executive functioning deficits (15/15); problems with withdrawal (majority); high levels of hyperactivity and anxiety (>50%); significant language delay (7/7) | NA |
| Zhang et al., 2010 [38] | 5 (3 females) | 3-40 yrs | Autistic traits (3/5) | NA | Developmental delay (4/5); cognitive impairment (5/5); hyperactivity (4/5); negative behaviors (5/5) | NA |
| Lee et al., 2013 [22] | 1 (male) | 3 yrs. 4 mos. | No ASD | DSM-IV | Developmental delay; mild intellectual disability; receptive and expressive language developmental delay; motor developmental delay | NA |
| Ercan-Sencicek et al., 2012 [5] | 1 (male) | 10 yrs. 10 mos. | No ASD | Developmental and psychological evaluations | Developmental delay; speech and language disability; reading disorder; disorder of written expression; learning disorder not otherwise specified; expressive language disorder | NA |
| Praticò et al., 2018 [2] | 1 (male) | 5 yrs | No ASD | ADOS-G, ADI-R | Psychomotor delay, severe language impairment; borderline cognitive delay; behavioral disturbances (hyperactivity, irascibility, and impulsivity). | NA |
| Sumathipala et al., 2015 [39] | 1 (female) | 4 yrs. | No ASD | NA | Severe expressive language impairment, borderline to mild intellectual disability | NA |
| Lee et al., 2012 [40] | 1 (male) | 17 yrs. | No ASD | Neurodevelopmental evaluation | Language delay (both receptive and expressive); moderate intellectual disability | NA |
| Magoulas et al., 2014 [23] * | 1 (1st family, mother) | 40 yrs. | No ASD | NA | History of developmental delay; intellectual disability; bipolar disorder; anxiety; attention deficit disorders | NA |
| 1 (1st family, child, male) | 5 yrs. | No ASD | NA | Global developmental delay; short attention span; low frustration tolerance; difficulty with transitions and changes to routine. | NA | |
| 1 (2nd family, mother) | 24 yrs. | No ASD | NA | Substantial speech delay; learning difficulties | NA | |
| Yusupov et al., 2011 [41] | 1 (mother) | ~35 (not specified) | No ASD | NA | Some language delay and learning problems | NA |
| 1 (1st child, female) | 3 yrs. 4 mos. | NA | NA | Global developmental delays (both fine motor delays and significant language delays) | NA | |
| 1 (2nd child, female) | birth - 21 mos. | NA | NA | NA | NA | |
| Current case | 1 (female) | No ASD | ADOS-2, ADI-R, DSM-5 TR | Developmental delay; mild intellectual disability; speech and language disorders |
References
- Treadwell-Deering, D.E.; Powell, M.P.; Potocki, L. Cognitive and behavioral characterization of the Potocki-Lupski syndrome (duplication 17p11.2). J. Dev. Behav. Pediatr. 2010, 31, 137–143. [Google Scholar] [CrossRef]
- Praticò, A.D.; Falsaperla, R.; Rizzo, R.; Ruggieri, M.; Verrotti, A.; Pavone, P. A New Patient with Potocki-Lupski Syndrome: A Literature Review. J. Pediatr. Genet. 2018, 7, 29–34. [Google Scholar] [CrossRef]
- Ciaccio, C.; Pantaleoni, C.; Milani, D.; Alfei, E.; Sciacca, F.L.; Canafoglia, L.; Erbetta, A.; D’Arrigo, S. Neurological phenotype of Potocki-Lupski syndrome. Am. J. Med. Genet. A 2020, 182, 2317–2324. [Google Scholar] [CrossRef]
- Potocki, L.; Bi, W.; Treadwell-Deering, D.; Carvalho, C.M.; Eifert, A.; Friedman, E.M.; Glaze, D.; Krull, K.; Lee, J.A.; Lewis, R.A.; et al. Characterization of Potocki-Lupski syndrome (dup(17)(p11.2p11.2)) and delineation of a dosage-sensitive critical interval that can convey an autism phenotype. Am. J. Hum. Genet. 2007, 80, 633–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercan-Sencicek, A.G.; Wright, N.R.D.; Frost, S.J.; Fulbright, R.K.; Felsenfeld, S.; Hart, L.; Landi, N.; Mencl, W.E.; Sanders, S.J.; Pugh, K.R.; et al. Searching for Potocki-Lupski syndrome phenotype: A patient with language impairment and no autism. Brain Dev. 2012, 34, 700–703. [Google Scholar] [CrossRef] [Green Version]
