
No Differences in Rotational Thromboelastometry Measurements between Portal and Peripheral Circulation in Cirrhotic Patients Undergoing TIPS
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
- mild/moderate liver cirrhosis: MELD < 15 or CP 5–6 points [stage A: mild cirrhosis] or CP 7–9 points [stage B: moderate cirrhosis]
- severe liver cirrhosis: MELD ≥ 15 or CP 10–15 points [stage C]
2.3. Blood Sampling
2.4. Rotational Thromboelastometry
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. TIPS Implantation and Procedure Related Data
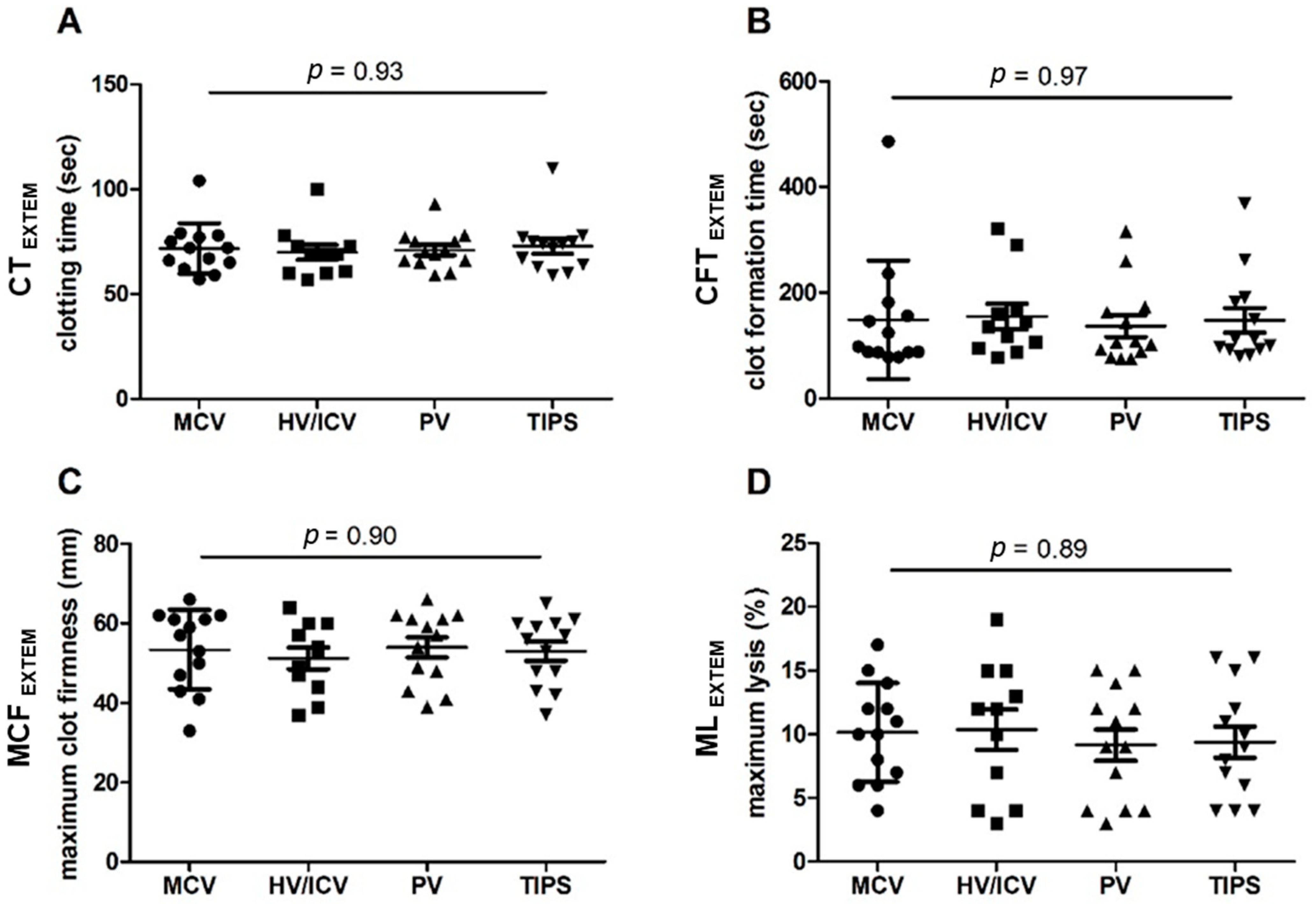
3.3. EXTEM Analysis in Blood Samples from Different Vascular Compartments during TIPS
- -
- Mean CT was 72 ± 12 s in MCV blood samples, 70 ± 12 s in HV/ICV blood samples, 71 ± 9 s in PV blood samples, and 73 ± 13 s in TIPS blood samples.
- -
- Mean CFT was 149 ± 112 s in MCV blood samples, 155 ± 80 s in HV/ICV blood samples, 137 ± 75 s in PV blood samples, and 148 ± 85 s in TIPS blood samples.
- -
- Mean MCF was 53 ± 10 mm in MCV blood samples, 51 ± 9 mm in HV/ICV blood samples, 54 ± 9 mm in PV blood samples, and 53 ± 9 mm in TIPS blood samples.
- -
- Mean ML was 10 ± 4% in MCV blood samples, 10 ± 5% in HV/ICV blood samples, 9 ± 4% in PV blood samples, and 9 ± 4% in TIPS blood samples.
4. Discussion
5. Conclusions
Ethical Approval
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rossle, M. TIPS: 25 years later. J. Hepatol. 2013, 59, 1081–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochar, N.; Tripathi, D.; McAvoy, N.C.; Ireland, H.; Redhead, D.N.; Hayes, P.C. Bleeding ectopic varices in cirrhosis: The role of transjugular intrahepatic portosystemic stent shunts. Aliment. Pharmacol. Ther. 2008, 28, 294–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiper, J.J.; de Man, R.A.; van Buuren, H.R. Review article: Management of ascites and associated complications in patients with cirrhosis. Aliment. Pharmacol. Ther. 2007, 26 (Suppl. 2), 183–193. [Google Scholar] [CrossRef] [PubMed]
- Attwell, A.; Ludkowski, M.; Nash, R.; Kugelmas, M. Treatment of Budd-Chiari syndrome in a liver transplant unit, the role of transjugular intrahepatic porto-systemic shunt and liver transplantation. Aliment. Pharmacol. Ther. 2004, 20, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, D.; Macnicholas, R.; Kothari, C.; Sunderraj, L.; Al-Hilou, H.; Rangarajan, B.; Chen, F.; Mangat, K.; Elias, E.; Olliff, S. Good clinical outcomes following transjugular intrahepatic portosystemic stent-shunts in Budd-Chiari syndrome. Aliment. Pharmacol. Ther. 2014, 39, 864–872. [Google Scholar] [CrossRef]
- Cardenas, A.; Kelleher, T.; Chopra, S. Review article: Hepatic hydrothorax. Aliment. Pharmacol. Ther. 2004, 20, 271–279. [Google Scholar] [CrossRef]
- Buechter, M.; Manka, P.; Gerken, G.; Canbay, A.; Blomeyer, S.; Wetter, A.; Altenbernd, J.; Kahraman, A.; Theysohn, J.M. Transjugular Intrahepatic Portosystemic Shunt in Patients with Portal Hypertension: Patency Depends on Coverage and Interventionalist’s Experience. Dig. Dis. 2018, 36, 218–227. [Google Scholar] [CrossRef]
- Wan, Y.M.; Li, Y.H.; Wu, H.M.; Xu, Z.Y.; Xu, Y.; Yang, L.H.; Wu, X.N.; Yang, J.H. Portal vein thrombosis before and after transjugular intrahepatic portosystemic shunt placement: An observational study (STROBE compliant). Medicine 2017, 96, e8498. [Google Scholar] [CrossRef]
- Jahangiri, Y.; Kerrigan, T.; Li, L.; Prosser, D.; Brar, A.; Righetti, J.; Schenning, R.C.; Kaufman, J.A.; Farsad, K. Risk factors for stent graft thrombosis after transjugular intrahepatic portosystemic shunt creation. Cardiovasc. Diagn. Ther. 2017, 7, S150–S158. [Google Scholar] [CrossRef]
- Lv, Y.; He, C.; Wang, Z.; Guo, W.; Wang, J.; Bai, W.; Zhang, L.; Wang, Q.; Liu, H.; Luo, B.; et al. Association of Nonmalignant Portal Vein Thrombosis and Outcomes after Transjugular Intrahepatic Portosystemic Shunt in Patients with Cirrhosis. Radiology 2017, 285, 999–1010. [Google Scholar] [CrossRef] [Green Version]