- Naumova, O.Y.; Dobrynin, P.V.; Gibitova, E.A.; Zhukova, M.A.; Rychkov, S.Y.; Zhukova, O.V.; Grigorenko, E.L. Identification of Pathogenic CNVs in Unexplained Developmental Disabilities Using Exome Sequencing: A Family Trio Study. Russ. J. Genet. 2021, 57, 1351–1355. [Google Scholar] [CrossRef]
- Zhukova, M.A.; Kornilov, S.A.; Simmons, E.; Grigorenko, E.L. Diagnostika razvitia yazika i rechi s pomoshchju yazikovikh shkal doshkol’nikov: Analiz individual’nogo sluchaya [Speech and Language Assessment using Preschool Language Scales: A Case Study]. Vopr. Psikhol. 2016, 5, 154–164. [Google Scholar]
- Talantseva, O.I.; Zhukova, M.A.; Trubitsyna, A.N.; Teedemaa, A.V.; Grigorenko, E.L. Psychometric Properties of the Preschool Language Scales, (PLS-5) in Russian-Speaking Children: A Classical and Item Response Theory Study. Clin. Psychol. Spec. Educ. 2022, 11, 174–195. [Google Scholar] [CrossRef]
- Zimmerman, I.L.; Steiner, V.G.; Pond, R.E. Preschool Language Scales–Fifth Edition (PLS-5); Pearson: Bloomington, MN, USA, 2011. [Google Scholar]
- Babyonyshev, M.; Hart, L.; Reich, J.; Kuznetsova, J.; Rissman, R.; Grigorenko, E.L. Otsenka Razvitiya Russkogo Yazy ‘ka [Assessment of the Development of Russian]. 2007; unpublished manual. [Google Scholar]
- Bracken, B.A.; McCallum, R.S. Universal Nonverbal Intelligence Test; PRO-ED: Austin, TX, USA, 2016. [Google Scholar]
- Ovchinnikova, I.V.; Zhukova, M.A.; Grigorenko, E.L. Aprobacija metodiki Vineland Adaptive Behavior Scales (VABS) na russkojazychnoj vyborke [Approbation of Vineland Adaptive Behavior Scales (VABS) on a Russian-speaking sample]. Vopr. Psikhol. 2018, 6, 134–146. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.V. Vineland Adaptive Behavior Scales; Pearson Assessment: San Antonio, TX, USA, 2005. [Google Scholar]
- Falkmer, T.; Anderson, K.; Falkmer, M.; Horlin, C. Diagnostic procedures in autism spectrum disorders: A systematic literature review. Eur. Child. Adolesc. Psychiatry 2013, 22, 329–340. [Google Scholar] [CrossRef]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule–2nd Edition (ADOS-2); Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. ADI-R. Interv’yu dlya diagnoctiki aytizma: Rykovodstvo [ADI-R. Autism Diagnostic Interview: Manual]; Western Psychological Services: Los Angeles, CA, USA; Giunti Psychometrics Rus: Moscow, Russia, 2014. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. ADOS-2. Autism Diagnostic Observation Schedule: Manual, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA; Giunti Psychometrics Rus: Moscow, Russia, 2016. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American psychiatric association: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]
- Soghoyan, G.; Ledovsky, A.; Nekrashevich, M.; Martynova, O.; Polikanova, I.; Portnova, G.; Rebreikina, A.; Sysoeva, O.; Sharaev, M. A Toolbox and Crowdsourcing Platform for Automatic Labeling of Independent Components in Electroencephalography. Front. Neuroinform. 2021, 15, 720229. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council on children with disabilities, section on developmental and behavioral pediatrics. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.G.; Park, S.J.; Yim, S.Y.; Sohn, Y.B. Clinical and cytogenetic features of a Potocki-Lupski syndrome with the shortest 0.25Mb microduplication in 17p11.2 including RAI1. Brain Dev. 2013, 35, 681–685. [Google Scholar] [CrossRef]
- Magoulas, P.L.; Liu, P.; Gelowani, V.; Soler-Alfonso, C.; Kivuva, E.C.; Lupski, J.R.; Potocki, L. Inherited dup(17)(p11.2p11.2): Expanding the phenotype of the Potocki-Lupski syndrome. Am. J. Med. Genet. A 2014, 164A, 500–504. [Google Scholar] [CrossRef]