- Tripodi, A. Tests of coagulation in liver disease. Clin. Liver Dis. 2009, 13, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Senzolo, M.; Germani, G.; Gatt, A.; Burroughs, A.K. Systematic review: Portal vein thrombosis in cirrhosis. Aliment. Pharmacol. Ther. 2010, 31, 366–374. [Google Scholar] [CrossRef]
- Moore, K.L.; Andreoli, S.P.; Esmon, N.L.; Esmon, C.T.; Bang, N.U. Endotoxin enhances tissue factor and suppresses thrombomodulin expression of human vascular endothelium in vitro. J. Clin. Investig. 1987, 79, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Lumsden, A.B.; Henderson, J.M.; Kutner, M.H. Endotoxin levels measured by a chromogenic assay in portal, hepatic and peripheral venous blood in patients with cirrhosis. Hepatology 1988, 8, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Ferro, D. Clotting activation and hyperfibrinolysis in cirrhosis: Implication for bleeding and thrombosis. Semin. Thromb. Hemost. 2013, 39, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Ferro, D.; Basili, S.; Lionetti, R.; Rossi, E.; Merli, M.; Riggio, O.; Bezzi, M.; Capocaccia, L. Ongoing prothrombotic state in the portal circulation of cirrhotic patients. Thromb. Haemost. 1997, 77, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.S.; Lee, F.Y.; Lee, S.D.; Tsai, Y.T.; Lin, H.C.; Lu, R.H.; Hsu, W.C.; Huang, C.C.; Wang, S.S.; Lo, K.J. Endotoxemia in patients with chronic liver diseases: Relationship to severity of liver diseases, presence of esophageal varices, and hyperdynamic circulation. J. Hepatol. 1995, 22, 165–172. [Google Scholar] [CrossRef]
- Mallett, S.V. Clinical Utility of Viscoelastic Tests of Coagulation (TEG/ROTEM) in Patients with Liver Disease and during Liver Transplantation. Semin. Thromb. Hemost. 2015, 41, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Saner, F.H.; Gieseler, R.K.; Akiz, H.; Canbay, A.; Gorlinger, K. Delicate balance of bleeding and thrombosis in end-stage liver disease and liver transplantation. Digestion 2013, 88, 135–144. [Google Scholar] [CrossRef]
- Bedreli, S.; Sowa, J.P.; Gerken, G.; Saner, F.H.; Canbay, A. Management of acute-on-chronic liver failure: Rotational thromboelastometry may reduce substitution of coagulation factors in liver cirrhosis. Gut 2016, 65, 357–358. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Morrison-McKell, T.; Macik, B.G. 40-Point-of-Care Hemostasis Testing. In Consultative Hemostasis and Thrombosis, 3rd ed.; Kitchens, C.S., Kessler, C.M., Konkle, B.A., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2013; pp. 717–729. [Google Scholar] [CrossRef]