- Molina, J.; Carmona-Mora, P.; Chrast, J.; Krall, P.M.; Canales, C.P.; Lupski, J.R.; Reymond, A.; Walz, K. Abnormal social behaviors and altered gene expression rates in a mouse model for Potocki-Lupski syndrome. Hum. Mol. Genet. 2008, 17, 2486–2495. [Google Scholar] [CrossRef] [Green Version]
- Richards, C.; Jones, C.; Groves, L.; Moss, J.; Oliver, C. Prevalence of autism spectrum disorder phenomenology in genetic disorders: A systematic review and meta-analysis. Lancet Psychiatry 2015, 2, 909–916. [Google Scholar] [CrossRef] [Green Version]
- Fombonne, E.; MacFarlane, H.; Salem, A.C. Epidemiological surveys of ASD: Advances and remaining challenges. J. Autism. Dev. Disord. 2021, 51, 4271–4290. [Google Scholar] [CrossRef]
- Amiet, C.; Gourfinkel-An, I.; Bouzamondo, A.; Tordjman, S.; Baulac, M.; Lechat, P.; Mottron, L.; Cohen, D. Epilepsy in autism is associated with intellectual disability and gender: Evidence from a meta-analysis. Biol. Psychiatry 2008, 64, 577–582. [Google Scholar] [CrossRef]
- Precenzano, F.; Parisi, L.; Lanzara, V.; Vetri, L.; Operto, F.; Pastorino, G.; Ruberto, M.; Messina, G.; Risoleo, M.; Santoro, C.; et al. Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications. Medicina 2020, 56, 419. [Google Scholar] [CrossRef]
- Sanchez-Valle, A.; Pierpont, M.E.; Potocki, L. The severe end of the spectrum: Hypoplastic left heart in Potocki-Lupski syndrome. Am. J. Med. Genet. A 2011, 155A, 363–366. [Google Scholar] [CrossRef] [Green Version]
- Portnova, G.; Neklyudova, A.; Voinova, V.; Sysoeva, O. Clinical EEG of Rett Syndrome: Group Analysis Supplemented with Longitudinal Case Report. J. Pers. Med. 2022, 12, 1973. [Google Scholar] [CrossRef] [PubMed]
- Cecchin, T.; Ranta, R.; Koessler, L.; Caspary, O.; Vespignani, H.; Maillard, L. Seizure lateralization in scalp EEG using Hjorth parameters. Clin. Neurophysiol. 2010, 121, 290–300. [Google Scholar] [CrossRef]
- Ouyang, C.S.; Yang, R.C.; Wu, R.C.; Chiang, C.T.; Lin, L.C. Determination of Antiepileptic Drugs Withdrawal through EEG Hjorth Parameter Analysis. Int. J. Neural Syst. 2020, 30, 2050036. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, M.; Won, D.; Manoharan, T.A.; Venkatachalam, V.; Chavan, R.M.; Nalla, H.D. Investigating electroencephalography signals of autism spectrum disorder (ASD) using Higuchi Fractal Dimension. Biomed. Tech. 2020, 66, 59–70. [Google Scholar] [CrossRef]
- Portnova, G.V.; Atanov, M.S. Nonlinear EEG parameters of emotional perception in patients with moderate traumatic brain injury, coma, stroke and schizophrenia. AIMS Neurosci. 2018, 5, 221. [Google Scholar] [CrossRef]
- Portnova, G.V.; Skorokhodov, I.; McGlone, F.; Varlamov, A. EEG Correlates of Tactile Perception Abnormalities in Children with Autism Spectrum Disorder. Sovrem. Tehnol. Med. 2019, 11, 169–174. [Google Scholar] [CrossRef]
- Stomnaroska, O.; Neskovska, L. Potocki-Lupski Syndrome Dup17p11.2 in a Girl with Hypotonia and Early Behavioural Disturbances. Prilozi 2021, 42, 91–94. [Google Scholar] [CrossRef]
- Shuib, S.; Saaid, N.N.; Zakaria, Z.; Ismail, J.; Abdul Latiff, Z. Duplication 17p11.2 (Potocki-Lupski Syndrome) in a child with developmental delay. Malays. J. Pathol. 2017, 39, 77–81. [Google Scholar]
- Zhang, F.; Potocki, L.; Sampson, J.B.; Liu, P.; Sanchez-Valle, A.; Robbins-Furman, P.; Navarro, A.D.; Wheeler, P.G.; Spence, J.E.; Brasington, C.K.; et al. Identification of uncommon recurrent Potocki-Lupski syndrome-associated duplications and the distribution of rearrangement types and mechanisms in PTLS. Am. J. Hum. Genet. 2010, 86, 462–470. [Google Scholar] [CrossRef] [Green Version]