- Vorweg, M.; Hartmann, B.; Knuttgen, D.; Jahn, M.C.; Doehn, M. Management of fulminant fibrinolysis during abdominal aortic surgery. J. Cardiothorac. Vasc. Anesth. 2001, 15, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Patidar, K.R.; Sydnor, M.; Sanyal, A.J. Transjugular intrahepatic portosystemic shunt. Clin. Liver Dis. 2014, 18, 853–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Franchis, R. Baveno VIF. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Zipperle, J.; Schlimp, C.J.; Holnthoner, W.; Husa, A.M.; Nurnberger, S.; Redl, H.; Schochl, H. A novel coagulation assay incorporating adherent endothelial cells in thromboelastometry. Thromb. Haemost. 2013, 109, 869–877. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | TIPS; n = 13 | Normal Range |
|---|---|---|
| Underlying liver disease (n) Primary sclerosing cholangitis (PSC) Alcoholic steatohepatitis (ASH) Hepatitis C virus (HCV) Autoimmune hepatitis Non-alcoholic steatohepatitis (ASH) Cryptogenic cirrhosis | 1 (8%) 6 (46%) 1 (8%) 2 (15%) 2 (15%) 1 (8%) | - |
| Sex (n) male female | 11 (85%) 2 (15%) | - |
| Age (years) | 60 (22; 74) | - |
| MELD § Score ≥15 points <15 points | 12 (8; 22) 4 (31%) 9 (69%) | - |
| Child-Pugh Score [Classification] 5–6 points [stage A] 7–9 points [stage B] 10–15 points [stage C] | 8 (6; 11) 1 (8%) 8 (61%) 4 (31%) | - |
| aPTT ‡ (s) | 29 (26; 66) | 24.4–32.4 |
| Thrombocytes (cells/nL) | 112 (29; 259) | 140–320 |
| INR † | 1.12 (1.05; 1.41) | - |
| Fibrinogen (mg/dL) | 269 (101; 627) | 180–350 |
| Hemoglobin (g/dL) | 10.6 (6.6; 14.5) | 13.7–17.2 |
| Bilirubin total (mg/dL) | 1.0 (0.6; 3.7) | 0.3–1.2 |
| Creatinin (mg/dL) | 1.1 (0.6; 5.0) | 0.9–1.3 |
| Albumin serum (g/dL) | 2.3 (2.1; 2.8) | 3.4–4.8 |
| CRP (mg/dL) | 1.3 (0.5; 13.7) | <0.5 |
| Ascites total protein (mg/dL) | 2086 (461; 3062) | - |
| Indication for TIPS variceal bleeding [high urgent procedure] refractory ascites [elective procedure] | 3 (23%) 10 (77%) | - |
| EXTEM Value | MCV | HV/ICV | PV | TIPS | Normal Range |
|---|---|---|---|---|---|
| CT, s | 72 (57; 104) | 69 (57; 100) | 70 (59; 93) | 74 (59; 110) | 35–80 |
| CFT, s | 98 (78; 486) | 136 (78; 321) | 106 (75; 316) | 112 (79; 368) | 35–160 |
| MCF, mm | 57 (33; 66) | 53 (37; 64) | 57 (39; 66) | 56 (37; 65) | 53–72 |
| ML, % | 10 (4; 17) | 12 (3; 19) | 9 (3; 15) | 9 (4; 16) | <15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedreli, S.; Manka, P.; Buechter, M.; Jahn, M.; Theysohn, J.M.; Canbay, A.; Katsounas, A. No Differences in Rotational Thromboelastometry Measurements between Portal and Peripheral Circulation in Cirrhotic Patients Undergoing TIPS. J. Pers. Med. 2023, 13, 424. https://doi.org/10.3390/jpm13030424
Bedreli S, Manka P, Buechter M, Jahn M, Theysohn JM, Canbay A, Katsounas A. No Differences in Rotational Thromboelastometry Measurements between Portal and Peripheral Circulation in Cirrhotic Patients Undergoing TIPS. Journal of Personalized Medicine. 2023; 13(3):424. https://doi.org/10.3390/jpm13030424
Chicago/Turabian StyleBedreli, Sotiria, Paul Manka, Matthias Buechter, Michael Jahn, Jens M. Theysohn, Ali Canbay, and Antonios Katsounas. 2023. "No Differences in Rotational Thromboelastometry Measurements between Portal and Peripheral Circulation in Cirrhotic Patients Undergoing TIPS" Journal of Personalized Medicine 13, no. 3: 424. https://doi.org/10.3390/jpm13030424