- Sumathipala, D.S.; Mandawala, E.N.; Sumanasena, S.P.; Dissanayake, V.H. 17p11.2 and Xq28 duplication detected in a girl diagnosed with Potocki-Lupski syndrome. BMC Res. Notes 2015, 8, 506. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.G.; Park, S.J.; Yun, J.N.; Yim, S.Y.; Sohn, Y.B. Reciprocal deletion and duplication of 17p11.2-11.2: Korean patients with Smith-Magenis syndrome and Potocki-Lupski syndrome. J. Korean Med. Sci. 2012, 27, 1586–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusupov, R.; Roberts, A.E.; Lacro, R.V.; Sandstrom, M.; Ligon, A.H. Potocki-Lupski syndrome: An inherited dup(17)(p11.2p11.2) with hypoplastic left heart. Am. J. Med. Genet. A 2011, 155, 367–371. [Google Scholar] [CrossRef] [PubMed]


| ADOS-2 Scales | Item | Score |
|---|---|---|
| Social affect (SA) | ||
| Language and communication | ||
| Reporting of events | A-7 | 2 |
| Conversation | A-8 | 1 |
| Descriptive, conventional, or informational gestures | A-9 | 1 |
| Reciprocal social interaction | ||
| Unusual eye contact | B-1 | 0 |
| Facial expressions directed to others | B-2 | 0 |
| Shared enjoyment in interaction | B-4 | 1 |
| Quality of social overtures | B-7 | 1 |
| Quality of social response | B-9 | 0 |
| Amount of reciprocal social communication | B-10 | 0 |
| Overall quality of rapport | B-11 | 0 |
| SA total | 6 | |
| Restricted and repetitive behavior (RRB) | ||
| Play, stereotyped behaviors and restricted interests | ||
| Stereotyped/idiosyncratic use of words or phrases | A-4 | 0 |
| Unusual sensory interest in play material/person | D-1 | 0 |
| Hand and finger and other complex mannerisms | D-2 | 0 |
| Excessive interest in or references to unusual or highly specific topics or objects or repetitive behaviors | D-4 | 0 |
| RRB total | 0 | |
| Overall total | 6 |
| UNIT-2 Composite | Index Score | 95% CI | Percentile Rank | Descriptive Classification |
|---|---|---|---|---|
| Memory | 73 | [67, 82] | 4 | Delayed |
| Reasoning | 65 | [61, 72] | 1 | Very delayed |
| Quantitative | 71 | [67, 77] | 3 | Delayed |
| Full scale battery | 64 | [61, 69] | 1 | Very delayed |
| Domain | Scores | V-Scores | Descriptive Classification | Standard Scores | Percentile |
|---|---|---|---|---|---|
| Receptive | 39 | 14 | Adequate | ||
| Expressive | 81 | 7 | Low | ||
| Written | 19 | 7 | Low | ||
| Communication | 28 | Low, mild deficit | 69 | 2% | |
| Personal | 66 | 9 | Low | ||
| Domestic | 24 | 10 | Moderately low, mild deficit | ||
| Community | 29 | 7 | Low | ||
| Daily living skills | 26 | Low, mild deficit | 65 | 1% | |
| Interpersonal relationship | 68 | 10 | Moderately low | ||
| Play and leisure time | 44 | 8 | Low | ||
| Coping skills | 39 | 12 | Low | ||
| Socialization | 30 | Moderately low | 73 | 4% | |
| Adaptive behavior composite | Low, mild deficit | 67 | 1% | ||
| Internalizing | 4 | 18 | Elevated | ||
| Externalizing | 1 | 16 | Average | ||
| Maladaptive behavior index | 9 | 17 | Average |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talantseva, O.I.; Portnova, G.V.; Romanova, R.S.; Martynova, D.A.; Sysoeva, O.V.; Grigorenko, E.L. Does the Potocki–Lupski Syndrome Convey the Autism Spectrum Disorder Phenotype? Case Report and Scoping Review. J. Pers. Med. 2023, 13, 439. https://doi.org/10.3390/jpm13030439
Talantseva OI, Portnova GV, Romanova RS, Martynova DA, Sysoeva OV, Grigorenko EL. Does the Potocki–Lupski Syndrome Convey the Autism Spectrum Disorder Phenotype? Case Report and Scoping Review. Journal of Personalized Medicine. 2023; 13(3):439. https://doi.org/10.3390/jpm13030439
Chicago/Turabian StyleTalantseva, Oksana I., Galina V. Portnova, Raisa S. Romanova, Daria A. Martynova, Olga V. Sysoeva, and Elena L. Grigorenko. 2023. "Does the Potocki–Lupski Syndrome Convey the Autism Spectrum Disorder Phenotype? Case Report and Scoping Review" Journal of Personalized Medicine 13, no. 3: 439. https://doi.org/10.3390/jpm13030439